
Abstract
Cranial CT scans are at the center of decision making in brain injuries in children because of their speed and ability to detect surgically relevant lesions. However, alternative techniques, such as conventional MRI may have advantages in terms of radiation exposure and sensitivity to detect brain injury. Susceptibility-weighted imaging (SWI), a relatively novel MRI sequence, shows promise in terms of its sensitivity in detecting hemorrhagic lesions; however, its clinical potential remains uncertain. In this observational study of children (5–16 years of age) with traumatic brain injury (TBI) at a tertiary pediatric emergency department (ED) we compared the ability of detecting traumatic brain lesions on acute CT and MRI/SWI ∼5 weeks post-injury based on detecting the presence or absence, extent, and type of traumatic brain lesions. We analyzed the results of 76 patients (53 male) after TBI (mean age 10.24±2.50 years, range 5.75–14.67 years). Glasgow Coma Score was 13–15 in 54 patients (71%), 9–12 in 13 patients (17%) and <8 in 9 patients (12%). CTs were completed in the ED; MRI and SWI were completed at a mean of 36.11±15.75 days post-injury. Detection of any lesions occurred on CT scan in 68%, on MRI in 54%, and on SWI in 86% of cases, and SWI detected additional lesions 30% of the time compared to CT and MRI. SWI may be more sensitive in detecting traumatic lesions than CT or MRI. This may be important for the ongoing management of TBIs and their prognosis.
Introduction
B
MRI has the capacity to detect some lesions that are not seen on CT and therefore has the potential to increase diagnostic accuracy, while reducing radiation risk in pediatric TBI (Lee et al., 2008; Suskauer and Huisman, 2009). Nonetheless, Ashwal and colleagues (2006) note that, in combination with clinical indicators such as the Glasgow Coma Scale (GCS), duration of coma, post-traumatic amnesia, and neurological signs, conventional brain imaging such as CT and MRI “still only correctly classifies about 80% of gross neurologic outcomes in children”, suggesting that further improvements in brain lesion identification and classification constitute an ongoing concern. The advent of novel MRI techniques in recent years has caused the medical community to reflect on imaging alternatives. Of these, susceptibility-weighted imaging (SWI) has been shown to be one of the most promising in the area of acquired brain injury (Tong et al., 2008). SWI is a specific MRI sequence that exploits the magnetic susceptibility differences between tissues by using a sequence that is sensitive to magnetic susceptibility phenomena and is therefore useful for identifying extravascular blood products (Haacke et al., 2004). In the context of brain trauma, SWI has been reported to significantly increase lesion detection, depicting up to six times more lesions and double the apparent volume of hemorrhagic lesions (Tong et al., 2003). SWI's increased sensitivity to blood products make it particularly useful for the detecting of microhemorrhages, the presence of which has been shown to be related to poor outcome in children with non-accidental brain trauma (Colbert et al., 2010).
Despite the potential of the SWI technique to improve management of pediatric TBI, few studies have examined differences in detection rates for parenchymal lesions. One other study compared multimodal neuroimaging techniques in children with TBI and found that conventional MRI techniques, such as T2 and fluid attenuated inversion recovery (FLAIR) and SWI provided more precise lesion detection and evaluation of 6–12 month outcomes than did CT (Sigmund et al., 2007). These results have implications for TBI management in the ED and for prediction of outcome, and suggest that further investigation of multimodal neuroimaging techniques in pediatric TBI is warranted. As part of a longitudinal cohort study, we scanned a large number of children after pediatric TBI with conventional MRI and SWI sequences. It became apparent that the findings with these neuroimaging modalities differed from those of the inital CT scans obtained during the acute phase.
As neuroimaging tools emerge, it is important to continuously evaluate their potential, as well as their limitations, in providing additional diagnostic and prognostic information in children with TBI. SWI may be such a tool if it can detect lesions where another imaging modality detected none or fewer lesions. This increased sensitivity may have ramifications for acute management as well as for outcome prediction and the need to target at-risk children for long-term follow-up and intervention. We set out to compare the detection of parenchymal brain lesions after pediatric TBI across three neuroimaging modalities: CT, MRI, and SWI.
