
Abstract
Many studies have addressed the question of whether intensive insulin therapy (IIT) provides better outcomes for brain-injured patients than does conventional insulin therapy (CIT), with conflicting results. We performed a systematic review and meta-analysis of the literature to estimate the effect of IIT on patients with brain injury. We searched MEDLINE, Embase, Cochrane Central Register of Controlled Trials (CENTRAL), and citations of key articles and selected
Introduction
G
Several studies have shown that hyperglycemia is associated with worse outcomes, including greater mortality (Bilotta et al., 2009b). The usual treatment for hyperglycemia, conventional insulin therapy (CIT), traditionally meant administering insulin when values were >200–220 mg/dL. In the light of reports of worse outcomes with hyperglycemia, a new therapeutic approach, intensive insulin therapy (IIT), was sought to maintain glucose levels within the range of 80–110 mg/dL. Following a landmark trial published in 2001 by van den Berghe (van den Berghe et al., 2001), which demonstrated the benefits of IIT among patients admitted to the intensive care unit (ICU), IIT gained popularity and had been recommended as the standard of care for critically ill patients by the American Diabetes Association (American Diabetes Association, 2008) and the American Association of Clinical Endocrinologists (Rodbard et al., 2007).
Subsequent randomized controlled trials (RCTs) and meta-analyses among critically ill patients failed to provide evidence of any mortality benefit of IIT (Brunkhorst et al., 2008; Finfer et al., 2009; Griesdale et al., 2009; Wiener et al., 2008). These differences may be because studies used different patient populations and methodologies. A positive effect of IIT was shown in a meta-analysis in patients admitted to the surgical ICU even though it was not found among patients admitted to medical ICUs (Griesdale et al., 2009). This implies that effects may vary in critically ill subpopulations, such as patients with brain injury, trauma, or surgical disease. Indeed, an RCT on the subpopulation of patients with traumatic brain injury (TBI) showed IIT to decrease mean intracranial pressure and the need of ventilator support, and improved long-term neurological outcomes (LTNO) (van den Berghe et al., 2005).
Brain injury is one of the leading causes of death and disability around the world and TBI alone in the United States accounts for >50,000 deaths, 1.2 million people with long-term disability, and an estimated cost burden of ∼$100 billion each year (Rutland-Brown et al., 2006; Selassie et al., 2008). Stroke is the third leading cause of mortality and the leading cause of serious long-term disability in the United States with ∼795,000 new or recurrent cases each year (Centers for Disease Control, 2001; Lloyd-Jones et al., 2010). We define brain injury as any acute damage to the brain tissue that leads to temporary or permanent impairment in brain function, including TBI, acute stroke, subarachnoid hemorrhage, and encephalitis. Patients with brain injury are particularly vulnerable to high blood glucose concentrations (Bilotta et al., 2009b). Both hypo- and hyperglycemia affect prognosis in brain-injured patients and there is an increasing belief that strict glucose control may benefit these patients (Godoy et al., 2010).
Many studies and RCTs have addressed the question of whether IIT provides better outcomes for brain-injured patients than does CIT, with conflicting results (Azevedo et al., 2007; Bilotta et al., 2007, 2008, 2009a; Bruno et al., 2008; Coester et al., 2010; Jacka et al., 2009; Johnston et al., 2009; Latorre et al., 2009; Thiele et al., 2008; van den Berghe et al., 2005; Vespa et al., 2006; Walters et al., 2006; Yang et al., 2009). We conducted the first meta-analysis of RCTs comparing IIT with CIT in patients with brain injury (TBI, stroke, encephalitis, and subarachnoid hemorrhage) to estimate the effect of this therapy in terms of mortality and other clinical outcomes.
Methods
Search strategy
We systematically searched MEDLINE, Embase, and the Cochrane Central Register of Controlled Trials (CENTRAL) for all comparative studies and conference abstracts comparing the effect of IIT to CIT among adult patients (age ≥16 years) with acute brain injury. Brain injury included TBI, subarachnoid hemorrhage, or encephalitis. We constructed search filters for 1) brain injury (traumatic, stroke, infection); and 2) insulin therapy, using a combination of MeSH terms and text word searches for synonyms. We separated these two concepts by the Boolean “AND” and limited the results (wherever possible) by limiting to comparative studies (details of search terms are provided in Appendix 1). No limits were applied on language or date of publication. The search was performed on May 6, 2010, and updated as of December 8, 2010. Additionally, we manually searched references of key articles. Conference abstracts were reviewed with Embase search results. This meta-analysis was performed in accordance with Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (Moher et al., 2009).
