
Abstract
Pressor response is carried in afferent fibers of somatic nerves to increase blood pressure (BP) and heart rate (HR) during static exercise in humans. However, there is no information that peripheral responses restore muscle contraction with nerve transfer operation. In this study, we aimed to assess isometric exercise-induced pressor responses in patients with brachial plexus injury (BPI) after intercostal nerve transfer (ICNT) to restore elbow flexor muscles. Systolic blood pressure (SBP), diastolic blood pressure (DBP), and HR during 2-min sustained isometric muscle contraction of elbow flexors at 20% and 35% of maximal voluntary contraction (MVC) on the unaffected side and the ICNT side, were measured in seven subjects with BPI treated with ICNT. SBP, DBP, and HR during 2-min sustained isometric muscle contraction of elbow flexors at 20% of MVC on the unaffected side were similar to those recorded before and after the exercise. However, the same variables increased significantly (p<0.001) during a similar type of exercise at 35% MVC on the unaffected side. On the ICNT side, no significant differences were noted in elbow flexors at 20% and 35% MVC. Isometric static exercise at 35% of MVC did not induce pressor and HR changes on the ICNT side. The difference in the responses between the two sides could have been caused by incomplete recovery of afferent nerve function following nerve repair, despite the restoration of efferent nerve function. Alternatively, the HR and BP responses to static contraction may depend upon the active muscle mass.
Introduction
S
There is no information on the pathways involved in the regulation of peripheral responses during static exercise in patients with postoperative brachial plexus injury (BPI). Patients with total type BPI show various dysfunctions of the muscles of the upper extremities after injury. Recovery of elbow flexor muscle function follows surgical repair of the brachial plexus using nerve grafting or intercostal nerve transfer (ICNT). In the ICNT, the intercostal nerves are directly sutured to the musculocutaneous nerves, and this surgery is one of the most common procedures used for reconstruction of the elbow flexor muscles in preganglionic types of injury (root avulsion) (Nagano, 1998; Nagano et al., 1989). Thus, the elbow flexor muscles are innervated by intercostal nerves after ICNT surgery. In patients who undergo the ICNT operation, the strength of the elbow flexors muscles is sufficient to flex the elbow, suggesting regeneration of the efferent nerve after ICNT; however, there is no information on the process of regeneration of the afferent nerves following ICNT.
Complete cervical spinal cord injury is associated with disruption of spinal reflexes that regulate cardiovascular responses during static exercise (Yamamoto et al., 1999). Yamamoto and associates (Yamamoto et al., 1999) reported that the mean arterial BP was increased during static exercise in such patients. However, no significant changes in HR were seen during static exercise and at 35% maximum voluntary contraction (MVC), compared with baseline condition (pre-exercise period) (Yamamoto et al., 1999). To our knowledge, however, no previous studies have examined the effects of ICNT on BP and HR response to static exercise in BPI patients.
The purpose of this study was to compare the postoperative cardiovascular responses to static exercise on the nerve transferred side with that on the unaffected side in BPI patients. For continuous arm muscle contraction, functional cardiovascular responses should supply oxygen and energy substrates to the muscles. Accordingly, for full assessment of afferent nerve regeneration, it is important to measure BP and HR during exercise. For this purpose, we measured BP and HR in seven BPI patients with ICNT during 2 min of sustained contraction of the elbow flexor muscles at 20% and 35% MVC of static exercise.
Methods
Subjects
The subjects were seven BPI patients with complete root avulsion and total paralysis of the upper extremity who had undegone ICNT for restoration of elbow flexion. Complete root avulsion was diagnosed using the criteria described by Nagano (Nagano, 1998). After classification of the brachial plexus lesion as preganglionic, no immediate recovery was expected, and improvement of motor function was expected to be achieved only by nerve transfer or other reconstructive procedures. The subjects underwent electrophysiological examinations intraoperatively to confirm the site of injury, including recording the somatosensory evoked potential (SEP) and evoked spinal cord potential (ESCP).