Methods
Study design
This was a prospective cohort study in a convenience sample of children presenting with TBI to the ED at a tertiary pediatric metropolitan hospital. The main goal of the larger study was to investigate social problems following TBI in school-age children. For the purposes of this study we analyzed neuroimaging findings obtained from the study.
Setting and population
The study was conducted at the Royal Children's Hospital (RCH), Melbourne, Australia. The tertiary ED has an annual census of 67,000. The baseline CT rate for TBI of any severity at RCH is 19% (Crowe et al., 2010). At RCH, published TBI guidelines (
Inclusion criteria
(i) age at injury 5.0–16.0 years; (ii) documented evidence of a closed head injury; and (iii) English speaking.
Exclusion criteria
(i) documented history of previous TBI; (ii) non-accidental injury; and (iii) evidence of a documented pre-existing neurological, psychiatric, or developmental disorder, including intellectual disability.
Primary outcome measure
Detection of absence or presence of any parenchymal brain lesions using three neuroimaging modalities (CT, MRI, SWI). Fractures were reported separately.
Protocol
The study was approved by the Human Research Ethics Committee. Parents of children with TBI were contacted by a research assistant after presentation to the ED. After providing informed consent, patients were scheduled for MRI scans between approximately 2 and 8 weeks post-injury; they were also evaluated with a battery of cognitive and social tests at 6, 12, and 24 months post-injury (these data are being analyzed separately). ED management of enrolled patients, including the decision to perform a cranial CT scan, was at the discretion of the treating ED clinician. ED clinicians were unaware of whether or not the child was a participant in this study when determining the child's acute management.
Neuroimaging
CT
A non-contrast CT scan was obtained according to standard head trauma hospital guidelines using a multidetector CT scanner (Siemens SOMATOM Sensation 16 CT, Erlangen, Germany) during the ED visit, including 1.5-mm axial scans reconstructed in axial, coronal, and sagittal planes and viewed at brain, bone, and soft-tissue windows. The most acute (first) CT scan was used for comparison with MRI and SWI.
Conventional MRI
All participants underwent MRI as part of the research protocol after being exposed to a mock scanner and attending a familiarization session, in accordance with ethics requirements. MR images were acquired as soon as possible after recruitment and consent to the study on a 3T Siemens Trio scanner (Siemens Medical Systems, Erlangen, Germany) using a 32-channel matrix head coil. Conventional MR sequences were performed according to the specifications outlined in Appendix 1. The total acquisition time was 31:53 min.
SWI
A SWI sequence was added to the MRI protocol described previously. SWI imaging is a variant of the standard 3D FLASH sequence that exploits the signal loss from shortened T2* characteristics of calcium- and deoxyhemoglobin-containing lesions. The images are T2* weighted because of the range of acceptable TEs used in the acquisition (18–22ms). The increased sensitivity to shortened T2* lesions is caused by the image reconstruction techniques used. Both magnitude and phase images are reconstructed from the data set. The phase images display a higher sensitivity to local susceptibility variations and, as such, are used as an image mask to be combined with the magnitude data set. The combined data set is then reconstructed using a sliding window (eight individual slices compressed into one image) minimum intensity projection (MIP) data set (acquisition time 3:57 min).
Lesion detection and data analysis
All MRI scans were coded by a pediatric neuroradiologist and a neuropsychologist blinded to the clinical details at ED presentation and to the CT scan results obtained during the acute ED visit, and entered into an SPPS software database (SPSS Inc, Chicago, IL). Scans were coded according to a modification of the Coffey system (Catroppa et al., 2008; Coffey and Figiel, 1991) in order to determine the presence of lesions and hemorrhage, and their location and severity based on the extent of hyperintensities as seen on T1- or T2-weighted images. For this brief report, only basic information regarding location and type are presented. The regions of abnormality identified on the MRI scans were reviewed on the CT scan to determine if corresponding changes were present on the CT scan.
