
Abstract
Acupressure is a complementary and alternative medicine (CAM) treatment using fingertips to stimulate acupoints on the skin. Although suggested to improve cognitive function, acupressure has not been previously investigated with a controlled design in traumatic brain injury (TBI) survivors, who could particularly benefit from a non-pharmacological intervention for cognitive impairment. A randomized, placebo-controlled, single-blind design assessed the effects of acupressure (eight treatments over 4 weeks) on cognitive impairment and state of being following TBI, including assessment of event-related potentials (ERPs) during Stroop and auditory oddball tasks. It was hypothesized that active acupressure treatments would confer greater cognitive improvement than placebo treatments, perhaps because of enhanced relaxation response induction and resulting stress reduction. Significant treatment effects were found comparing pre- to post-treatment change between groups. During the Stroop task, the active-treatment group showed greater reduction in both P300 latency (p = 0.010, partial η2 = 0.26) and amplitude (p = 0.011, partial η2 = 0.26), as well as a reduced Stroop effect on accuracy (p = 0.008, partial η2 = 0.21) than did the placebo group. Additionally, the active-treatment group improved more than did the placebo group on the digit span test (p = 0.043, Cohen's d = 0.68). Together, these results suggest an enhancement in working memory function associated with active treatments. Because acupressure emphasizes self-care and can be taught to novice individuals, it warrants further study as an adjunct treatment for TBI.
Introduction
T
Considering the prevalence of TBI and the associated disability, it is important to investigate treatments to assist TBI survivors with persistent impairments, and exploring non-pharmacological treatments could be especially beneficial. Acupressure is a complementary and alternative medicine (CAM) treatment administered by applying pressure with the fingertips to acupoints, points on the skin designated as such by traditional Chinese medicine. Although there is some evidence that acupressure may enhance cognitive function (Clancy et al., 1996; Krebs and Brown, 1998), there is a dearth of controlled studies. Acupressure has been found to modify alertness in healthy medical professionals (Harris et al., 2005) and fatigue in patients with renal disease (Tsay, 2004), but there is little research on the effects of acupressure on cognitive function in general, and none in the English-language literature on the efficacy of acupressure for TBI. Acupressure could be a particularly useful treatment for TBI survivors because it can be taught to novice users and as such, can be used independently of funds, insurance, or a practitioner.
Although the mechanism by which acupressure affects the body remains unknown, there is evidence that it may modulate the autonomic nervous system (Felhendler and Lisander, 1999; McFadden and Hernández, 2010; Sugiura et al., 2007), and elicit the “relaxation response”, a physiological response that includes reduced respiration, heart rate, and blood pressure (Benson et al., 1974). A previous placebo-controlled, single-blind study in our laboratory in stroke survivors found active acupressure treatments to elicit a significantly faster and greater relaxation response than did placebo acupressure treatments (McFadden and Hernández, 2010). Other studies have found induction of the relaxation response to improve cognitive function through methods such as yoga (Subramanya and Telles, 2009) and meditation (Newberg et al., 2010; So and Orme-Johnson, 2001), although not all studies of yoga or meditation have shown significant improvement (Canter and Ernst, 2003; Oken et al., 2006). Additionally, Hanna–Pladdy and colleagues found induction of the relaxation response through a deep-breathing relaxation session to decrease cognitive complaints in individuals with mild TBI (Hanna–Pladdy et al., 2001).
The current study aims to determine whether acupressure treatments (specifically, Jin Shin acupressure [Burmeister, 1997; Mines, 1982, 2003]) affect cognitive sequelae following TBI. Specifically, a randomized, placebo-controlled, single-blind design was used to test the hypothesis that active acupressure treatments would confer greater improvement in cognitive function than would placebo acupressure treatments, as assessed by a neuropsychological test battery and event-related potentials (ERPs) during Stroop (Stroop, 1935) and auditory oddball tasks.
To our knowledge, there are no studies in the English-language literature that use ERPs to evaluate possible neural effects of acupressure. Indeed, the use of ERPs in the current study allows for a noninvasive neurophysiological measure of performance on cognitive tasks in real time (Spikman et al., 2004). The Stroop Color and Word Test (Stoelting Co., Wood Dale, IL, 1994), a measure of working memory (Lesak et al., 2004) and attention (Bohnen et al., 1992) was used in the current study as it is a common assessment for cognitive impairment in TBI (Bagiella et al., 2010; Bohnen et al., 1992; Marsh and Smith, 1995; Potter et al., 2002) and is sensitive to effects of TBI even in those with apparently good recovery (Bagiella et al., 2010). Oddball paradigms are commonly used clinically and experimentally with ERP recording to assess working memory and attention (Hruby and Marsalek, 2003; Polich, 2004) and have also been used to assess cognitive dysfunction in individuals with TBI (Potter and Barrett, 1999; Rugg et al., 1993; Sivak et al., 2008).
The current study used a multi-level approach to assess the effects of acupressure on cognitive function, employing a large range of self-report, behavioral, and neural measures. In addition to the neurophysiological measures using ERPs, the neuropsychological test battery included a multitude of tests that have been found to measure the following cognitive functions: working memory (digit span test), attention (digit symbol and digit span tasks [Lesak et al., 2004], and the Comprehensive Trail-Making Test [CTMT] [Dikmen et al., 1995; Lesak et al., 2004; Wang et al., 2007]), processing speed ([digit symbol test; Wang et al, 2007] and the CTMT [Dikmen et al., 1983, 1995]), tactual spatial problem solving (tactual performance test [Dikmen et al., 1983]), motor functioning and speed (the finger tapping test [Dikmen et al., 1983, 1995]), and health-related quality of life (Sickness Impact Profile [SIP] [Pagulayan et al., 2006]). Furthermore, state of being was assessed with the State Anxiety Inventory, the Center for Epidemiologic Studies Depression Scale (CES-D), the Perceived Stress Scale (PSS), and the UCLA Loneliness Scale, and physical activity and sleep were assessed with the Stanford Seven-Day Physical Activity Recall (7D-PAR) survey.
It was hypothesized that active acupressure treatments (eight treatments over 4 weeks) would improve cognitive function more than would placebo acupressure treatments in participants with mild-to-moderate TBI. In addition to increasing improvement on the neuropsychological test battery and state of being assessments, it was hypothesized that active acupressure would have a greater effect on ERP measurements than that seen with placebo treatments.
