
Abstract
Precise assessment of motor deficits after traumatic spinal cord injury (SCI) in rodents is crucial for understanding the mechanisms of functional recovery and testing therapeutic approaches. Here we analyzed the applicability to a rat SCI model of an objective approach, the single-frame motion analysis, created and used for functional analysis in mice. Adult female Wistar rats were subjected to graded compression of the spinal cord. Recovery of locomotion was analyzed using video recordings of beam walking and inclined ladder climbing. Three out of four parameters used in mice appeared suitable: the foot-stepping angle (FSA) and the rump-height index (RHI), measured during beam walking, and for estimating paw placement and body weight support, respectively, and the number of correct ladder steps (CLS), assessing skilled limb movements. These parameters, similar to the Basso, Beattie, and Bresnahan (BBB) locomotor rating scores, correlated with lesion volume and showed significant differences between moderately and severely injured rats at 1–9 weeks after SCI. The beam parameters, but not CLS, correlated well with the BBB scores within ranges of poor and good locomotor abilities. FSA co-varied with RHI only in the severely impaired rats, while RHI and CLS were barely correlated. Our findings suggest that the numerical parameters estimate, as intended by design, predominantly different aspects of locomotion. The use of these objective measures combined with BBB rating provides a time- and cost-efficient opportunity for versatile and reliable functional evaluations in both severely and moderately impaired rats, combining clinical assessment with precise numerical measures.
Introduction
T
In contrast to all other methods, locomotor scoring, similarly to numerous clinical scales, gives the opportunity to assess locomotor functions in a fast and simple way without the need for training the animals or special equipment. The most commonly if not exclusively used scales in the last few years have been the Basso, Beattie, and Bresnahan (BBB) open-field locomotor rating scale for rats (Basso et al., 1995), and the Basso mouse scale (BMS) for mice (Basso et al., 2006). The BBB scale, based on observations of the pattern of locomotor recovery following thoracic contusion SCI in rats, consists of 22 points (scores) assessing joint movements, stepping, limb coordination, toe clearance, tail position, and trunk stability (Table 1). The range of the BBB scale includes the entire range of motor abilities, from normal gait (score 21) to complete paralysis of the hindlimbs (score 0). Although meaningful and useful, the BBB scale, like all ordinal scales, has disadvantages: the distinction of each category (score) is arbitrary, the assessment is subjective, and the scale is non-linear (i.e., an increase in the score, for example from 3 to 6, does not mean a two-fold improvement of locomotion). The BBB scale is well suited for analyses of rats with complete transection or contusions of various severities of the thoracic spinal cord (Basso et al., 1996; Kloos et al., 2005), but its sensitivity for other SCI models like cervical lesions is limited (Martinez et al., 2009; Webb and Muir, 2005; Zörner et al., 2010).
The table is reproduced from the original article without definitions. Highlighted in bold are attributes estimated by single-frame motion analysis parameters.
The message of the brief overview is that all widely used methods for locomotion analysis after SCI in rodents have advantages and limitations, and accordingly, it has been recommended that (1) a battery of measures appropriate for a specific type of injury and deficit should be used, and (2) objective numerical measures are preferable to ordinal data (Fouad and Pearson, 2004; Muir and Webb, 2000). Considering these recommendations, a novel approach, the single-frame motion analysis (SFMA), has been created for assessment of gait deficits after thoracic compression of the spinal cord in mice (Apostolova et al., 2006). The principles and implementation of this method, initially devised for and applied to mouse femoral nerve injury models (Irintchev et al., 2005), are simple. Mice are video recorded using a home-quality video camera during performance of tasks requiring no special training: walking on a runway (beam) towards their home cage, or catching the tip of a pencil with their hindlimbs while held by the tail. Using non-commercial software, single frames from the video sequences are selected to assess numerically, by measurements of angles and distances, specific aspects of body and limb movements in space: paw placement and body weight support during ground locomotion, which are essential components of the BBB scale, as well as target-reaching pursuits in space. Similarly to kinematics, the method provides quantitative information about limb and body movements. Unlike kinematics, the measurements are discontinuous (i.e., limited to defined phases of motion), and the approach demands no special knowledge or equipment. In addition, the battery of tests includes quantitative analysis of skilled locomotion using number of CLS as a measure, and assessment of locomotor abilities using the BBB or BMS rating scale as a functional clinical measure. The battery of tests in the described approach has proved useful and reliable in a series of studies on knockout mice and therapeutic interventions in wild-type mice (Apostolova et al., 2006; Chen et al., 2007, 2010; Jakovcevski et al., 2007; Lee et al., 2009; Mehanna et al., 2010). Considering the usefulness, simplicity, and reliability of the approach, here we tested its applicability to a rat SCI model. We compared functional loss and recovery over a 9-week post-operative observation period in rats with severe and moderate thoracic compression, and analyzed the relationships between different parameters and their dependence on the extent of tissue damage.
Methods
Animals
A total of 34 adult (175–200 g) female Wistar rats (strain Unilever HsdCpb:WU; Harlan Winkelmann, Borchen, Germany) were used. The rats were fed standard laboratory food (Ssniff, Soest, Germany), provided tap water ad libitum, and kept in a conditioned animal room (23°C, 12-hour artificial light-dark cycle). All experiments were conducted in accordance with the German Law on the Protection of Animals, and the procedures were approved by the local animal care committee. Ten rats were used in pilot experiments to optimize the spinal cord compression procedure and establish the methods for functional analysis. For the experiments reported here, 24 rats were trained to climb an inclined ladder for 2 weeks, and then subjected to either moderate or severe spinal cord compression (n=12 per group).
Spinal cord injury
Rats were anesthetized with 1.8 vol % isoflurane (Forene, Abbott, Germany) in 0.6 L/min O2 (Conoxia, Linde, Germany) and 1.2 L/min N2O, and laminectomy was performed at the T8 level under a surgical microscope. The exposed spinal cord was compressed with watchmaker's forceps (Dumont #5; Fine Science Tools, Heidelberg, Germany) closed by the drive pin of an electromagnet according to the method of Curtis and associates (1993; Fig. 1). The forceps and the electromagnetic drive were mounted on a metal block attached to a stereotaxic frame, which allows precise positioning of the forceps tips on both sides of the spinal cord without damage to the dura mater (Fig. 1A). The degree of closure of the forceps was controlled by a limiting pin passing through a hole drilled in the stationary blade of the forceps and advanced by a calibrated screw (Fig. 1B). Another calibrated screw controlled a closing pin used to manually advance the moving blade and thus measure cord diameter. The blades of the forceps were positioned on either side of the spinal cord and then carefully closed until they were adjacent to the dura. The blade distance was read from the calibrated screw, giving the diameter of the cord. The limiting pin was then introduced between the blades to restrict compression to 25% and 50% of the measured diameter for moderate and severe injury, respectively. The cord was compressed for 1 sec by timed current to the electromagnetic drive. The skin was then closed using 6-0 nylon sutures (Ethicon, Norderstedt, Germany). The operated rats were kept at 37°C for 12 h to prevent hypothermia. Afterwards, they were housed individually in standard cages and the bladders were voided manually twice daily. One animal with severe injury died 2 days after the operation. One rat with moderate injury showed very mild walking disabilities after the operation and was excluded from further observations.