Results
Characteristics of study subjects
During the study period there were a total of 77 patients who presented to the ED with confirmed TBI as classified by the ED electronic database based on ICD 10 codes SO69, SO98, S099; met the inclusion criteria for TBI; and were enrolled in the study. There was one patient who did not undergo SWI scanning for technical reasons, and who was therefore excluded from the analyses. Of the remaining 76 patients, we analyzed the results of 48 patients with TBI who in addition to the research MRI and SWI, had a cranial CT scan during the initial ED visit. In addition, there were 28 patients who presented to the ED, were enrolled, and had MRI/SWI scans as part of the research project, but had received no CT scan in ED as per clinical decision by the ED clinicians. These patients will be described separately.
Enrolled patients who had a CT scan in the ED, as well as MRI and SWI (n=48) had a mean age of 10.2±2.6 years (range 5.8–14. 7 years). Of these, 32 were male. GCS on ED presentation was 13–15 in 28 cases (58.3%), 9–12 in 11 cases (22.0%), and ≤8 in 9 cases (18.8%). All CTs were completed acutely (e.g., while the patient was in ED); MRI and SWI were completed at a mean of 38.4±18.3 (range 4–111) days after ED presentation.
Main results
Results of lesion detection analysis across the three modalities revealed the following observations, detailed in Table 1. In 12 cases (25%) scans revealed no trauma-related intracranial pathology in any of the three modalities (GCS 15 in 7 cases, 14 in 1 case, and 11 in 1 case). Of the remaining 36 cases, detection of any possible parenchymal lesions occurred in CT scan in 24 cases (66.7%), MRI in 20 cases (55.6%), and SWI in 30 cases (83.3%). In 5 cases (13.9%), lesion detection was comparable across modalities and in 2 cases (5.6%) both CT and SWI detected pathology, but not in the same areas. There were 6 cases (18.9%) of varying severity levels: GCS 15 (2 cases), 14 (1 case), 9 (1 case), 6 (1 case), and 4 (1 case), in which lesions were detected only on CT scan. Notably, 4 of the injuries were subdural, and only 2 involved intra-axial lesions (1 frontal hematoma, 1 parieto-occipital contusion) not detected on MRI or SWI. There were no cases in which only MRI detected lesions. However, there were also 6 cases (18.9%) in which only SWI detected lesions, and all were in patients with mild TBI as defined by GCS 13 (1 case), 14 (3 cases), and 15 (2 cases).
B, bilateral; MRI, conventional MRI sequences; DAI, diffuse axonal injury; ENC, encephalomalacia; GCS, Glasgow coma scale; GM, gray matter; H, hemorrhage; L, left; R, right; SWI, susceptibility-weighted imaging; WM, white matter.