Methods
Participants
Participants aged 18–44 were recruited from the Denver/Boulder (Colorado) community via newspaper/newsletter advertisement and flyers. This age range was chosen because the lifetime cost of TBI is highest for individuals in this age range (Kraus and Chu, 2005); to reduce response heterogeneity in neuropsychological, neurophysiological, and physical function; and because it has been used previously in studies of TBI (Dikmen et al., 1983). Participants completed a series of eligibility questions in addition to the Brain Injury Screening Questionnaire (BISQ) (Research and Training Center, New York, NY) over the telephone to determine eligibility for the study. The BISQ has been shown to reliably distinguish between brain injury and other conditions (e.g., spinal cord injury) including the absence of disability (Cantor et al., 2004; Gordon et al., 2000). Participants eligible for the current study must have experienced a mild-to-moderate TBI at least 9 months and no more than 5 years prior to beginning the study, and be experiencing lasting deficits as a result of the injury, as assessed by the BISQ. Results of the BISQ must have been “positive” for brain injury, including the participant's experiencing symptoms common to brain injury, supporting that the symptoms resulted from the injury (e.g., difficulty learning new skills and new information, being easily distracted) (Gordon et al., 2000). Participants were only eligible if the BISQ determined that there was sufficient probability that current symptoms were a result of their self-reported history of TBI. As acupressure has not previously been investigated in survivors of TBI, the current study sought to recruit those with mild-to-moderate TBI rather than severe TBI, although there were no anticipated side effects based upon prior work (McFadden and Hernández, 2010). Eligibility criteria required participants to have experienced an alteration of consciousness, either through loss of consciousness or being dazed and confused following a blow to the head, but not to have experienced loss of consciousness for longer than 24 h, as per common guidelines for mild/moderate TBI classification (McCrea, 2008; Summers et al., 2009). Participants were deemed ineligible if they smoked, as this could impact cognitive function because of the cholinergic actions of nicotine (Ernst et al., 2001; Verbois et al., 2003). Additionally, participants were excluded if they were taking any drugs for recreational, psychiatric, or medical purposes (unrelated to the brain injury) or had had prior experience with acupressure. Participants gave informed consent and all aspects of the present study were in accordance with and approved by the University of Colorado Institutional Review Board.
Design
A randomized, placebo-controlled, single-blind design was used. The study involved three phases: pre-treatment assessment, acupressure treatments (active or placebo), and post-treatment assessment. After being stratified by gender, consented individuals were randomly assigned to receive active or placebo acupressure treatments; a random number generator was used to assign participants to condition in blocks of four. The acupressure practitioner was provided with a sealed envelope prior to each participant beginning their first treatment session, revealing the treatment she was to administer. As such, only the practitioner knew the type of treatment being administered. Acupressure treatments (40 min in duration) were administered twice per week for 4 weeks, for a total of eight treatments. Participants were blinded to which treatment condition they were assigned and all data collection, entry, and analyses were done by blinded individuals.
Phase one: Pre-treatment assessment
Participants first answered demographical questions, followed by an assessment of attitudes towards and use of complementary medicine using the Complementary, Alternative, and Conventional Medicine Attitudes Scale (CACMAS) (McFadden et al., 2010), and an assessment of past, present, and likely future use of 17 CAM modalities (McFadden et al., 2010). A modified version of the revised Life Orientation Test (LOT-R) (Scheier et al., 1994) was also administered. These questionnaires were used to measure baseline CAM usage, attitudes, and optimism among participants, to ensure that there were no differences between the active-treatment and placebo groups at baseline.
Questionnaires to assess state of being were administered during both pre- and post-treatment assessment sessions to explore treatment effects. These were the PSS (Cohen et al., 1983), the CES-D (Radloff, 1977), the State Anxiety Inventory (State portion of the State-Trait Anxiety Inventory [Mind Garden, Inc., Menlo Park, CA]) (Spielberger et al., 1970) and the UCLA Loneliness Scale (Version 3) (Russell, 1996). Physical activity and sleep levels in the week prior to testing were then assessed using a modified version of the 7D-PAR survey (Blair et al., 1985).
To assess cognitive function, participants next completed a battery of neuropsychological tests: the digit span and digit symbol subtests from the Wechsler Adult Intelligence Scale-Revised (WAIS-R) (Wechsler, 1981) and the CTMT (Reynolds, 2002), as well as the finger tapping test (Psychological Assessment Resources, Inc., Lutz, FL) and tactual performance test (Psychological Assessment Resources, Inc., Lutz, FL) from the Halstead–Reitan Neuropsychological Test Battery (Reitan, 1969). These are common tests previously and extensively used in the TBI literature (Dikmen et al., 1983, 1991, 1995, 2000; Temkin et al., 2007; Wang et al., 2007). Additionally, these tests allowed us to target a variety of neuropsychological constructs (e.g., working memory and attention, motor speed, spatial problem solving), while being sufficiently brief to not overburden participants when combined with additional measures. Health-related quality of life was assessed with the SIP (Gilson et al., 1975) and all measures were administered and scored according to standard methods from the literature.
Following the neuropsychological test battery, ERP data were recorded from 28 tin electrodes sewn into a stretch-lycra cap (Electro-Cap International, Eaton, OH), positioned according to the 10–20 international system (Jasper, 1958). Electrodes were also placed on the supra- and sub-orbit of the right eye to assess vertical eye movements, on the outer canthi of both eyes to assess horizontal eye movements, and over the left and right mastoid bones. Active scalp sites were referenced online to the left mastoid. Impedances were below 10 KΩ at all sites. ERP recordings were amplified with a gain of 500 using Neuroscan SynAmps amplifiers (Neuroscan, Inc., Sterling, VA), with a filter bandpass of 0.15–30 Hz and digitized at 1000 Hz. Offline, data were re-referenced to a computed average of the left and right mastoid bones and submitted to a regression procedure for correction of eyeblink artifact (Semlitsch et al., 1986). Epochs were created starting 100 ms prior to stimulus onset and lasting for 1000 ms following stimulus onset, and baseline corrected to the mean voltage of the pre-stimulus period. Each trial was visually inspected for remaining ocular or other artifact; any trials in which artifact was detected were deleted from further analyses (Kubota and Ito, 2007).
