
Abstract
The use of a prognostic model to aid clinician decision-making with regard to decompressive craniectomy for patients with severe neurotrauma has not been examined. Thus in this study we assessed whether an internationally validated prediction model would influence clinician decision-making about craniectomy. A two-part structured interview, given before and after knowing the predicted risks of unfavorable neurological outcomes at 6 months, was used to assess the participants' recommendations about performing decompressive craniectomy in three patients with severe traumatic brain injury. The participants rated their preferences when there was no surrogate decision maker available, when the next of kin requested surgical intervention, when the patient had an advance directive, and when the participant was the injured party. A visual analogue scale (1–10) was used to assess the strength of their opinions. A total of 50 neurosurgeons and intensive care physicians participated in this study. The participants were significantly more likely to recommend decompressive craniectomy for their patients than for themselves, especially when the next of kin of the patient demanded the procedure, and were more similar in their own preferences to patients who had advance directives. Clinicians' preferences to perform the procedure for both themselves and their patients was significantly reduced after knowing the predicted risks of unfavorable outcomes, and these changes in attitude were consistent across those with different specialties, regardless of the amount of experience caring for similar patients, or religious background. In conclusion, the predicted risks of unfavorable outcomes influenced clinician decision-making about recommending decompressive craniectomy for patients with very severe neurotrauma.
Introduction
T
Quality of recovery after severe neurotrauma is important. Evidence suggests that neurotrauma is not a discrete event, but is instead a disease process associated with many long-term complications (Masel and DeWitt, 2010). Our previous study showed that functional outcomes after decompressive craniectomy can be quite poor in some patients (Honeybul et al., 2010). The decision to offer life-saving, but not restorative, surgery to patients with severe neurotrauma can be difficult. Balancing the risk of not doing enough against the risk of doing too much with the result of poor neurological recovery is emotionally challenging, both for health care providers and the families of patients. This dilemma has always been a difficult one that is often complicated by the inability to reliably predict outcome.
While there have been many studies that have emphasized the importance of age (Aarabi et al., 2006; Guerra et al., 1999; Howard et al., 2008; Steyerberg et al., 2008; Ucar et al., 2005), Glasgow Coma Scale (GCS) score (Cremer et al., 2006; Guerra et al., 1999; Steyerberg et al., 2008; Ucar et al 2005), pupillary reactions (Cremer et al., 2006; Steyerberg et al., 2008; Ucar et al 2005), extracranial injuries (Steyerberg et al., 2008; Ucar et al., 2005), and radiological appearance (Cremer et al., 2006; Munch et al., 2000; Steyerberg et al., 2008), the CRASH study provided the first user-friendly web-based outcome prediction model, one that has been internally and externally validated with a large number of patients in both high- and low-income countries (Perel et al., 2008).
The model provides a percentage risk of an unfavorable outcome at 6-months follow-up. Unfavorable outcomes are defined by the Glasgow Outcome Scale (GOS) as severely disabled, persistent vegetative state, or dead. By applying this model to a large cohort of patients who have had a decompressive craniectomy, and for whom 18-month follow-up data are available, we have previously demonstrated how this percentage risk can be used as an index of injury severity, and may be useful as a guide to inform clinicians about the possible risk of poor neurological outcomes (Honeybul et al., 2009, 2010). The potential utility of a prognostic model to assist clinician decision-making regarding decompressive craniectomy has yet to be evaluated.
We hypothesized that the objective data generated by a well-validated prognostic model, the CRASH prediction model, may be useful in assisting the clinician's decision to recommend decompressive craniectomy for patients with severe neurotrauma, and thus we conducted a structured-interview study to assess whether the predicted risks of unfavorable neurological outcomes affect clinician opinions when recommending decompressive craniectomy for patients with severe neurotrauma.
Methods
After obtaining hospital ethics committee approval, a total of 50 neurosurgeons, intensive care specialists, and registrars, working in three adult public tertiary hospitals in Western Australia, were approached for this study. All participants were interviewed individually using a structured format. They were shown the following three clinical patient case reports.
