
Abstract
Cytokine measurement directly from the brain parenchyma by means of microdialysis has documented the activation of certain procedures in vivo, after brain trauma in humans. However, the intercalation of the micro-catheter insertion with the phenomena triggered by the head trauma renders the assessment of the findings problematic. The present study attempts to elucidate the pure effect of minimal trauma, represented by the insertion of the micro-catheter, on the non-traumatized human brain. Microdialysis catheters were implanted in 12 patients with drug-resistant epilepsy, and subjected to invasive electroencephalography with intracranial electrodes. Samples were collected during the first 5 days of monitoring. The dialysate was analyzed using bead flow cytometry, and the concentrations of interleukin (IL)-1, IL-6, IL-8, IL-10, IL-12, and tumor necrosis factor-α (TNF-α) were measured. The levels of IL-1 and IL-8 were found to be raised until 48 h post-implantation, and thereafter they reached a plateau of presumably baseline values. The temporal profile of the IL-6 variation was different, with the increase being much more prolonged, as its concentration had not returned to baseline levels at the fifth day post-insertion. TNF-α was found to be significantly raised only 2 h after implantation. IL-10 and IL-12 did not have any significant response to micro-trauma. These findings imply that the reaction of the neuro-inflammatory mechanisms of the brain exist even after minimal trauma, and is unexpectedly intense for IL-6. Questions may arise regarding the objectivity of findings attributed by some studies to inflammatory perturbation after head injury.
Introduction
The impact of traumatic brain injury (TBI) on the mechanisms of neuro-inflammation has been widely studied. It has been proven that a variety of inflammatory mediators, among which cytokines play a major role, participate in the traumatic sequelae. Several experimental studies have investigated the activation of neuro-inflammatory processes after brain trauma, and have noted an increase in the production of various cytokines.
The expression of interleukin-1 (IL-1) has been found to rise significantly after experimental brain injury, as indicated either by the increased levels of the corresponding mRNA (Fassbender et al., 2000; Holmin et al., 1997; Yan et al., 1992), or by the detection of the cytokine itself in brain extracts (Knoblach and Faden, 2000; Nieto-Sampedro and Berman, 1987; Taupin et al., 1993), or in the cerebrospinal fluid (CSF) and the brain parenchyma (Woodroofe et al., 1991). Tumor necrosis factor-α (TNF-α)–related mRNA has also been repeatedly detected at increased levels after experimental traumatic lesions (Holmin et al., 1997), leading to the early neuronal expression of the cytokine (Knoblach et al., 1999). TNF-α was also detected in the CSF (Stover et al., 2000), and in brain extracts (Taupin et al., 1993), with short delays (3–8 h) after the occurrence of trauma. Regarding interleukin-6 (IL-6), its expression is also activated after experimental traumatic injury to the brain (Holmin et al., 1997; Yan et al., 1992), and its concentration is increased in the CSF (Stover et al., 2000), and in the brain (Taupin et al., 1993; Woodroofe et al., 1991). The increased production of IL-6 occurs in injured astrocytes, as demonstrated in cultures of human cells (Hariri et al., 1994).
Other cytokines have been less studied by means of experimental models of TBI. However, several factors have been studied with regard to neural injury of various etiologies. Interleukin-8 (IL-8) is implicated in various inflammatory diseases of the central nervous system (CNS; Van Meir et al., 1992). Interleukin-10 (IL-10) has been proved to possess a neuroprotective influence attributable to its anti-inflammatory properties (Balasingam and Yong, 1996). Finally, interleukin-12 (IL-12) is implicated in autoimmune pathologies of the CNS (Becher et al., 2002). The response of these cytokines to brain trauma has been investigated mainly in clinical studies, as discussed later.
Furthermore, the role of neuro-inflammation regarding the evolution of traumatic injury, and consequently the influence of these mechanisms on the clinical outcome, are still under discussion. IL-1 is expressed more intensely after severe brain injury, even in remote areas of the brain (Kinoshita et al., 2002), and its widely accepted detrimental influence on outcome (Rothwell, 2003) has been indirectly demonstrated by the beneficial effect of its natural antagonist, IL-1ra (Tehranian et al., 2002; Toulmond and Rothwell, 1995). However, in some studies no relation with the outcome has been found (Knoblach and Faden, 2000), and it has been shown that IL-1 is also linked to neurotrophic mechanisms (DeKosky et al., 1996). The role of TNF-α after brain injury has been advocated to be detrimental by some relevant studies (Shohami et al., 1997), as it is responsible for delayed axonal damage (Kita et al., 2000). These properties are likely to have a negative impact on neurological outcome (Knoblach et al., 1999). Nevertheless, a favorable influence of TNF-α on both clinical and histological levels has also been demonstrated (Scherbel et al., 1999; Sullivan et al., 1999), strongly implying that this cytokine plays also a dual role regarding the sequelae of TBI. Concerning IL-6, it is considered necessary for the activation of neuro-inflammatory mechanisms (Penkowa et al., 1999), and its overall influence is probably neuro-protective after neural trauma (Swartz et al., 2001). Finally, the anti-inflammatory properties of IL-10 render it strongly neuro-protective after brain trauma, by an IL-1–suppressing mechanism (Knoblach and Faden, 1998).
Efforts to document the role of the above-mentioned phenomena in humans have been based mainly on clinical studies that detect elevated cytokine levels in the CSF and in the plasma of patients who have suffered severe head injuries. However, the efficacy of these studies is hampered by two issues. First, it is reasonable to argue that cytokines produced in the brain are highly diluted in the CSF (Woodroofe et al., 1991), and moreover, plasma is a pool in which such products of various deleterious processes (e.g., sepsis) accumulate, so minute fluctuations are likely to be undetected, and even the recorded ones may not result from events taking place in the CNS. Second, the concentration of cytokines in CSF and plasma, even when safely attributed to brain processes, reflect a global neuro-inflammatory response, and do not provide information concerning focal phenomena. These drawbacks have been overcome by the use of microdialysis. Apart from sampling directly from the extracellular fluid of the brain parenchyma, microdialysis offers the possibility to study the effect of minimal trauma, generated by the implantation of the micro-catheter itself (Mellergard et al., 2008).