The Stroop Color and Word Test (Stoelting Co., Wood Dale, IL, 1994) was adapted for computer administration using PsyScope v. 1.2.5 (Cohen et al., 1993). Prior to beginning the task, participants were tested for color-blindness using Ishihara's Test for Color Deficiency (Kanehara Trading, Inc., Tokyo, Japan, 2007) and only completed the task if it was determined that they were able to distinguish between the colors used in the task. Responses during the task were made verbally, using a headphone/microphone set (Radioshack Optimus PRO 50MX Stereo Headphones, Fort Worth, TX) connected to the computer via button box to record response times. Before task onset, microphone sensitivity was tested by having participants read aloud days of the week presented in the center of the computer screen.
Participants first completed the 96 trials in the congruent block, in which words (“RED”, “BLUE”, or “GREEN”) were presented in the matching color (e.g., “RED” in red letters). Next, the 96 trials in the incongruent block were completed, in which words were presented in a non-matching color (e.g., “RED” presented in green letters). Participants were instructed to say aloud the color of the letters rather than reading the actual word. Lastly, participants completed the 96 trials in the neutral block, in which a row of four X's was presented in the center of the screen in red, blue, or green, and participants were asked to name aloud the color in which the X's were presented. Prior to each 96-trial block, participants completed a practice of 6 trials to ensure task comprehension. There was a 1500 ms inter-stimulus interval between word presentation (beginning when a response was made) and all words were presented on a black background in a dimly lit room for easy visibility. Participants were instructed to give all responses as quickly and accurately as possible and to avoid making any additional sounds so the microphone would not be triggered inappropriately. The task only advanced to the next trial after a response was made. Accuracy was recorded by a research assistant seated behind the participant.
A three-armed paradigm was used for the auditory oddball task (for review, see Polich, 2004), programmed with PsyScope Version 1.2.5 (Cohen et al., 1993). Participants were asked to discriminate between a frequently presented standard stimulus, an infrequently presented target stimulus (the “oddball”), and an infrequently presented non-target distracter stimulus (a white noise burst). They were instructed to respond by button press to only the target stimulus, and not to respond to the standard or distracter stimuli.
All participants reported normal hearing prior to this task. To ensure that participants were able to hear the tones presented during the task, a brief test was conducted in which participants indicated they could hear a 1000 Hz tone administered both at and below the level at which stimuli would be presented. Stimuli were created with SoundStudio3 (Freeverse, Brooklyn, NY) and presented at 75 dB SPL (measured by Radioshack Digital-Display Sound-Level Meter, Fort Worth, TX) using Optimus PRO 50MX Stereo Headphones. The target stimulus was a 1000 Hz tone and the standard stimulus was a 500 Hz tone, both presented for 70 ms (50 ms with 10 ms rise/fall time). The distracter stimulus used was a white noise burst, presented for 100 ms (80 ms with 10 ms rise/fall time), which was slightly longer than the tones to make it distinguishable as white noise. During the task, 400 stimuli were presented, consisting of the standard, target, and distracter stimuli with probabilities of 0.75, 0.125, and 0.125, respectively (300 trials, 50 trials, 50 trials). The 400 stimuli were presented in pseudorandom order, such that target or distracter stimuli were never presented consecutively (i.e., there was always at least one standard tone separating them). There was an inter-stimulus interval of 1300 ms between all stimuli.
Prior to beginning the task, participants listened to the three stimuli with the research assistant and were instructed to only respond to target stimuli. Following this, participants completed a practice of 30 stimuli and began the task after confirming they understood the procedure. After presentation of the first 200 stimuli, participants were given a chance to take a brief break before the remaining 200 stimuli, to help prevent drowsiness. Participants were notified of this break prior to task onset, and a message on the screen invited participants to rest briefly if desired and to push the button when ready to resume the task. To reduce eye movement, it was suggested that participants focus on a fixation point on the computer screen during the task.
Phase two: Acupressure treatments
Within a week after completing the pre-treatment assessment, participants began the acupressure treatment sessions. During treatment sessions, participants lay face up on a massage table, fully clothed with shoes removed, as is common practice for acupressure treatments (Burmeister, 1997; Mines, 1982). A Jin Shin (acupressure) practitioner, with over 20 years of clinical and educational experience and appropriate certification, administered treatments (active or placebo) behind a closed curtain. The practitioner was also trained in use of the placebo acupoints, which were established by T.D.H. (Hernández et al., 2003) and are points not found on established acupressure point charts. The placebo acupoints were each assigned a number and, using a random number generator, put into a matching sequence for each customary Jin Shin (acupressure) treatment.
During treatment, the practitioner applied pressure with her fingertips to different sites on the body, in sequence (for detail, see McFadden and Hernández, 2010). The entire treatment itself lasted 40 min. The placebo control procedure involved stimulation of the placebo acupoints and was designed to be indistinguishable from the active treatment session, to have the same duration, and to contain the same amount of physical contact. This placebo procedure has been used in previous studies in our laboratory (Hernández et al., 2003; McFadden and Hernández, 2010), and subjective credibility ratings made by participants following treatments have indicated that the placebo treatments were as credible as the active acupressure treatments (McFadden and Hernández, 2010). To guarantee matching practitioner/participant interactions for both treatment types, only scripted dialogue was used. Eight treatments were administered (twice weekly for 4 weeks) as our previous studies have found eight to be an optimal number to elicit treatment effects (McFadden and Hernández, 2010). A research assistant seated on the other side of the curtain was present during all treatment sessions to monitor the interaction between participants and the practitioner.
As has been done previously (McFadden and Hernández, 2010), expectancy was assessed (Myers et al., 2008) before treatments. To see if expectancy levels changed throughout the series of treatments, expectancy was assessed prior to treatments 1, 3 and 6. Participants also rated treatment credibility (Shapiro, 1981) immediately following treatments 2, 5, and 8.
