
Abstract
Craniotomy has been accepted as the treatment of choice for the management of acute epidural hematomas (AEDH). However, in practice, it seems possible to evacuate AEDH via a single burr hole instead of the traditional craniotomy in certain circumstances. Among 160 patients with AEDH meeting criteria for evacuation admitted to the emergency and accident division of our center between 2006 and 2009, we found 8 cases of hematoma appearing isodense to brain parenchyma on computed tomography (CT), who had concomitant coagulopathy. These patients were managed by burr-hole drainage for treatment of the liquefied AEDH. A closed drainage system was then kept in the epidural space for 3 days. In all 8 patients, AEDH was evacuated successfully via burr-hole placement over the site of hematoma. The level of consciousness and other symptoms improved within the first day, and no patient required an additional routine craniotomy. For patients with slowly-developing AEDH in the context of impaired coagulation, burr-hole evacuation and drainage might be a less invasive method of treatment compared to conventional craniotomy.
Introduction
C
In practice, it is possible to evacuate AEDH via a single burr hole instead of the traditional craniotomy technique under certain conditions. In such a situation, the hematoma should be fairly liquefied rather than clotted, and able to flow out of the burr hole. Most often, this form of hematoma does not develop from tearing of dural arteries or sinuses, but are caused by gradual oozing from venous injury or dural surface stripping.
In this series we report 8 cases of AEDH with concomitant coagulopathy who were managed by a single burr-hole evacuation technique.
Methods
Among 160 patients with AEDH meeting the criteria for evacuation admitted to the emergency and accident division of our center between 2006 and 2009, we found 8 cases of hematoma appearing isodense to brain parenchyma on computed tomography (CT) associated with some form of coagulopathy. These included 5 males and 3 females, with the age ranging from 3 to 22 years (mean 11.5 years). All 8 cases had a history of head injury due to fall or direct impact. Admission Glasgow Coma Scale (GCS) scores ranged from 12 to 15. Three patients had post-traumatic loss of consciousness, 5 had nausea and vomiting, and 1 developed seizure. All patients complained of severe headache. The mean interval between trauma and obtaining brain CT was 5.5 h. There were 3 cases of skull fracture, though none were depressed fracture. In evaluating lab tests, all 8 patients had coagulopathy; 1 had dysfibrinogenemia, 2 had hemophilia (including one female carrier), 1 had von Willebrand disease, and impaired prothrombin time (PT) or bleeding time (BT) was seen in 4 patients.
Patient data are summarized in Table 1. We chose the candidates for burr-hole drainage on the basis of (Cordobés et al., 1981) density of the hematoma on CT (i.e., isodense to brain parenchyma), and (Greenberg J, et al., 1985) presence of some form of coagulopathy to assume that the hematoma was liquefied. The patients were operated as soon as possible to ensure the most favorable outcome. Hematoma size, pupillary status, and the amount of midline shift were not used in the selection process as inclusion or exclusion criteria for the evacuation technique mentioned.
This patient had a ventriculoperitoneal shunt for hydrocephalus since childhood.
GCS; Glasgow Coma Scale; PT, prothrombin time; INR, International Normalized Ratio; LOC, loss of consciousness; TT, thrombin time; BT, bleeding time (Duke method); vWD, von Willebrand disease.
Method
All cases of AEDH had been first evaluated for primary life support measures, neurological status, and lab tests. If needed, the patients were intubated and appropriate medications were prescribed. Platelets, intravenous vitamin K, and fresh frozen plasma or coagulation factors were administered as necessary to correct the underlying coagulopathy. Those with AEDH of more than 1 cm thickness, midline shift of greater than 0.5 cm, neurological deficit, or decreased level of consciousness accompanied with mass effect were assessed for urgent surgical intervention. In those with isodense AEDH and coagulopathy, under general anesthesia and in appropriate position and prep (for the switch to craniotomy if required), a 2.5-cm skin incision was made over the site of the greatest diameter of the hematoma, preferably on the fracture site. A burr hole (15 mm diameter) was then made to see if the liquefied hematoma exited completely so that the dura came in contact with the inner table of the skull, or if the clot could not be totally evacuated, necessitating a conventional craniotomy. In the former situation, closed vacuum drainage was placed over the epidural space, and the skin was closed with 2 or 3 stitches. The drainage system was removed after the bleeding stopped and when CT revealed resolution of the hematoma (in all cases by day 3).