However, all the microdialysis studies published until now concerning the fluctuation of cytokines as the result of trauma were performed on patients with severe traumatic, hemorrhagic, or ischemic brain injury. This methodological issue renders the interpretation of the findings ambiguous, mainly considering the efforts to detect the pure effect of a minimal, micro-catheter–induced trauma on the mechanisms of neuro-inflammation (Mellergard et al., 2008), as the post-traumatic general neuro-inflammatory and metabolic deterioration could possibly overwhelm the response to the micro-traumatic insertion of the catheter. Also, the global post-traumatic influence on neuro-inflammatory mechanisms, both in injured (Helmy et al., 2010; Hillman et al., 2007; Hutchinson et al., 2007), and in remote (Winter et al., 2004) brain locations, cannot be differentiated from the microtrauma effect evoked by the catheter implantation. To our knowledge, the present study is the first to measure the fluctuation of cytokines after the occurrence of microtrauma in brains that have not suffered severe acute injury, allowing more detailed recording of their concentrations in the post-implantation period.
Methods
Inclusion criteria
Patients suffering from drug-resistant epilepsy of extra-temporal origin who underwent intracranial electrode placement for the localization of the epileptic focus were included in this study. All the patients were selected through the diagnostic and therapeutic protocol for the surgical treatment of epilepsy used in the Department of Neurosurgery of the University of Athens (Unit of Surgical Treatment of Epilepsy). Namely, when a meticulous non-invasive investigation, which includes imaging (magnetic resonance imaging, magnetic resonance spectroscopy, and single-photon emission computed tomography) and neurophysiological (video-encephalography and Wada test) studies, along with the evaluation of the clinical features of epilepsy, fail to lead to the exact localization of the epileptic focus, an invasive investigation by the use of intracranial electrodes may be justified (Engel and Ojemann, 1993).
All the included patients signed an informed consent for the placement of microdialysis catheters along with deep intracranial electrodes. The research protocol aimed mainly to study cytokine fluctuations in the interstitial fluid of the brain parenchyma before and after epileptic activity, and data from microdialysis measurements were not integrated into the decision-making process regarding the treatment of epilepsy.
Surgical technique: Post-operative course
All patients underwent the craniotomies needed for the implantation of the deep and cortical electrodes. During the operation two or three microdialysis catheters were implanted in selected areas of the brain parenchyma, along with deep electroencephalogram (EEG)-recording electrodes. The choice of these areas was individualized and driven in each case by the indications of the antecedent non-invasive methods mentioned above. Hence by default, these areas included probable epileptic foci.
After the operation the patient was awakened and hospitalized in the video-EEG recording ward. The correct placement of intracranial electrodes and microdialysis catheters was confirmed by a brain CT scan (Fig. 1). The video-EEG recording was terminated after yielding adequate conclusions regarding the patient's further management. Then a second operation was performed for the realization of the decided surgical treatment, as indicated by the findings of the recording. At the same time, the microdialysis catheters were removed.
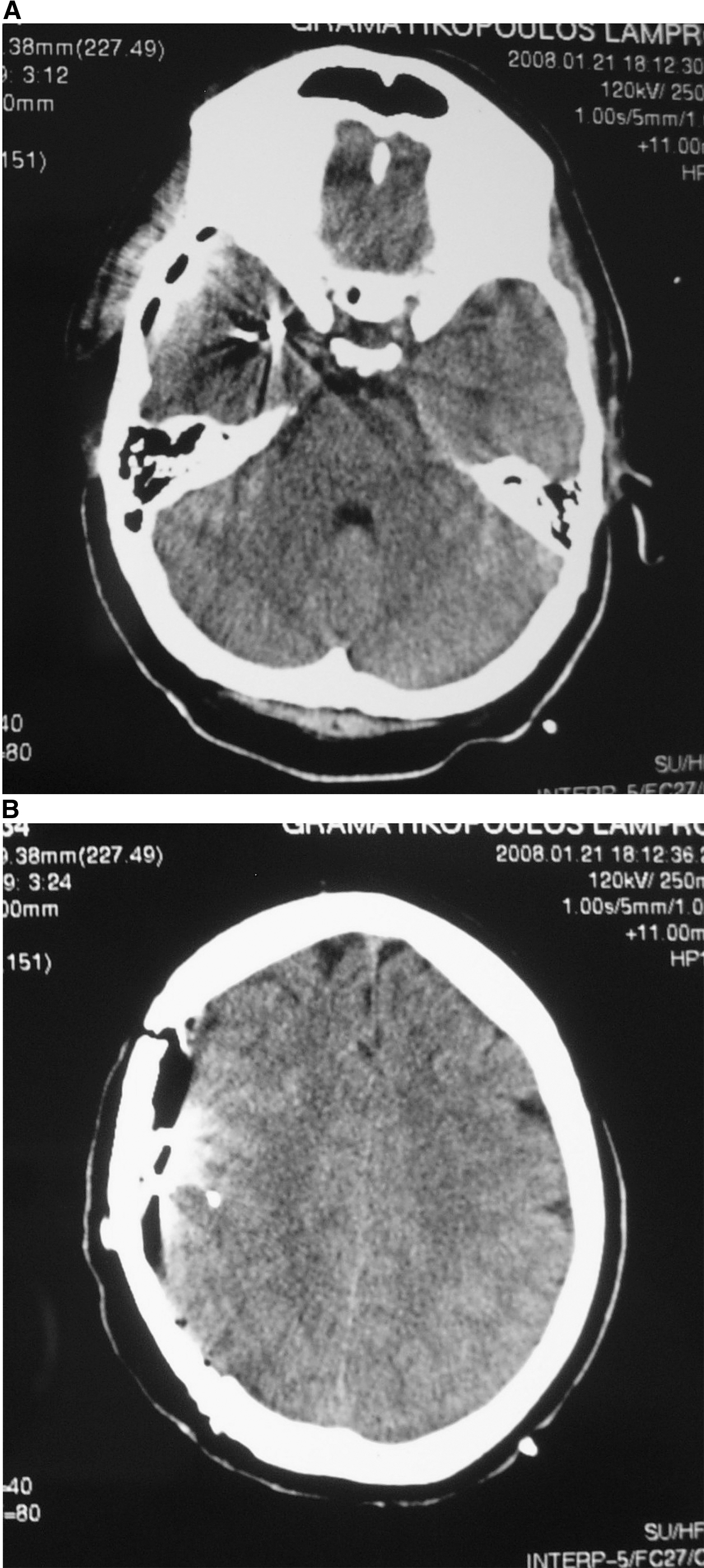
Computed tomography (CT) scan of a patient after the implantation of two microdialysis catheters, in the right medial temporal lobe (
Microdialysis: Sampling
The method of microdialysis has been widely used as a bedside monitoring tool to assess the evolution of brain damage after traumatic, ischemic, or hemorrhagic incidents. Likewise it has been the research tool of numerous studies, mainly concerning the above-mentioned pathologies. Recently, the ability to measure macromolecules has been added to monitor the metabolic markers of ischemia, and is being more frequently used in clinical practice (Bellander et al., 2004; Reinstrup et al., 2000). This represents a new way to apply microdialysis as a research tool. Some variations of the method have been described (Hillman et al., 2005,2006). In the present study, CMA 71 Brain MD microdialysis catheters (CMA Microdialysis, Solna, Sweden) were used in all cases. The membrane of this type of catheter is permeable to macromolecules, which renders them suitable for the measurement of cytokines in the dialysate (Hutchinson et al., 2005, 2007). These catheters were connected to CMA 107 pumps, with the perfusion rate adjusted to 0.3 μL/min.
