
Abstract
Oxidative stress is a major contributor to the secondary injury process after experimental traumatic brain injury (TBI). The importance of oxidative stress in the pathobiology of human TBI is largely unknown. The F2-isoprostane 8-iso-prostaglandin F2α (8-iso-PGF2α), synthesized in vivo through non-enzymatic free radical catalyzed peroxidation of arachidonic acid, is a widely used biomarker of oxidative stress in multiple disease states, including TBI and cerebral ischemia/reperfusion. Our hypothesis is that harvesting of biomarkers directly in the injured brain by cerebral microdialysis (MD) is advantageous because of its high spatial and temporal resolution compared to blood or cerebrospinal fluid sampling. The aim of this study was to test the feasibility of measuring 8-iso-PGF2α in MD, ventricular cerebrospinal fluid (vCSF), and plasma samples collected from patients with severe TBI, and to compare the MD signals with MD-glycerol, implicated as a biomarker of oxidative stress, as well as MD-glutamate, a biomarker of excitotoxicity. Six patients (4 men, 2 women) were included in the study, three of whom had a focal/mixed TBI, and three a diffuse axonal injury (DAI). Following the bedside analysis of routine MD biomarkers (glucose, lactate:pyruvate ratio, glycerol, and glutamate), two 12-h MD samples per day were used to analyze 8-iso-PGF2α from 24 h up to 8 days post-injury. The interstitial levels of 8-iso-PGF2α were markedly higher than the levels obtained from plasma and vCSF (p<0.05), supporting our hypothesis. The MD-8-iso-PGF2α levels correlated strongly (p<0.05) with MD-glycerol and MD-glutamate, which are widely used biomarkers of membrane phospholipid degradation/oxidative stress and excitotoxicity, respectively. This study demonstrates the feasibility of analyzing 8-iso-PGF2α in MD samples from the human brain. Our results support a close relationship between oxidative stress and excitotoxicity following human TBI. MD-8-iso-PGF2α in combination with MD-glycerol may be useful biomarkers of oxidative stress in the neurointensive care setting.
Introduction
T
ROS/RNS can be defined as an oxygen/nitrogen species with one or more unpaired electrons (Freeman and Crapo, 1982), including the superoxide (O2 •−), hydroxyl radical (OH•) and nitric oxide (NO•). Superoxide (O2 •−) is generated via normal cell metabolism (Zalba et al., 2007), and this physiological ROS production is effectively balanced by the endogenous scavenger systems, including mitochondrial manganese superoxide dismutase (Mn-SOD), intra- and extracellular copper/zinc superoxide dismutase (Cu/Zn-SOD), catalase, and glutathione (Halliwell, 2006).
Following acute brain injury including TBI and ischemic stroke, numerous mechanisms including intracellular Ca2+ overload, inhibition of the mitochondrial respiratory chain, release of arachidonic acid from membrane phospholipids, and accumulation of hypoxanthine lead to the overproduction of superoxide (Bayir and Kagan, 2008; Fiskum et al., 1999). Superoxide is not considered harmful, but may readily react with nitric oxide (NO•) to form peroxynitrite (ONOO−) or dismutate to hydrogen peroxide, which reacts with iron to form hydroxyl radicals (OH•), with the capacity to damage cells by lipid peroxidation, protein oxidation, and DNA damage.
Isoprostanes are synthesized in vivo mainly via non-enzymatic, free radical-catalyzed peroxidation of arachidonic acid (Morrow et al., 1990). One of the most studied isoprostanes, 8-iso-prostaglandin F2α (8-iso-PGF2α; molecular weight 454.5 Da), is overproduced in diverse disorders such as atherosclerosis, rheumatoid arthritis, hypertension, and Alzheimer's disease, all of which are associated with oxidative stress (Basu, 2008; Morrow et al., 1992). 8-iso-PGF2α measured in blood or cerebrospinal fluid (CSF) has been implicated as a useful marker of oxidative stress in cerebral ischemia/reperfusion in a porcine cardiac arrest model and in cardiac arrest patients (Basu et al., 2000; Wiklund et al., 2005), as well as in CSF of human pediatric and adult TBI patients (Bayir et al., 2002,2004).