Selection criteria
In duplicate and independently, we screened all studies and selected articles that satisfied the inclusion criteria: 1) comparative study (trials, cohorts, case-controls); 2) the study population consisted of adults with brain injury (or the study reported outcomes of such patients as a subgroup analysis); 3) the study compared IIT to CIT; and 4) the study reported one or more of the outcomes of mortality, infections, hypoglycemic episodes, and LTNO. The exclusion criteria were: 1) studies with an intervention other than IIT, for example, glucose insulin potassium; 2) studies with no CIT arm, for example, IIT versus no insulin treatment or IIT versus saline with no insulin; 3) studies of subgroup analysis in which stratified randomization by the subgroup was not conducted; and 4) studies with a mixed patient population consisting of those with diagnoses other than those included in our definition of acute brain injury, for example, spinal cord injury. We included only RCTs for this analysis. IIT was defined as target blood glucose concentration of, at most, <150 mg/dL (8.3 mmol/L) (Wiener et al., 2008). Disagreements were resolved by consensus or group discussion. Articles in a language other than English were translated with the help of colleagues fluent in the foreign language.
Data abstraction and quality assessment
We extracted data in duplicate and independently for each study onto a standardized data extraction sheet. Disagreements were resolved by re-checking the article in question. We abstracted information on study characteristics, characteristics of the population under study, operational definitions, and outcomes. Two authors, with discussion and consensus, assessed the quality of randomized trials using the Cochrane tool to assess risk of bias (Higgins and Green, 2009). Definitions of IIT and hypoglycemia were used as they were used by authors in the study, with the intention to check for heterogeneity by definition if needed. Emails were sent to the corresponding or first authors of the studies if data were missing. We waited for responses from authors up to a period of 8 weeks until mid-July 2010.
Statistical analysis
Pooled relative risk estimates with their 95% confidence intervals were calculated for RCTs. Effect estimates were obtained by calculating trial-specific ratios based on intention-to-treat analysis. Our primary outcomes were early and late mortality; early mortality being defined as in-hospital mortality and late mortality being defined as 90 day or 6 month mortality. Secondary outcomes included in-hospital overall infection rates, number of hypoglycemic episodes, and LTNO. LTNO was re-coded as “good” or “bad” using the modified Rankin Scale (mRS) or Glasgow Outcome Scale (GOS), as reported by the authors. Good LTNO was defined as an mRS score of 4–6 or a GOS score of 4–5. One study (van den Berghe et al., 2005) defined good neurological outcome as a Karnofsky score of ≥60 at 12months. We included this definition in our analysis, with a plan to remove it if results proved to be heterogeneous.
We used a DerSimonian and Laird random effects model with inverse variance weights for all of our outcomes. Between-study heterogeneity was assessed using Cochran's Q statistic and the I2 statistic (Higgins et al., 2003). We considered a p value ≤0.1 or an I2 value of ≥50% as evidence of heterogeneity. A 0.5 continuity correction was applied to all four cells in case a zero value was present. A priori potential sources of heterogeneity were identified as patient population (traumatic vs. a-traumatic), definition of IIT(≤110 mg/dL vs. ≤150 mg/dL) (≤6.1 mmol/L vs. ≤8.3 mmol/L), definition of hypoglycemia (≤60 mg/dL vs. ≤80 mg/dL) (≤3.33 mmol/L vs. ≤4.44 mmol/L), risk of bias (low, unclear, high) (Higgins and Green, 2009), percentage of patients with diabetes (<50% vs. >50%). If heterogeneity was found, we assessed differences by random effects meta-regression using the abovementioned variables. Subgroup analyses were performed if the source of heterogeneity was determined. If the source of heterogeneity was not identified by meta-regression, we performed sensitivity analysis by eliminating one study at a time checking for resolution of heterogeneity.
We assessed publication bias by Egger test and visual inspection of the funnel plot (Egger et al., 1997). We considered a p value of >0.05 as evidence of significant publication bias. All analyses were performed on STATA version 10.1 (Stata/SE, College Station, TX).
Results
Literature search and study characteristics
Our initial search strategy yielded 2988 studies of which 2807 were unique (Fig. 1). After screening titles and abstracts, we removed 2751 studies and detailed screening of full text articles excluded another 43 studies leaving 13 potentially suitable studies for the meta-analysis. Of these, 9 were RCTs (Bilotta et al., 2007, 2008, 2009a; Bruno et al., 2008; Coester et al., 2010; Johnston et al., 2009; van den Berghe et al., 2005; Walters et al., 2006; Yang et al., 2009). We included only the 9 RCTs in this analysis. The study characteristics are presented in Table 1. All publications were recent (from 2005 to 2010) and were not limited to a specific region. A total of 1160 subjects were included in the meta-analysis. Mean age ranged from 37 to 75 years and the percentage of males ranged from 31% to 87%. Most studies reported a high percentage of patients with diabetes. Authors used different target ranges for IIT and defined hypoglycemia differently. Three studies reported on patients with severe TBI (Glasgow Coma Scale [GCS] score ≤8), three reported on patients with stroke, one reported exclusively on patients with aneurysmal subarachnoid hemorrhage, and two studies included patients with “brain injury” which comprised of all of the abovementioned patient populations.