The first sample was collected 2 h after implantation and sampling continued at 2-h intervals thereafter. Thus each collection micro-tube contained 36 μL of dialysate. For this study we used samples collected 2, 6, 12, 24, 48, 72, 96, and 120 h after implantation. Immediately after collection, the micro-tube was placed in deep refrigeration (−78°C), where it was stored until the time of measurement.
Cytokine measurement
We used bead flow cytometry for the measurement of cytokines in the collected dialysate. This method has been used in past studies, and it results in measurements of high validity (Elshal and McCoy, 2006), and permits the simultaneous measurement of multiple analytes in small sample volumes (Morgan et al., 2004), which was a necessity in the present study. The Luminex cytokine measurement kit was used (Biosource, Nivelles, Belgium); this enabled the measurement of IL-1, IL-6, TNF-α, IL-8, IL-10, and IL-12. The lowest value measurable by this method was 2.5 pg/mL for all of the cytokines. The highest value provided for each cytokine was 10,000 pg/mL. Higher concentrations necessitated multiple dilutions of the collected fluid, which was not feasible due to the small volumes.
Statistical analysis
For the fluctuation of cytokine concentrations in the brain parenchyma after microdialysis catheter implantation, boxplot diagrams were built. First the overall statistical significance of the post-microtraumatic fluctuation of each cytokine was tested by the Kruskal-Wallis test. The statistical significance of the variations of values at each time point was tested using non-parametric Wilcoxon paired analysis. The Wilcoxon index (Z) and the resulting statistical significance as expressed by p value was calculated.
We constructed general linear models for the analysis of differences between fluctuation curves. We used linear regression models for the analysis of factors influencing cytokine values and their interdependence.
In all cases, p values <0.05 were defined as statistically significant. We used SPSS 17.0 software to perform these calculations.
Results
Patients, sampling, and cytokine measurements
Twelve patients were included in this study. Another two underwent invasive EEG monitoring after a second operation for electrode placement, due to focus localization issues. Thus cytokine fluctuations after microdialysis catheter implantation was recorded in 14 cases. None of the patients had any complications attributable to microdialysis catheter implantation. One patient had post-operative meningitis 4 days after the second operation, which was performed to treat epilepsy. This was attributed to a CSF leak from one of the skin exit points of the electrodes, which occurred during EEG monitoring. The patient's condition improved with focused antibiotic treatment.
For this microdialysis protocol, 31 catheters were implanted. Four of the catheters had major malfunctions, and the other 27 yielded a reliable series of cytokine measurements. The mean time of microdialysis sampling was 4.05 days. In total, 186 microvials were collected, containing interstitial fluid in which at least one of the cytokines had a measurable value. Patient characteristics and data concerning the microdialysis catheters are shown in Table 1.
Patient Demographics and Exact Locations of Microdialysis Catheter Implantation
These two patients underwent a second operation for electrode re-placement.
Detectable levels of IL-1 were found in 137 samples, ranging from trace amounts to 827.4 pg/mL. IL-6 had quantities that covered the spectrum of measurable values. It was measurable in 154 samples, whereas in 5 of the samples its concentration was undetectable, and in 27 samples it was higher than the highest measurable level. IL-8 was measurable in 161 samples. In 10 of them its value was undetectable, and in 15 it was above the highest identifiable level. IL-10 was measurable in 132 samples and undetectable in 54 (the highest measured concentration was 16.2 pg/mL), while IL-12 was detectable in 102 samples and undetectable in 84 (the highest measured concentration was 14.0 pg/mL). TNF-α was measurable in 108 samples and undetectable in 78 (the highest measured concentration was 72.7 pg/mL). The values of the six cytokines are shown in Table 2.
Microdialysis Sampling Results
Shown are the numbers of samples in which the cytokines were of measurable concentrations. The two numbers in parentheses are the numbers of samples that had values lower than minimum detectable values, and higher than maximum measurable values, respectively. The values shown in the columns “Minimum value” and “Maximum value” correspond to the lowest and highest levels recorded in an individual patient.
IL-1, interleukin-1; IL-6, interleukin-6; IL-8, interleukin-8; IL-10, interleukin-10; IL-12, interleukin-12; TNF-α, tumor necrosis factor-α.
Concerning the fluctuation of cytokines, The Kruskal-Wallis test revealed statistically significant variations in the levels of IL-1, IL-6, IL-8, and TNF-α. These results are shown in Table 3.
Statistical Significance of Cytokine Fluctuations Within the First 120 Hours After Micro-catheter Implantation by Kruskal-Wallis Testing
IL-1, interleukin-1; IL-6, interleukin-6; IL-8, interleukin-8; IL-10, interleukin-10; IL-12, interleukin-12; TNF-α, tumor necrosis factor-α.