Oxidative stress following TBI is thought to be closely associated with excitotoxicity (i.e., glutamate-mediated intracellular accumulation of Ca2+), leading to membrane phospholipid degradation and the formation of arachidonic acid (for references see Hillered et al., 2005). Another end product of this phospholipid degradation process is glycerol (Clausen et al., 2005; Hillered et al., 2005; Marklund et al., 1997; Nguyen et al., 2007), which has also been implicated as a biomarker of oxidative stress (Clausen et al., 2005; Lewen and Hillered, 1998; Merenda et al., 2008). Another potentially important link between oxidative stress and excitotoxicity is the microglial antiporter system Xc
Microdialysis (MD) is the only bedside monitoring tool that can evaluate, hour-by hour, the focal neurochemistry of the injured human brain, and is being used as a clinically relevant monitoring method in neurointensive care units (neuro-ICUs) worldwide (Goodman and Robertson, 2009; Hillered et al., 2006; Tisdall and Smith, 2006). Our basic hypothesis is that harvesting of biomarkers directly in the injured brain tissue provides chemical signals with a better temporal and spatial resolution, and also avoids biomarker degradation, compared to conventional CSF or blood sampling methods (Liu et al., 2010; Marklund et al., 2009). Although other techniques such as gas chromatography/mass spectrometry (GC/MS), liquid chromatography/mass spectrometry (LC-MS), and enzyme immunoassay (EIA) have been used to measure isoprostanes in a variety of compartments (Basu, 2008), we chose to quantify 8-iso-PGF2α in the MD samples with a radioimmunoassay (RIA) previously developed and characterized within the group (Basu, 1998).
The aims of the present study were to: (1) explore the feasibility of measuring 8-iso-PGF2α in cerebral MD samples from neuro-ICU patients with severe TBI, (2) to compare 8-iso-PGF2α levels in the cerebral interstitial compartment (MD) with vCSF and blood, and (3) to study the relationship between MD-8-iso-PGF2α and MD-glycerol as well as MD-glutamate, widely used biomarkers of membrane phospholipid degradation/oxidative stress and excitotoxicity, respectively.
Methods
All research procedures described herein were approved by the Regional Ethical Review Board at Uppsala University and informed consent was obtained from the patient's closest relative.
Patients
Six patients with severe TBI arriving to the Uppsala University Hospital Neuro-ICU with a motor component of the Glasgow Coma Scale (GCS, Teasdale and Jennett, 1974) of 3–5, corresponding to a Reaction Level Scale (RLS) score of 3–6 (Stalhammar et al., 1988) were included in the present study (Table 1). All patients were mechanically ventilated and following admission to our unit, an intracranial pressure (ICP) monitoring device was inserted, and evacuation of significant mass lesions was immediately performed when needed. Three patients were classified as a focal/mixed TBI, and three patients a diffuse axonal injury (DAI), according to CT criteria (Marshall et al., 1992). All patients were treated in the neuro-ICU using an ICP-guided protocol with mild hyperventilation (partial carbon dioxide pressure [Pa
This patient fell and sustained a severe TBI due to a ruptured aneurysm.
Computed tomography (CT) characteristics using the worst CT scan during the neuro-ICU stay (Servadei et al., 2000) according to the Marshall classification (Marshall et al., 1992).
+, ++, and +++ is a semiquantitative scale indicating the degree of subarachnoid blood; RF-crt, right frontal, inserted via craniotomy; cx, contusion; GMS, motor component of the Glasgow Coma Scale; RLS, Reaction Level Scale; eGOS, extended Glasgow Outcome Scale; M, male; F, female; MVA, motor vehicle accident; RF, right frontal; LF, left frontal; N/A, data missing; fx, fracture; Pneumothx, pneumothorax; Th, Thoracic; tSAH, traumatic subarachnoid hemorrhage; IVH, intraventricular hemorrhage; DI2, diffuse injury 2; BF, bifrontal; SDH, subdural hematoma; EML, evacuated mass lesion; EDH, epidural hematoma; Ccx, cortical contusion; Bil. Syl, bilateral Sylvian fissure; LSyl, left Sylvian fissure; Bcist, basal cisterns; MD, microdialysis; NA, not applicable; 0, normal; 1, compressed yet visible; 2, compressed; BF, bifrontal; LT, left temporal; LFP, left frontoparietal; TBI, traumatic brain injury.