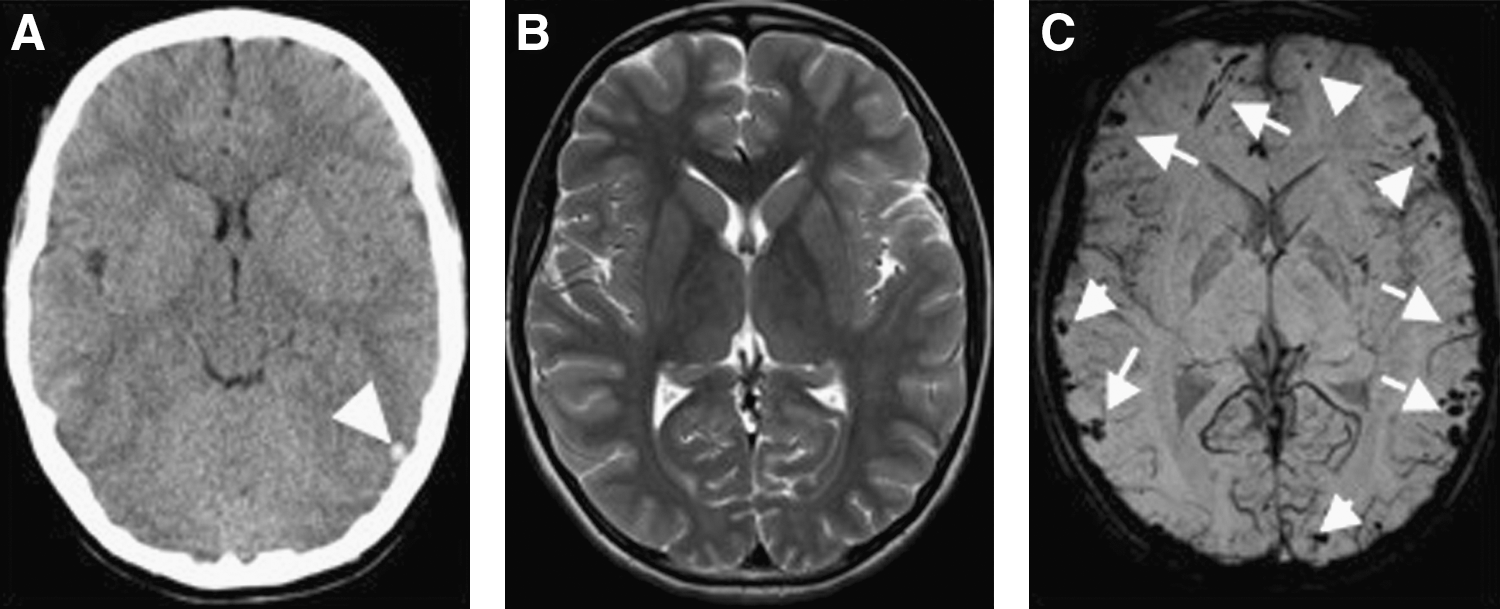
Despite the finding that, overall, detection of the presence of any lesion occurred more frequently with CT than with MRI, as noted previously (66.7 vs. 55.6%), there were nonetheless 15 cases (41.6%) in which MRI detected additional lesions compared to CT. In 4 of these cases, SWI was just as effective as MRI at lesion detection; however, there were a further 11 (30.5%) cases in which SWI detected the most extensive pathology of all three modalities (see example, Fig. 1). These 11 cases combined with the 6 cases in which only SWI detected pathology suggest that in total, SWI was the most sensitive modality in 47.2% of cases, and more sensitive than CT, but at least as sensitive as MRI in 21 cases (58.3%). An important observation of the cases in which SWI was the most sensitive, is that there were 11 cases (52.4%) in which CT was normal, and 7 cases in which MRI was normal (33.3%).
Results of
We also analyzed the 28 patients with TBI who were part of the overall study, but who were excluded from the main analysis as they had no CT scan prescribed in the ED (mean age=10.3±2.3 years, range 6.3–14 years) (Table 2). All of these patients had mild TBI with GCS 13 to 15 without focal or diffuse neuropathology, except for one patient who had a GCS of 12. All had been discharged home from the ED. In 6 (21.4%) of these patients, neuroimaging conducted 6–8 weeks later (mean 32.79±9.50 days) showed parenchymal abnormalities either on MRI (3), SWI (1), or both (2).
B, bilateral; MRI, conventional MRI sequences; GCS, Glasgow coma scale; GM, gray matter; H, hemorrhage; L, left; R, right; SWI, susceptibility-weighted imaging; WM, white matter.
Of the 48 patients with CT in the ED, 9 (18.7%) patients underwent neurosurgical procedures including elevation of skull fractures (3), and decompressive craniotomy with external ventricular drain (1).
Discussion
Recent large-scale multicenter studies have derived decision rules for TBI management in children (Dunning et al., 2006; Kuppermann et al., 2009; Osmond et al., 2010). These focus on the question of who may or may not require a head CT scan. The key finding of this study is that initial CT scan findings after TBI are generally a poorer marker of structural parenchymal lesions than is MRI, and especially SWI, when scanned more than 4 weeks post-injury. Overall, SWI detected neuropathology more frequently and detected a greater number of lesions than did MRI and CT.
