
Abstract
An autoregulation-oriented strategy has been proposed to guide neurocritical therapy toward the optimal cerebral perfusion pressure (CPPOPT). The influence of ventilation changes is, however, unclear. We sought to find out whether short-term moderate hypocapnia (HC) shifts the CPPOPT or affects its detection. Thirty patients with traumatic brain injury (TBI), who required sedation and mechanical ventilation, were studied during 20 min of normocapnia (5.1±0.4 kPa) and 30 min of moderate HC (4.4±3.0 kPa). Monitoring included bilateral transcranial Doppler of the middle cerebral arteries (MCA), invasive arterial blood pressure (ABP), and intracranial pressure (ICP). Mx -autoregulatory index provided a measure for the CPP responsiveness of MCA flow velocity. CPPOPT was assessed as the CPP at which autoregulation (Mx) was working with the maximal efficiency.
During normocapnia, CPPOPT (left: 80.65±6.18; right: 79.11±5.84 mm Hg) was detectable in 12 of 30 patients. Moderate HC did not shift this CPPOPT but enabled its detection in another 17 patients (CPPOPT left: 83.94±14.82; right: 85.28±14.73 mm Hg). The detection of CPPOPT was achieved via significantly improved Mx-autoregulatory index and an increase of CPP mean. It appeared that short-term moderate HC augmented the detection of an optimum CPP, and may therefore usefully support CPP-guided therapy in patients with TBI.
Introduction
I
Methods
The analysis was performed on data collected from 30 patients with TBI (39.0±14.1 y) with Glasgow Coma Score <12, analgosedated with propofol and fentanyl, and mechanically ventilated. Approval for monitoring and analysis was given by our local ethical committee. Inclusion criterion was a normocapnic baseline with CPP >70 mm Hg and end-tidal CO2 (ETCO2) of >35 mm Hg (4.7 kPa). Exclusion criteria were respiratory failure and being in the early phase of TBI, to avoid the risk of ischemia caused by a hypocapnic change of cerebral blood flow, which may be critically reduced for up to 48 h after TBI (Sioutos et al., 1995).
The monitoring included: • Radial artery blood pressure (ABP; Edwards Lifesciences, Irvine, CA) • Intraparenchymal ICP (Codman MicroSensors ICP Transducer, Codman & Shurtle, Raynham, MA) • Mainstream ETCO2 (Marquette Solar 8000M, GE Medical Systems, United States) • Arterial CO2 partial pressure (PaCO2) using an AVL Omni blood gas analyser (AVL Omni, Graz, Austria) • Flow velocity (FV) assessed using a head band with transcranial Doppler probes insonating the middle cerebral arteries (MCA) bilaterally at a depth of 51–53 mm.
Following a 20-min recording of baseline data at constant ETCO2, the minute volume of the ventilator was increased by 15 to 20% and was kept stable for another 30 min of moderate HC. If this intervention resulted in the violation of standard treatment guidelines, the protocol was abandoned. Care was taken not to deceed limits of PaCO2<3.5 kPa and/or jugular bulb oxygen saturation (SJO2)<55%. The analgosedation was kept unchanged during baseline and HC.
Analog signals were sampled at 30 Hz and digitized using waveform time integration. Averaged 6-sec values for ICP, ABP, CPP, FV, and respiratory rate were calculated and stored continuously on a computer. Data analysis was performed using ICM+ software (Cambridge University, Cambridge, England). Autoregulation was assessed continuously using the Mx-autoregulatory index (Mx) which was calculated as the moving correlation coefficient between consecutive 24 samples of 10-sec averages of FV and CPP waveforms. Mx principally may vary between −1 and +1. Previous studies, based on analysis of outcome from a large cohort of TBI patients have shown Mx ≤0.25 if autoregulation is intact, whereas disturbed autoregulation is reflected by values > 0.25, as reported by Czosnyka and associates (1996). Hence, increasing Mx signifies worsening autoregulation whereas decreasing Mx indicates improving autoregulation. This method for autoregulation testing has been validated against others (Reinhard et al., 2004).
For the determination of the optimum CPP in each patient, CPP was plotted against Mx-values over the periods of baseline and moderate HC separately. The relationship between Mx and CPP was assessed using a second degree polynomial regression analysis. CPPOPT – CPP value at the Mx minimum was determined if CPP and Mx showed a significant U-shaped correlation (p<0.05). For the comparison between baseline and moderate HC as well as between patient subgroups, we applied the mixed between-within subjects ANOVA of the multiple interdependencies between Mx-autoregulatory index, baseline ICP, CPP, CPPOPT, FV, ABP, and CO2 using SPSS 17.0 analysis. In addition, a Student's t-test for paired samples of CPPOPT at baseline and HC was performed. The homogeneity of variances of CPPOPT between baseline and HC was evaluated using Bartlett's test. Statistical significance was set at p<0.05.
Results
Baseline ICP of 30 patients included in this analysis ranged from 5.2 to 27.6 mm Hg. Patients were studied 72±12 h after TBI at baseline PaCO2 of (5.02±0.35kPa) and moderate HC of (4.25±0.33kPa). In response to HC, ICP and FV dropped significantly from baseline whereas CPP was slightly increased (Table 1).