Follow-up assessment was performed with regular neurological examination and CT on days 1 and 3 (usually before removing the drainage tube), and whenever necessary.
Results
In all 8 patients, AEDH was evacuated successfully via burr-hole placement over the site of the hematoma, and the dura adhered to the bone after evacuation of the hematoma. The level of consciousness and other symptoms improved within the first day after surgery. No patient required an additional routine craniotomy. All patients were at normal functional level at discharge (Glasgow Outcome Scale score 1).
The hematoma was located in the supratentorial region in 6 patients (Fig. 1), and in the posterior fossa in 2 other cases (Fig. 2). None of the supratentorial hematomas was in the temporal area, or in the vicinity of the foramen spinosum or the branches of the middle meningeal artery. During the surgical procedures, neither active bleeding nor bleeding from a torn artery was observed.

A 3-year boy with a history of dysfibrinogenemia presented with lethargy, headache, vomiting, and seizure 4 h after a fall down a staircase. (
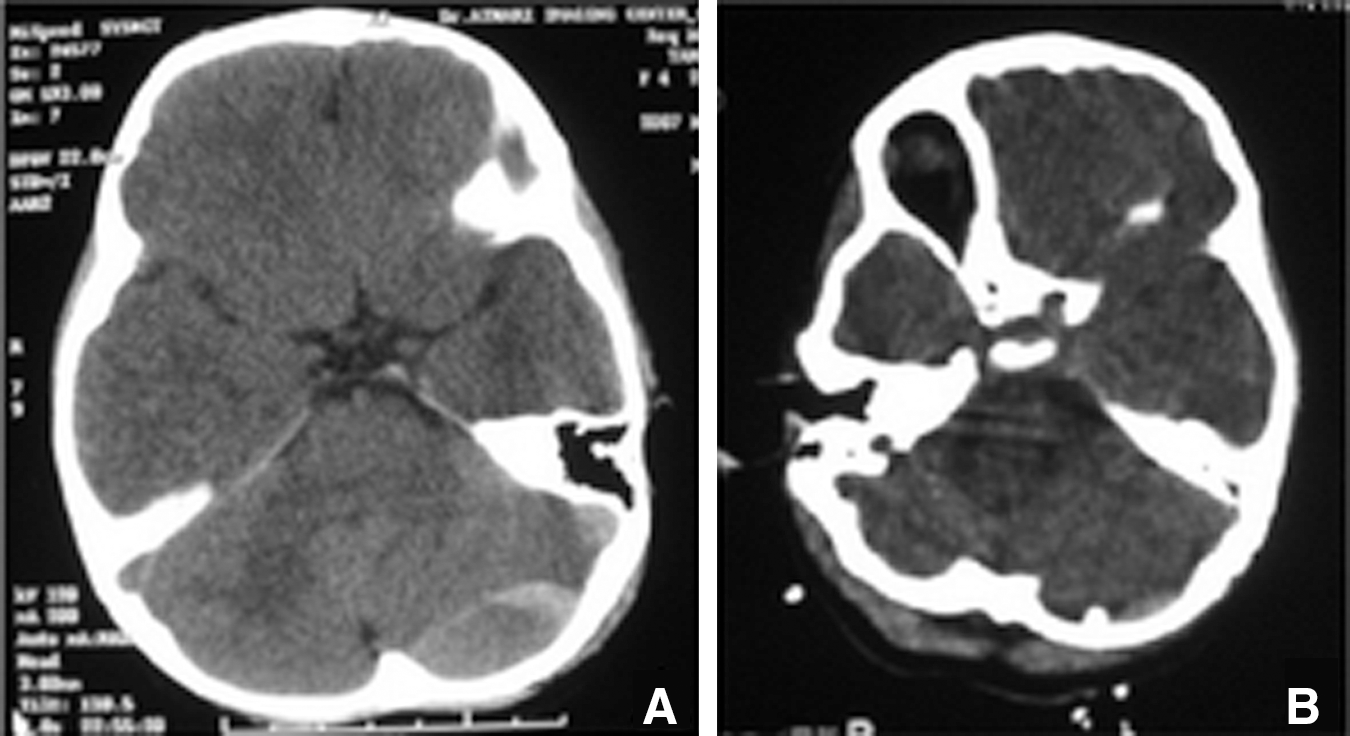
A 4-year girl was admitted with drowsiness and severe headache 8 h after a direct impact head trauma. (
Follow-up brain CT on the first and third post-operative days revealed no re-accumulation or residual hematoma. The closed drainage system was kept in place for 3 days in all cases, and was removed after no residual hematoma or mass effect was seen on brain CT scans (Figs. 1 and 2). None of the patients developed surgical complications such as wound infection and collection, or further neurological problems. One patient who had a preoperative seizure experienced status epilepticus after surgery, which was managed with anticonvulsants according to the standard protocol, and had no other episodes of seizure were seen in long-term follow-up.
Discussion
The decision to perform a surgery in a patient with a traumatic extra-axial hematoma is dependent on neurosurgical judgment (Tallon et al., 2008). Radiological and neurological indications for surgical treatment of an extra-axial hematoma consist of: supratentorial lesions of at least 1 cm thickness, containing more than 30 mL of blood, presence of mass effect with a decline in the level of consciousness, and development of new focal