Case 1
A 52-year-old female motorcyclist was involved in a motor vehicle accident. Her initial GCS was 11 (E3, M6, V2), and her pupils were equal and reactive. She had sustained major pelvic and lower limb fractures. She is currently intubated, sedated, and ventilated in the intensive care unit on day 2 following the injury. Her intracranial pressure (ICP) was persistently above 30 mm Hg, despite insertion of an external ventricular drain and maximal medical management. CT scan of the brain reveals diffuse petechial hemorrhages, traumatic subarachnoid hemorrhage, a non-evacuated hematoma, and midline shift (Fig. 1).
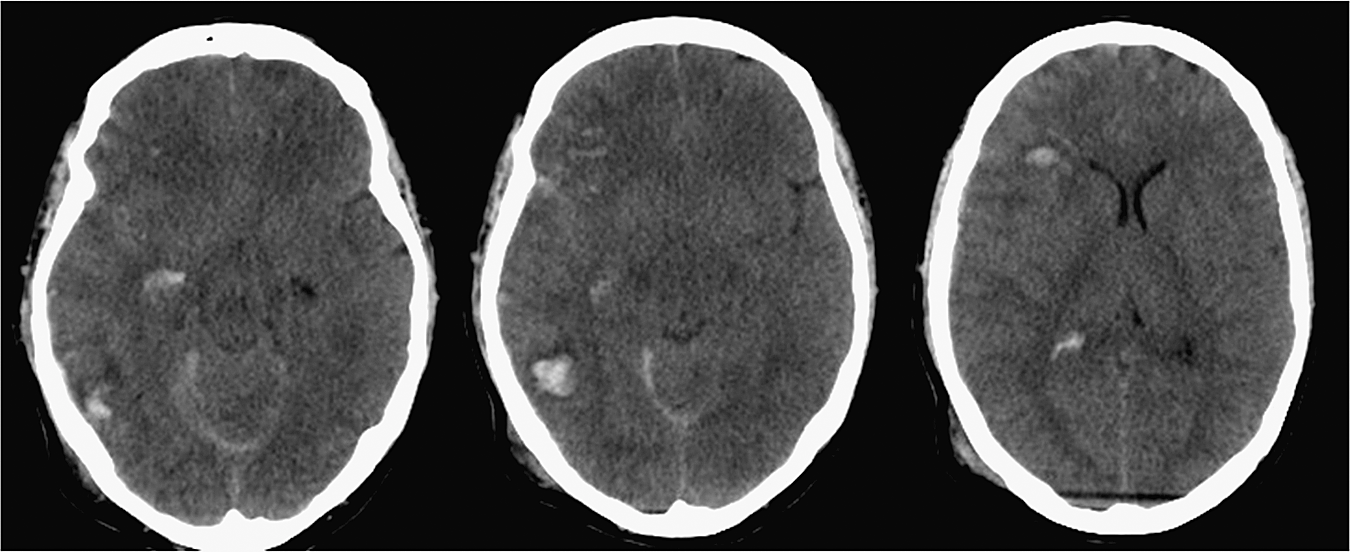
Imaging of the 52-year-old female motorcyclist involved in a motor vehicle accident.
Case 2
A 59-year-old male suffered a fall. His initial GCS score was 6 (E1, M4, V1), his right pupil was unreactive, and his left pupil was reactive. There were no other injuries. He is intubated, sedated, and ventilated in the intensive care unit on day 2 following injury. His ICP was persistently above 30 mm Hg despite insertion of an external ventricular drain and maximal medical management. CT scan of the brain revealed diffuse petechial hemorrhages, traumatic subarachnoid hemorrhage, and a non-evacuated hematoma (Fig. 2).