Phase three: Post-treatment assessment
Approximately 48 h after their last acupressure treatment, participants completed the post-treatment assessment. This assessment consisted of the same measures as the pre-treatment assessment except for demographical measures, the CACMAS, CAM usage, and the modified LOT-R. ERP data were again recorded while participants completed the Stroop and auditory oddball tasks (see procedure described previously). As compensation for study participation, participants were offered a voluntary acupressure self-care class, held following study completion after all measures had been taken. In the self-care class, participants were given a self-care manual and taught, by the same practitioner who had administered the study treatments, to self-administer Jin Shin acupressure. This compensatory mechanism was offered to all participants, allowing even those who had been assigned to the placebo group the opportunity to experience treatments involving the active acupressure points.
Statistical analyses
Data were analyzed using SPSS 17.0 (SPSS Inc., Chicago, IL). State of being, physical activity, neuropsychological test battery, and SIP data were analyzed using t-tests to assess differences within groups (simple pre- to post-treatment changes in active-treatment and placebo groups, using paired t-tests) as well as the differences between those group changes (active vs. placebo, using independent samples t-tests). Cohen's d was found for t-tests using G*Power Version 3.2.1 (Faul et al., 2007). A composite score was created for the neuropsychological test battery, by ranking the change scores for each participant from least to most improved on each test, then obtaining a mean rank across the tests (similar to Dikmen et al., 2000). Group differences in composite change scores were analyzed using an independent samples t-test. Expectancy and credibility data were analyzed using repeated measures analysis of variance (ANOVA), given that the questionnaires were administered multiple times throughout the experiment. Behavioral data from the Stroop and auditory oddball tasks (reaction time and accuracy) were also analyzed using repeated measures ANOVA, to assess main effects of group (placebo or active), stimulus (Stroop: congruent vs. incongruent vs. neutral; auditory oddball: target vs. standard vs. distracter), and session (pre- vs. post-treatment), as well as any interactions among variables, using the Greenhouse–Geisser correction. Potential confounding variables (age, gender, time since injury, number of injuries, number of TBI-sensitive symptoms reported on the BISQ, expectancy levels, and credibility levels) were controlled by adding them into the model using analysis of covariance (ANCOVA).
In the Stroop and auditory oddball tasks, we quantified the P300 ERP component because of its association with working memory (Kok, 2001; Polich, 2004; Spikman et al., 2004) and because it is commonly investigated in these tasks (Hruby and Marsalek, 2003; Ilan and Polich, 2001; Polich, 2004). P300 amplitude is thought to reflect the degree of working memory engagement, and latency to reflect the speed with which working memory operations occur (Hruby and Marsalek, 2003; Polich, 2004). The P300 component was defined as the largest positive-going deflection within 250–400 ms post-stimulus onset in both the Stroop and auditory oddball tasks. Additionally, for the Stroop task, we quantified two components associated with cognitive control: N2 and N450 components were quantified because they have been consistently investigated in Stroop tasks and are thought to reflect cognitive control processes (Larson et al., 2009; Vanderhasselt and De Raedt, 2009). The N2 component was defined as the largest negative-going deflection within 200–300 ms post-stimulus onset, with the N450 component being the largest negative-going deflection within 400–500 ms post-stimulus onset. Before these peaks were quantified, data were filtered offline with a 9 Hz low-pass zero-phase filter. Peak latency for all components was measured from the time of stimulus onset, with amplitude measured relative to pre-stimulus baseline. Grand average ERP waveforms were created for active-treatment and placebo groups by session (pre- or post-treatment assessment) and stimulus type for each task (Stroop and auditory oddball).
ERP latency and amplitude were analyzed using repeated measures ANOVA to assess main effects of group (active vs. placebo), stimulus (Stroop: congruent vs. incongruent vs. neutral; auditory oddball: target vs. standard vs. distracter), and session (pre- vs. post-treatment), as well as any interactions among variables, using the Greenhouse-Geisser correction. Potential confounding variables (age, gender, time since injury, number of injuries, number of TBI-sensitive symptoms reported on the BISQ, expectancy levels, and credibility levels) were controlled by adding them into the model using ANCOVA.
Results
Participants
Many screened for participation were ineligible for such reasons as length of time since brain injury, age, or having no lasting TBI-related sequelae, among others (see Fig. 1). Of the 42 participants completing the study, 21 were randomly assigned to active acupressure treatments, whereas the other 21 were randomly assigned to placebo acupressure treatments. Eleven participants completed all aspects of the study except for the ERP testing, because of initiation of neuropsychological data acquisition preceding ERP data acquisition for seven participants (four active, three placebo) and four participants declining to take part in the ERP portion of the study (one active, three placebo). Seven participants were excluded from analyses for various reasons (see Fig.1), resulting in analyses for 21 participants in the active-treatment group and 17 participants in the placebo group for the state of being, physical activity, neuropsychological test battery and SIP analyses, with 14 participants in the active-treatment group and 10 participants in the placebo group for the ERP analyses. All exclusions were made in a blinded fashion, prior to data analyses, and groups were not significantly different on demographical measures following exclusions.

Participant flow through study.
There were no significant differences between the active-treatment and placebo groups in any of the demographical information collected (Table 1), p > 0.05. Additionally, there were no significant differences between groups in terms of reported cause of injury (e.g., equal numbers reported because of motor vehicle accident, sports, etc.). Furthermore, there were no significant differences between the active-treatment and placebo groups on the modified LOT-R, the CACMAS, or in past, present, or probable future use of CAM (Table 1), p > 0.05. Importantly, there were no significant main effects of treatment type on expectancy ratings (p > 0.05) or credibility ratings (p > 0.05), indicating that participants in both groups were equally expectant prior to treatments and also judged treatments to be equally credible. Interestingly, there was a significant linear effect of time on credibility rating, such that credibility rating increased with each administration of the credibility questionnaire, and this was equally so for both active-treatment and placebo groups [F (2, 72) = 5.07, p = 0.010, partial η2 = 0.12]. There was no effect of time on expectancy rating (p > 0.05).
Mean ± SEM unless otherwise indicated.
LOC, loss of consciousness (note: all were unconscious for <24 h); BISQ, Brain Injury Screening Questionnaire; TBI, traumatic brain injury; CACMAS, Complementary, Alternative and Conventional Medicine Attitudes Scale (mean score on a scale of 1–7, with 1 = strongly disagree to 7 = strongly agree); CAM (complementary and alternative medicine) usage out of 17 listed types; LOT-R, modified version of the revised Life Orientation Test (sum, with a minimum possible score of 0 [least optimistic] to 42 [most optimistic]).