To date, there are very few studies comparing cranial CT results after pediatric TBI when obtained in the acute ED phase, with MRI/SWI findings in the early recovery phase. In one other study, these modalities were also compared after pediatric TBI (Sigmund et al., 2007); however, CT and MRI scans were obtained ∼1 week apart and the TBI sample included only hospitalized patients who had an indication for further MRI scanning. A study by Woischneck and colleagues (2003) similarly compared imaging modalities (CT and MRI) 8 days apart and found MRI to have a high predictive value for outcome; however, a SWI sequence was not included and only children with severe injuries were studied. In the current study, all children recruited underwent MRI scanning regardless of injury severity and regardless of whether they had an indication for MRI scanning or not. We also included patients for MRI scanning who did not undergo CT in the ED because of the perceived mild nature of their injury, which has never been examined before. This is significant in light of data indicating that even mild brain injuries can cause structural or functional brain disturbances, often not evident on CT imaging (MacKenzie et al., 2002; Povlishock, 1993; Umile et al., 2002). In general, when all modalities detected pathology, MRI detected more parenchymal lesions than did CT scans, and SWI detected more lesions than did MRI, often ones that were bilateral, multifocal, or affecting additional areas. Interestingly, even though there were a number of cases in which MRI was more sensitive than CT in terms of number of lesions detected, there was as a greater percentage of cases in which CT indicated the presence of pathology compared to MRI (67% vs 56%). This is most likely because of the delayed timing of the MRI scans, which were performed on average 1 month post-injury, after which time it is possible that acute injuries may have resolved naturally or through evacuation via neurosurgical procedures (two cases of craniotomy).
These observations support those of previous studies in which quantitative analyses have confirmed the greater sensitivity of SWI to hemorrhagic lesions (Chastain et al., 2009; Sigmund et al., 2007; Tong et al., 2003). These observations have potential implications for outcome prediction based on location and extent of lesions. There has been some positive support for the ability of SWI to predict functional outcome (Kou et al., 2010; Wu et al., 2010). For example, Tong and colleagues (2004) found that the number and volume of hemorraghic lesions detected with SWI correlates with long-term outcome using the Pediatric Cerebral Performance Scale. In contrast, Chastain and colleagues (2009) recently reported that SWI may not be as useful as conventional MRI and CT at predicting outcomes, however, outcomes were based on a simple outcome dichotomization (good/bad) and results may be different when more precise measures are used. Future studies should focus on relating multimodality imaging methods to specific cognitive and functional outcomes in order to determine their prognostic potential.
Of particular interest are patients who had negative CT scans or no CT scan in the ED because of low clinical suspicion of significant brain injury, but were found to have parenchymal lesions with MRI and/or SWI. Absence of need for a CT or negative CTs during the acute phase are generally regarded as encouraging prognostic indicators in terms of the need for neurosurgical intervention and longer term outcome (Dunning et al., 2006; Kuppermann et al., 2009; Osmond et al., 2010). However, some studies have highlighted the imperfections of CT when used alone in outcome prediction (Maas et al., 2005; Zhu et al., 2009), showing, for example, that in cases of mild brain injury, age at injury and other clinical variables are stronger predictors than CT (Jacobs et al., 2010). Furthermore, the establishment of clear links between underlying pathology and the sequelae of mild TBI remains a challenge and there are numerous cases of mild TBI in which children are slow to recover or experience persistent post-concussive symptoms, but have no evidence of underlying structural brain changes seen on CT (Taylor et al., 2010; Wozniak et al., 2007; Yeates, 2010). Clinical research and studies in animals indicate that there may, nonetheless, be underlying structural and functional abnormalities only evident using alternate neuroimaging techniques (Elson and Ward, 1994; Giza and Hovda, 2001; Levin et al., 1987). It may be that more sensitive techniques, such as SWI, are able to discern subtle structural changes that explain neurological, cognitive, or behavioral symptomatology. Among patients who did not undergo CT scans, two had small gliotic lesions visible only on MRI. It is probable that because the lesions were gliotic and not associated with hemorrhage, they had high T2 and FLAIR signal on conventional MRI, but were not visible on SWI because of its particular susceptibility to blood products. Clinicians will need to be aware of these findings in terms of TBI management, outcome, neurorehabilitation, need for follow-up, and return to play, in the case of sports-related concussions.