ICP, intracranial pressure; ABP, arterial pressure; Fv-MCA, flow velocity; Mx, Mx autoregulatory index; CPP, cerebral perfusion pressure; CPPOPT, optimal CPP; R2 (CPP/ Mx), correlation coefficient for second order polynomial regression.
All values given as mean±standard deviation.
Differences between baseline and HC: # p<0.05; ## p<0.01 as well as between patients maintaining and patients establishing CPPOPT, **p<0.01.
Effects on Mx-autoregulatory index seemed to depend upon normocapnic baseline values of Mx (left -MCA: r2 =0.74; right MCA: r2 =0.78, p<0.01; Fig. 1B). Patients with impaired Mx autoregulation (left: 0.33±0.149; right: 0.37±0.24) seemed to have improved significantly (left: 0.06±0.27; right: −0.001±0.17, p<0.001) whereas those with normal Mx baseline (left: −0.26±0.24; right: −0.27±0.23, p<0.05) did not significantly change (Fig.1B).

(
The U-shaped relationship between Mx-indices and CPP values was found in 12 patients at baseline and in 29 patients during moderate HC. Moreover, Mx indicated a significantly better autoregulatory function in those with a detectable baseline CPPOPT (Table 1).
Moderate HC was found to have either maintained or established this U-shaped CPP–Mx relationship (examples in Fig. 2A–F). In patients maintaining this relationship, Bartlett's test indicated homogenous variances of CPPOPT at baseline and HC. There were no significant differences between CPPOPT during moderate HC and normocapnic baseline (examples: Fig. 2A,D; Table 1). In 17 patients, CPPOPT was established via moderate HC. This was related to an increased CPP mean (example: Fig. 2C,F) and/or improved Mx-indices (example: Fig. B,E). One patient, however, did not establish a U-shaped relationship between CPP and Mx during moderate HC, which seemed to have been associated with an unstable ABP and caused hypocapnic CPP to fall below its normocapnic baseline (normocapnia: 76.25±0.69; moderate HC: 70.58±1.45 mm Hg).
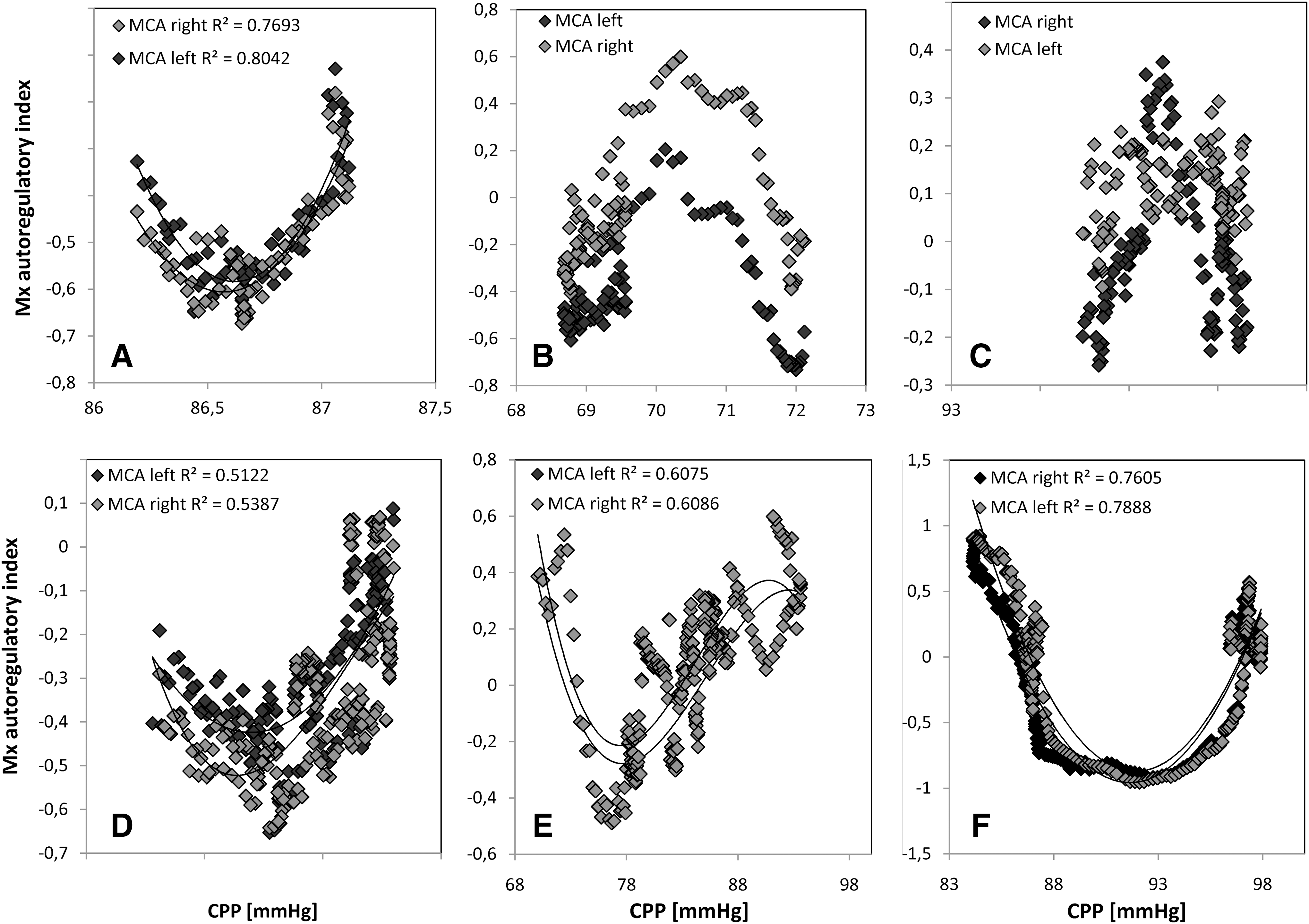
CPP–Mx relationship at baseline (top row) and moderate HC (bottom row). Examples for patients maintaining
Discussion
This study analyzed the optimal CPP during normocapnia and brief moderate HC on the basis of Mx-autoregulatory indices. The method is based on earlier results averaged from 187 patients with TBI (Czosnyka et al., 2001) having shown that: 1) Mx reacts dynamically to changes in perfusion pressure; 2) The relationship between Mx (autoregulation assessed continuously using transcranial Doppler ultrasonography) and CPP followed a U-shape curve indicating that inadequately low CPP and excessively high CPP are both associated with autoregulatory failure; and 3) The curve converged toward a minimal Mx, which marked the CPP at the best achievable state of autoregulation.
Our current analysis has focused on the individual CPPOPT in 30 patients with TBI. In 18 out of these patients, however, baseline monitoring of Mx and CPP did not enable determination of the CPPOPT. Would periods >20 min baseline have to be monitored in order to detect the CPPOPT? Although we cannot exclude that, for example, a 30-min baseline monitoring would have enabled detection of CPPOPT in a larger number of patients, this assumption seems to be unlikely when compared with the literature. Steiner and associates (2002) showed that in 40% of patients with TBI, CPPOPT may not be detectable even during long-term monitoring. Authors therefore recommended either prolonging the monitoring period, or titrating the CPP around an estimated optimum via pharmacological blood pressure manipulation.