Flow diagram: study selection process.
IIT, Intensive insulin therapy; CIT, Conventional insulin therapy; SAH, Subarachnoid hemorrhage; TBI, Traumatic brain injury; DM, Proportion of patients with diabetes at baseline; GCS, Glasgow Coma Scale; NA, Not applicable.
Outcomes
Five studies (total n=407) were included the analysis related to early mortality whereas eight studies (total n=1135) reported late mortality. The risk of both early and late mortality was not affected by treatment group; early mortality RR=1.04 (95% CI=0.75, 1.44) and late mortality RR=1.07 (95% CI=0.91, 1.27) (Figs. 2 and 3). No significant heterogeneity was found for either of the primary outcomes, with both having an I2 value of 0%. Eight studies (total n=1135) reported LTNO. As with mortality, the use of IIT did not have an effect on LTNO (Fig. 4) where the relative risk for “good” outcome was 1.10 (95% CI=0.96, 1.27). Again, no heterogeneity was discovered in the pooled studies (p=0.32 and I2=15%).
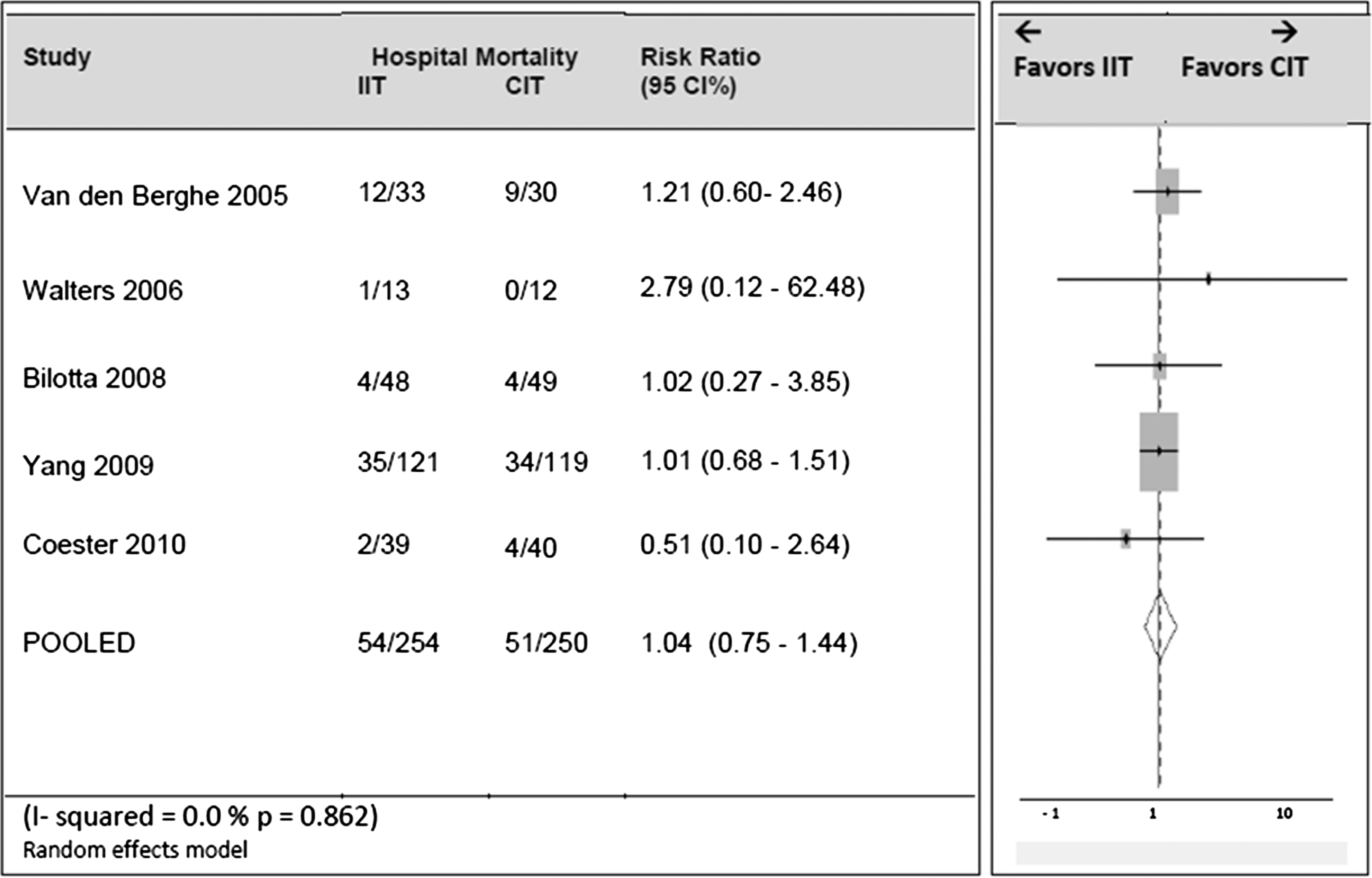
Forest plot with risk ratios and 95% CI of hospital mortality in randomized controlled trials comparing intensive insulin therapy (IIT) to conventional insulin therapy (CIT).