Expectancy rating: mean score on a scale of 1–9, with 1 = least expectant to 9 = most expectant; Credibility rating: mean score on a scale of 1–9, with 1 = least credible to 9 = most credible.
State of being and physical activity
There was a marginally significant treatment effect on the PSS, such that those in the active-treatment group indicated a larger reduction in subjective stress levels post-treatment than did those in the placebo group [t (36) = 1.88, p = 0.069, Cohen's d = 0.59]. Also, although the active-treatment group had a significantly lower score on the CES-D from pre- to post-treatment, the placebo group only showed a marginally significant reduction in CES-D score from pre- to post-treatment (Table 2). However, this change from pre- to post-treatment was not significantly different between groups. There were also no significant group differences between pre- to post-treatment changes in score on the State Anxiety Inventory or the UCLA Loneliness Scale, or on physical activity levels and average amount of sleep as measured by the 7D-PAR, p > 0.05 (Table 2).
For all measures mean ± SEM.
The first two p value columns reflect change from pre- to post-treatment within each group (active and placebo), whereas the last column reflects the difference in change (pre- to post-treatment) between groups (group difference: active vs. placebo).
p < 0.001, †p < 0.01, ‡p < 0.05, ∫p < 0.08.
Perceived Stress Scale: sum, with a minimum possible score of 0 (never stressed) and maximum possible score of 56 (often stressed); CES-D, Center for Epidemiologic Studies Depression Scale: mean score, with 0 = least depression and 60 = most depression; State Anxiety Inventory: mean score on a scale of 1-4, with 1 = not at all anxious to 4 = very anxious; UCLA Loneliness Scale: sum, with a minimum possible score of 20 (never lonely) and a maximum possible score of 80 (often lonely); 7D-PAR, Seven-Day Physical Activity Recall survey, average estimated h of sleep and total estimated h of moderate, hard, and very hard physical activity in the past 7 days; Digit span: sum of maximum number recalled correctly in digits forward plus maximum recalled correctly in digits backward (17 possible); Digit symbol: number completed correctly (93 possible); CTMT, Comprehensive Trail-Making Test: composite index score; Finger tapping test: mean number of taps in 10 sec using dominant hand; Tactual performance test: total min to complete test; SIP, Sickness Impact Profile: sickness score from 0 to 100.
Neuropsychological test battery and health-related quality of life
Those in the active acupressure group significantly improved from pre- to post-treatment on the digit span test (measured as the sum of the maximum number recalled in digits forward plus maximum recalled in digits backward) compared to those in the placebo group: t (36) = 2.09, p = 0.043, Cohen's d = 0.68 (Table 2). This effect could not be accounted for by age, gender, time since injury, number of injuries, number of TBI-sensitive symptoms reported on the BISQ, expectancy levels, or credibility levels. Whereas scores in both groups significantly improved from pre- to post-treatment assessment, there were no significant differences in improvement between the active-treatment and placebo acupressure groups on the digit symbol test, the CTMT, the finger tapping test, the tactual performance test, or the SIP (p > 0.05). However, there was a marginally significant effect seen in the neuropsychological test battery composite score, such that the active-treatment group improved overall more than the placebo group [t (36) = 1.85, p = 0.073, Cohen's d = 0.59].
Stroop task
Data for the P300 component are reported at the Pz electrode, as analyses revealed that to be the electrode at which the greatest amplitude was found. Amplitude was greatest at the FCz electrode for the N450 component and at the Fz electrode for the N2 component, therefore data were analyzed accordingly at those electrodes. These scalp distributions are consistent with previous research (Ilan and Polich, 2001; Larson et al., 2009; Vanderhasselt and De Raedt, 2009).
ERP data showed a significant session (pre- or post-treatment) by treatment group (active or placebo) interaction in the Stroop task, such that those in the active-treatment group demonstrated a reduction in P300 amplitude and latency overall compared to those in the placebo group: F (1, 22) = 7.90, p = 0.010, partial η2 = 0.26 and F (1,22) = 7.74, p = 0.011, partial η2 = 0.26, respectively (Fig. 2). These effects could not be accounted for by age, gender, time since injury, number of injuries, number of TBI-sensitive symptoms reported on the BISQ, expectancy levels, or credibility levels. To further explore this interaction, simple effects of the pre- to post-treatment change for each group (active and placebo) were investigated separately for each stimulus type (congruent, incongruent, and neutral) using paired t-tests. These analyses found that the active-treatment group showed a significant reduction in P300 amplitude from pre- to post-treatment for both incongruent [t (13) = 4.66, p < 0.001, Cohen's d = 1.25] and neutral [t (13) = 4.83, p < 0.001, Cohen's d = 1.29] stimuli, and showed a marginally significant reduction in amplitude for congruent stimuli [t (13) = 1.905, p = 0.079, Cohen's d = 0.51], whereas the placebo group did not show any significant change in P300 amplitude from pre- to post-treatment, p > 0.05 (Table 3). However, the placebo group showed a significantly longer P300 latency post-treatment compared to pre-treatment during both incongruent [t (9) = −3.29, p = 0.009, Cohen's d = 1.06] and neutral [t (9) = − 3.30, p = 0.009, Cohen's d = 1.05] trials. Latency in the placebo group post-treatment was also longer, but not significantly, during congruent trials (p > 0.05). Whereas the active-treatment group showed a shorter P300 latency overall post-treatment compared to pre-treatment, this was not significant for any of the stimuli (congruent, incongruent, or neutral), p > 0.05. There were no significant treatment effects found among the N2 or N450 components (p > 0.05).