neurological signs (Prabhu et al., 2004). Patients with AEDHs who meet surgical criteria and receive prompt surgical treatment can have an excellent prognosis, presumably owing to limited underlying primary brain damage (Tallon et al., 2008). Prompt evacuation of the clot through a craniotomy, with tenting of the dura to the bone edges, is the accepted method for the treatment of pure traumatic AEDH following closed head injury (Liu et al., 2006). In certain emergency situations, an alternative method for rapid and effective hematoma evacuation can be of considerable value to save the patient's life and achieve good functional outcomes.
Use of burr holes in the surgical management of traumatic brain injury
Rapid placement of a single burr hole can be used in certain circumstances in the management of acute brain trauma; for example, in case of a rapidly enlarging temporal AEDH of arterial source that jeopardizes the patient's life, placement of a burr hole over the temporal region can save the patient's life while the surgeon completes the craniotomy for hematoma evacuation (Paci et al., 2009). Exploratory burr holes, once used frequently, are now employed to a lesser extent, because lesions can be rapidly identified through CT imaging (Cordobés et al., 1981).
Minimally invasive techniques in the management of traumatic brain injury
A small number of minimally invasive methods have been reported in the literature for the management of AEDH in certain circumstances. As neonatal epidural hematoma (EDH) is more liquefied than the adult counterpart, and it is amenable to needle aspiration under transcranial ultrasound guidance for a massive EDH seen following vacuum-assisted delivery (Noguchi et al., 2005). Also, aspirating a cephalhematoma to evacuate a communicating epidural hematoma in a newborn infant with no neurological signs has been successfully employed to avoid more invasive surgical intervention (Smets and Vanhauwaert, 2010).
In a pilot study, a novel method of urokinase instillation using a closed suction drain has been proposed for post-craniotomy epidural hematoma as a feasible method with no complications and better outcomes (Park et al., 2008). Drilling the skull with instillation of urokinase into the hematoma space has been reported in 22 cases of traumatic EDH in another series (Liu et al., 2008).