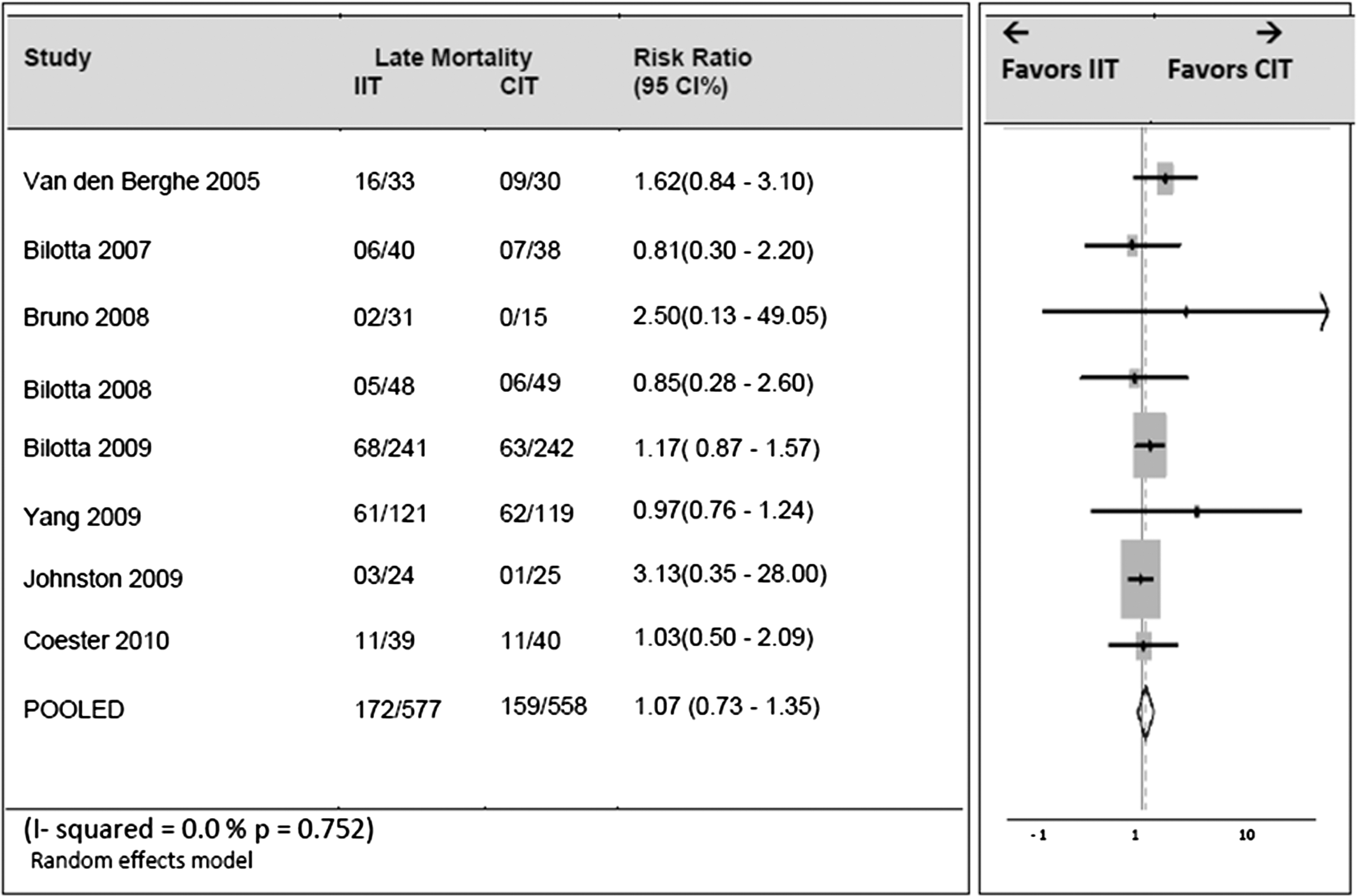
Forest plot with risk ratios and 95% CI of late mortality in randomized controlled trials comparing intensive insulin therapy (IIT) to conventional insulin therapy (CIT).