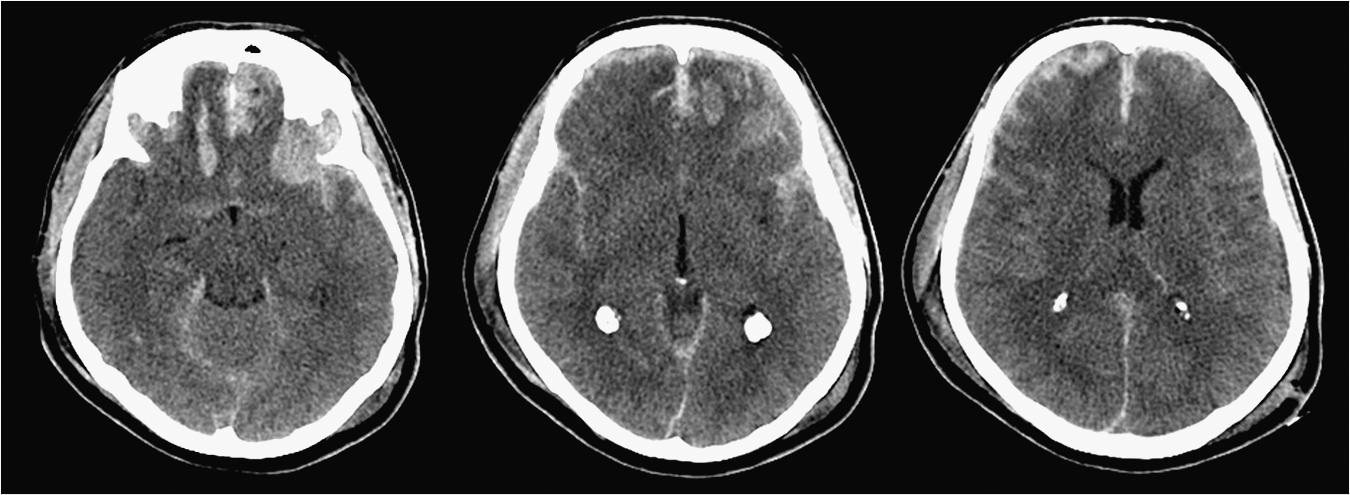
Imaging of the 59-year-old male who was injured following a fall.
Case 3
A 42-year-old male sustained an isolated head injury following an assault. His initial GCS score was 4 (E1, M2, V1), and his pupils were small and unreactive. There were no other injuries. He is intubated, sedated, and ventilated in the intensive care unit on day 1 following the injury. The ICP has persistently been above 30 mm Hg despite insertion of an external ventricular drain and maximal medical management. CT scan of the brain revealed diffuse petechial hemorrhages, scattered traumatic subarachnoid hemorrhages, obliteration of the basal cisterns, a non-evacuated hematoma, and midline shift (Fig. 3).

Imaging of the 42-year-old male with an isolated head injury following an assault.
In all three cases there was no cardiovascular instability, and a repeat CT scan showed no changes. No other specific information regarding outcome prediction was given, other than to point out that in case 1 the female motorcyclist was initially obeying commands, in case 2 there was a fixed pupil, and in case 3 the pupils were unreactive and the basal cisterns were obliterated.
A simple visual analogue scoring (VAS) system (range 1–10) was used to assess the strength of the inclination of the participant to perform decompressive craniectomy (i.e., a score of 10 signified the strongest recommendation to proceed with surgery, and a score of 1 signified the strongest disinclination to proceed with surgery). All VAS assessments were obtained after interpreting the clinical and CT data for the three cases, and participants were given four different scenarios at the time of decision-making. These four clinical scenarios were: No family or friends of the patient are present to provide surrogate advice. The parents of the patient are present, and despite being told of the possibility of a poor outcome, they are insistent on any medical intervention that might improve the chance of survival. The patient is a professional motorcyclist who has an advance directive stating that they do not want medical intervention that will leave them disabled. The participant him- or herself is the patient at that age, with the presenting findings.