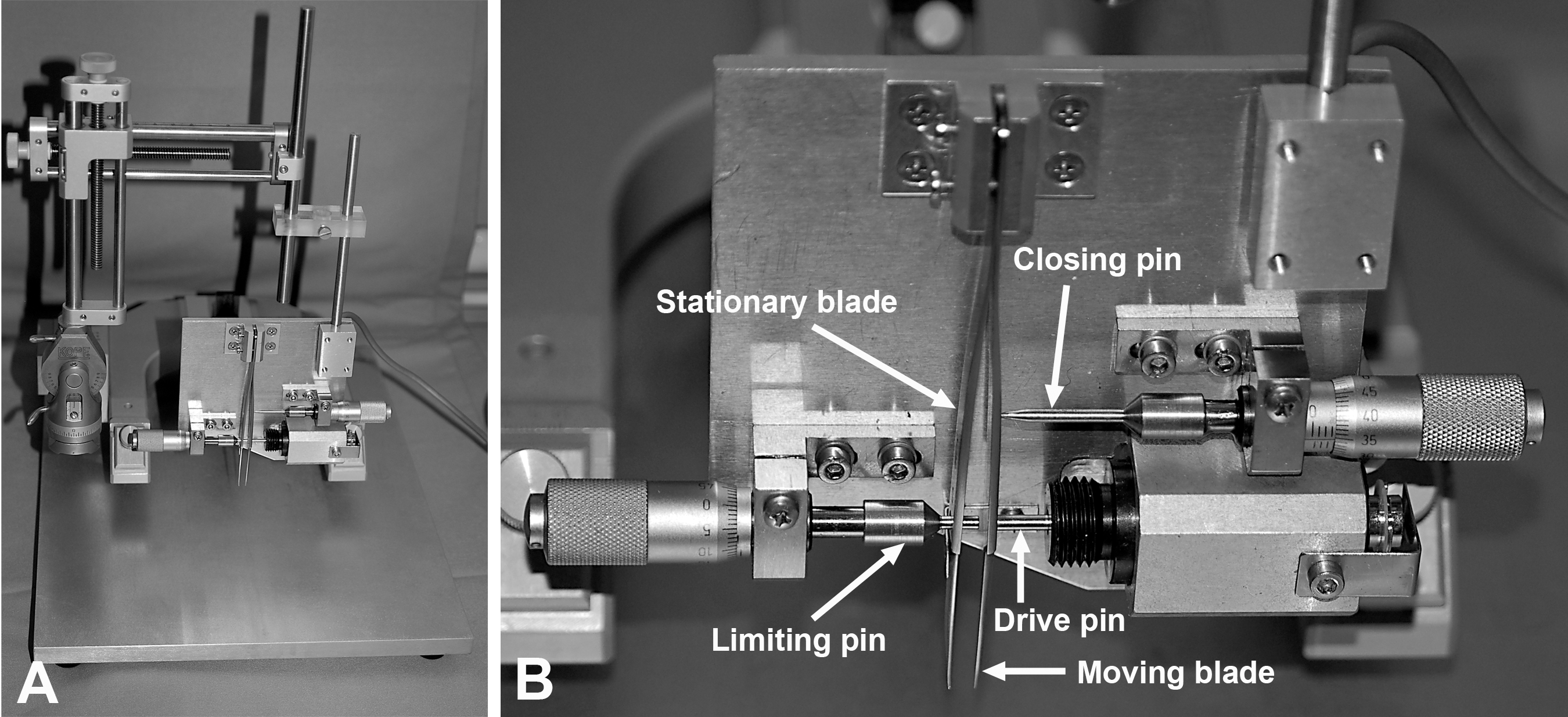
The spinal cord compression device (Curtis et al., 1993). (
Locomotor rating
Locomotor functions were evaluated using the Basso, Beattie, and Bresnahan (BBB) rating scale (Basso et al., 1995). Scoring was done by two independent investigators (S. Angelova and F. Wirth) using video recordings of beam walking (see below) observed at slow playback speed (Apostolova et al., 2006). Assessment was performed prior to injury (0 weeks) and 1, 3, 6, and 9 weeks after SCI. Scores for the left and right extremities were averaged. An advantage of the beam-walking test is that the animals perform many step cycles on the beam without motivators (see below). In contrast, rewards have to be used to stimulate movements of the animals in the classical open-field test (Basso, 2004). In addition, the close-view videos of the beam-walking trials allow precise visual examination, and thus evaluation of limb and body movements by the investigators. And, not least important in the context of this study, the use of beam walking for locomotor rating allows for functional evaluation using BBB scores and numerical parameters (see below) under the same test conditions.