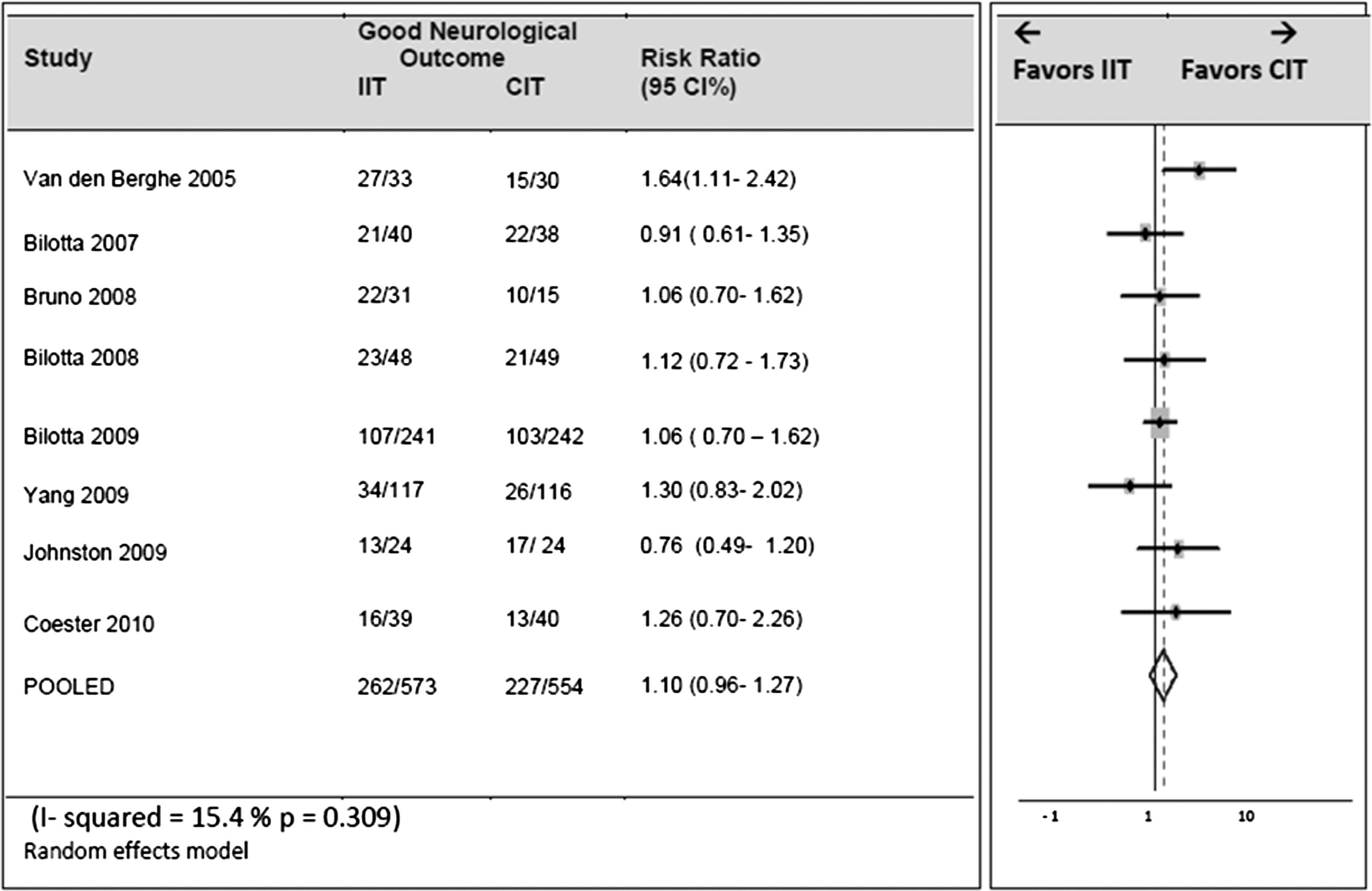
Forest plot with risk ratios and 95% CI of long-term neurological outcome in randomized controlled trials comparing intensive insulin therapy (IIT) to conventional insulin therapy (CIT).