Microdialysis and bedside biomarkers in the neuro-ICU
Intracerebral MD was initiated, in conjunction with the insertion of an ICP monitoring device, through MD catheters inserted via a burr hole (n=5), 1–2 cm anterior to the coronal suture, or in the pericontusional tissue following craniectomy for the removal of a mass lesion (n=1). In all patients care was taken to insert the MD catheter obliquely into the cortex using a non-traumatic technique to achieve a position with the major part of the membrane surface within the gray matter. This was confirmed by evaluating the CT scans of each patient. Theoretically this positioning should enable the MD catheter tip to follow the movements of the brain without further tissue damage. Figure 1 shows the MD probe and ICP monitor probe in patient 2. We used CMA-71 MD catheters with a membrane length of 10 mm and a 100-kDa nominal molecular weight cut-off polyarylethersulfone (PAES) membrane (CMA Microdialysis, Stockholm, Sweden). The outflow hydrostatic pressure of the perfusion system was set at the zero mid-cranial reference level by taping the collecting vials at the bandage on the patient's head to avoid additional hydrostatic effects on fluid recovery of the catheter (Hillman et al., 2005). Perfusion of the catheters was performed using artificial CSF (Perfusion Fluid CNS; CMA Microdialysis), containing 147 mM NaCl, 2.7 mM KCl, 1.2 mM CaCl2, and 0.85 mM MgCl2, at a rate of 0.3 μL/min using a CMA106 microinjection pump (CMA Microdialysis). The rationale for using this perfusion fluid was the data from Hutchinson and associates (Hutchinson et al., 2005), showing similar in vivo extraction efficiency for small molecules with the CMA-71 compared with the CMA-70 (20-kDa cutoff ) catheter. At least 2 h passed after insertion of the probe and the start of sampling, to allow for normalization of changes due to probe insertion. MD samples (approximately 18 μL) were obtained hourly and analyzed bedside for glucose, lactate, pyruvate, and urea, with an enzymatic colorimetric technique on a CMA 600 Microdialysis Analyser (CMA Microdialysis). The lactate/pyruvate (L/P) ratio was calculated. Urea was monitored to control the probe performance (Ronne-Engstrom et al., 2001). After bedside analysis, the remaining samples were stored on ice for up to 12 h in the neuro-ICU, and then at −20°C for up to 7 days, pending analysis of glutamate and glycerol on a CMA 600. The remaining samples were stored at −70°C until further analyzed for isoprostane.

A computed tomography (CT) scan image from patient 2 confirming the location of the microdialysis (MD) catheter. Arrow A points to the intracranial pressure monitor, and arrow B at the MD catheter.
The CMA 600 Analyser was automatically calibrated when started, as well as every sixth hour, using standard calibration solutions from the manufacturer (CMA Microdialysis). Quality controls at two different concentrations for each substance were performed every weekday. Imprecision values for between-assay coefficient of variation was <10% for all analytes.
Blood, ventricular cerebrospinal fluid, and urine sampling
Arterial plasma (heparin), vCSF, and urine samples were collected simultaneously on a daily basis following morning rounds, normally between 11
Radioimmunoassay of 8-iso-PGF2α
MD, plasma, CSF, and urine samples were analyzed for 8-iso-PGF2α by an RIA as previously described (Basu, 1998). To achieve a sample size sufficient for the analysis of 8-iso-PGF2α the microdialysate samples from 12 consecutive hours were pooled. The cross-reactivities of the 8-iso-PGF2α antibody with 15-keto-13,14-dihydro-8-iso-PGF2α, 8-iso-PGF2α, PGF2α, 15-keto-PGF2α, 15-keto-13,14-dihydro-PGF2α, TXB2, 11β-PGF2α, 9β-PGF2α, and 8-iso-PGF3α, were 1.7, 9.8, 1.1, 0.01, 0.01, 0.1, 0.03, 1.8 and 0.6%, respectively. The detection limit was 23 pmol/L (8 pg/mL).
The levels of 8-iso-PGF2α in urine samples were used as a methodological control to verify a reasonable urinary output compared to published reference data (Basu, 2008), since to our knowledge there are no published reference data for 8-iso-PGF2α in MD samples from the human brain. Therefore, only the average urinary level of the patient group is presented in the text, while the primary interest was focused on the MD, vCSF, and blood levels in the illustrations.
Statistical methods
Statistical analyses were made using Statistica® software (StatSoft, Tulsa, OK). The hourly measurements of lactate, pyruvate, glutamate, glucose, and glycerol were averaged for the 12 h corresponding to the pooled sample used for 8-iso-PGF2α analysis. Medians of 8-iso-PGF2α and the routine biomarkers from each patient were subjected to weighted non-parametric correlation analysis (Spearman Rank correlation), for which the weight was determined by the number of samples from each patient. Samples from vCSF, plasma, and urine were matched to the corresponding pooled MD samples so that the 12-h MD sampling period started at least 3 h before snap sample collection. Data were analyzed statistically using non-parametric tests (Kruskal-Wallis analysis of variance [ANOVA], followed by Mann-Whitney U tests). All MD data are presented as dialysate concentrations without correction for in vivo recovery.
Results
Patients
The mean age of the patients was 37±22 years (range 15–67 years), and there were four male and two female patients. The clinical and radiological characteristics for each patient are shown in Table 1.