Single-frame motion analysis (SFMA)
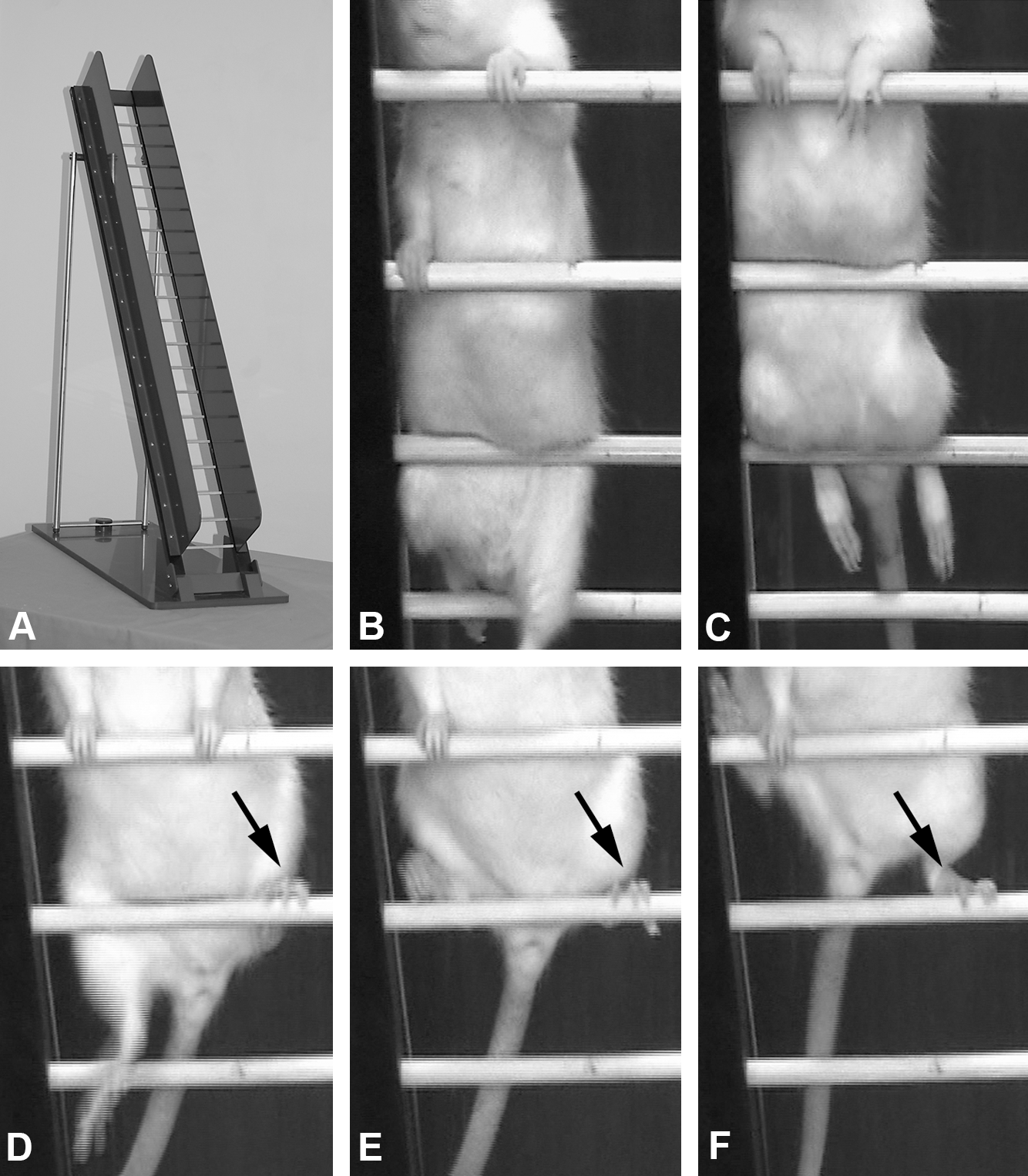
Locomotor tests were performed as described for mice with SCI (Apostolova et al., 2006) using a walking platform (“beam”, Fig. 2A), and an inclined ladder with dimensions adapted to the size of adult rats (Fig. 3A). The pilot experiments showed that rats, similarly to mice, readily perform the beam-walking test, in which the animals walk on the wooden platform towards their home cage (Fig. 2A). Unlike mice, most rats are reluctant to climb up an inclined ladder, and they were therefore trained for this test. Each training session was short (10–15 min per animal), and was performed 5 days/week for 2 weeks. For both tests, the only reward motivating the animals to perform the tasks was the return to the safe home cage.

Beam walking analysis. (
Ladder climbing test. (
Beam walking
The runway bar was made of a wooden plate (1500 mm long, 120 mm wide, and 20 mm thick) fixed on 200-mm-high feet (Fig. 2A). The rats were video recorded prior to SCI from the left and right side during beam walking with a video camera (Panasonic NV-DS12) at 25 frames per second. The video recordings were repeated 1, 3, 6, and 9 weeks after SCI. The animals were not trained to walk between recording sessions. Per time point and animal, at least two walking trials were recorded per side (left- and right-side views). The video sequences were examined using VirtualDub 1.6.19, a video capture/processing utility written by Avery Lee (free software available at
The FSA is the angle at which the hindpaw is placed on the ground at the beginning of the stance phase. The angle is defined by a line parallel to the dorsal surface of the paw and the horizontal line, and is measured using video frames in which the paw is seen in initial firm contact with the ground (Fig. 2B). In intact rats, the stance phase is well defined and the angle is smaller than 20° (Fig. 2B). After spinal cord injury, the rats drag behind their hindlimbs with dorsal paw surfaces facing the beam surface, and the angle is increased to 130°-140° (Fig. 2C). In severely disabled rats, “step cycles” were defined by the movements of the forelimbs. Video frames in which the angle appeared to have its lowest values for individual cycles, typically following a visible attempt to flex the extremity, were used for measurements. In less severely disabled rats, which performed stepping of variable quality (dorsal or plantar), the angle was measured upon dorsal or ventral placement of the paw on the ground after a swing phase or after a forward sweep of the paw over the beam surface. The FSA has been defined as an objective measure of stepping (plantar or dorsal), a major attribute in the BBB score (Table 1). Per time point of observation, 3 to 6 measurements were made for each hindlimb (i.e., 6 to 12 step cycles, defined according to the stepping ability of the animal as described above, were analyzed per animal). The values for the left and right paw of each animal were averaged. These analyses were performed by one investigator (J. Ankerne).
The RHI is defined as height of the rump (“a” in Fig. 2B and C), or the vertical distance from the dorsal aspect of the animal's tail base to the beam, normalized to the thickness of the beam measured along the same vertical line (“b” in Fig. 2B and C). For each animal and trial, the maximum RHI was estimated using video frames of 3 to 6 step cycles. The RHI is a numerical estimate of the ability to support body weight, an attribute in the BBB rating scale (Table 1).
Another parameter used previously for evaluation of non-weight bearing voluntary limb movements is the limb extension-flexion ratio (Apostolova et al., 2006). For measurements of this parameter, the animals have to perform a pencil test, in which they are held by the tail and allowed to grasp a pencil with its forepaws. As our preliminary experiments showed, rats would never perform the pencil test.
