
Abstract
Guidelines for patients with severe traumatic brain injury (sTBI) published in 2007 recommend providing early nutrition after trauma. Early enteral nutrition (EN) started within 48 h post-injury reduces clinical malnutrition, prevents bacterial translocation from the gastrointestinal tract, and improves outcome in sTBI patients sustaining hypermetabolism and hypercatabolism. The aim of this study was to examine the effect of early EN support on survival rate, Glasgow Coma Scale (GCS) score, and clinical outcome of sTBI patients. Medical records of sTBI patients with GCS scores 4–8 were recruited from 18 hospitals in Taiwan, excluding patients with GCS scores ≤3. During 2002–2010, data from 145 EN patients receiving appropriate calories and nutrients within 48 h post-trauma were collected and compared with 152 non-EN controls matched for gender, age, body weight, initial GCS score, and operative status. The EN patients had a greater survival rate and GCS score on the 7th day in the intensive care unit (ICU), and a better outcome at 1 month post-injury. After adjusting for age, gender, initial GCS score, and recruitment period, the non-EN patients had a hazard ratio of 14.63 (95% CI 8.58–24.91) compared with EN patients. The GCS score during the first 7 ICU days was significantly improved among EN patients with GCS scores of 6–8 compared with EN patients with GCS scores of 4–5 and non-EN patients with GCS scores of 6–8. This finding demonstrates that EN within 48 h post-injury is associated with better survival, GCS recovery, and outcome among sTBI patients, particularly in those with a GCS score of 6–8.
Introduction
V
The routes chosen for nutritional support include enteral and parenteral feedings. In 1980s, Rapp and colleagues reported that total parenteral nutrition (TPN) provided better and easier nutritional support in brain-injured patients than enteral nutrition (EN), and produced improved outcomes (Rapp et al., 1983; Young et al., 1987b). However, other reports indicated that there is no difference in calorie intake and nitrogen balance between TPN and EN, when they persistently attempted to provide EN for sTBI patients (Borzotta et al., 1994; Hadley et al., 1986; Hausmann et al., 1985). Administering EN to sTBI patients has been associated with fewer complications and infection, better gastrointestinal capability and integrity, less hyperglycemic risk, and lower cost compared with TPN (Grahm et al., 1989; Hadley, 1996; Lepelletier et al., 2010; Suchner et al., 1996). However, gastrointestinal intolerance that may cause diarrhea, and abdominal distension is a potential difficulty with providing early EN to injured patients. It has been reported that several strategies, such as post-pyloric feeding, semi-recumbent position, feeding rate downregulation, formula modulation, and use of pro-motility agents may facilitate early EN support for nutritional improvement in critical care patients (Cook et al., 2008; Grahm et al., 1989; Hadley, 1996; Kattelmann et al., 2006; Rhoney et al., 2002). Recently, several studies have recommended that EN should be supplied to sTBI patients immediately after trauma, but that TPN should be provided when the EN cannot be supported, or nutritional goals have not been reached by EN by 1 week post-injury (Cook et al., 2008; de Aguilar-Nascimento and Kudsk, 2008; Pepe and Barba, 1999; Wilson and Tyburski, 1998).
The objectives of this multi-center cohort study were to investigate the effect of EN support (provided within 48 h post-trauma) with non-EN support (given by only intravenous transfusion for 7 days) on the survival rate and Glasgow coma scale (GCS) score of sTBI patients for the first 7 days in the intensive care unit (ICU), and the clinical outcome of patients at 1 month post-injury. The initial GCS score (4–5 or 6–8) was further used to estimate the effect of different nutritional support on survival rate and GCS score variations over 7 ICU days.
Methods
Patient collection
This study was approved by the relevant institutional review board for human research in Taiwan, and the procedure complied with the Declaration of Helsinki. The medical records of patients used in this study were collected from 18 hospitals in Taiwan, including Mackay Memorial Hospital, National Taiwan University Hospital, Taipei Veterans General Hospital, Tri-Service General Hospital, Taipei City Hospital Renai Branch, Buddhist Tzu Chi General Hospital Taipei Branch, Shin Kong Wu Ho-Su Memorial Hospital, Taipei Medical University Hospital, Taipei Municipal Wan Fang Hospital, Chung Shan Hospital, Changhua Christian Hospital, Central Clinic General Hospital, Po-Jen General Hospital, Taiwan Adventist Hospital, Taipei City Hospital Zhongxing Branch, Taipei City Hospital Yangming Branch, Chi-Mei Medical Center, and Hualien Armed Forces General Hospital.
Patients with sTBI and GCS scores between 4 and 8 were eligible for recruitment into this human study from January 2002 to May 2010. Patients with a GCS score ≤3 were excluded because their condition was too severe to allow feeding. The data collected included the recruitment time, gender, age, body weight, initial GCS score, operative status, and nutritional intervention. Further data obtained included GCS score and survival during the first 7 days in the ICU and, finally, the outcome at 1 month post-injury. Regular meetings were held between the hospitals to verify that all eligible patients were enrolled, and that the recording was complete.