Table 1 lists the clinical data for these patients. They included six men and one woman who had no other medical history apart from BPI of preganglionic avulsion injuries. Although Subject 2 was a teenager, he was included in this study based on his well-developed secondary male sex characters and muscle strength equal to that of adults. During the ICNT, the third and fourth intercostal nerves were sutured directly to the musculocutaneous nerves as near as possible to their motor ends without using free grafts. The intercostal nerves were cut at the costochondral junction, and a cable was established and tunneled subcutaneously through the axilla to the arm (Nagano et al., 1989). All surgical procedures were performed by the same surgeon. At the time of the study, the strength of the elbow flexors muscles was sufficient to flex the elbow easily and to maintain their strength. The experimental protocol was approved by the Human Investigation Committee of Hamamatsu University School of Medicine, and each subject gave informed written consent.
Recording of hemodynamic variables
Systolic blood pressure (SBP) and diastolic blood pressure (DBP) were monitored continuously by photoplethysmography (noninvasive blood pressure monitoring system, MUB101; Medisens, Saitama, Japan) after confirming the absence of laterality of BP in the upper extremities. This system measures finger arterial BP using a fast servosystem attached to an inflatable finger cuff, and blood volume in a finger artery is kept constant during each pulse cycle and detected by a photoplethysmograph. In our study, the sensor was placed on the middle finger of the hand on the unexercised side.
HR was recorded continuously throughout the experiment using a three-lead electrocardiogram (ECG), and calculated by the R-R interval. Subjects were instructed to breathe regularly and to avoid Valsalva-like maneuvers during exercise.
Throughout the experiments, we ensured no abdominal muscle contraction by surface electromyography. After measurement of MVC, 2 min of isometric 20% MVC and 35% MVC exercise were performed.
Study protocol
Experiments were performed in an air-conditioned laboratory (ambient temperature, 27°C). All subjects reported to the laboratory at Hamamatsu University School of Medicine and rested on a comfortable bed in a supine position with the elbow kept at 90° flexion and the forearm kept at supination position. Each subject performed the isometric MVC with the elbow at 90° (static exercise) using a hand-held dynamometer (PowerTrackII, JTECH Co., Japan).
At least 20 min before the experiment, MVC was measured for both the ICNT side and the unaffected side. MVC represented the maximum force generated in two trials separated by at least a 2-min rest. After the 2-min rest period (pre-exercise period), the subject performed static exercise at 20% MVC for 2 min (exercise period), and then rested for 5 min (recovery period). SBP, DBP, and HR were measured continuously during the pre-exercise, exercise, and recovery periods. After the return of all cardiovascular variables to the baseline value, 35% MVC static exercise was performed using a protocol similar to that of the 20% MVC static exercise. Throughout the experiments, we did not observe any skeletal muscle contraction except in the examined elbow flexors.
Statistical analysis
HR and BP were recorded continuously throughout the experiment and the mean values were averaged every 30 sec. These data were expressed as mean±SEM. Significant changes in each parameter during the exercise and recovery periods, relative to the pre-exercise period, were examined by repeated measures analysis of variance with Tukey-Kramer test for multiple comparisons. Differences between the ICNT side and the unaffected side were examined for statistical significance using the Mann-Whitney U test. A p value <0.01 was considered statistically significant.
Results
The experiments were performed 2–10 years after ICNT. The muscle strength in all subjects was sufficient to flex the elbow easily and to maintain the strength for more than 2 min. The MVC of elbow flexors on the ICNT side was 18–77 Nm and 8.7–36.5% (mean, 22.9±8.5%) of MVC on the unaffected side (Table 2).
Cardiovascular response to 20% MVC static exercise
On the unaffected side, SBP, DBP, and HR remained unchanged throughout the pre-exercise, exercise, and recovery period (Figs. 1 and 2). At 20% MVC static exercise on the ICNT side, no significant differences were recorded in SBP, DBP, and HR throughout the pre-exercise (130.3±5.6, 67.4±3.8 mm Hg, 67.7±2.9 bpm, respectively), exercise (131.6±2.7, 68.8±1.9 mm Hg, 67.7±1.3 bpm, respectively), and recovery period (128.8±1.2, 67.2±0.9 mm Hg, 66.8±0.7 bpm, respectively) (Figs. 3 and 4).