Eight studies (total n=1082) reported number of hypoglycemic episodes. There were more hypoglycemic episodes in the IIT group; RR=1.72 (95% CI=1.20, 2.46) (Fig. 5). However, significant heterogeneity was found (p=<0.001, I2=89%). Meta-regression with the a priori variables demonstrated none of them to be significantly associated with the outcome. Sensitivity analysis by removing one study at a time did not decrease heterogeneity below 50%. We deemed this outcome to have intractable heterogeneity, and therefore its pooled effect estimate was determined to be inconclusive.

Forest plot with risk ratios and 95% CI of number of hypoglycemia episodes in randomized controlled trials comparing intensive insulin therapy (IIT) to conventional insulin therapy (CIT).
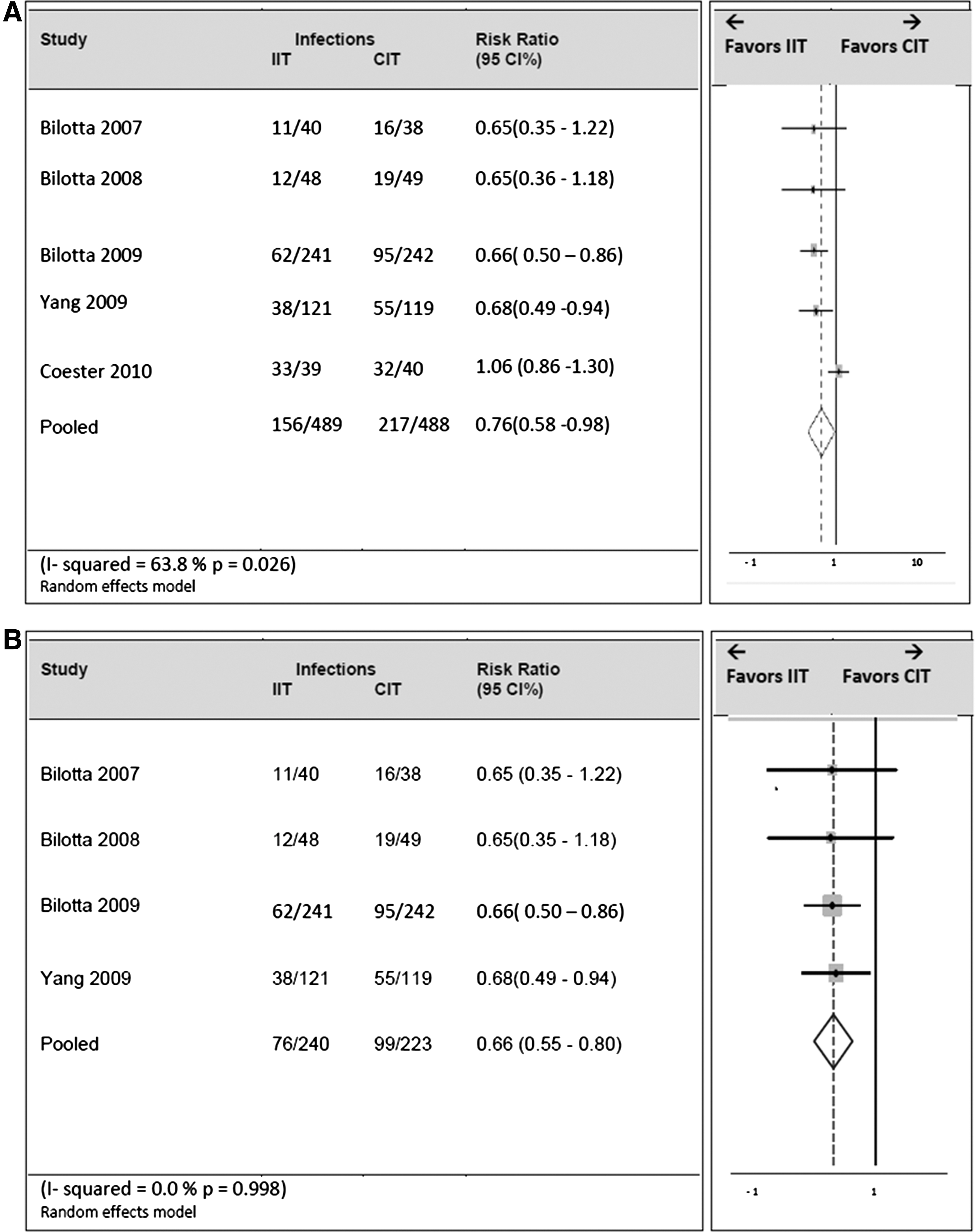
Infections were reported by five RCTs (total n=977). IIT had a protective effect against infection with a relative risk of 0.76 (95% CI=0.58–0.98) (Fig. 6). However, there was heterogeneity (I2=64%). Upon sensitivity analysis, removal of the study by Coester and coworkers eliminated the heterogeneity (I2=0%). A comparative inspection of each study identified the RCT by Coester and coworkers (Coester et al., 2010) to have a different patient population. It had a younger and predominately male population with a very low prevalence of diabetes compared to the other studies (Table 1). After the removal of the RCT by Coester and coworkers, the protective effect of IIT on infection increased in magnitude (RR=0.66, 95% CI=0.55, 0.80) (Fig. 6b).