Nutritional support
We further excluded the effect of TPN support because there were no more than 5 cases of sTBI patients provided with TPN from the 1st to the 7th ICU day. The number of patients supplied with EN after the 3rd ICU day was small, and these patients were also excluded. A total of 297 cases were collected, including 145 EN patients and 152 non-EN patients. Patients in the EN group received nutrition consisting of 52.9% carbohydrate, 31.1% fat, and 16.4% protein, beginning within 48 h post-injury. Calories were supplied starting at 500 kcal/patient/day and increased gradually to the estimated requirement of each patient. Patients in the non-EN group were given intravenous transfusion only, to maintain the balance of fluid and electrolytes over 7 ICU days. Comparisons of demographic data between non-EN and EN patients are shown in Table 1. The distribution of gender, age, body weight, initial GCS score, and operative status were similar across the two groups.
Statistical analysis
After the data were cleaned and checked for completeness, descriptive statistics were generated and univariate categorical comparisons (χ2-test) were made between the non-EN and EN groups. The variables used included the recruitment time (2 categories), gender (male or female), age (4 categories), body weight (5 categories), initial GCS score (2 categories), operative status (yes or no), and outcome (5 categories). The Kaplan-Meier method was used to construct survival curves of sTBI patients, and the log-rank analysis was used to test the survival rate of these patients with different nutritional supports and initial severities over 7 ICU days. The survival rate was also evaluated by using a Cox regression model to examine multivariate hazard ratio (HR) between non-EN and EN patients before and after adjusting for their age, gender, initial GCS score, and recruitment period. The GCS scores of sTBI patients in different nutritional groups and injury severities over 7 ICU days were analyzed using the repeated-measure analysis of variance (ANOVA) and multiple Bonferroni comparisons test, and the data are expressed as means±SD.
All statistics were performed by using the SPSS software (SPSS, Chicago, IL), version 17.0. The differences were considered significant at p<0.05.
Results
The percentage of sTBI patients who had EN support increased significantly between 2007 and 2010 (p=0.005) as is shown in Table 2. The survival curve over 7 ICU days improved slightly during 2007–2010 (p=0.073) compared with that observed during 2002–2006 (data not shown).
Table 3 shows the outcome of non-EN and EN patients at 1 month post-injury. Clinical outcome for the EN patients was significantly better (p<0.001) than for the non-EN patients, with fewer deaths. Over the first 7 ICU days, the survival curve of non-EN patients was markedly reduced (p<0.001) compared with the EN group (Fig. 1A). The survival rate was 89.0% among EN patients on the 7th ICU day, compared with only 15.8% for the non-EN group. The risk of fatality in non-EN patients was significantly increased in comparison with that in EN patients (HR 13.55, 95% CI 8.00–22.92). After adjusting for age, gender, initial GCS score, and recruitment period, the non-EN patients still had an HR of 14.63 (95% CI 8.58–24.92) compared with EN patients. In addition, GCS scores among EN patients were significantly increased (p<0.05) in comparison with non-EN patients, especially on the 5th, 6th, and 7th ICU days (Fig. 1B).

Survival rate (
The survival rates and GCS scores were further evaluated by the sub-grouping of patients into initial GCS scores of 6–8 (Group A) and 4–5 (Group B). Total sTBI patients in Group A revealed a markedly better survival rate (p<0.05) than patients in Group B over 7 ICU days (data not shown). In addition, the GCS scores of all patients in Group A were significantly higher (p<0.001) than those in Group B from the 1st to 7th ICU day (data not shown). When controlled for nutritional support, the GCS score of EN patients in Group A was still significantly increased (p<0.001) each day within 1 week post-injury period in the ICU compared with that of EN patients in Group B (Fig. 2A). However, no significant difference was observed between the different initial severities among non-EN patients since the 3rd ICU day (Fig. 2B). In addition, GCS scores were significantly elevated in EN patients (p<0.05) compared with non-EN patients within Group A, particularly from the 2nd to the 7th ICU day (Fig. 2C). The EN patients still had higher GCS scores than the non-EN patients within Group B on the 2nd, 3rd, 4, and 5th ICU days, although the difference was not significant between EN and non-EN patients with an initial GCS of 4–5 at the end of the first week after injury (Fig. 2D).