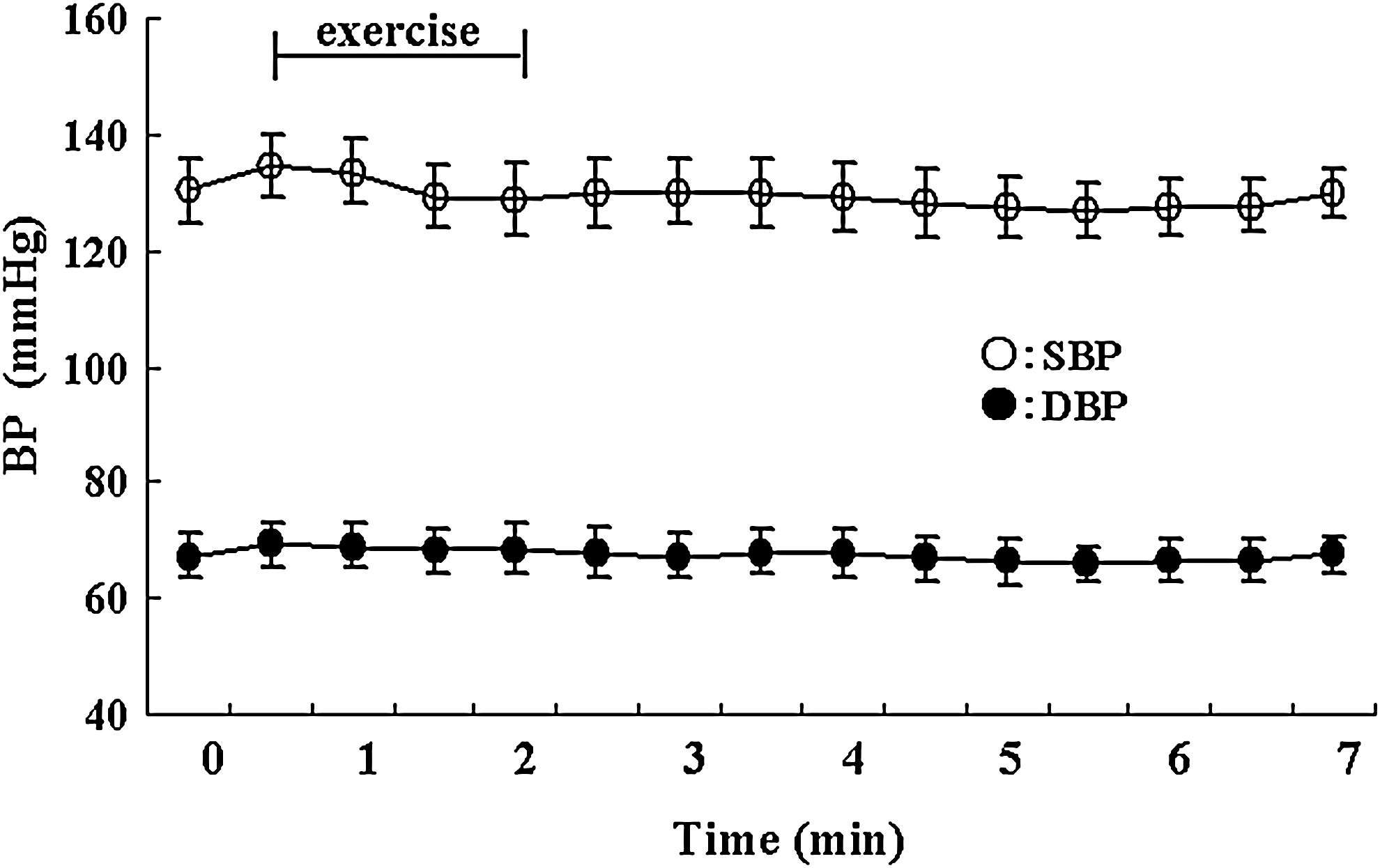
Changes in systolic blood pressure (SBP) and diastolic blood pressure (DBP) measured before exercise, during 2-min static exercise at 20% of maximum voluntary contraction (MVC) performed using the unaffected upper extremities of patients with brachial plexus injury (BPI), and post-exercise during a recovery period. Data are mean±SEM of seven patients.