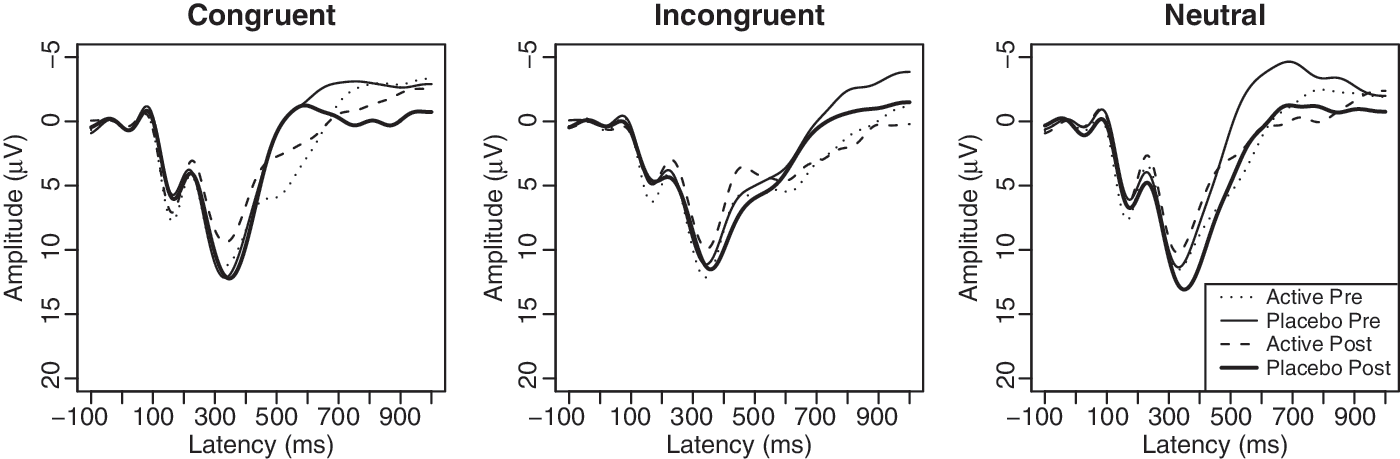
Grand average ERP waveforms at Pz during the Stroop Color and Word Test. ERP, event-related potentials.
Difference in change from pre- to post-treatment within each group (active and placebo).
p < 0.001, †p < 0.01, ‡p < 0.08.
Looking at reaction times during the Stroop task, a significant main effect of stimulus was found [F (2, 44) = 158.68, p < 0.001, partial η2 = 0.88]. Reaction times were significantly different among all three stimuli, such that both active-treatment and placebo groups had longer reaction latencies to incongruent stimuli than to both congruent and neutral stimuli, and longer reaction latencies to neutral stimuli than to congruent stimuli (Table 4). However, there were no significant effects of session (pre- or post-treatment) or treatment group (active or placebo), p > 0.05.
Difference in change from pre- to post-treatment within each group (active and placebo).
p < .08.
RT, reaction time.
There were significant main effects of session [F (1, 22) = 4.73, p = 0.041, partial η2 = 0.18] and stimulus [F (2, 44) = 19.66, p < 0.001, partial η2 = 0.47] on accuracy during the Stroop task. This was such that across treatment group and stimulus type, participants were more accurate during the pre-treatment assessment than during the post-treatment assessment. Also, across treatment group and session (pre- or post-treatment), participants were correct on fewer trials during the incongruent block than during either the congruent or neutral blocks (Table 4).
There was also a significant interaction among treatment group, stimulus type, and session [F (2, 44) = 5.89, p = 0.008, partial η2 = 0.21]. To explain this interaction, analyses were broken down to investigate how the Stroop effect changed from pre- to post-treatment for each group. The premise of the Stroop effect is that incongruent trials will prove more difficult than congruent or neutral trials, because the automatic reading response interferes with naming the incongruent ink color (Bohnen et al., 1992; Potter et al., 2002). To investigate this, difference scores were calculated for incongruent vs. congruent accuracy as well as for incongruent vs. neutral accuracy, for both pre- and post-treatment sessions (Table 5). There were no significant differences between active-treatment and placebo groups in the incongruent/congruent Stroop effect or the incongruent/neutral Stroop effect pre-treatment (p > 0.05). However, after the treatment series, the active-treatment group demonstrated a reduction in the incongruent/congruent Stroop effect that was not seen in the placebo group [t (22) = 3.20, p = 0.004, Cohen's d = 1.27], i.e., there was an active treatment-associated reduction in interference during the task. There was also a significant treatment effect seen in the incongruent/neutral Stroop effect, such that the active-treatment group again showed a reduced Stroop effect from pre- to post-treatment compared to the placebo group [t (22) = 2.35, p = 0.028, Cohen's d = 0.96]. To further explore this, the simple effects of the change from pre- to post-treatment in both groups were tested using paired t-tests. In the incongruent/congruent comparison, the active-treatment group showed a marginally significant reduction in interference from pre- to post-treatment [t (13) = 2.01, p = 0.066, Cohen's d = 0.54]. However, in the same comparison, the placebo group showed a significant increase in interference from pre- to post-treatment [t (9) = 2.29, p = 0.048, Cohen's d = 0.72]. The simple effects for the incongruent/neutral comparisons were not significant for either group (p > 0.05).
Difference in change from pre- to post-treatment within each group (active and placebo).
p < 0.05, †p < 0.08.
Auditory oddball task
During an oddball task, it is expected that both the target and distracter stimuli will elicit a P300 component, which will not be apparent in reaction to the standard stimuli (Polich, 2004). A classic oddball effect was seen during this task: there was a significant main effect of stimulus, such that P300 amplitude was increased for both the target (oddball) and the distracter (white noise) compared to the standard tone [F (2,44) = 56.61, p < 0.001, partial η2 = 0.72]. There was also a significant main effect of stimulus for P300 latency, such that participants demonstrated decreased latency to the distracter (white noise) compared to the standard and target tones, perhaps because of the salience of the stimulus: F (2,44) = 11.02, p = 0.002, partial η2 = 0.33 (Fig. 3). There were no significant effects of treatment group, nor were there any interactions between treatment group and stimulus or session (p > 0.05). Similarly, there were no significant differences in reaction time or accuracy in responses to oddball stimuli from pre- to post-treatment assessment in either group (p > 0.05). Although there were no significant treatment effects, there was a significant main effect of stimulus when one looked at the percentage of false positive responses (button press to either standard or distracter stimuli), such that participants made more false positive responses to distracter stimuli than to standard stimuli [F (1, 22) = 18.03, p < 0.001, partial η2 = 0.45], again perhaps because of stimulus salience (Table 6).