Ladder climbing test
After the beam-walking test, the rats were video recorded while climbing up an inclined ladder as described previously for spinal cord-injured mice (Apostolova et al., 2006). The rat ladder (Fig. 3A) is made of a plastic frame (1280 mm long, 190 mm wide, with a central dimension of 1200×120 mm), and has 19 round wooden rungs (6 mm in diameter) spaced at equal intervals (60 mm), and 150-mm-high side walls. The ladder is fixed in an inclined position (55°) using a plastic platform and metal feet. The rats were placed at the bottom rungs of the ladder and climbing was video recorded from a position below the ladder (i.e., viewing the ventral aspect of the animal; Fig. 3B–F). After initial training, the rats learned to climb up to the top of the ladder, and even severely disabled animals after SCI could do this using their forelimbs with the body weight support provided by the inclined position of the ladder. The video recordings were observed at slow-speed playback, and the CLS (correct placing of the hindpaw and sustained position until the next forward move; Fig. 3D and E) over 16 rungs were counted. These initial observations indicated that the ladder-climbing test could provide an opportunity for quantitative evaluation of complex motor behavior for the whole span of functional capabilities, from the non-injured state to complete paralysis. The ladder-climbing analyses were performed by one investigator (K. Wellmann).
Recovery indices
The recovery index (Apostolova et al., 2006; Irintchev et al., 2005) is an individual estimate of recovery for any given parameter and is calculated in percent as:
where Y0, Y1, and Y1+n are values prior to operation, 1 week after injury, and a time point n weeks after the first week, respectively. This measure estimates gain of function (Y1+n–Y1) as a fraction of the functional loss (Y0–Y1) induced by the injury. It may attain 0 or negative values if no improvement or further impairment occur during the observation time period. The index cannot be calculated if the injury causes no impairment [i.e., when (Y0–Y1) is 0]. Overall recovery indices can be calculated on an individual animal basis as means of recovery indices for individual parameters. The overall indices are more complex estimates of recovery than the individual parameters, and represent scores for individual animal performance based on objective assessment of different aspects of locomotion.
Histology and lesion volume estimation
Nine weeks after SCI all rats were deeply anesthetized with ether and perfused transcardially first with physiological saline for 30 sec, then with 4% formaldehyde in 0.1 M phosphate-buffered saline (PBS), pH 7.4, for 20 min. A spinal cord portion between vertebrae T7-T9 was dissected free. Following cryoprotection in 20% sucrose solution in PBS, longitudinal sections (25 μm thick) were cut on a cryostat and mounted on SuperFrost Plus slides.
According to the fractionator sampling strategy, each fifth longitudinal section (a total of at least 10 equidistant sections through the spinal cord) was used for staining with cresyl violet (Nissl stain). A Zeiss microscope equipped with a CCD Video Camera System (Optronics Engineering Model DEI-470, Goleta, CA, supplied by Visitron Systems, Puchheim, Germany), combined with the analyzing software Image-Pro Plus 6.2 (Media Cybernetics, Silver Spring, MD) was used to quantify the areas (in μm 2 ) of the lesions in each tissue section at a primary magnification of 2.5×. The volume was calculated according to the Cavalieri method (Gundersen and Jensen, 1987; Gundersen et al., 1988; West and Gundersen, 1990). Measurements were performed by two observers (J. Ankerne and M. Ashrafi), who were blinded to the treatment of the animals.
Statistical analysis
Statistical analyses were performed using Sigma Plot 11 software (SPSS, Chicago, IL). Data were analyzed for distribution and equal variance and appropriate parametric or non-parametric tests were used. Correlation analyses were performed with the Spearman test. The threshold value for acceptance of differences was 5%. Details of the statistical methods used are given in the text and figure legends. Data are presented as scatterplots or mean values with standard errors of the mean (SEM).
Results
Functional recovery after severe and moderate SCI estimated by BBB rating and SFMA
We first analyzed locomotor functions in rats with severe or moderate SCI using the BBB rating scale. At 1 week after SCI, the mean BBB score of severely injured rats was 1.2 (range 0–4, normal value 21). In functional terms, this means that the hindlimbs were completely paralyzed, or could slightly to moderately be moved in 1–3 joints (Table 1). During the following weeks, a statistically significant improvement was observed in these rats (Fig. 4A). From a functional point of view, however, the improvement was minor. At 9 weeks, the average BBB score reached 4.4 (range 1–9). Only 2 out of 11 animals could occasionally perform plantar stepping (score 9, Table 1) meaning that as a whole, this group did not regain functionally meaningful walking abilities. The rats moved along the beam using the forelimbs while the hindlimbs were dragged behind, and movements in hindlimb joints did not support the forward movement in a significant way.