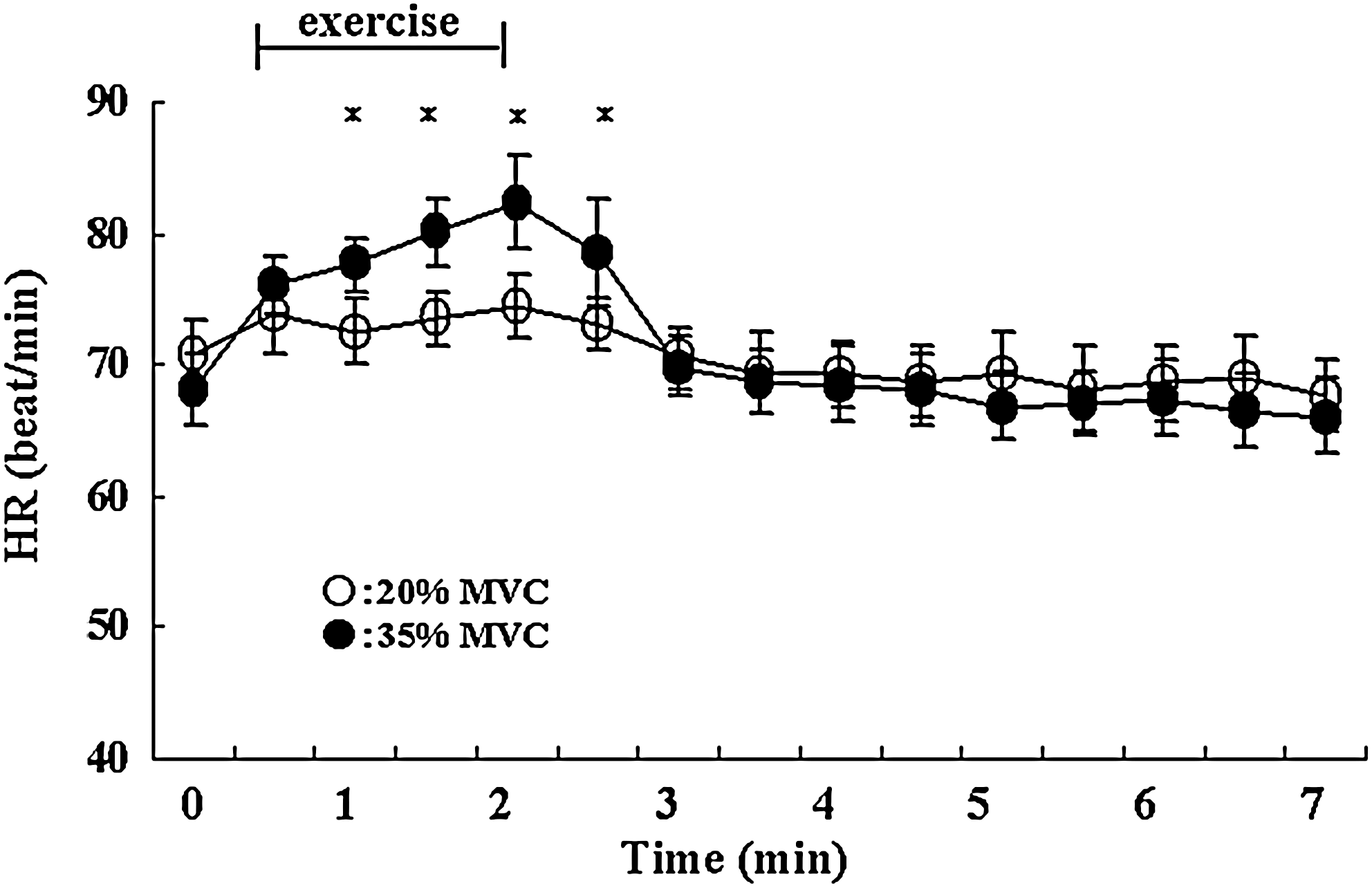
Changes in heart rate (HR) in beats per minute (bpm) measured before exercise, during 2-min static exercise at 20% and 35% of maximum voluntary contraction (MVC), performed using the unaffected upper extremities of patients with brachial plexus injury (BPI), and post-exercise during a recovery period. Data are mean±SEM of seven patients. *p value is <0.01.
Changes in systolic blood pressure (SBP) and diastolic blood pressure (DBP) measured before exercise, during 2-min static exercise at 20% of maximum voluntary contraction (MVC), performed using the intercostal nerve transfer (ICNT)-operated upper extremities of patients with brachial plexus injury (BPI), and post-exercise during a recovery period. Data are mean±SEM of seven patients.