In a clinical series, 11 of 13 patients harboring traumatic EDH were successfully treated by placement of a flexible tube through a burr hole, followed by continuous suction under negative pressure, and only two cases required secondary traditional craniotomy (Liu et al., 2006). The authors of this article emphasized the slow-developing nature of the hematoma from a non-arterial source as a means of selecting cases for this approach.
Venous versus arterial bleeding
It should noted that cases of AEDH of non-arterial origin differ from the more common arterial subtype in terms of nature, location, surgical planning, and outcome (Yilmazlar et al., 2005; Suzuki et al., 2004). Non-arterial AEDH should be suspected if preoperative CT scans show the hematoma over a venous sinus or over the posterior fossa convexity, with the sinus-origin group tending to be more associated with skull fracture (Yilmazlar et al., 2005). Non-arterial AEDH should be suspected if a preoperative CT scan shows the hematoma over a venous source. It may be hypothesized that bleeding through the epidural space from a venous source is more readily controllable by the tamponade effect of an enlarging brain, effacing the dura to the undersurface of the bleeding fractured calvaria. Since the clinical course during the pre-surgical period was relatively benign in our patients (according to their GCS scores), and the mean interval from the traumatic head impact to the diagnosis of AEDH was 5.5 h, it could be assumed that the hematomas evolved rather slowly (presumably of venous origin; diploic or meningeal) compared to a more typical rapidly-growing arterial AEDH, which can cause rapid clinical deterioration.
The role of coagulopathy
In the current series, eight cases of traumatic EDH with hematomas appearing isodense to the brain parenchyma on CT scans with some kind of coagulopathy were managed by burr-hole placement followed by closed drainage. The hematomas were evacuated successfully in all patients, and the level of consciousness and pupillary size (if impaired) returned to normal post-operatively. The coagulopathy problem, which was present in all cases, can be a helpful prerequisite for the success of this proposed minimally-invasive approach. Despite the fact that it normally takes 5–15 min for blood to clot (appearing as a hyperdense mass on CT; Greenberg et al., 1985), brain CTs obtained in our patients after a mean interval of 5.5 h after trauma revealed the hematomas to be isodense to the brain parenchyma, implying incomplete clot formation. Surgical observation disclosed that the liquefied blood completely exited from the burr hole with no evidence of dense clot formation. Furthermore, in patients with coagulopathy and a higher risk of intraoperative bleeding, which may be more difficult to control during a routine craniotomy, the less invasive burr-hole evacuation method can be advantageous by causing fewer intraoperative hemorrhagic complications. For patients in this category, burr-hole evacuation and drainage might constitute a more feasible, faster, and safer method of treatment.
Limitations of the burr-hole method
The described method has some restrictions. For instance, this procedure is unlikely to be effective in controlling a major source of arterial or sinus bleeding. In our series, no arterial bleeding was observed in the surgical site, and there was no depressed fracture overlying a major sinus. The neurological deficits seen in our patients were relatively benign as assessed by admission GCS scores (ranging from 12–15), and the average interval was 5.5 h from the impact to the time of radiological diagnosis. It seems that such a technique would not be useful in cases of rapid clinical deterioration, as is the case in those with AEDH having a major arterial source who require immediate surgical control. This result is in accord with that of Liu and colleagues, who held that this method is less efficient when the source of bleeding is from the foramen spinosum, and that those with slowly-developing hematomas are better candidates for this technique (Liu et al., 2006).
Conclusions
Considering their medical background, the epidural hematomas described here did not develop from tearing of dural arteries or sinuses, and were instead caused by gradual oozing from venous injury or dural surface stripping. Therefore, it seems that for patients with slowly-developing EDH in the context of impaired coagulation (i.e., liquefied hematomas), our proposed technique of burr-hole drainage might constitute a less invasive and therefore safer method of treatment compared to conventional craniotomy. Indeed, such a conclusion requires further evaluation in studies with larger sample sizes along with controls.
Footnotes
Author Disclosure Statement
No competing financial interests exist.