IL-1
The median values of IL-1 at successive time points after catheter implantation are shown in Table 2. Its concentration was raised at 2 h and peaked 6 h after implantation. Thereafter it declined to baseline levels (Fig. 2). Statistical analysis showed that a statistically significant decline continued until 48 h post-implantation. Median IL-1 values decreased from 42.5 pg/mL at 6 h post-implantation, to 21.1 pg/mL at 12 h (p=0.001), 11.4 pg/mL at 24 h (p=0.014), and to 4.1 pg/mL at 48 h (p=0.031) post-implantation, as shown in Table 4. Thereafter the values stabilized and further fluctuations were not statistically significant.

Boxplot showing the fluctuations in interleukin-1 (IL-1) levels (*statistically significant fluctuation).
Median Concentrations of the Studied Cytokines at Each Time Point After Catheter Implantation
These values correspond to the significance of the difference of each median value compared to the previous one. Statistically significant differences are shown in bold.
IL-1, interleukin-1; IL-6, interleukin-6; IL-8, interleukin-8; IL-10, interleukin-10; IL-12, interleukin-12; TNF-α, tumor necrosis factor-α.
IL-6
IL-6 concentrations peaked 6 h after catheter implantation. High levels were maintained for 24 h, after which they decreased gradually (Fig. 3). Median values are presented in Table 2. The decline remained statistically significant, as the value dropped from 3688.0 pg/mL at 24 h to 1019.8 pg/mL at 48 hours (p=0.001), to 242.2 pg/mL at 72 h (p=0.041), to 48.0 pg/mL at 96 h (p=0.007), and finally to 22.5 pg/mL at 120 h post-implantation (p=0.043). This analysis is also shown in Table 4.
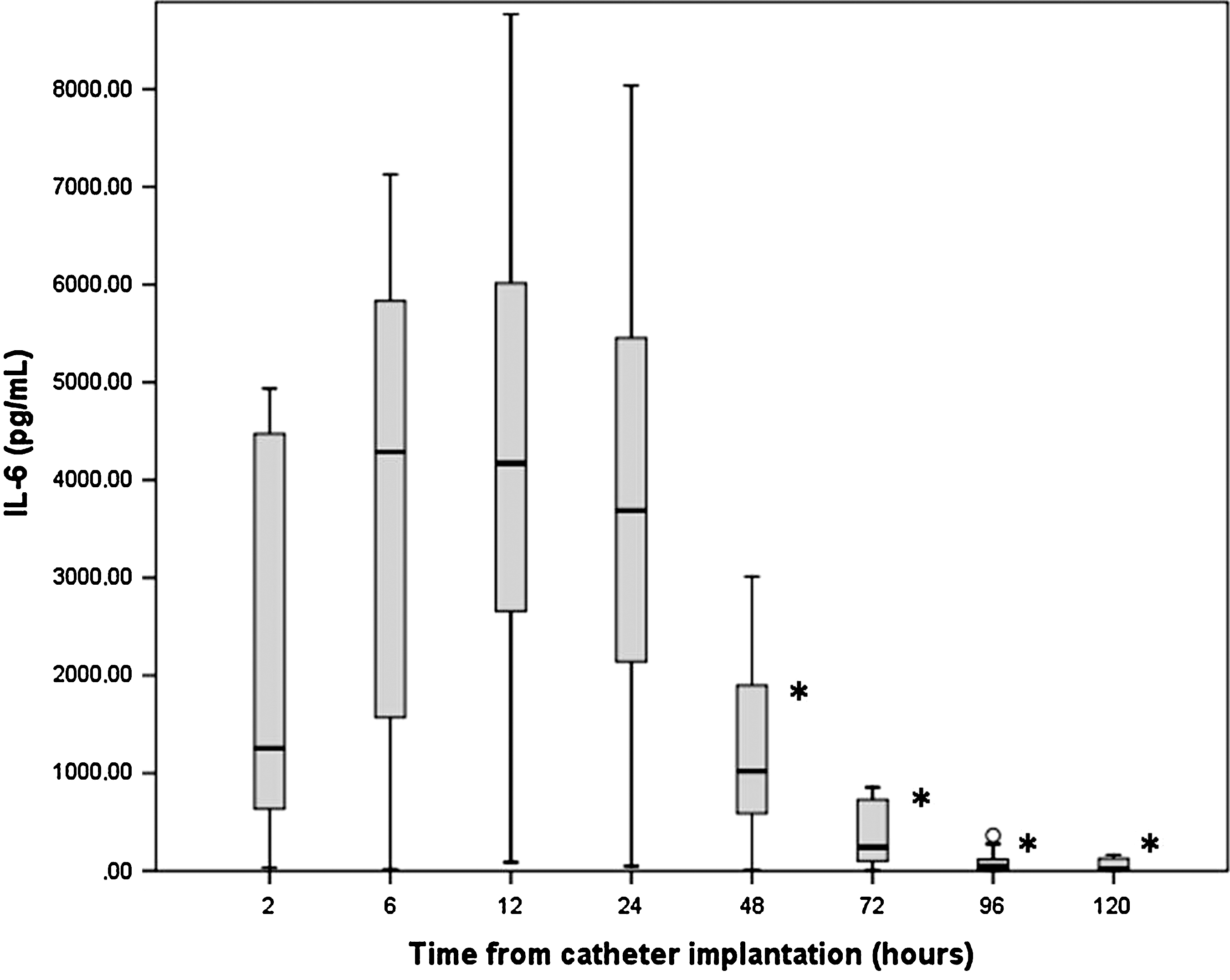
Boxplot showing the fluctuations in interleukin-6 (IL-6) levels (*statistically significant fluctuation).
IL-8
Six hours after implantation IL-8 reached its peak value. The decline that followed remained statistically significant until 48 h post-implantation. At 6 h the median IL-8 concentration was 3819.2 pg/mL. At 12 h after implantation it dropped to 1651.8 pg/mL (p=0.003), at 24 h to 878.5 pg/mL (p=0.001), and at 48 h to 308.4 pg/mL (p=0.009). Thereafter the decrease continued without reaching statistical significance (Fig. 4). These values, along with all median IL-8 values at successive post-implantation time points, are cited in Table 4.

Boxplot showing the fluctuations in interleukin-8 (IL-8) levels (*statistically significant fluctuation).