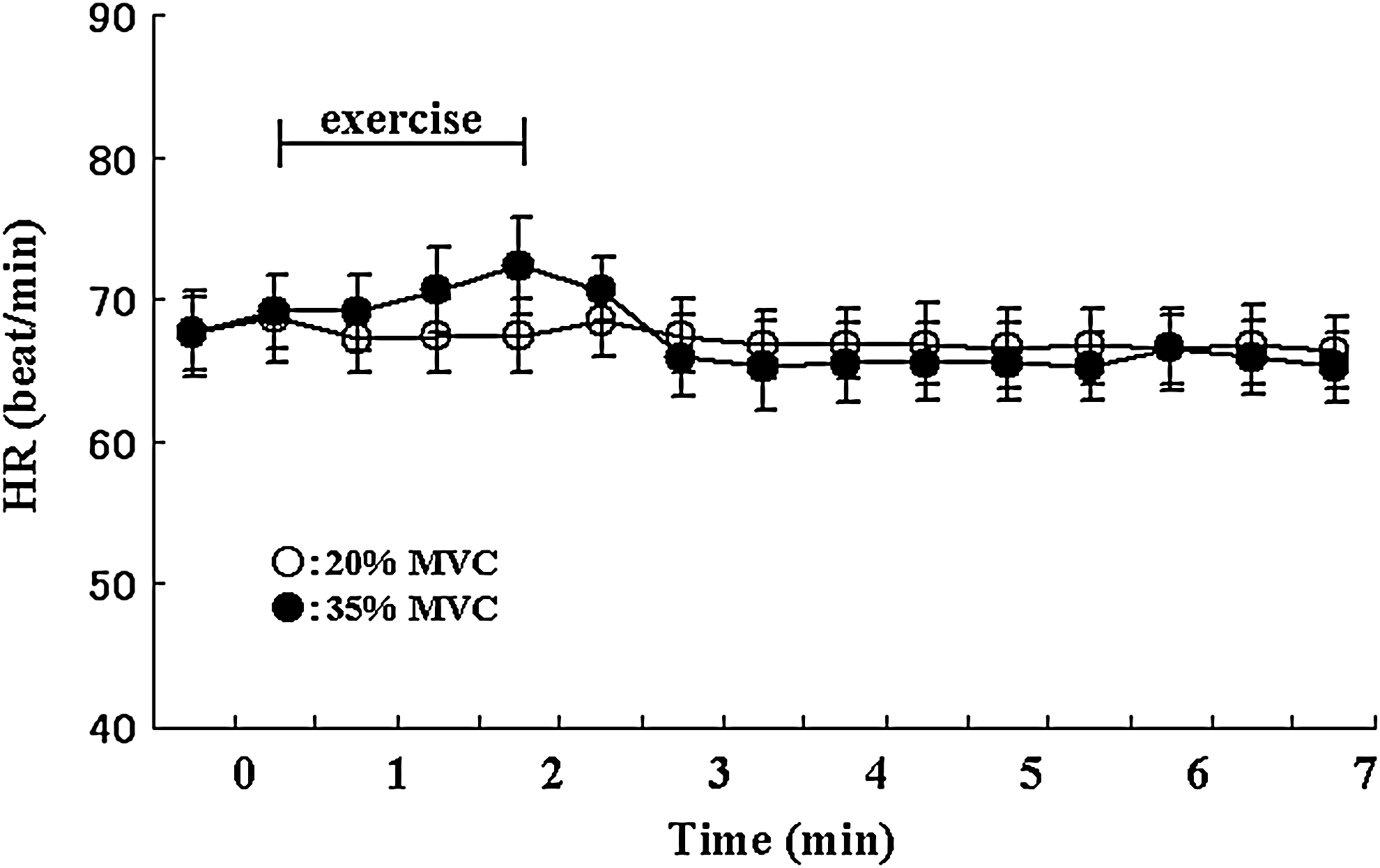
Changes in heart rate (HR) in beats per minute (bpm) measured before exercise, during 2-min static exercise at 20% and 35% of maximum voluntary contraction (MVC), performed using intercostal nerve transfer (ICNT)-operated upper extremities of patients with brachial plexus injury (BPI), and post-exercise during a recovery period. Data are mean±SEM of seven patients.