Microdialysis and bedside biomarkers in the neuro-ICU
Microdialysis was started at a mean of 19.5±3.6 h after injury, and the average duration of sampling was 97±45 h. The critical values considered in this study were glucose<1.0 mmol/L; L/P ratio>40; lactate>3.8 mmol/L; pyruvate<120 μmol/L; glutamate>15 μmol/L; and glycerol>100 μmol/L, based on published data and our own experience (Reinstrup et al., 2000; Schulz et al., 2000). Five out of six patients had consistently high lactate concentrations during the monitoring period (patients 2–6). Two of the six patients had glutamate concentrations within the normal range (patients 1 and 4). Three patients (patients 3, 5, and 6) had initially high concentrations of glutamate, which abated over time, and one patient initially had a normal concentration of glutamate, which was then markedly increased at ∼50 h post-TBI (patient 2). Three patients (patients 4, 5, and 6) had initially high concentrations of glycerol (>100 μmol/L), that normalized over time, two had initially normal concentrations that increased over time to markedly elevated levels (>100 μmol/L; patients 2 and 3), and one had normal concentrations throughout the monitoring period (patient 1).
8-iso-PGF2α concentrations in interstitial fluid, CSF, plasma, and urine
In the plasma and vCSF, 8-iso-PGF2α levels were low, reaching 134.6±56 pmol/L and 135.2±69 pmol/L, respectively (Fig. 2). In the urine, 8-iso-PGF2α levels reached 701±280 pmol/L (not shown) when corrected for creatinine (Sjogren et al., 2005). The level of 8-iso-PGF2α was significantly higher in the MD samples (1057±326 pmol/L) compared to CSF and plasma (p<0.05; Fig. 2). The MD 8-iso-PGF2α levels decreased over time in three patients. Two patients showed high concentrations throughout the sample collection (>1500 pmol/L), and one patient had a concentration consistently at approximately 800 pmol/L (Fig. 3).

Concentrations of 8-iso-PGF2α in different compartments, presented as the median value, quartiles, and non-outlier range. The microdialysis (MD) samples showed significantly higher concentrations of 8-iso-PGF2α (marked with an asterisk; p<0.05) than plasma and cerebrospinal fluid (CSF; 8-iso-PGF2α, F2-isoprostane 8-iso-prostaglandin F2α).
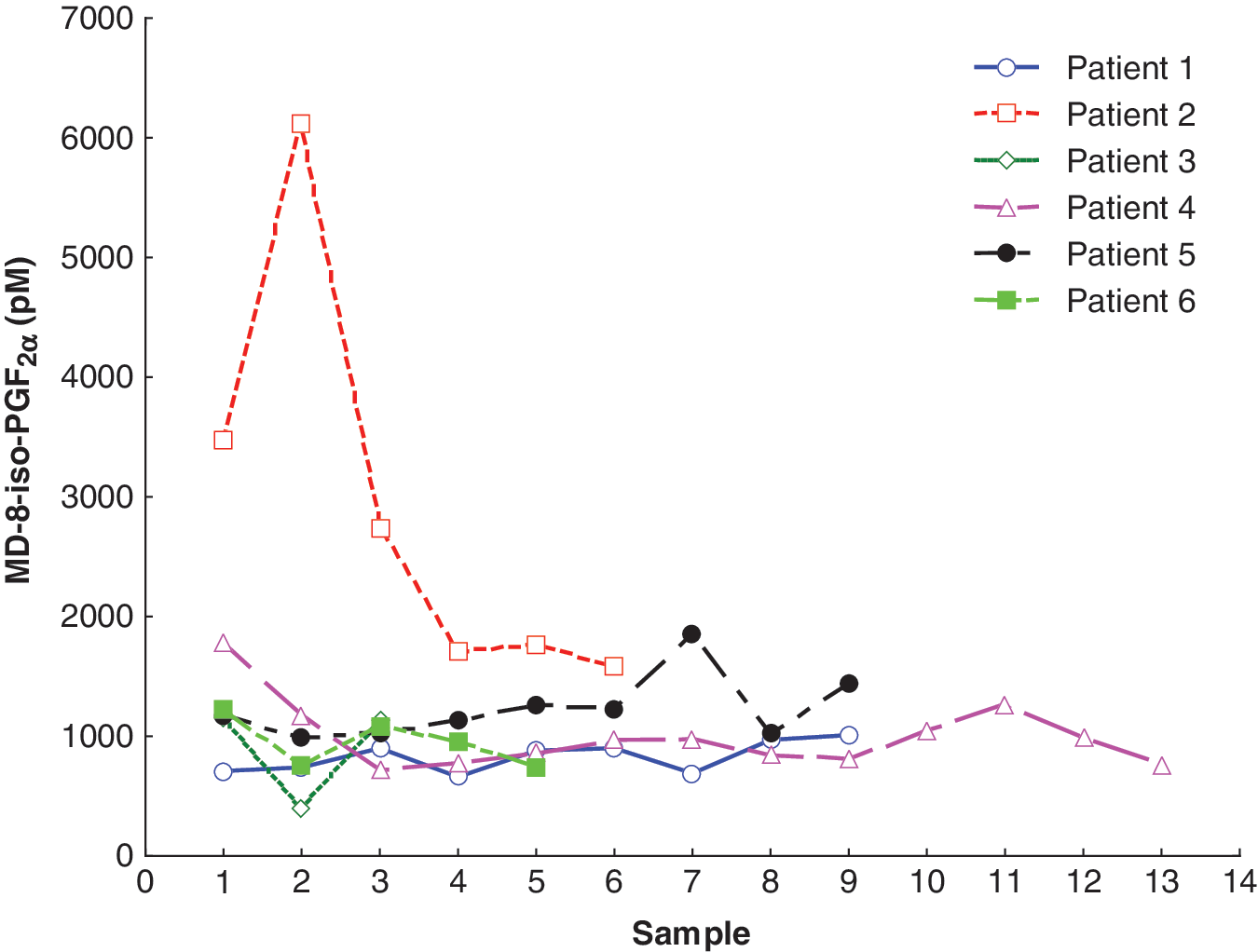
Individual concentrations of 8-iso-PGF2α in brain interstitial fluid using intracerebral microdialysis (MD; patients 1, 4, and 5 with focal TBI; patients 2, 3, and 6 with diffuse axonal injury; 8-iso-PGF2α, F2-isoprostane 8-iso-prostaglandin F2α; TBI, traumatic brain injury).
Relations among 8-iso-PGF2α and other MD biomarkers