These studies, in combination with our results, suggest that whereas CT may be important for early classification of brain injury, accurate diagnosis, and need for neurosurgery, MRI in combination with a SWI sequence may increase injury detection accuracy and sensitivity. There are other advantages to the use of MRI and SWI during the acute phase post-injury, such as absence of radiation, though all three techniques may require sedation depending upon the patient's age and injury severity. Until we better understand the importance of parenchymal lesions identified on MRI and SWI, physicians and their patients should be cautious about interpreting negative initial CT scans as reassuring or excluding neuropathology.
Limitations and Conclusions
This study has a number of limitations. The study group was a convenience sample in a setting with a CT scan rate for TBI of 19% (Crowe et al., 2010), higher than the rate reported in a United Kingdom-derived clinical TBI decision rule (Dunning et al., 2006) and lower than the ∼50% reported from North America (Kuppermann et al., 2009; Osmond et al., 2010). Our description of the presence and absence of lesions and the number of lesions is a coarse measure. More sophisticated quantitative analyses are needed to describe the exact extent and location of lesions detected by different neuroimaging modalities. We excluded children <5 years of age because of the ethical and technical complications of additionally requiring general anesthesia for the research scans. The study group still included a relatively wide age range and future studies may also investigate the potential of these techniques in younger versus older children. CT and MRI/SWI were performed at a mean of 5 weeks. Four patients (1 mild, 1 moderate, 2 severe) had significantly longer scan intervals (70–111 days) because they were medically unstable (e.g. had had neurosurgery) or unable to tolerate the MRI scanning procedure without sedation. The logistics of scanning children with both modalities concurrently can be difficult ethically and within a clinical context. SWI is sensitive to blood products and it can therefore be assumed that lesions are visible very early in the acute phase and that they could persist well into the chronic phase, although the time frame of their resolution would depend primarily on their size. It is possible that some pathology detected acutely in the ED on CT had resolved before MRIs were completed, which may lead to an underestimation of the potential of MRI and SWI in terms of lesion detection in comparison to the acute CT. Alternatively, initial lesions may have been too subtle to detect early on, and may have become more prominent even on CT at a later time. Ultimately, the detection of lesions or of a greater number of lesions only represents a structural description in this study. This study should be repeated with CT, MRI, and SWI conducted in parallel in the acute post-injury phase. Ideally this should include patients who were excluded from scanning by the application of TBI decision rules. These results will also need to be correlated with functional outcome and long-term sequelae to understand the importance of parenchymal changes detected by MRI. This study indicates that SWI may be more sensitive in detecting traumatic parechymal lesions than CT or conventional MRI, and the results are important for the management and prognosis of TBI.
Footnotes
Acknowledgments
We gratefully acknowledge the financial support of the Victoria Neurotrauma Initiative (No. CO6E1) and the research assistance of Ms. Louise Crossley.
Author Disclosure Statement
No competing financial interests exist.
Appendix 1
| Conventional MRI scanning specifications (MRI) |
|---|
| Transverse turbo spin-echo (TSE) aligned parallel to the AC–PC line (TR=6380 ms, TE=93 ms, ETL=17, bandwidth 189 Hz/px, resolution 0.6×0.6×3.5 mm); sagittal 3D MPRAGE (TR=1900 ms, TE=2.15 ms, IR prep=900 ms, parallel imaging factor (GRAPPA) 2, flip angle 9 degrees, BW 200 Hz/px, 176 slices, resolution 1×1×1 mm); sagittal 3D T2-weighted nonselective inversion preparation SPACE (Sampling Perfection with Application-Optimized Contrast using different flip-angle Evolution) (TR=6000ms, TE=405ms, TI=2100 ms, water excitation, GRAPPA PAT2, 176 slices, 1×1×1 mm resolution matched in alignment to the 3D T1-weighted sequence). |
| Susceptibility-weighted imaging scanning specifications (SWI) |
|---|
| Images are acquired as a 3D slab-selective transverse volume (TR=28 ms, TE=20ms, flip angle 15 degrees, flow compensation, BW=120Hz/px, GRAPPA PAT2, magnitude/phase reconstruction, resolution 0.9×0.6×1.5 mm, mean number of slices 72. |