Cardiovascular response to 35% MVC static exercise
On the unaffected side, SBP, DBP, and HR increased significantly (p<0.01, each) during the exercise period (131.7±3.2, 70.4±1.8 mm Hg, 79.1±1.3 bpm, respectively) compared with the pre-exercise period (120.5±6.9, 59.3±2.6 mm Hg, 68.3±2.7 bpm, respectively) but returned to the pre-exercise levels immediately after exercise (120.5±1.5, 60.6±0.7 mm Hg, 68.0±0.8 bpm, respectively) (Figs. 2 and 5).
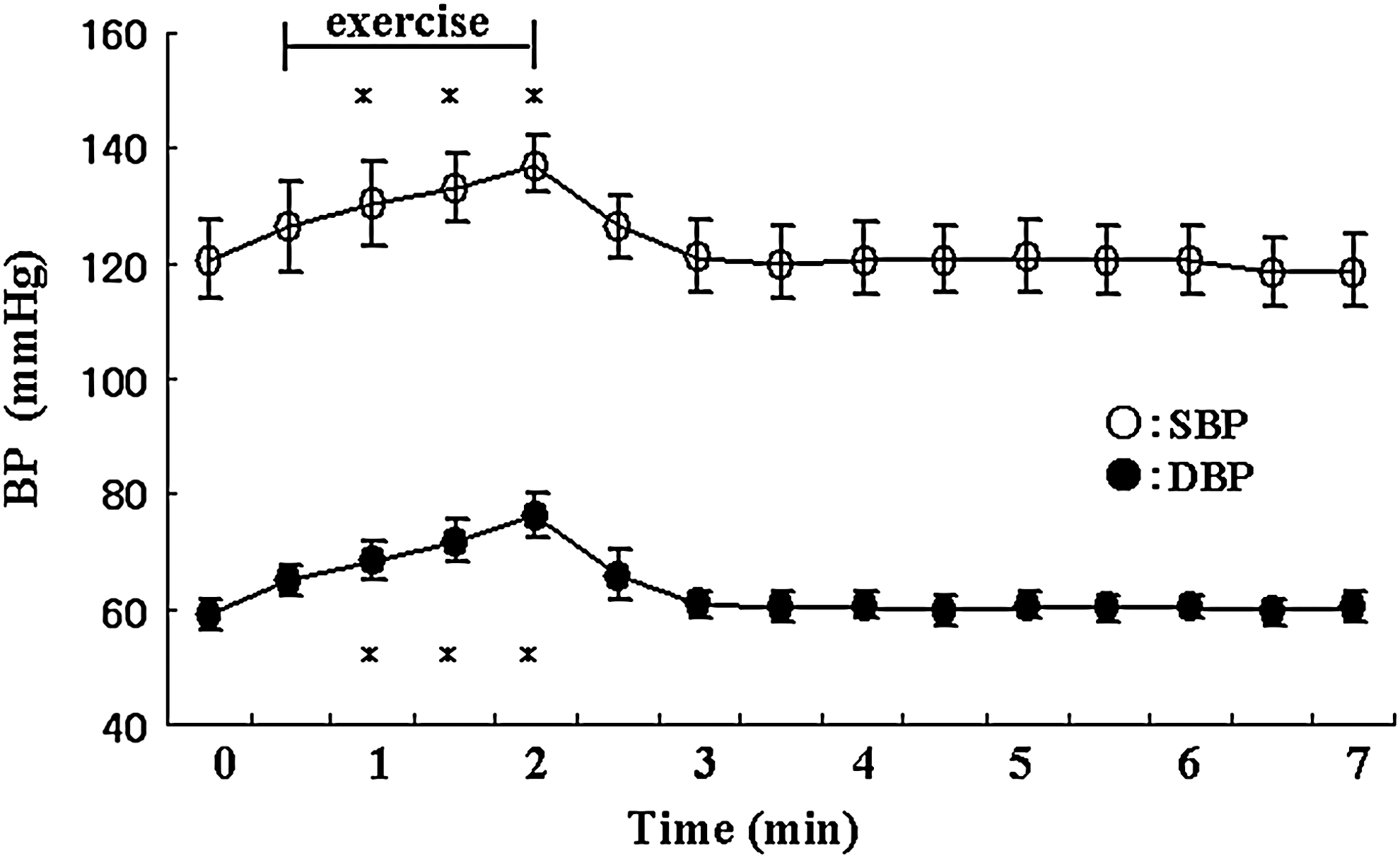
Changes in systolic blood pressure (SBP) and diastolic blood pressure (DBP) measured before exercise, during 2-min static exercise at 35% of maximum voluntary contraction (MVC), performed using the unaffected upper extremities of patients with brachial plexus injury (BPI), and post-exercise during a recovery period. Data are mean±SEM of seven patients. *p value is <0.01
On the ICNT side, no significant changes were noted in SBP, DBP, and HR throughout the pre-exercise (130.6±3.4, 68.1±3.3 mmHg, 67.6±2.6 bpm, respectively), the exercise (133.0±1.8, 71.3±1.6 mmHg, 70.4±1.4 bpm, respectively), and the recovery periods (130.9±1.0, 68.4±0.8 mm Hg, 66.3±0.7 bpm, respectively) (Figs. 4 and 6).