TNF-α
The median value of TNF-α 2 h after implantation was 5.6 pg/mL. At 6 h this fell to 3.7 pg/mL, a decrease that was statistically significant (p=0.035). After this point, the changes in TNF-α levels were not statistically significant (Fig. 5). These data are presented in Table 4.

Boxplot showing the fluctuations in tumor necrosis factor-α (TNF-α) levels (*statistically significant fluctuation).
IL-10 and IL-12
Concerning these two cytokines, no statistically significant fluctuations were recorded during the first 120 post-implantation hours (Figs. 6 and 7). The median values of IL-10 fluctuated between 3.7 and 4.9 pg/mL, and median values of IL-12 varied between 3.1 and 3.9 pg/mL, while no IL-12 was found in the vials collected 120 h after catheter implantation. These data are also presented in Table 4.
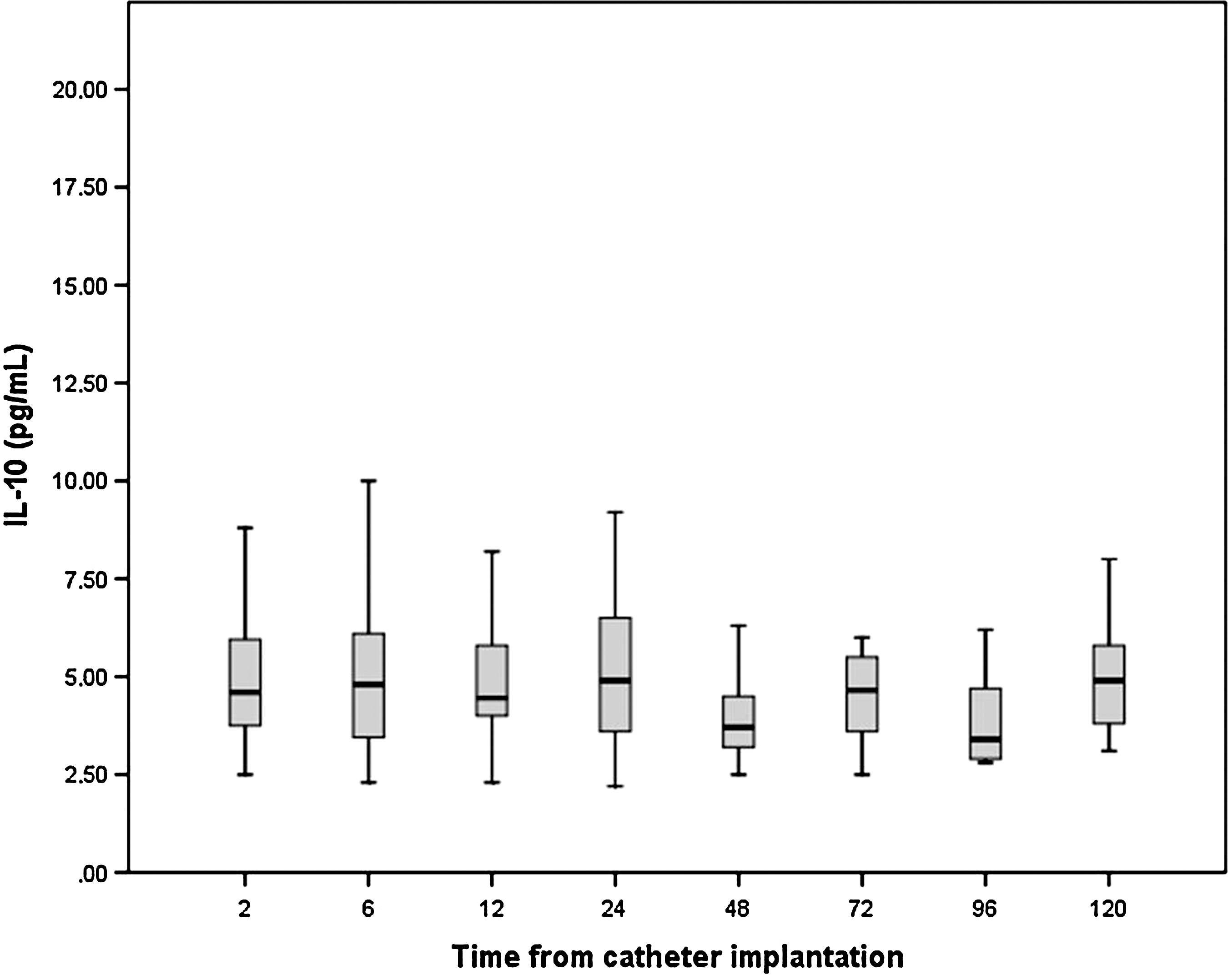
Boxplot showing the fluctuations in interleukin-10 (IL-10) levels (*statistically significant fluctuation).

Boxplot showing the fluctuations in interleukin-12 (IL-12) levels (*statistically significant fluctuation).
The influence of gliosis and epileptic activity on the results
As mentioned above, this study was performed in the context of a protocol aiming to investigate the relationship between epileptic activity and neuro-inflammation, by the use of microdialysis catheters implanted in the brain parenchyma of chronic epileptic patients while they were under video-EEG monitoring by intracranial electrodes. The characteristics of our patient population influenced the interpretation of the results concerning the neuro-inflammatory sequelae of micro-trauma. For that reason, we have cited here the most relevant results of the epilepsy-oriented part of the study, in order to clarify any possible relationships.