The participants were then shown the CRASH collaborators outcome prediction model of the three patient cases and their predicted risk of unfavorable outcomes, along with the prognostic criteria of the model (Table 1). They were also shown the observed outcomes of patients with a similar predicted risk (or index of injury severity), in a large cohort of neurotrauma patients in Western Australia (Fig. 4; Honeybul et al., 2010). The participants were then asked the same questions again to rate their recommendations to proceed or not with decompressive craniectomy. The participants' responses before and after knowing the predicted risks of unfavorable outcomes were then compared.
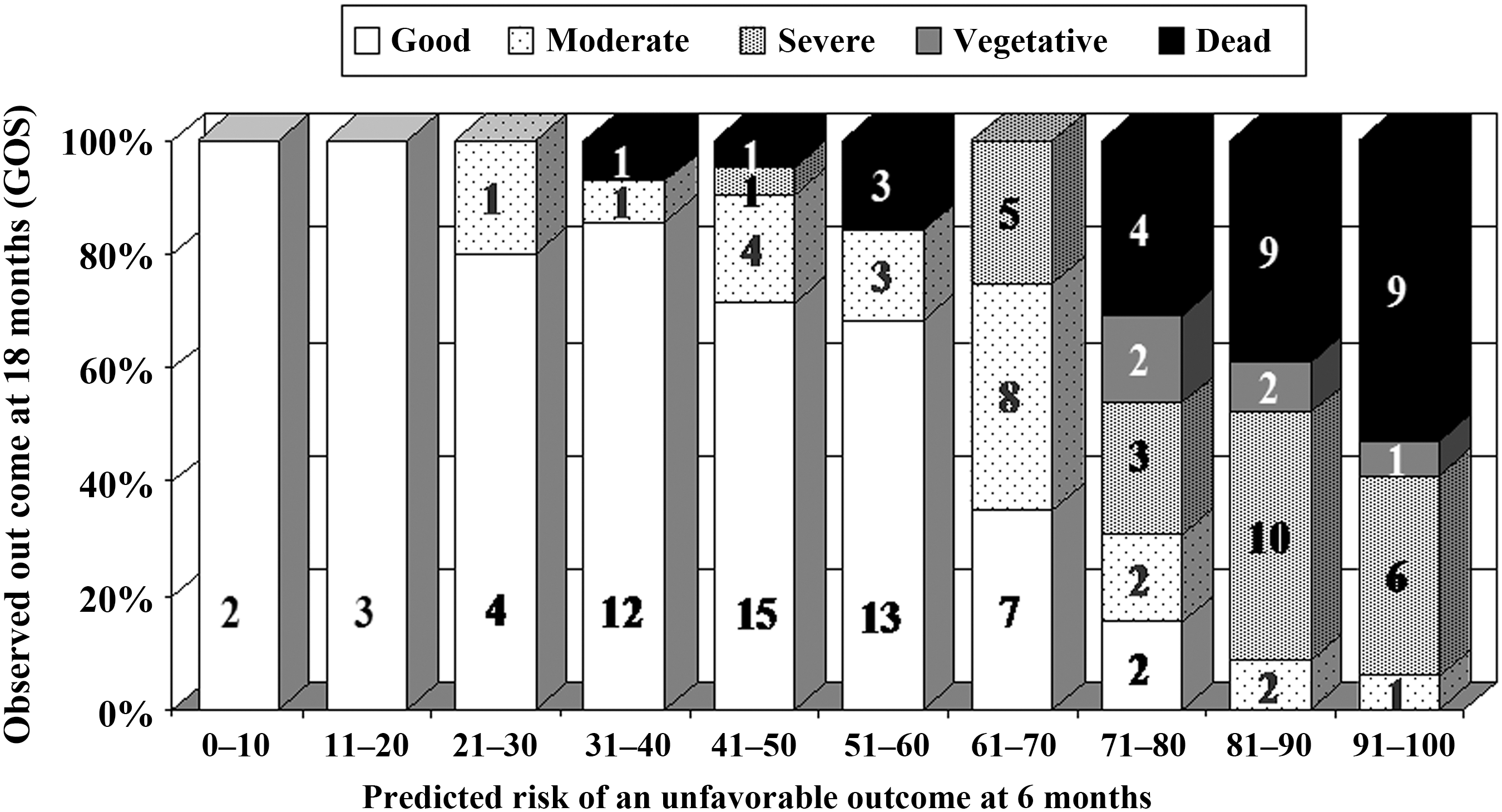
The prediction of an unfavorable outcome and the observed outcomes for patients with similar levels of predicted risk (or index of injury severity), in a large cohort of neurotrauma patients who had a decompressive craniectomy in Western Australia between the years 2004 and 2008 (Honeybul et al., 2010; GOS, Glasgow Outcome Scale).