Changes in systolic blood pressure (SBP) and diastolic blood pressure (DBP) measured before exercise, during 2-min static exercise at 35% of maximum voluntary contraction (MVC), performed using the intercostal nerve transfer (ICNT)-operated upper extremities of patients with brachial plexus injury (BPI), and post-exercise during a recovery period. Data are mean±SEM of seven patients.
Discussion
The present study is the first that investigated changes in BP and HR during static exercise in BPI patients who had undergone ICNT surgery. All patients who were treated with nerve transfer of the third and fourth intercostal nerves to the musculocutaneous nerve to restore elbow flexion, had BPI with complete root avulsion, and exhibited useful elbow flexion. Thus, at the time of our study, the elbow flexor muscles of our patients were innervated by the intercostal nerves. The best indications for this operation are that patients are <40 years of age and that the operation is performed within 6 months after injury (Nagano et al., 1989). All our subjects satisfied these two criteria.
At skeletal muscle tension of 20% MVC and higher, fatigue occurs rapidly (Lind, 1970). For example, at 20% MVC, the contraction can be held for only 10–12 min. At 30% MVC, the duration is ∼ 5 min, whereas at 50% MVC, it is 1–2 min (Lind, 1970). Therefore, we measured BP and HR in our patients during 2 min of sustained contraction of the elbow flexor muscles at 20% and 35% MVC bilaterally. Apart from the examined elbow flexor muscles, no contraction of other skeletal muscles was noted during the test. The muscle strength during elbow flexion was strong enough to flex the elbow easily in all subjects and sufficient enough to maintain the strength after ICNT. However, the muscle strength of the reinnervated muscles on the ICNT side was weaker than that of muscles on the unaffected side. Usually, the effect of ICNT surgery appears 3–6 months later, and it is mostly complete at 24 months. The present study was conducted 2–10 years after ICNT surgery.
The cardiovascular response to static exercise is regulated by both central and peripheral mechanisms (Goodwin et al., 1970; McCloskey and Mitchell, 1972; Mitchell et al., 1981). The central mechanism involves transmission of impulses from the motor cortex to the medullary cardiovascular center. Afferent impulses from the exercising muscles reach the spinal cord and ascend in the spinothalamic tract to the medullary cardiovascular center (Shepherd et al., 1981). The peripheral mechanism consists of a reflex pathway originating from the contracting muscle. Although this pathway has not been elucidated completely, the possible involvement of a reflex pathway that originates from the skeletal muscle and chemically affects the pressor response to forceful isometric contraction has been described (Seals et al., 1983). Although the pressor responses should reflect the activity of efferent nerves, previous studies reported only changes in mean BP (Cui et al., 2006; Herr et al., 1999). In the present study, no changes were noted in SBP and DBP during static exercise on the affected side, whereas both SBP and DBP increased significantly on the unaffected side. These results suggest that the efferent nerve influenced SBP and DBP in our subjects.
The pressor response is mediated by small myelinated type III fibers and unmyelinated type IV afferent fibers (Johansson, 1962; Mitchell et al., 1977; Skoglund, 1960). Group III and IV muscle afferents consist of several different subpopulations including nociceptors that are activated by noxious chemical, mechanical, or thermal stimuli (Kniffki et al., 1981). The pressor reflex and related receptors are connected to the pressor subgroup III and group IV afferent fibers. Therefore, physical exercise is accompanied by cardiovascular and respiratory changes that are initiated reflexively by activation of neural receptors within the exercising muscles. The most probable source of afferent input for the reflex responses seen during static exercise is that from muscle receptors. The pressor response is carried in the afferent fibers of somatic nerves (Tallarida et al., 1981).