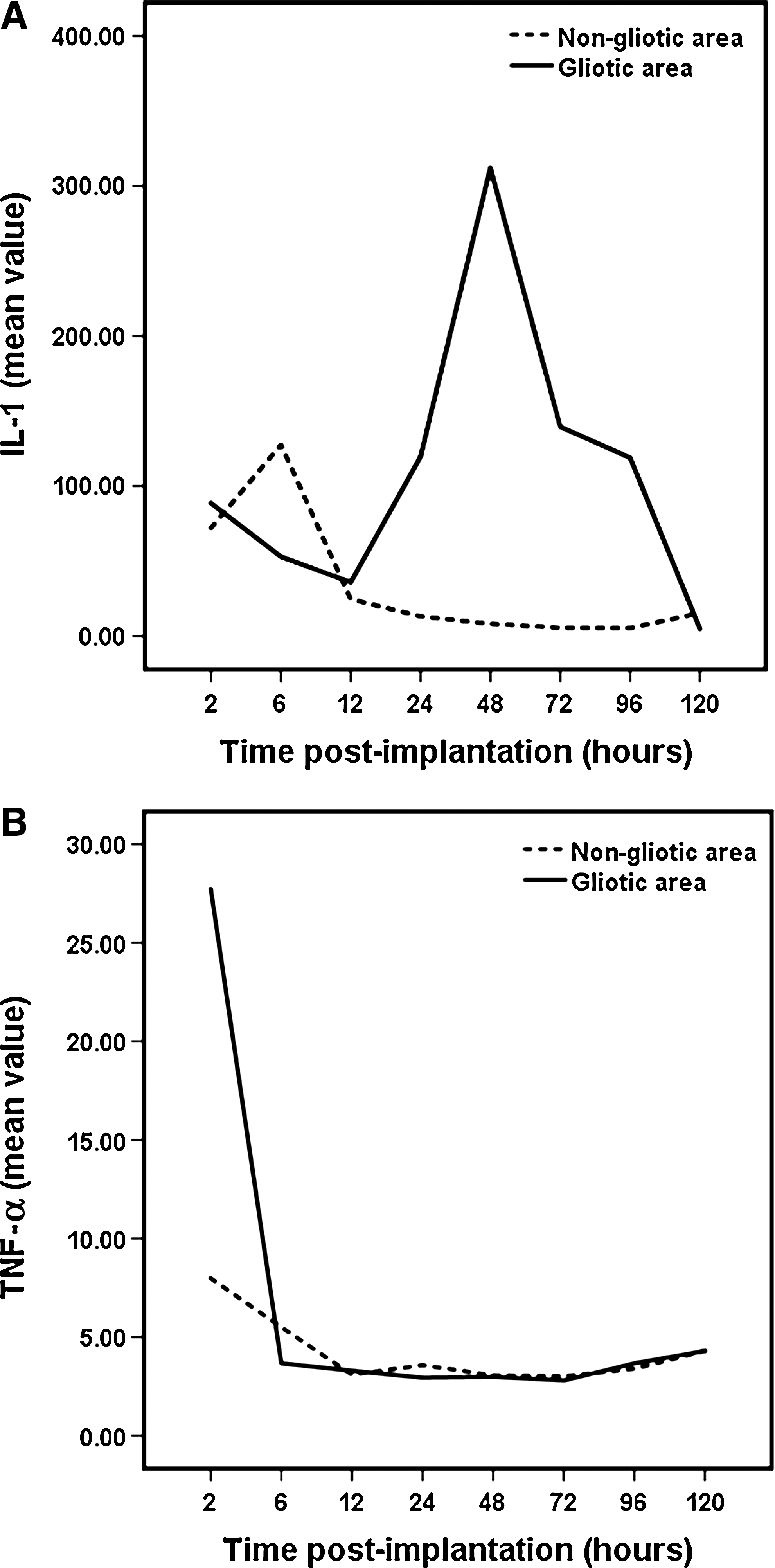
The post-implantation fluctuations of IL-1 and TNF-α were interpreted to reveal any possible differences in the fluctuation in gliotic and in non-gliotic areas. The two fluctuation curves for IL-1 are shown in Figure 8A. The use of general linear model analysis revealed a statistically significant difference between the two curves (p=0.004). From this graph it is obvious that the micro-traumatic response of IL-1 is more intense in gliotic areas. Regarding TNF-α, its post-implantation response in gliotic and non-gliotic areas is shown in Figure 8B. The difference between the two curves was statistically significant (p=0.029). Regarding IL-6 and IL-8, no statistically significant difference was found for their response in gliotic and non-gliotic areas (p=0.852 and p=143, respectively). Data were not sufficient to assess the levels of IL-10 and IL-12.
(
The influence of epileptic seizures on the values of IL-1 and IL-6, as measured at least 48 h after the catheter implantation, is presented in Table 5. Concerning IL-1, at no time point did we find a statistically significant value shift. In contrast, the value of IL-6 was significantly increased 24 h after the seizure (p=0.046), and levels declined thereafter, with the decrease being statistically significant in the period 48–72 h after the seizure (p=0.041). However, this significant change in IL-6 levels was not verified by Kruskal-Wallis analysis, as shown in Table 6 (p=0.079). In the same table, we present the results of a regression analysis concerning various possible factors that may influence the levels of IL-6 in samples collected at least 48 h after implantation. This analysis proved that the most important factor is the length of time post-implantation, which verifies the prolongation of the micro-trauma effect for long after 48 h post-implantation for IL-6. The corresponding analyses did not reveal significant effects of epileptic activity for any of the other studied cytokines.
Median Values of Interleukin-1 (IL-1) and Interleukin-6 (IL-6) at Various Points After Epileptic Activity
Statistically significantly different values compared to the previous values are shown in bold.
Linear Regression Analysis of the Factors Influencing the Levels of Interleukin-6 (IL-6) Post-48 Hours After Implantation
The tolerance index is the relevance of each significant factor in the statistical prediction model.
Discussion
Methodological issues and possible drawbacks
The methodology of the present study allowed the sampling of extracellular fluid from brains not subjected to severe trauma. The use of microdialysis, a minimally-traumatic method, in patients without cerebral injury, was justified along with the use of deep intracranial electrodes, which was deemed necessary given the severity of their epilepsy and the expected benefit of the operative treatment. Microdialysis has been used in similar cases in some studies in the past, mainly for the measurement of neurotransmitters (During and Spencer, 1993; Wilson et al., 1996), and metabolic markers of ischemia (Cornford et al., 2002; During et al., 1994), and their correlation with seizure occurrence, while another study used the same methodology to correlate adenosine levels with the phases of sleep (Zeitzer et al., 2006).