Results of our study showed that moderate HC has enabled detection of the CPPOPT in a larger number of patients, and suggest that short-term moderate HC may offer an effective alternative for detecting the CPPOPT within minutes rather than hours. Moreover, the accelerated detection of CPPOPT would be a prerequisite for detecting changes of CPPOPT, especially in the early phase after TBI, when the autoregulatory function may change rapidly (Czosnyka et al., 1996). When moderate HC is, however, applied repeatedly, cerebral oxygenation will need to be monitored to prevent ischemia.
The augmented detection of CPPOPT during moderate HC in 17 out of 30 patients included into this study seemed to have been related to an improved Mx-autoregulation and to a shift toward greater CPP. Mx-autoregulatory indices revealed that moderate HC has established a normal FV responsiveness to spontaneous CPP fluctuations despite differences in baseline autoregulation. This HC-induced optimization of Mx- autoregulation has also been described by Piechnik and associates (1999) in normal volunteers and is assumed to be directly related to its vasoconstrictive effect. Paulson and associates (1990) have demonstrated that the hypocapnic vasoconstriction does not shift, but, rather, expands the plateau region of the cerebral autoregulatory curve. This may explain why short-term moderate HC did not significantly change CPPOPT in those with a detectable optimum at normocapnic conditions. Moreover, we hypothesize that a wider autoregulatory plateau may have also enhanced the detection of the optimal perfusion pressure when CPPOPT was outside the normocapnic CPP range or significantly above the normocapnic CPP mean. After brief moderate HC, the CPP–Mx relationship has converged toward a CPPOPT in each of 29 patients with TBI. However, long-term application of HC is no therapeutic option, as it may reduce cerebral blood flow and pose the risk of brain ischemia. As long as the critical PaCO2 levels are not specified, moderate HC has to be limited to a brief time span and normocapnia should be re-instituted as soon as is feasible, as described by Bratton and associates (2007).
The most obvious therapy to be influenced by autoregulation monitoring is the optimization of CPP. Short-term moderate HC may provide useful support to a CPP-guided therapy as it augments the detection of CPPOPT. This brief test warrants further investigation, to determine whether CPPOPT changes in the time course after TBI.
Footnotes
Acknowledgments
The authors thank the whole team participating in data collection, and all the nursing and research staff at the Department of Neurosurgery.
Author Disclosure Statement
Dr. C. Haubrich is supported by a Feodor-Lynen scholarship from the Alexander-von-Humboldt Foundation; Dr. M. Kasprowicz is a scholar of the Foundation for Polish Science; and Dr. M. Czosnyka and Dr. P. Smielewski are supported by MRC grant No.: G9439390, ID 65883. Dr. M. Czosnyka is on unpaid leave from Warsaw University.
ICM+ software (