The efferent and afferent nerve pathways are damaged during ICNT. The ICNT involves restoration of the efferent nerves, in which the intercostal nerve is directly sutured to the musculocutaneous nerve, resulting in the restoration of elbow flexion. However, the strength of the reinnervated muscle on the ICNT side in BPI patients was significantly weaker than that on the unaffected side. Furthermore, the mean 35% MVC on the ICNT side was ∼ 20% (range, 8.7–36.5%) of that on the unaffected side. Does functional recovery of the afferent fibers of the somatic nerve occur in BPI subjects after ICNT? During the 2-min sustained isometric muscle contraction of elbow flexors at 20% MVC, no increases were noted in SBP, DBP, and HR on the unaffected side, but at 35% MVC, isomeric contraction, SBP, DBP, and HR on the unaffected side significantly increased during the exercise period. These findings suggest that the workload of 20% MVC on the unaffected side of BPI subjects results in excitatory signals that are probably insufficient to stimulate BP and HR. Our results are consistent with those of Stebbins and associates (Stebbins et al., 2002). In the presence of an afferent input, the sympathetic activity to blood vessels was augmented, resulting in increased peripheral vessel tone, which in turn resulted in an increase in BP (Sinoway et al., 1989). Moreover, static exercise increased HR, which was mainly triggered by the central command (Mark et al., 1985), and the chronotropic response to static exercise resulted primarily from withdrawal of parasympathetic activity within HR of ∼100 bpm (Hollander and Bouman, 1975; Rowell, 1993). In static exercise, the stroke volume does not increase, and at higher tensions it decreases, so that the ensuing tachycardia is the main contributor to the increase in cardiac output. There is mild but widespread peripheral vasoconstriction in static exercise so that the increased cardiac output results in increased BP (Lind et al., 1967).
On the ICNT side, no significant changes were seen in SBP and DBP during 2-min sustained isometric muscle contraction of elbow flexors at 20% and 35% MVC. A relevant factor in the pressor response is the fraction of the maximum isometric tension exerted by any muscle group. For example, a 35%MVC contraction of elbow flexor muscles on the ICNT side and a 35% MVC contraction of the same muscle on the unaffected side against an immovable force resulted in the same degree of pressor response, despite the fact that the absolute tensions involved were different (Lind, 1970). Therefore, there is no cardiovascular response to exercise caused by the lack of chemosensitive afferent impulses. It is possible that surgery results in severance of the pathways that transmit chemosensitive afferent impulses from the injured muscles of the upper extremities in BPI, despite the restoration of efferent nerve function.
On the other hand, Seals and coworkers (Seals et al., 1983) indicated that the magnitude of the cardiovascular response to static contraction correlated with the mass of the active muscles. Furthermore, the cardiovascular response to muscle contraction is dependent upon the magnitude of force or tension produced during contraction (Kaufman and Foster, 1996). At the same % MVC, the magnitude of increases in BP and HR correlated with the size of the active muscle mass. In BPI patients, the workload on the ICNT side was almost 20% of that on the unaffected side, and therefore the excitatory signals were probably insufficient to active BP and HR.
Recent advances in biomedical technology have vitalized the field of regenerative medicine, and further progress in cranial and peripheral nerve surgery is expected in the future. The present study is the first to evaluate the regeneration of both the efferent and afferent nerves, and it found a discrepancy between autonomic nervous system response and recovery of motor function. Assessment of the cardiovascular responses to static exercise in patients who have undergone regenerative surgical techniques provided important information, because continuation of exercise is linked to the cardiovascular response. The present study emphasizes the need to evaluate the neural recovery process after neurotrauma in humans. Long-term follow-up of the patients is warranted, including examinations using newer technologies such as functional MRI of the brain and spinal cord.
Conclusions
The present study demonstrated that static exercise at 35% of MVC did not increase HR and BP on the ICNT side in subjects who had undergone nerve repair surgery. However, on the unaffected side, the same magnitude of static exercise resulted in a significant increase of HR and BP. The difference between the two sides is probably caused by incomplete recovery of afferent nerve function following the operation, despite the restoration of efferent nerve function. Alternatively, the HR and BP responses to static contraction may depend upon the active muscle mass.
Footnotes
Author Disclosure Statement
No competing financial interests exist.