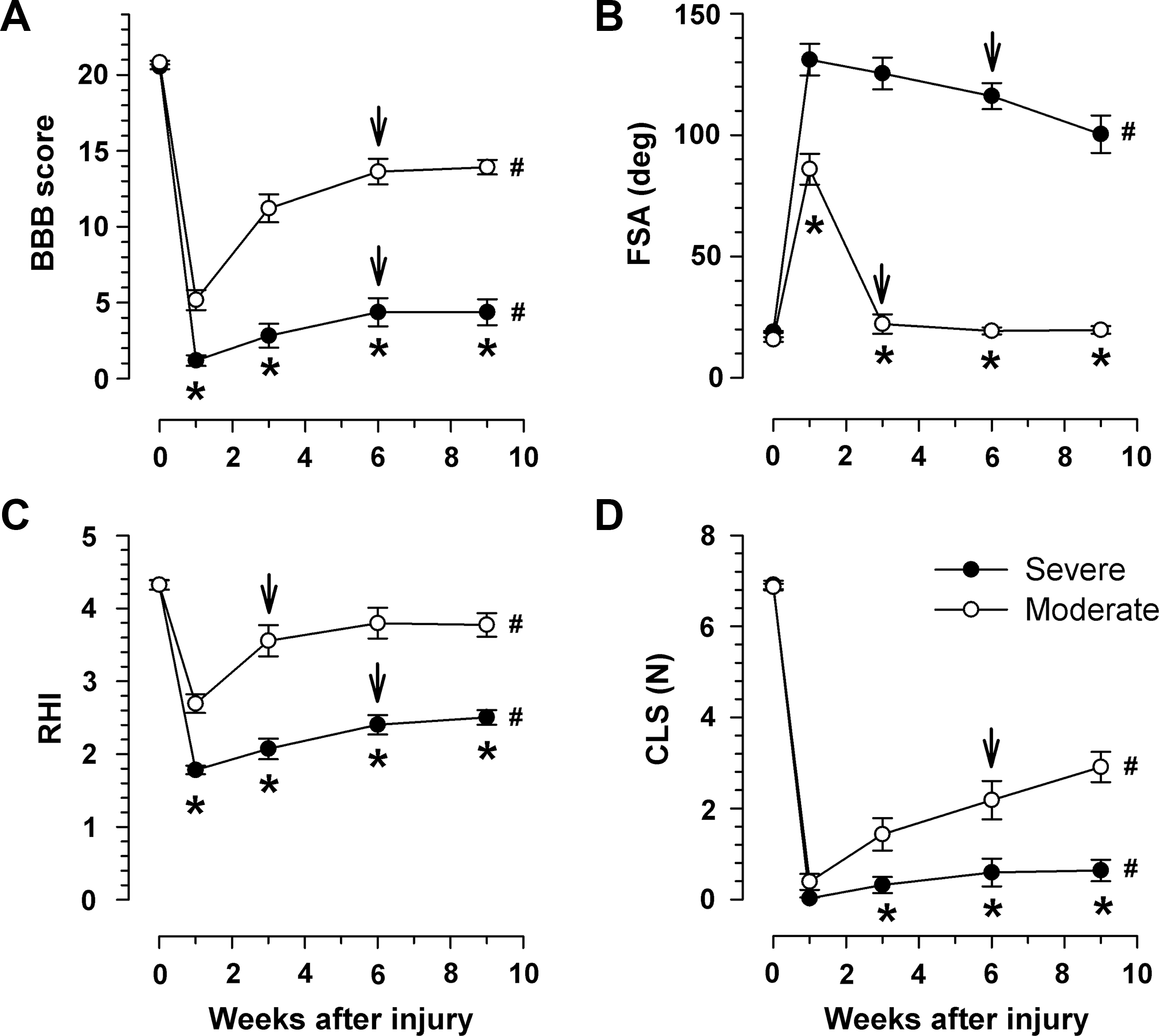
Time course and degree of functional recovery after severe and moderate spinal cord injury (SCI). Shown are mean values±standard error of the mean (SEM; n=11 per group) of locomotor rating scores (Basso, Beattie, and Bresnahan [BBB];
After moderate SCI, the rats were less impaired at 1 week (mean score 5.2, range 2–8), and showed better performance at all later time points compared with severe injury (Fig. 4A). At 9 weeks, the mean scores for moderately-injured rats reached 14 (range 12–16). This means that these animals were capable of consistent plantar stepping and forelimb-hindlimb coordination (i.e., the rats could walk, even if specific fine aspects of locomotion like toe-clearance, paw and tail position, and trunk stability were not normalized; Table 1). Maximum recovery in moderately-injured rats, similarly to severely-injured animals, was reached at 6 weeks after SCI (arrows in Fig 4A; see the figure legend for definition of maximum recovery).
Analysis of stepping using the foot-stepping angle (FSA) revealed, similarly to the BBB scores, significantly different degrees of impairment in the two groups 1 week after SCI (Fig. 4B). In the severely-injured group, the angle changed from an average of about 20° prior to injury to 130° at 1 week, and only gradually and slightly decreased thereafter, to a minimum of 100° at 9 weeks. Angles larger than 90° indicate that the toes or the dorsal paw surface rather than the plantar surface touched the ground during ground locomotion (Fig. 2C). Therefore, the conclusion that can be drawn from the FSA results for the severely-injured rats is that the animals did not recover plantar stepping within the 9-week observation time period. After moderate SCI, the angle increased, as compared with non-injured rats, to about 90° at 1 week, and abruptly returned to normal at 3 weeks after SCI. These results show that between 1 and 3 weeks the pattern of stepping changed from dorsal to plantar, which represents a substantial functional improvement.
The second SFMA parameter, the RHI, estimates the ability of the hindlimbs to support body weight during ground locomotion. This ability was significantly, and to different degrees, impaired 1 week after severe and moderate SCI compared with intact animals (Fig. 4C). As for the BBB scores, the index increased after the first week in both groups, but remained significantly below normal values throughout the observation time period. Maximum recovery was achieved by 6 and 3 weeks in the moderately- and severely-injured groups, respectively.
The third SFMA parameter was the number of CLS. Proper placement of the paws and maintenance of a stable position of the paw on the rungs to support body weight during climbing (Fig. 3D–F) require higher levels of motor and sensory control than overground locomotion. In accordance with this notion, the estimates for the two animal groups using this parameter differed from the estimates of walking (BBB, FSA, and RHI). We found, in contrast to the other measures, no difference between severely- and moderately-injured rats at 1 week (Fig. 4D). At that time point, virtually no animal was able to step on the ladder rungs (Fig. 3B and C). This did not improve in the severely-injured rats until the end of the observation time period. In the moderately-injured group, similarly to RHI, the CLS gradually increased with time and maximum recovery was reached at 6 weeks.
From these observations we can conclude that all 4 parameters used can detect functional differences between moderately- and severely-injured rats. Differences in the assessment of impairment and recovery among the parameters suggest that these measures estimate different aspects of locomotion in a partially overlapping or non-overlapping fashion.
Correlations between functional parameters and scar volume
We next addressed the question of whether the functional differences between the two experimental groups were due to different extents of tissue damage. We estimated total lesion volume using cresyl violet-stained sections of spinal cords (Fig. 5A) and the Cavalieri principle. In support of our expectation, we found that the lesion volume at 9 weeks after SCI was almost twice as large in severely- as in moderately-injured rats (6.2±0.50 versus 3.3±0.29 mm3, n=8 per group, p=0.002 by two-sided t-test). Regression analyses revealed significant correlations between the functional estimates at 9 weeks and lesion volume (Fig. 5B–E). The BBB scores and CLS correlated positively, and the RHI and FSA correlated negatively with the lesion volume. For BBB and FSA, the coefficients of determination (r2) were 0.69 and 0.72 (Fig. 5B and C), indicating that about 70% of the variability in these estimates could be explained by variability in lesion volume. Highly significant also were the correlation coefficients for the RHI and CLS (r2=0.51 and 0.49, respectively, Fig. 5D and E). The overall conclusion from these results is that all functional parameters were correlated with the extent of tissue damage induced by the spinal cord compression.