We found strong, statistically significant correlations between the levels of MD-8-iso-PGF2α and MD-glycerol (r=0.830, p<0.05), as well as MD-glutamate (r=0.626, p<0.05; Table 2). The calculated factors of dependency (r2; 0.69 and 0.39, respectively) suggest that about 70% of the MD-glycerol signal and 40% of the MD-glutamate signal is related to oxidative stress, based on the assumption that 8-iso-PGF2α is a specific marker for oxidative stress (Awad et al., 1993; Basu, 2008; Morrow et al., 1992). Furthermore, MD-8-iso-PGF2α correlated negatively with MD-L/P ratio (r=–0.554; p<0.05). There was a weak correlation between MD-8-iso-PGF2α and MD-lactate and MD-pyruvate levels (r=0.41; p<0.05), and no correlation with MD-glucose (Table 2).
Bold values are statistically significant (p<0.05; n=45), weighted for the number of samples per patient. The strongest correlation was found between MD-8-iso-PGF2α and glycerol (r=0.83; p<0.05), followed by MD-8-iso-PGF2α and glutamate (r=0.63, p<0.05).
L/P, lactate/pyruvate ratio; MD, microdialysis; 8-iso-PGF2α, F2-isoprostane 8-iso-prostaglandin F2α.
8-iso-PGF2α levels and focal versus diffuse brain injury
Patients with a focal TBI had lower MD-8-iso-PGF2α levels (mean 1019±160 pmol/L) than the levels observed in patients with diffuse brain injury (mean 1776±1012 pmol/L). However, due to the difference in the number of observations, and the variance in patients with diffuse axonal injury, this did not reach statistical significance.
Illustrative cases
Patient 2, diffuse brain injury
This 19-year-old male patient fell 2.5 m and suffered a TBI. Initially the patient was RLS 4 (GCS 6–7), and a CT scan showed minimal bifrontal contusions, traumatic subarachnoid hemorrhage, cerebral swelling, and signs of a diffuse brain injury. The patient received intraparenchymal ICP monitoring, and initially the ICP was slightly elevated at ∼20 mm Hg, which responded to hyperventilation. At ∼28 h post-injury, the patient self-extubated and was immediately re-intubated. ICP gradually normalized and hyperventilation was discontinued at ∼56 h post-injury. The patient was GMS 5 and was extubated at ∼80 h post-injury. However, at approximately 6 days post-injury, the patient became more confused, and a CT scan showed increased swelling, and the patient was again intubated and high-dose pentobarbital treatment was needed to control the elevated ICP. At the end of the stay in the neuro-ICU, the patient was again extubated, and had GCS score 13–14 and RLS score 1–2. The patient made an uneventful recovery with an eGOS score of 7 at long-term follow-up. This patient had a peak in the 8-iso-PGF2α levels of more than 5000 pmol/L (Fig. 4A), which decreased when hyperventilation was discontinued. The same pattern was observed for MD-glutamate, which also reached very high levels at the early stage. MD-glycerol levels gradually increased in a delayed fashion during the monitoring period, reaching a high concentration (>100 μmol/L) 88 h after injury (Fig. 4A). The L/P ratio did not reveal signs of ongoing ischemia (data not shown).