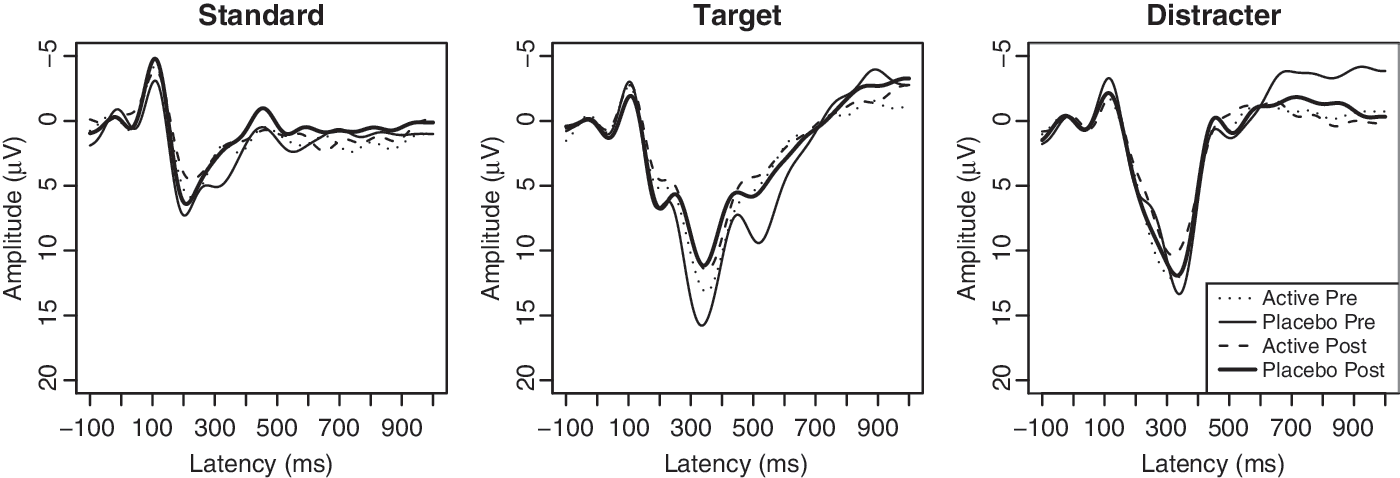
Grand average ERP waveforms at Pz during the auditory oddball task. ERP, event-related potentials.
Difference in change from pre- to post-treatment within each group (active and placebo): all ns.
Discussion
Significant treatment effects were found in the Stroop task, such that those in the active acupressure group demonstrated a reduction in both P300 latency and amplitude compared to those in the placebo acupressure group. The P300 component is thought to be a measure of working memory and selective attention (Hruby and Marsalek, 2003; Polich, 2004; Spikman et al., 2004). Specifically, P300 latency is said to reflect the speed of cognitive processing in working memory and P300 amplitude is hypothesized to represent the allocation of cognitive resources (Hruby and Marsalek, 2003; Kok, 2001; Polich, 2004). Whereas there can be different interpretations of P300 amplitude reduction (Ilan and Polich, 2001; Kok, 2001), given that we also saw reduced P300 latency in the active-treatment group, albeit not to a statistically significant degree, we interpret these findings as an indication of reduced neural resources allocated to task completion, possibly suggesting an improvement in cognitive function. In support of this, recovery following TBI has also been associated with decreased demand for the additional “neural recruitment” identified via neuroimaging during working memory tasks following TBI (Hillary et al. 2010; Nakamura et al., 2009).
Interestingly, while the active-treatment group showed a significant reduction in P300 amplitude during the Stroop task that was not seen in the placebo group, the placebo group did show a significant change in latency from pre- to post-treatment. Whereas the active-treatment group demonstrated a reduction in latency (although it was not significant), the placebo group showed a significantly increased latency post-treatment compared to pre-treatment, in both the incongruent and neutral stimuli. Given that the placebo group did not show any detrimental effects of treatment on other measures, and in fact improved on many measures (CES-D, digit symbol, CTMT, finger tapping test, tactual performance test, SIP), it is possible that this increase in latency could be fatigue-driven rather than a result of the placebo intervention itself. Fatigue is common following TBI (Arciniegas and Silver, 2006; Riggio and Wong, 2009) and the ERP measures were the last measures to be taken during the assessment sessions, which lasted 2–3 h. As such, it could be that the increase in latency reflects increased fatigue due to this being the last session in the series of study sessions and the ERP being among the last measures in that session. As the active-treatment group did not show this increase in latency, it could be that the active treatments acted as a “buffer” of sorts against the fatigue experienced during testing. This is consistent with previous studies in the literature that have suggested efficacy of acupressure for reducing fatigue (Tsay, 2004) and increasing alertness (Harris et al., 2005). Future studies will include measures of fatigue to specifically test for this.
It was also found that when looking at accuracy during the Stroop task, the active-treatment group demonstrated a marginally significant reduction in interference after the treatment series that was not seen in the placebo group, suggesting treatment-associated improvement on the task even though there were no group differences in reaction time during the task. This reduced Stroop effect, in which there was less of a discrepancy between the more difficult incongruent trials and the easier congruent and neutral trials, suggests that the active acupressure treatments may have improved selective attention (Ilan and Polich, 2001). Together with the ERP data, it appears that whereas both groups were able to successfully complete the task, the active-treatment group may have required less processing time and fewer neural resources post-treatment than did the placebo group, suggesting an increase in function of working memory and attention. However, in addition to the active-treatment group showing a reduction in interference, the placebo group demonstrated an increase in interference during the Stroop task. As with the increase in P300 latency seen in the placebo group post-treatment, this could reflect increased TBI-associated fatigue that was buffered by the active acupressure treatments. One limitation of the accuracy data, however, is that the lowest score was 94% correct. As such, there was little room for improvement from pre- to post-treatment. Interestingly, even with this apparent ceiling effect, the active-treatment group still demonstrated improvements compared to the placebo group. Future studies can include a more difficult task to further investigate the effects of active acupressure on both improved performance and fatigue reduction.
A classic oddball effect was seen in both groups in the auditory oddball task, such that the P300 component was elicited to the target and distracter stimuli, but not to the standard stimuli. However, no significant treatment effects were found. One possible reason for this could be that the task was too easy for participants, as the oddball tone (1000 Hz) was easily distinguishable from the standard tone (500 Hz) (Katayama and Polich, 1998). Future studies can use a more difficult task (e.g., 950 Hz compared to 1000 Hz) to determine if there might be any treatment effects.