Correlations between functional parameters and lesion volume 9 weeks after spinal cord injury (SCI). Lesion volume was estimated from spaced-serial sections (
Correlations between functional parameters
We were further interested whether and what kind of correlations existed between different functional parameters. Analyses using data from all animals (severely and moderately injured) at 9 weeks after SCI showed significant co-variations for all pairs of parameters (Fig. 6A–F). All regression models were non-linear, and the visual impression from the scatterplots was that of different degrees of co-variations within ranges of high and low disability. We analyzed the correlations between FSA, RHI, and CLS on the one hand, and BBB scores on the other hand, separately for the severe- and moderate-injury groups (Fig. 6A–C). We found significant negative correlations between the FSA and BBB scores for both groups of animals (Fig. 6A). Both the slope and the correlation coefficient for the moderate SCI group were lower than those for severe injury (-2.3 and 0.69 versus −8.0 and 0.89, respectively). This means that within the low score range (<10), FSA rapidly declines as BBB increases (by 8° per point), while this decline is less pronounced in the lower range (BBB score >10, 2.3°/point). The results for the RHI showed an inverse trend compared with the foot-stepping angle (Fig. 6B). The slope of the regression line and the correlation coefficient for moderately-injured rats were higher than those of severely-injured rats (0.25 and 0.67 versus 0.06 and 0.56, respectively). These results indicate that the FSA and the RHI change relative to the BBB scores at different rates within different ranges of functional impairment. Although a significant co-variation was indicated by the overall correlation coefficient for CLS and BBB scores, no correlations between the two groups of rats were found when analyzed separately (Fig. 6C). Thus, although the CLS generally increased as walking improved, the relationship between the two parameters was relatively weak. Similarly to the correlations with BBB scores, we analyzed the co-variations between SFMA parameters. For both RHI and CLS, we found correlations with the FSA for severely-, but not for moderately-injured rats (Fig. 6D and E). No within-group correlations were found between CLS and RHI (Fig. 6F). These results suggest that the three SFMA parameters predominantly estimate different aspects of locomotion.
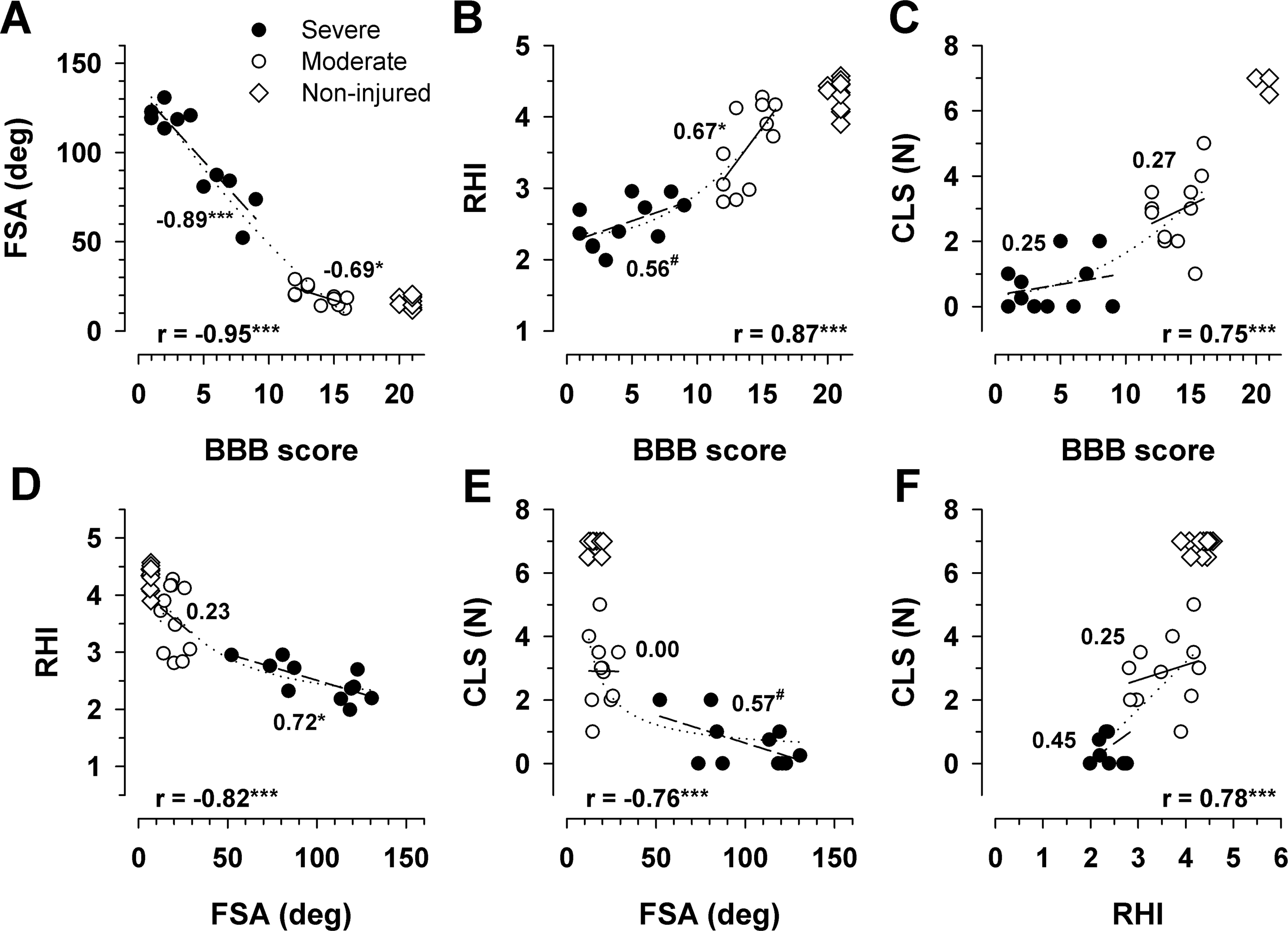
Correlations between functional parameters 9 weeks after spinal cord injury (SCI). Scatterplots of individual values (n=11 per group) with coefficients of correlation (r at the x-axes) calculated for all values (severe and moderate). The numbers adjacent to the groups of solid and open symbols indicate correlation coefficients calculated separately for severely- and moderately-injured rats, respectively. Shown are also regression lines for the whole population, and for severely-injured and for moderately-injured rats (dotted, dashed, and solid lines, respectively; # p<0.10, *p<0.05, ***p<0.001). The pre-operative values (non-injured) of the rats in the moderate injury group are plotted as reference for normal values and were not included in the correlation analyses (FSA, foot-stepping angle; RHI, rump-height index; CLS, correct ladder steps).