Statistical analysis
A paired t-test was used to assess the mean differences in VAS scores of the participants before and after knowing the predicted risks of unfavorable outcomes of the three patients for the different scenarios. Wilcoxon's rank test was used to generate the p values of the differences. Stratified analyses according to medical specialty, age, religious background (Christianity, Hinduism, Buddhism, no religion, or other), and extent of experience caring for similar patients were also conducted. All analyses were performed using SPSS for Windows (version 13.0; SPSS Inc., Chicago, IL), and significance was set at p < 0.05.
Results
Of the 60 potential participants approached for the study, a total of 16 neurosurgical specialists and registrars, and 34 intensive care specialists and registrars in Western Australia participated in the study (83.3%). The characteristics of the participants are shown in Table 2.
Opinions regarding intervention prior to seeing the predicted and observed outcomes
Prior to seeing the outcome prediction and the observed outcome, the mean scores reflected the progressively greater severity of injury of cases 1, 2, and 3. Thus there was a strong tendency towards intervention in case 12 (mean score 7.35), and a tendency not to intervene in case 3 (mean score 4.21; Tables 3a, 3b, and 3c).
p < 0.001.
p < 0.001.
p < 0.001.
The family requests made at intervention had little effect on the participants' opinions, although there was a marginal tendency towards being more likely to intervene. The presence of an advance directive had a more significant effect, with participants being less likely to advocate intervention in case 2 (mean score 3.73) and in case 3 (mean score 2.89).
If the participant was the injured party there was a tendency toward advocating intervention in case 1 (mean score 6.62), but not in case 2 (mean score 3.81), or case 3 (mean score 3.15).
Opinions regarding intervention after seeing the predicted and observed outcomes
Having seen the prediction of an unfavorable outcome for each patient, and the observed outcomes of patients with similar predictions of unfavorable outcome (or index of injury severity), there was a significant reduction in the mean scores, reflecting participants' views that they would be less likely to advocate surgical intervention in all four scenarios at the time of decision-making (p < 0.01 for all).
Opinions regarding intervention combining all responses both before and after seeing the predicted and observed outcomes
Overall, a clinician's tendency to proceed with a decompressive craniectomy if they themselves were the patient (mean score 3.58), was similar to what they recommended for patients with an advance directive (mean score 3.19; mean difference = −0.39; 95% CI −0.39, 0.16; p = 0.193).
However, they were significantly more likely to perform a decompressive procedure for their patients (mean score 4.7; mean difference = 1.12; 95% CI 0.59, 1.65; p = 0.001), and slightly more so when the next of kin was requesting intervention (mean score 5.05; mean difference = 1.47; 95% CI 0.93, 2.01; p = 0.001).
The reductions in the strength of their recommendations to proceed with decompressive craniectomy after knowing the predicted risks of unfavorable outcomes were consistent across different specialties, positions, levels of prior experience caring for similar patients, religious backgrounds, and age of the participant.
Discussion
Clinical decisions are usually based on a combination of factors such as clinical experience, data from the published literature, and discussions with the patient regarding his or her particular preference. When deciding whether or not to perform a decompressive craniectomy in a patient with a severe head injury, the clinician invariably has to rely on surrogate decision-makers to establish what outcomes would and would not be acceptable to the patient if it were possible to ask them directly. In the context of decompressive craniectomy for severe head injury, if these discussions are dichotomized as either life or death, it is likely that the surrogate decision-maker will fail to recognize another significant category, namely survival with a neurological condition that is unacceptable to the patient.