A significant treatment effect was found in the digit span test, such that participants in the active-treatment group improved compared to those in the placebo group. This is particularly interesting given the observed treatment-associated improvement on the Stroop task, as both tasks are measures of working memory and attention (Bohnen et al., 1992; Lesak et al., 2004). Although the improvements seen in the active-treatment group were significantly greater than those seen in the placebo group, the clinical relevance of a one-point increase on the digit span task is worth discussing. Given that improvements were seen in multiple measures of working memory, and that we found moderate-to-large effect sizes, we believe that these results are clinically significant. Working memory dysfunction is a commonly cited problem following TBI (Arciniegas and Silver, 2006; Dikmen et al., 2009; Eslinger et al., 2007), and improvements (even if seemingly numerically small) in working memory would be applicable to many real-life situations, such as remembering telephone numbers, grocery lists, and appointments. Future studies could explore the real-life consequences of working memory improvement in TBI survivors following acupressure treatments by incorporating measures such as academic or work performance, or following verbal directions to a geographical location.
Although there were no significant treatment effects seen in the other tests given in the neuropsychological test battery, when looking at them together using a composite score, a marginally significant treatment effect was found: those in the active-treatment group improved more on the neuropsychological test battery overall than did those in the placebo group, also suggesting enhanced cognitive function following active treatments. That the active-treatment group improved more than the placebo group also suggests that this enhanced performance was a result of more than simply practice effects. Indeed, the active treatment-associated neural response seen during the Stroop task could be the mechanism underlying the functional improvement.
Those in the active-treatment group also reported a marginally significant reduction in subjective stress rating compared to those in the placebo group, as measured with the PSS. This reduction in subjective stress could be the result of an increased relaxation response experienced by the active-treatment group. Following TBI, individuals may be particularly sensitive to anxiety and stress (Bryant et al., 2010; Gouvier et al., 1992; Hanna–Pladdy et al., 2001), which can exacerbate or unmask cognitive deficits (Ewing et al., 1980; Hanna–Pladdy et al., 2001). As such, a treatment that reduces stress and increases the relaxation response could be particularly beneficial to those experiencing cognitive impairments resulting from TBI. Furthermore, given that 86% of participants in the current study were college students, a population that often experiences high levels of stress (Tosevski et al., 2010), stress reduction would be particularly beneficial in this group with co-occurring TBI. Pilot data from a subset of TBI survivors in the present study showed that, similar to our prior study in stroke survivors (McFadden and Hernández, 2010), there was a greater and faster reduction in heart rate during active treatments compared to during placebo treatments, although this difference was not statistically significant (unpublished data, available upon request). Future studies will include this measure to ascertain if the significant effects of acupressure on heart rate are replicated in a population other than stroke survivors.
There were no significant differences between the active-treatment and placebo groups in expectancy levels. This is important, as expectancy has been shown to influence treatment outcome (Price et al., 2008; Shapiro, 1981). Furthermore, there were no significant differences between the credibility ratings the participants in the active-treatment and placebo groups gave the treatments, which is important to establish that the placebo treatment was as credible as the active treatment. This suggests that participants were unaware of which treatment group they were in during the study. Interestingly, a questionnaire administered at the end of the study (after all data collection was complete) revealed that whereas only 42.9% of participants in the active group correctly guessed which type of treatment they had received, 70.6% of those in the placebo group guessed correctly, but this was not statistically significant. It seems that this group difference only appeared after study completion, when participants were asked to retrospectively look back on the treatments as a whole, after the post-treatment assessment measures had been taken.
In a study of CAM, it is also necessary to establish that the participants in the placebo and active-treatment groups are not different in their attitudes toward and usage of CAM, as this could influence their receptivity to the treatments they receive during the study. Importantly, there were no baseline differences between the active-treatment and placebo groups in their attitudes toward conventional and complementary medicine, or in the number of types of CAM they had used in the past, were currently using, or would be open to use in the future. The two groups also did not differ in their baseline level of optimism, which could affect treatment expectations and treatment effects (Scheier and Carver, 1992).
A potential limitation of the current study is that TBI status was determined using self-report rather than medical records or neuroimaging methods. However, given the stringent inclusion criteria and the reliability of the BISQ screening tool in identifying brain injury (Cantor et al., 2004; Gordon et al., 2000), as well as the inability of some common imaging methods to identify mild TBI (Belanger et al., 2007), the current study sample should be representative of mild TBI survivors. As participants were not recruited from a medical center, but from the general population, future studies could involve participants with recently clinically diagnosed TBI recruited from a medical setting. Another potential limitation is that the current study focused on acute benefits of acupressure treatment, as post-treatment measures were taken approximately 48 h after the last treatment administration. Although significant treatment effects were found, the enduring nature and long-term clinical relevance of these effects remains to be determined. Future studies will assess enduring benefits of acupressure treatments, as well as whether the statistically significant enhancement of the relaxation response is replicable in additional populations.
In conclusion, acupressure may confer a functional benefit in TBI survivors above and beyond that seen with placebo acupressure, specifically by improving cognitive, neurophysiological, and neuropsychological function. To our knowledge, this is the first controlled study of acupressure to show functional improvement following TBI. The mechanism underlying this improvement remains unknown, but could be the result of an increased relaxation response, which has been suggested to break the stress–disease link (Esch et al., 2003). Given the adverse consequences of stress following TBI, it is valuable to show that an enhanced relaxation response in this population can lead to a reduction in stress as well as to cognitive benefit. Additionally, since it is highly accessible, can be taught to the novice individual, and has no apparent side effects, acupressure warrants further study as an adjunct treatment following TBI.
Footnotes
Acknowledgments
We thank Jin Shin (acupressure) practitioners Christine Palafox, B.A., C.M.T., N.C.T.M.B. and Tara Dempsey, B.A., and all study participants. We also thank professional research assistant Kate Hoversten, B.A. for help with data collection; undergraduate research assistants D. Frank Distel and Samantha Kile for help with data acquisition/entry; undergraduate research assistant Nathan Faes for help with data entry; and professional research assistant Jessica Sannan, B.S. and departmental information technology specialist Jon Roberts, M.A. for technical support. This work was supported by funding from the Colorado Traumatic Brain Injury Trust Fund.
Author Disclosure Statement
No competing financial interests exist.