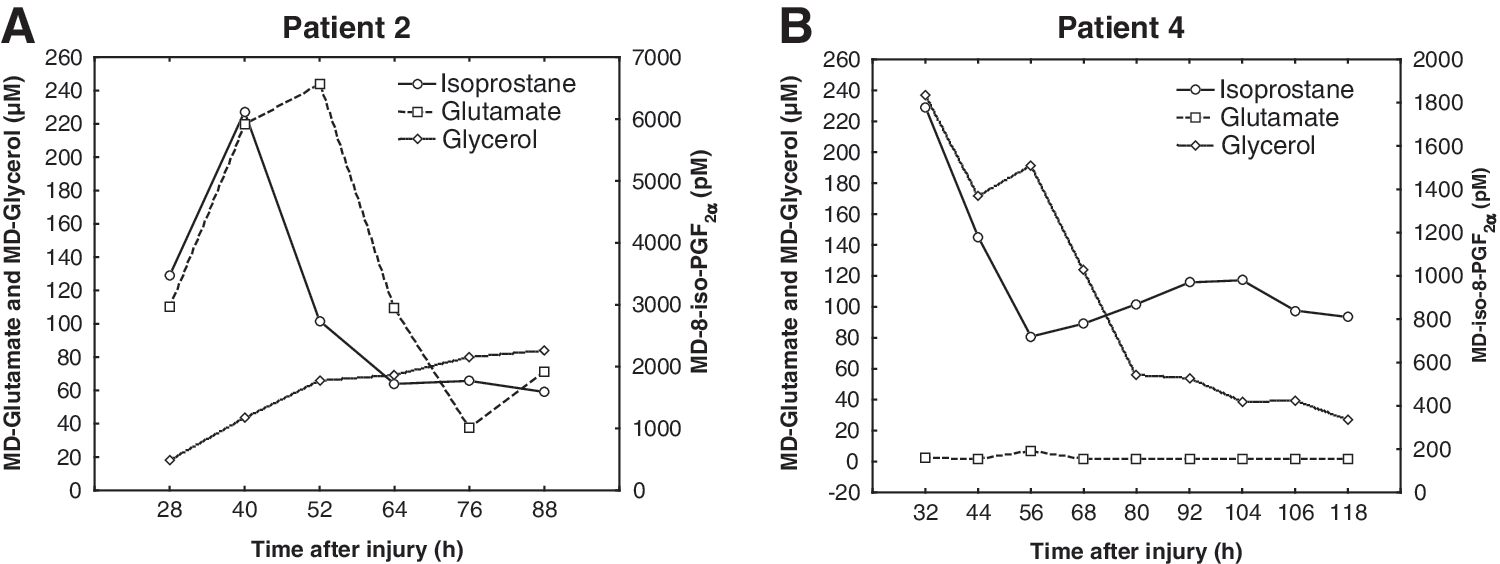
Illustrative cases. (
Patient 4, focal brain injury
This patient fell backwards, struck his head, and was initially unconscious. In the emergency department at the primary hospital, he had GMS score of 5 (RLS 3), and had left-sided weakness. Following intubation, a CT scan showed a frontal right epidural hematoma, bifrontal contusions, and a skull fracture. Initially the patient was stable, but at ∼30 h post-TBI, the right pupil dilated and a CT scan showed marked progress of the right-sided frontal contusion that was immediately evacuated and intraparenchymal ICP monitoring and a pericontusional MD probe was inserted via the right-sided craniotomy. After the contusion hematoma was evacuated, ICP was within the normal range, and the patient had an uneventful clinical course during the neuro-ICU stay. He was subsequently extubated, and had GMS and RLS scores of 6 and 2, respectively, prior to departure from our unit. At long-term follow-up, he had an eGOS score of 3. In this patient, MD-glutamate levels were consistently low (Fig. 4B). In contrast, initial MD-glycerol levels were markedly elevated, and then gradually subsided (Fig. 3B). The MD-8-iso-PGF2α levels were initially above 1500 pmol/L, decreasing to under 1000 pmol/L 2 days after injury, after which there was a slow increase over the next 2 days (Fig. 4B).