Concerning possible drawbacks, the cytokine concentrations in the brain parenchyma may be underestimated using this method (Hillman et al., 2005; Hutchinson et al., 2005), due to a depleting effect in the catheter's micro-environment resulting from the continuous fluid perfusion (Clough et al., 2002). However, this effect is an intrinsic disadvantage of the method, affecting all the relevant studies. Furthermore, what is more interesting and more objectively interpretable is the trend toward cytokine fluctuation, a concept that is widely accepted regarding the clinical application of the method to assess the markers of ischemia. We reasonably assume that in our study the fluctuations of the measured cytokines can be safely interpreted.
The microdialysis catheters were inserted in proximity to deep electrodes used to monitor electroencephalographic activity. This could lead to the hypothesis that the neuro-inflammatory reaction recorded in this study was a result of the electrode implantation and not of the catheter itself. However, these electrodes are minimally-invasive themselves, and even in this case, the micro-trauma caused is comparable to that related to micro-dialysis. Hence this fact does not alter the essence of our conclusions.
Due to the characteristics of the patient population, some of the catheters were implanted in gliotic brain areas. Cerebral gliosis in these cases is not the result of an acute traumatic insult, but it still may affect neuro-inflammatory processes (De Simoni et al., 2000; Eriksson et al., 1999). According to the cited data from the same study protocol, the fluctuations of IL-1 and TNF-α in gliotic areas is significantly, albeit slightly, more intense than in healthy brain areas. For these two cytokines there is evidence of a significant post-micro-traumatic reaction. However, due to the above-mentioned drawbacks related to chronic gliosis, the results of the present study concerning the micro-traumatic responses of IL-1 and TNF-α should be interpreted with caution.
Also, all of these patients had epileptic seizures during monitoring. There is evidence that epileptic activity influences neuro-inflammatory mechanisms, which are often accompanied by cytokine increases within the brain parenchyma (De Simoni et al., 2000; Lehtimaki et al., 2003; Peltola et al., 2000). The interpretation of this relationship is beyond the scope of the present study. However, it may be hypothesized that epileptic activity may alter the cytokine fluctuation patterns that are otherwise attributed to micro-trauma. According to data from our patients concerning the influence of seizures on the cytokine levels after the micro-trauma effect ends, as shown in Tables 5 and 6, epileptic seizures only cause a significant rise in IL-6 levels. Hence the action of IL-1 is unaffected by the occurrence of epileptic activity. Moreover, the linear regression analysis that we performed proved that IL-6 levels remained statistically significant during the entire 120-h monitoring period. The significance of the influence of epileptic activity was thus not confirmed, and IL-6 has a tolerance index of 97.5% (Table 6), meaning that the results can be explained by a time-dependent model in 97.5% of the samples. Finally, the distribution of these incidents within the monitoring period, and during the subsequent period post-micro-trauma, is random, and does not influence the pattern of the cytokine fluctuation attributed to micro-trauma, even for IL-6.
Cytokine concentrations and fluctuations
The post-traumatic concentrations of IL-1 have been found to be raised in the CSF of patients with TBI (Chiaretti et al., 2005; Hayakata et al., 2004; Shiozaki et al., 2005). This increase was confirmed to occur in the brain parenchyma by studies that used microdialysis (Helmy et al., 2010; Hillman et al., 2007; Hutchinson et al., 2007; Mellergard et al., 2008; Winter et al., 2004). In particular, increased extracellular IL-1 has been shown to be more associated with post-traumatic ischemia than to macroscopically-injured parenchyma (Hillman et al., 2007), and to correlate with worse outcomes (Hutchinson et al., 2007). Parenchymal IL-1 was also found to reach significantly higher levels than in plasma. In these studies, levels of extracellular IL-1 in the brain were raised 6–24 h after micro-catheter insertion, and subsided to lower values thereafter (Helmy et al., 2010; Mellergard et al., 2008).
The fluctuations of IL-1 recorded in our study peaked 6 h after microtrauma. This pattern is generally in accord with the IL-1 response seen after brain trauma, as has been described in other experimental studies (Giulian and Lachman, 1985; Nieto-Sampedro et al., 1987; Woodroofe et al., 1991), and also in clinical studies that measured IL-1 levels in the CSF (Hayakata et al., 2004), or the extracellular fluid (Helmy et al., 2010; Mellergard et al., 2008). However, unlike findings of similar microdialysis studies measuring the effects of microtrauma, we found that levels did not normalize until 24 h post-implantation (Helmy et al., 2010; Mellergard et al., 2008).
The response of IL-6 after TBI has also been the subject of numerous studies. At a clinical level, most of these studies have found considerably increased concentrations of IL-6 in the CSF (Chiaretti et al., 2005; Hayakata et al., 2004; Kossmann et al., 1995,1996; Kushi et al., 2003; Maier et al., 2001; McClain et al., 1991; Singhal et al., 2002). These studies had diverse IL-6 fluctuation patterns, with peaks reported to occur 6 h post-injury (Hayakata et al., 2004), 24 h post-injury (Chiaretti et al., 2005, Kushi et al., 2003), and even up to 7 days post-injury (Kossmann et al., 1996). Astrocytes have been shown to be a source of IL-6 production after TBI (Hariri et al., 1994). IL-6 in the post-injury period has been found to be beneficial by most researchers (Singhal et al., 2002; Winter et al., 2004). Nevertheless, neutral (Kalabalikis et al., 1999) and unfavorable (Chiaretti et al., 2005; Hayakata et al., 2004) effects of CSF or plasma levels have also been described.
Some microdialysis studies have endeavored to delineate the pattern of IL-6 fluctuations after head injury (Helmy et al., 2010; Hillman et al., 2007; Winter et al., 2004), or after insertion-induced micro-trauma (Mellergard et al., 2008). According to these studies, major head trauma leads to raised extracellular levels of IL-6 within the first post-traumatic day, subsiding on the second day (Helmy et al., 2010; Hillman et al., 2007), while post-implantation fluctuations are reported to peak 12 h after catheter insertion (Mellergard et al., 2008). Our results showed a substantially different pattern, consisting of a peak lasting from 6–24 h post-implantation, which was followed by a continuous decline that did not reach baseline levels until 120 h post-implantation, indicating micro-trauma effects lasting at least 5 days.