Comparisons of parameters using normalized values
We also made within-group comparisons between the SFMA parameters and BBB scores using recovery indices (RI, Fig. 7). The recovery index is an individual measure normalizing gain of function after the first week to loss of function between 0 and 1 week (Fig. 7A). Comparisons of indices at 3, 6, and 9 weeks after moderate SCI showed significant differences between all pairs of parameters at any given time point (Fig. 7B). At 9 weeks, a high degree of recovery was achieved for the FSA (95%), moderate recovery for the BBB scores and the RHI (56% and 66%, respectively), and recovery was lowest for CLS (42%). The conclusion from these results is that the 4 parameters show different outcomes after moderate SCI in the same animal group. For severely-injured rats, generally no differences between the outcome measures were found (Fig. 7C). The lack of between-measure differences in this group was due the o overall low degree of recovery, reaching a maximum of 10–28% at 9 weeks.
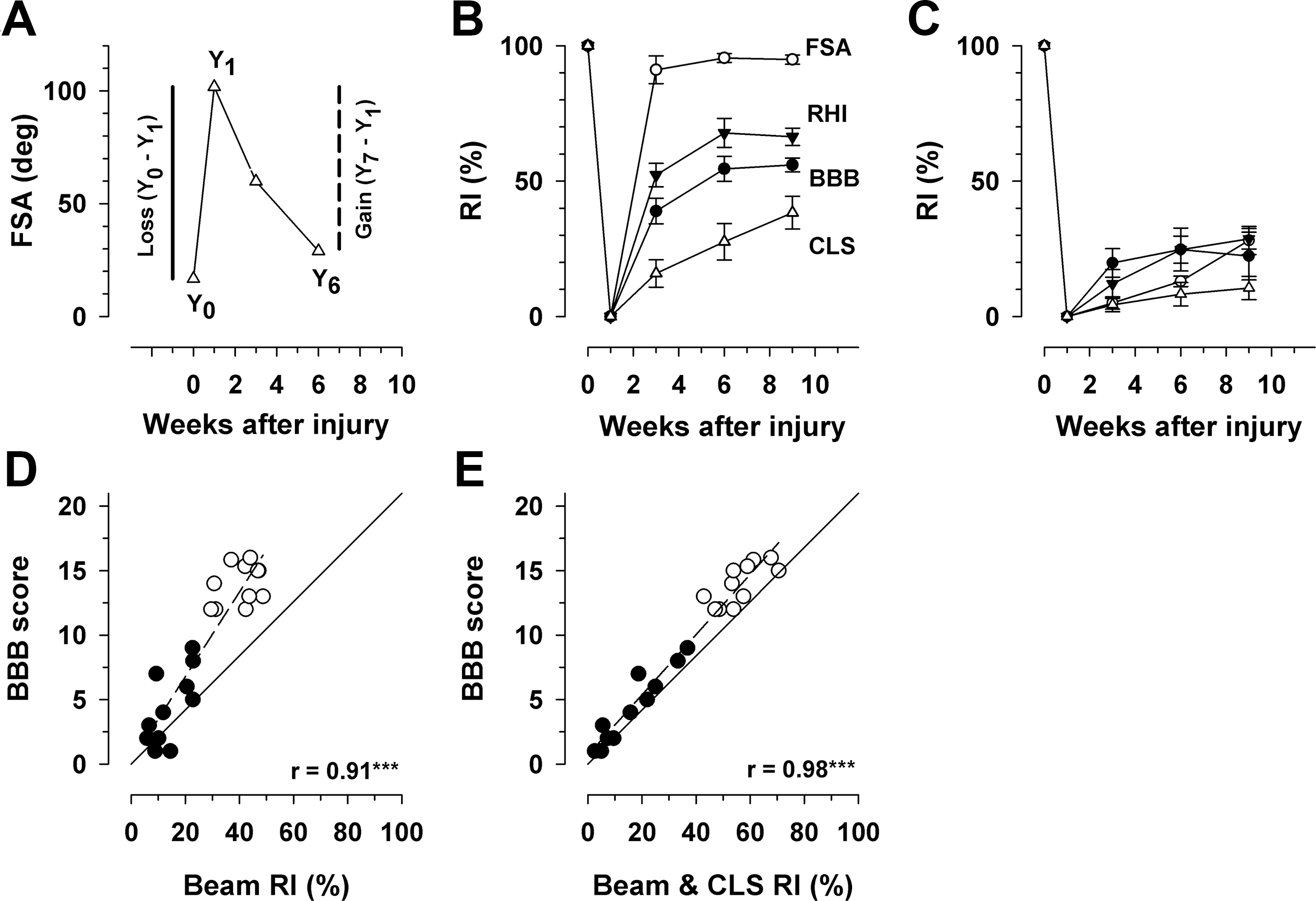
Comparisons of parameters using recovery indices. (
The recovery indices also allow calculations of more complex measures, overall indices based on numerical parameters. Thus the average of the indices for the FSA and the RHI gives an overall estimate of beam-walking recovery (“Beam RI” in Fig. 7D). Plots of this index against BBB scores of severely- and moderately-injured rats at 9 weeks showed a very good correlation (r=0.91, Fig. 7B). A more complex recovery index including all 3 SFMA parameters, the “Beam & CLS RI,” was best correlated with the BBB scores (r=0.98, Fig. 7E). In contrast to the non-linear correlations seen between SFMA parameters and BBB scores (Fig. 6A–C), the correlations between the overall indices and BBB scores were linear within the whole range of values (i.e., including both severely- and moderately-injured rats; Fig. 7D and E). Thus, including different outcome measures in an overall index increases the agreement between numerical estimates and BBB ratings. However, this agreement is not that of 1-to-1 measures, as is evident from the deviations of the regression lines seen in Figure 7D and E, which is the line of ideal agreement connecting the points at which the two parameters have their lowest and highest possible values (score 0 versus RI 0%, and score 21 versus RI 100%).
Discussion
Here we show that the SFMA is well suited for locomotor analysis of rats with SCI. Similarly to the BBB rating, the SFMA parameters allow us to detect motor impairments ranging from normal walking capabilities to complete paralysis. The degree of impairment and time course of recovery estimated in the same group of animals differed among the parameters. These differences could be expected, since the SFMA measures provide objective numerical data on individual, defined aspects of locomotion.