Discussion
In this study we evaluated the feasibility of measuring interstitial levels of 8-iso-PGF2α, a widely used biomarker for oxidative stress, using intracerebral MD in neuro-ICU patients with severe TBI. We also measured and compared 8-iso-PGF2α levels in other compartments, including vCSF and plasma. Finally, we studied the relations between MD-8-isoPGF2α levels and MD-glycerol, as well as MD-glutamate, widely used biomarkers of membrane phospholipid degradation/oxidative stress and excitotoxicity, respectively. Our main findings were that 8-iso-PGF2α can be measured in MD samples, and that the levels of MD-8-iso-PGF2α were distinctly higher than in vCSF and blood, supporting our basic hypothesis of the usefulness of harvesting biomarkers directly in the injured brain tissue. Importantly, there was a strong relation between MD-8-iso-PGF2α, MD-glycerol, and MD-glutamate levels, supporting the link between oxidative stress, membrane phospholipid degradation, and excitotoxicity, as previously suggested in the experimental TBI setting (Lewen et al., 2000; Schulz et al., 1995).
Following TBI, the secondary injury process markedly exacerbates, up to several times, the size of the primary lesion. Experimental evidence clearly demonstrates the important role of oxidative stress (Hall, 1993; Kontos and Wei, 1986; Marklund et al., 2001a; Shohami et al., 1997) following TBI, and inhibition of ROS has consistently been shown to attenuate the histological and behavioral deficits (Clausen et al., 2008; Hall et al., 2010; Marklund et al., 2001b). Following experimental TBI (Roof et al., 1997; Tyurin et al., 2000), and global cerebral ischemia (Idris et al., 2005), in animal models, early F2-isoprostane levels were markedly increased. Although F2-isoprostane in CSF has been shown to correlate with clinical neurological outcomes in a small study of patients with severe TBI (Wagner et al., 2004), bedside tools for monitoring ROS activity in human TBI are lacking, and have hampered our understanding of the role of oxidant activity in humans. Since F2-isoprostanes are stable and extremely sensitive and robust markers of secondary oxidant injury (Awad et al., 1993), they could be useful target markers for oxidative stress following human TBI, as suggested in studies of vCSF in pediatric and adult TBI patients (Bayir et al., 2002, 2004).
In the present report, we found that the interstitial (MD) levels of 8-iso-PGF2α were markedly (five- to sixfold) higher than in vCSF and plasma, supporting our basic hypothesis about the advantage of sampling with MD directly in injured brain tissue, thus improving spatial and temporal resolution of the biomarker. Notably, a significantly higher level of 8-iso-PGF2α in the MD samples compared to the other compartments was found, even though no correction for in vivo recovery (currently unknown) was done, suggesting that the 8-iso-PGF2α levels obtained by MD may be markedly underestimated. The 8-iso-PGF2α levels in plasma samples were in line with those found in previous reports using a pig model of cardiac arrest and the same analytical method for measuring free 8-iso-PGF2α (Wiklund et al., 2005). These levels are not directly comparable with the studies of Bayir and associates (Bayir et al., 2002, 2004), who used a different assay to measure the total amount of 8-iso-PGF2α. The concentrations of 8-iso-PGF2α in the normal, uninjured human brain are still unknown.
In the validation part of the study, we found a strong correlation between MD-8-iso-PGF2α and MD-glycerol. MD-glycerol is a widely used biomarker in the neuro-ICU setting, and can readily be measured at the bedside using commercially available MD analyzers. MD-glycerol is generally thought to reflect cell membrane phospholipid (PL) degradation following brain injury, leading to an accumulation of arachidonic acid (AA) and other free fatty acids (for references see Hillered et al., 2005). Since AA is an important substrate for ROS production that may trigger additional membrane degradation, MD-glycerol has also been implicated as a biomarker of oxidative stress (Clausen et al., 2005; Lewen and Hillered, 1998). The strong correlation between MD-8-iso-PGF2α and MD-glycerol in this study supports the close relationship between membrane PL degradation and oxidative stress in the human brain following TBI. The finding that about 70% of the MD-glycerol signal is related to oxidative stress (as indicated by the factor of dependency and the assumption that 8-iso-PGF2α is a specific marker for oxidative stress) supports the experimental TBI studies implicating MD-glycerol as a biomarker of oxidative stress (Lewen and Hillered, 1998; Merenda et al., 2008). Taken together, our results suggest that MD-8-iso-PGF2α, together with MD-glycerol, may prove to be clinically useful as markers of oxidative stress, once a bedside analytical method for 8-iso-PGF2α becomes available.