We found no evidence of publication bias by means of Egger test (p=0.50) and visual inspection of the Egger plot for the outcome “late mortality” (Appendix 2). Most studies had a low risk of bias; however a few did have an unclear risk (Table 2). Across the studies, the risk of bias was assessed to be low.
SG, Sequence generation; AC, Allocation concealment; B, Blinding, IO, Incomplete outcome data; SO, Selective outcome reporting; OB, Other sources of bias; Y, Yes=low bias; N, No=high bias; U, Unclear; SAH, Subarachnoid hemorrhage; TBI, Traumatic brain injury; DNR, Do not resuscitate
Discussion
In this meta-analysis of brain injured patients, IIT did not demonstrate a mortality benefit nor did it improve LTNO when compared with CIT. However, we found a protective effect of IIT on the rate of overall infections.
Even though the RCTs differed with respect to type of brain injury and definition of IIT, no heterogeneity was demonstrated with respect to mortality. Both hospital mortality and long-term mortality (3-month or 6-month) were unaffected by IIT in all the RCTs. The mortality benefit of IIT in brain injury was unclear; however the effect in critically ill patients has been thoroughly researched. Since the landmark trial by van den Berghe in 2001, which demonstrated critically ill patients to benefit from IIT, a number of trials have had conflicting results (Griesdale et al., 2009; Marik and Preiser, 2009; van den Berghe et al., 2001; Wiener et al., 2008).
The NICE-SUGAR study, a recent multinational multicenter RCT consisting of 6104 patients in 42 ICUs across Australia, New Zealand, Canada, and the United States virtually brought an end to this discussion about the use of IIT in critically ill patients and actually demonstrated a harmful effect of IIT with an odds ratio of 1.14 (95% CI 1.02, 1.28) (Finfer et al., 2009). Meta-analyses by Wiener (Wiener et al., 2008) in 2008 and by Griesdale (Griesdale et al., 2009) and Marik (Marik and Preiser, 2009) in 2009 all demonstrated no difference in either in-hospital or long-term mortality among ICU patients with IIT. These discrepancies could be explained by methodological differences among studies that have different patient populations, glucose target ranges, feeding policies, and variable accuracy of tools used for glucose measurement and insulin infusion (Gunst and van den Berghe, 2010). Griesdale and coworkers in a subgroup analysis within their meta-analysis did demonstrate a benefit of IIT in patients admitted to surgical ICUs. As opposed to ICU patients in general, patients with brain injury seem to be uniformly unaffected by IIT as demonstrated in all nine trials in this meta-analysis. The NICE-SUGAR study was performed on critically ill adults admitted to the ICU with diagnoses other than those of our inclusion criteria, and was therefore not included in our analysis.
LTNO at 3 or 6 months was also unaffected by IIT. The RCT by van den Berghe (van den Berghe et al., 2005) was the only study that demonstrated significant favorable LTNO by IIT. However in this study, LTNO was measured at 12 months by a Karnofsky score as opposed to at 3 or 6 months mRS or GOS as in other studies. The adverse events related to hyperglycemia are well established (Bilotta et al., 2009b). Hyperglycemia is a known independent predictor of neurological outcome and mortality (Jeremitsky et al., 2005; Rovlias and Kotsou, 2000). It is associated with brain ischemia, inflammation, oxidative stress, lactic acidosis, imbalances between excitatory and inhibitory amino acids, and mitochondrial and endothelial dysfunction, which lead to neuronal damage and worse outcomes (Bilotta et al., 2009b). Reducing blood sugar levels in brain-injured patients is an established necessity. However the best way to do this remains unclear, and no guidelines exist for this purpose. Our analysis demonstrates comparable neurological outcomes with IIT and CIT.