The first impression from the comparisons between severely- and moderately-injured rats (Fig. 4) is that any one of the parameters used is sufficient to substantiate the conclusion that the graded compression has produced two different levels of motor incapability. This is generally true, but the use of the battery of measures provides the opportunity for a more reliable and comprehensive analysis of the motor deficits. For severely-injured rats, the average BBB scores showed that the animals were almost completely paralyzed at 1 week, and recovery, reaching a maximum at 6 weeks, was restricted to enhanced movements in hindlimb joints without restoration of body weight support and plantar stepping (Fig. 4A and Table 1). The FSA verified that plantar stepping was not restored; despite improvement after the first week post-injury, the angles remained larger than 100° up to the ninth week, meaning that the paws were placed dorsally (Figs. 2C and 4B). Despite a lack of true stepping, with time after injury the movements of the hindlimbs became sufficient to lift the trunk to about a quarter of the original rump height (Figs. 4C and 7C). Finally, the rats were unable to step on the ladder rungs at 1 week after injury, and no improvement occurred up to the ninth week (Fig. 4D).
The usefulness of different measures for the interpretation of motor deficits is also apparent when the results for the moderately-injured group are considered. The animals reached, on average, a score of 14 on the BBB scale at 6–9 weeks after SCI (Fig. 4A). The interpretation of this outcome is not immediately comprehensive because this category (score 14) is defined in a complex way (Table 1). Generally, the BBB result suggested that the gait of the animals was characterized by frequent to consistent plantar stepping with body weight support, and frequent to consistent forelimb-hindlimb coordination. The FSA measurements confirmed, in a precise numerical way, that the animals completely recovered plantar stepping at 3 weeks post-lesion (Fig. 4B). The RHI showed that the rump height reached about 60% of the original level, meaning that the ability to support body weight recovered to a significant degree (Fig. 4C). Finally, in a parallel to improvement of overground locomotion, with time after injury the rats significantly improved stepping during ladder climbing (Fig. 4D).
From the above considerations it becomes apparent that each of the individual parameters supports and supplements the other measures in a meaningful way. This is important, because on the one hand, the numerical parameters estimate individual attributes of locomotion. The FSA estimates only paw placement, and the RHI measures body weight support. Both attributes are essential components of the BBB scale (Table 1), and their numerical estimates correlate well with the BBB scores (Fig. 6A and B). However, the overall assessment of the walking abilities using these two parameters deviates from the BBB scoring (Fig. 7B and D). Such a deviation is expected, considering that the BBB scale includes, in addition to stepping and body weight support, other attributes (toe clearance and position and forelimb-hindlimb coordination) that have increasingly stronger influence on the rating as locomotion improves (Table 1). On the other hand, general measures like locomotor scores may assess different degrees of changes in individual aspects of locomotion (Basso, 2004). This notion is supported by data on the effects of gene mutations or treatments on the outcome of spinal cord compression in mice as assessed by rating scores and SFMA parameters (Table 2). These studies have shown that, as estimated by BBB rating, mice deficient in the expression of the extracellular matrix molecule tenascin-R (TNR-/- mice, Apostolova et al., 2006), or the cell recognition molecule close homologue of L1, CHL1 (CHL-/- mice, Jakovcevski et al., 2007), recover better from compression SCI compared with wild-type littermates (TNR+/+ and CHL1+/+ mice, respectively). Better outcome by BMS rating has also been found in C57BL/6 mice treated with a polysialic acid (PSA) peptide mimetic compared with control peptide-treated mice. In good agreement with the rating, the FSA and the overall RI indicate significant improvement in all three cases. However, in contrast to the stepping ability (FSA), body weight support was better than in control mice only in CHL1-/- mice. The ability of non-weight-bearing limb movements as measured by the pencil test with the extension-flexion ratio (EFR) is improved in CHL1-/- and PSA-treated, but not TNR-/- mice.
Summary of results from studies of mice with spinal cord injury (SCI) using the combination of rating and single-frame motion analysis (SFMA).
FSA, foot-stepping angle; RHI, rump-height index; EFR, extension-flexion ratio; RI, recovery index; TNR-/- and TNR+/+, tenascin-R-deficient and wild-type mice, respectively; CHL1-/- and CHL1+/+, close homologue of L1-deficient and wild-type mice, respectively; PSA, polysialic acid;↑, better function;=, no difference.
Finally, in none of the cases was improvement seen in precise locomotion as measured by correct stepping during ladder climbing. These examples clearly demonstrate an advantage of the SFMA approach. The numerical parameters estimate distinct aspects of motion controlled by different neural circuits. This allows, by combining the functional analysis with quantitative histology, one to search for the neural substrates, for example synaptic inputs to motoneurons or monoaminergic innervation of the lumbar spinal cord, that affect specific functional outcomes (Apostolova et al., 2006; Jakovcevski et al., 2007; Lee et al., 2009).
The SFMA approach has several characteristics that meet the requirements for a useful behavioral test in SCI research (Basso, 2004; Fouad and Pearson, 2004; Muir and Webb, 2000). The estimates are quantitative (objective), and theoretically are more sensitive than semi-quantitative end-point measures. Each parameter estimates a distinct aspect of locomotion, providing the opportunity to search for neural substrates of specific behaviors. The use of normalized values allows more complex estimates of motor abilities by recovery indices than with individual parameters, numerical scores for overall performance. The method can be generalized as shown here by adapting the approach used for SCI mice to rats. The method is standardized in that the conditions and phases of locomotion used for the analyses are well defined, and previous work with mice has demonstrated the reproducibility of the approach. In contrast to other quantitative approaches like kinematic and kinetic measurements (Muir and Webb, 2000; Murray et al., 2004), and gait analysis using the CatWalk system (Hamers et al., 2006; Koopmans et al., 2005), the SFMA tests are simple, and require cheap equipment and no specific knowledge or training of personnel. More importantly, with the exception of SFMA, all quantitative methods require a relatively high level of motor abilities of the animals, including consistent stepping, which preludes their use in studies of severely impaired animals. One important limitation of the SFMA approach is that it does not measure limb coordination, an important aspect of locomotion and recovery after SCI (Basso, 2004; Koopmans et al., 2005).
In conclusion, the objective measures used in this study allow estimations of motor functions in rats over the whole range of deficits seen after SCI, from normal overground locomotion and ladder climbing to complete paralysis. The SFMA approach provides reliable and versatile measures that can be performed in any laboratory, and is well supplemented by BBB ratings. In cases of moderate motor impairments that allow consistent stepping, its addition to the currently used battery of tests to measure coordination as assessed by simple walking track analysis (de Medinaceli et al., 1982), or the sophisticated CatWalk gait analysis system, appears reasonable.
Footnotes
Acknowledgments
This study was financially supported by the Forschungsförderungsprogramm Köln Fortune of the Medical Faculty University of Cologne, and by the Jean-Uhrmacher-Foundation.
Author Disclosure Statement
No competing financial interests exist.