MD-glutamate is widely used as a marker of excitotoxicity in the neuro-ICU setting, and can be readily analyzed at the bedside with MD analyzers. We found a significant correlation between MD-8-iso-PGF2α and MD-glutamate in this study. This correlation probably reflects the well-known causal relationship between the intracellular accumulation of Ca2+ caused by glutamate receptor overactivation, leading to phospholipase activation, and membrane phospholipase degradation, as revealed by numerous experimental TBI studies (for references see Hillered et al., 2005). To our knowledge, this is the first direct demonstration of this relationship in the human brain following TBI. Our finding that about 40% of the MD-glutamate signal is related to oxidative stress (as indicated by the factor of dependency and the assumption that 8-iso-PGF2α is a specific marker for oxidative stress) is intriguing, and may reflect another potentially important link between oxidative stress and excitotoxicity via the microglial antiporter system Xc
Although there were marked inter-individual differences in 8-iso-PGF2α levels, there was a difference between patients with focal and diffuse brain injury, although this was not statistically significant. We observed that 8-iso-PGF2α levels appeared to be lower in focal compared to diffuse TBI, warranting further study.
Methodological considerations and limitations
Admittedly, since this is a small feasibility study including only six patients, the results need to be confirmed in a larger series of patients. However, despite the small number of patients, our findings are novel, significant, and important in the context of translation of our knowledge of secondary injury mechanisms in animal models of TBI to human patients in the neuro-ICU setting.
Similarly to other clinical TBI studies, we were unable to present any data from non-injured controls for comparison because of the invasiveness of the methodology. In future studies, reference data may be obtained from patients with infratentorial conditions requiring invasive ICP monitoring.
We plan to perform in vivo recovery experiments in the neuro-ICU employing the extrapolation-to-no-flow rate method (Jacobson et al., 1985).
There has been some controversy regarding the specificity of 8-iso-PGF2α as a marker of oxidative stress because of possible enzymatic production of 8-iso-PGF2α by cyclooxygenase (COX). This was based on data from Pratico and associates, who found that in vitro COX inhibition of human platelets reduced the amount of 8-iso-PGF2α in culture media (Pratico et al., 1995). However, this has been refuted in several other in vivo studies (Bachi et al., 1997; Belton et al., 2000; Pratico et al., 1998).
Even though the sensitivity of the assay is good on low pg/mL levels (the detection limit was 8 pg/mL; Basu, 1998), our initial pilot experiments showed that we needed to pool MD samples to obtain the volume needed to analyze 8-iso-PGF2α. This is because of the routine measurement of other MD biomarkers (glucose, lactate, pyruvate, glutamate, glycerol, and urea), leaving a small remaining hourly sample for the isoprostane assay. We therefore decided on a feasibility study design with pooling of 12 hourly MD fractions to be on the safe side (allowing for repeated analyses if needed), resulting in poor temporal resolution. An optimized study design allows for quantification of 8-iso-PGF2α in MD fluid with a temporal resolution of 2 h in our follow-up study, which we believe is relevant for this biomarker in the neurointensive care setting.
The implantation of an MD probe/catheter causes a brief rise in metabolite levels, including glutamate and lactate. However, our own and other studies have shown that this effect dissipates after less than an hour (Hillered et al., 1990; Nilsson et al., 1990; Sumbria et al., 2010), suggesting that it should have no impact on our data with MD sampling commencing≥2 h following implantation.
The data shed light on the interpretation of MD biomarkers currently used extensively in neuro-ICU settings around the world. The data supporting MD-glycerol as a useful marker of oxidative stress appear particularly intriguing. Thus, MD-8-iso-PGF2α and MD-glycerol in combination may prove to be useful as biomarkers of oxidative stress in the neuro-ICU setting, both as monitoring tools and as surrogate end-points in neuroprotective drug development.
Conclusions
This study demonstrates the feasibility of analyzing 8-iso-PGF2α in MD samples from the human brain following TBI. The highest concentrations of 8-iso-PGF2α were found in MD samples, compared to vCSF and blood, suggesting that the interstitial compartment is the preferred site for harvesting this biomarker. Our results support a close relationship between excitotoxicity and oxidative stress following human TBI, and that MD-8-iso-PGF2α in combination with MD-glycerol may be useful biomarkers of oxidative stress in the neuro-ICU setting.
Footnotes
Acknowledgments
The authors would like to thank Mrs. Inger Ståhl-Myllyaho and Eva Sejby for analyzing the samples, and Dr. Lars Berglund for statistical consultation.
This study was supported by the Swedish Research Council, the Swedish Brain Foundation, Uppsala University Hospital, the Selander Foundation, and the Åhlén Foundation.
Author Disclosure Statement
No competing financial interests exist.