A beneficial role of IIT was found in the rate of overall infections. Initially we found some heterogeneity, which after the removal of the RCT by Coester and coworkers became homogenous with an RR of 0.66. The RCT by Coester was in a Brazilian population of predominantly male subjects with a much lower mean age and almost none had diabetes (Coester et al., 2010). This corresponds to a number needed to treat of 7. One less patient will suffer an infection for every eight patients treated with IIT over CIT. This is a very similar estimate to Wiener and coworkers' meta-analysis in ICU patients, in which they found IIT to be associated with decreased risk of septicemia with an RR of 0.76 (95% CI 0.59, 0.97). Hyperglycemia has been associated with increased infections and length of stay (Bochicchio et al., 2007; Jeremitsky et al., 2005). Fewer infections may lead to a shorter length of hospital stay and therefore a decrease in overall cost of treatment. This may prove to be an important aspect of IIT and should be elucidated further. It may also be worthwhile to look at the effect of IIT on infections in a specific group of patients with encephalitis. The RCT by Bilotta in 2008 demonstrated a significantly reduced median ICU stay of 7.7 days in the IIT group as opposed to 10 days in the CIT group (Bilotta et al., 2008). Coester and coworkers, however, did not demonstrate a difference in the length of ICU stay (Coester et al., 2010). Our meta-analysis cannot provide conclusive evidence on the effect of IIT on the length of stay or on hospital costs. Because of the limited number of studies and the way infections were reported, we were unable to perform subgroup analysis regarding types of infections, which would have been interesting and should be studied further.
Hypoglycemic episodes have been a much feared effect of IIT. A recent multicenter RCT studying the effects of IIT versus CIT in critically ill patients was terminated before completion because of a higher number of hypoglycemic episodes in the IIT group (Brunkhorst et al., 2008). Almost all RCTs in our meta-analysis showed a higher number of hypoglycemic episodes with IIT among brain-injured patients. The larger trials, however, were closer to the null. There was a high degree of heterogeneity, with an I2 of 89%, which remained upon sensitivity analysis. Even though none of the a priori selected variables showed significance upon meta-regression, it is possible that hypoglycemic episodes vary by patient population or definition of hypoglycemia or other factors. Our meta-regression was limited by the number of RCTs available. The meta-analysis by Marik and Preiser demonstrated parenteral nutrition to be significantly associated with the outcome (Marik and Preiser, 2009). IIT was beneficial in trials in which a high number of calories were given, and harmful where a low percentage of calories were provided parenterally. We cannot draw conclusions about the effect of IIT on hypoglycemic episodes. As we found intractable heterogeneity, it is better not to pool the estimates of this outcome (O'Rourke and Detsky, 1989).
It is interesting to note that even though the number of hypoglycemic episodes may have been more in the IIT group, this did not lead to higher mortality or worse neurological outcomes. Hypoglycemia has been shown to have adverse effects on brain metabolism and cerebral perfusion leading to irreversible neuronal damage (Bilotta et al., 2009b). Recent evidence, however, suggests that it is the variability in blood glucose levels rather than the actual value that predicts outcomes (Egi and Bellomo, 2009). We were not able to analyze the effect of IIT on blood glucose variability in our analysis.
The studies used in our analysis used different definitions of IIT and of hypoglycemia and varied in patient characteristics and diagnosis. This variation provides a diverse group of patients, and as results for primary outcomes were homogenous, it adds strength to the current study. Further meta-analysis for each specific subgroup of patients would be interesting to look at once enough RCTs are conducted for robust analysis. We were, however, limited by the data available and were unable to determine the effect of IIT on important outcomes such as length of stay and glucose variability. Tools used to assess LTNO varied among studies and may be a potential limitation of this outcome, however, even though it is not ideal, we feel that dichotomizing the outcomes into “good” or “bad” addressed this issue fairly and provided us with a reasonable effect estimate. Additionally the meta-regression approach to determine heterogeneity in our population is limited by the small number of RCTs used. Some important factors might have been missed because of this lack of power.
This is the first systematic analysis of studies comparing IIT to CIT in brain-injured patients. Our analysis of current evidence suggests that IIT has no mortality or long-term neurological benefit in patients with brain injury. IIT does, however, have a protective role in decreasing the rate of infections. Because IIT does not improve upon the primary outcomes—mortality and neurological—it is not recommended for controlling hyperglycemia in patients with brain injury. CIT that targets glucose concentrations between 180 and 215 mg/dL (10-12 mmol/L) suffices.
Footnotes
Acknowledgments
We thank Drs. Karen Johnston, Edward Nemergut, Ariane Coester, Matthew Walters, Jose Raimundo, and Askiel Bruno for providing us with additional data required for our analyses. We also thank Drs. Chung Hsieh, Julie Goodman, and Russel de Souza for methodological advice.
Author Disclosure Statement
No competing financial interests exist.
Appendix 1: Search Terms
Appendix 2
*Publication bias has been tested using the outcome for long term mortality (this outcome included the highest number of RCTs n=7)