Until recently this outcome has been difficult to predict. A previous study demonstrated that by using the CRASH collaborators outcome prediction model as an index of injury severity, it is possible to compare the predicted outcome with the observed long-term outcome. Once the injury reaches a certain level of severity, life-saving intervention is likely to leave the patient severely disabled (Honeybul et al., 2010).
In this study we demonstrated how the opinions of a group of clinicians familiar with the procedure can be influenced by the predicted risk of an unfavorable outcome, and the observed outcome at 18 months' follow-up. The utility of the prognostic model appears to be consistent across participants with differing backgrounds. While we agree with the CRASH collaborators that it should not replace clinical judgment, our results suggest that data from a reliable prognostic model, such as the CRASH prognostic model, can be used as an index of injury severity, and may facilitate the discussion of realistic outcome expectations among health care givers and patients' families.
The finding that participants' tendencies to proceed with decompressive craniectomy for themselves was much less than what they would choose for their patients if no surrogate was available is an interesting one. The reasons behind this result remain unclear. Possible reasons include medicolegal issues, unpleasant experiences when caring for patients with poor neurological outcomes, and a strong belief in quality of life rather than length of survival.
This study has some significant limitations. First, although we included most intensive care and neurosurgical clinicians in this study, the effect of a prognostic model on the opinions of the nurses, physiotherapists, and more importantly, families of patients with severe traumatic brain injury, were not assessed and remain uncertain. What constitutes an unfavorable outcome varies among differing subcultures, religious groups, and levels of education. Time also may have an effect, as in some cases patients continue to improve long after the initial head injury (Hoofien et al., 2001; Sbordone et al., 1995). What may be perceived as unfavorable initially may become less so as time passes, and this requires consideration when making decisions, both in the short and the long term. Second, the participants were the sole decision-makers in some of the clinical scenarios used in this study. The decision to perform decompressive craniectomy is difficult, and often involves multiple stakeholders in clinical practice. In addition, though the use of predicted and observed outcomes has shown how clinical decisions may be influenced, whether this induces clinicians to make correct decisions is debatable. For example in case 1, the clinicians were less likely to intervene having seen the observed outcomes of patients with similar levels of injury. However, the observed outcome revealed that 4 of the 13 patients with a similar outcome prediction had a favorable outcomes, and indeed 2 of these patients achieved good outcomes at 18-months' follow-up. It could be argued that it would be difficult not to proceed based on these data, and that the correct clinical decision would be to perform surgical decompression. This highlights the limitations of the artificial interview process, in which one tends to give a more idealistic response than they would in a real-life situation. However, it does demonstrate that this group of physicians may be relatively risk-averse. Finally, using a mathematical model based on historical data will always have limitations. The MRC CRASH study was not designed to provide data for an outcome prediction model, and while the model appears to be robust, there are several variables that have also been shown to influence outcome, such as coagulopathy (Ho et al., 2010), MRI findings (Woischneck et al., 2010; Zheng et al., 2007), and advances in brain tissue oxygen monitoring (Adamides et al., 2009; Spiotta et al., 2010). Surgical and intensive care therapies continue to advance, and constant re-evaluation of each patient is required to avoid poor decision-making for these unfortunate patients with severe traumatic brain injury.
Summary
This study has demonstrated that the CRASH collaborators predictive model may have some influence upon clinician decision-making. In all instances, in light of a high predicted risk of a poor functional prognosis, we found a significant shift away from the use of decompressive craniectomy. This study also demonstrated that clinicians would do less for themselves as patients than they would undertake for their patients. This leads to the question of whether clinicians are intrinsically biased in their recommendations about decompressive craniectomy for patients with severe traumatic brain injury. Future research should be undertaken that involves the entire health-care community that serves patients with severe head injuries.
Footnotes
Author Disclosure Statement
No conflicting financial interests exist.