Both the lymphocyte-promoting and angiogenetic properties of IL-8 have been proven to play an important role in the response to brain trauma (Zlotnik et al., 2000). Raised concentrations of IL-8 have been recorded during the post-traumatic period in the plasma and CSF of patients (Hayakata et al., 2004; Kushi et al., 2003; Maier et al., 2001; Whalen et al., 2000), with peak values reported within the first 24 h, and by microdialysis in the extracellular fluid of the brain parenchyma (Helmy et al., 2010; Mellergard et al., 2008). Furthermore, most authors advocate a correlation of raised IL-8 with unfavorable outcomes (Hayakata et al., 2004; Kushi et al., 2003; Whalen et al., 2000), attributed to its triggering of an immune reaction, while the pathophysiology of CNS damage is thought to play an important role in the dysfunction of the blood–brain barrier (Kossmann et al., 1997). In a study assessing microtrauma's effects by the use of microdialysis, IL-8 levels were attenuated up to 6 h after catheter implantation (Mellergard et al., 2008). In our study this pattern was confirmed. Moreover, a gradual rise occurred before this peak, starting at 2 h post-implantation, a finding not seen in past reports. The values of extracellular IL-8 continued to decrease until day 5; however, statistical significance was only documented up to 48 h post-implantation.
TNF-α is implicated in the neuro-inflammatory sequelae of brain injury, particularly in the secondary phenomena and the occurrence of brain damage through biochemical paths leading to neuronal apoptosis. Concerning its fluctuations seen after TBI, TNF-α has been shown to rise in the CSF (Stover et al., 2000) and the brain parenchyma (Knoblach et al., 1999) immediately after trauma in experimental studies. On a clinical level, this increase has been measured by a few studies in the CSF of patients with TBI (Hayakata et al., 2004; Shiozaki et al., 2005). In a microdialysis study, TNF-α concentrations in the extracellular fluid have also been found to increase (Helmy et al., 2010). In our study, TNF-α levels were already increased at the first point of evaluation 2 h after implantation, and then plateaued before returning to baseline levels.
The role of IL-10 in brain damage remains unclear. This cytokine, which has well-documented anti-inflammatory properties, has been found to be raised in the CSF in clinical studies after TBI (Hayakata et al., 2004; Shiozaki et al., 2005). However, its rate increase is significantly lower than that of other cytokines, implying that the IL-10 activation threshold is higher than those of other factors, whereas some studies have shown constant CSF levels of IL-10, indicating that its increase in plasma is the result of peripheral neuro-inflammatory processes (Maier et al., 2001). Although increased IL-10 values have been correlated with unfavorable outcomes (Shiozaki et al., 2005), its injection in animals improved outcomes (Knoblach and Faden, 1998). Apart from the above-mentioned studies that measured IL-10 in the CSF and the plasma of patients with severe brain injury, its concentration in the extracellular fluid has been found to be increased in a study using microdialysis in a similar population on the fourth post-traumatic day (Helmy et al., 2010), while after micro-trauma it did not show any significant fluctuations (Mellergard et al., 2008). In the present study, IL-10 fluctuations were characterized by an absence of peaks, advancing the hypothesis that the activation of IL-10-related mechanisms do not have the same intensity in the brain as other inflammatory mediators.
Finally, IL-12 has been less studied, considering its response to cerebral trauma. In a microdialysis study it has been found to increase several days after severe brain injury (Helmy et al., 2010). Another study found significantly increased levels of IL-12 in the CSF of patients with head injuries (Stahel et al., 1998). In the present study, no significant fluctuations were documented, which implies a limited role after TBI.
Conclusions regarding the effects of micro-trauma
Overall, the present study permits a clear examination of the effect of micro-trauma on the mechanisms of neuro-inflammation. Also, even if the chronically epileptic brain is not technically injured, it is certainly affected by the biochemical disturbances seen following traumatic injury, which influences neuro-inflammatory processes. Furthermore, a retrospective consideration of the results reveals that the median values of all cytokines were at very low levels, approaching the non-detectable levels of cytokines seen in the normal CNS. This indicates that our patient population is nearly normal from a neuro-inflammatory point of view.
The measurement of cytokines in this micro-environment, which is significantly more disengaged from the global neuro-inflammatory turbulence induced by severe brain injury than the patients in other relevant studies, reveals an intense response of IL-6, which lasts for at least 5 days after catheter insertion. Moreover, IL-1 and IL-8 had fluctuations lasting at least 48 h and peaking 6 h post-implantation, whereas TNF-α peaked 2 h after the occurrence of micro-trauma. These data supplement similar findings of other studies. On the contrary, IL-10 did not respond to micro-trauma, indicating that the threshold for its activation (as has been shown in studies performed on severely damaged brains) is significantly higher than that of the other factors.
Apart from conclusions related to the interactions between traumatic and neuro-inflammatory events, the results of the present study lead to interesting conclusions about the concessions made regarding the use of invasive monitoring methods. It is obvious that even a micro-traumatic incident is sufficient to alter the micro-environment of the brain, raising questions about the damage done using this method (Stenken et al., 2010). Concerning the brain, the alterations seen last for several days in some cases, such as those that occur for IL-6, IL-1, and IL-8. This prolonged effect may be adequate to refute the argument that in the case of microdialysis, measurements can be safely interpreted 24 h after implantation. This also renders dubious the interpretation of the fluctuations in cerebral cytokines made in other microdialysis studies, which may have underestimated the effects of micro-trauma (Hillman et al., 2007; Winter et al., 2004).
Baseline cytokines levels
The estimation of baseline cytokine levels in the extracellular fluid of the brain parenchyma is theoretically feasible according to our data, given the application of microdialysis in non-traumatized brains. Nevertheless, it is probable that these measurements will yield values deviating from those seen in normal brains, as the epileptic brain, though it is not acutely damaged, cannot be considered to be normal, particularly from a neuro-inflammatory point of view. Thus as expected, cytokine levels were lower than those found in other microdialysis studies performed on more seriously injured brains (Hillman et al., 2007; Mellergard et al., 2008). In particular, IL-1 peaks at values of 4.0–5.5 pg/mL, IL-6 at 50 pg/mL, and IL-8 at levels below 100 pg/mL. TNF-α, IL-10, and IL-12, baseline levels vary between 3.0 and 5.0 pg/mL.
Footnotes
Author Disclosure Statement
No competing financial interests exist.