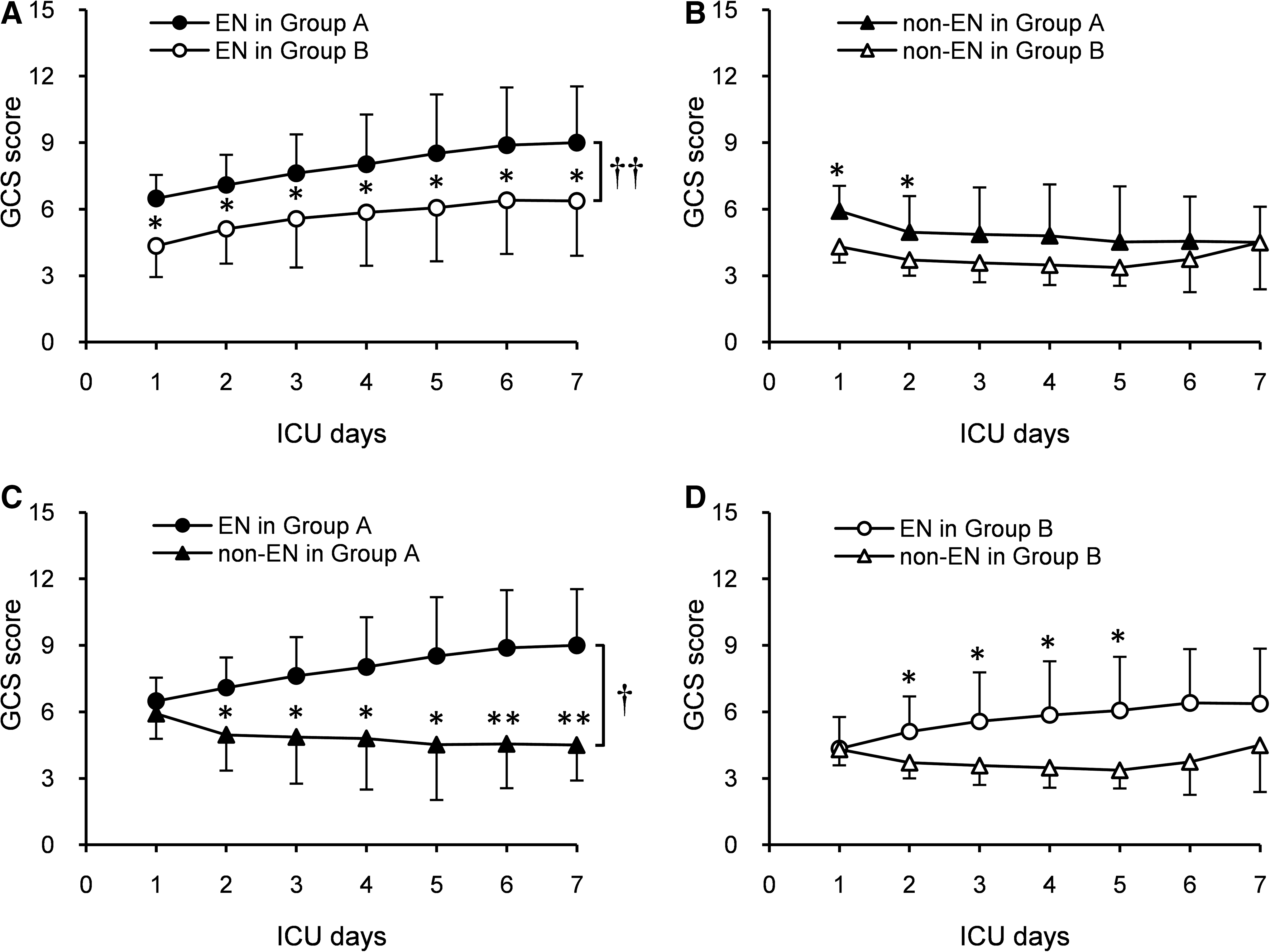
Glasgow Coma Scale scores of non-EN and EN patients with initial GCS scores of 6–8 (Group A) and 4–5 (Group B) over 7 ICU days. † p<0.05, †† p<0.001 (non-EN vs. EN over 7 days). *p<0.05, **p<0.01 (non-EN vs. EN within a day).
Discussion
The percentage of EN patients markedly increased during 2007–2010, indicating gradual acceptance of the guidelines for nutritional support of sTBI management published by the United States and Taiwan from 2007 onwards (Bratton et al., 2007; Chen and Hsu, 2007; Rapp et al., 1983; Young et al., 1987b). Also, the survival curve over 7 ICU days improved during 2007–2010. Therefore, we consider that this modification in survival rate may be associated with the increase in patients receiving EN support as a result of the 2007 early nutritional recommendations for sTBI patients.
Demographic data showed no differences between non-EN and EN groups in this study. Recent studies have indicated that the timing of EN support might be a predictor of clinical malnutrition, such as pedal edema, closely related to survival rate and clinical outcome (Dhandapani et al., 2007; Grahm et al., 1989; Hartl et al., 2008). As is shown in our results, EN provided within 48 h post-injury could markedly increase survival and GCS score of sTBI patients over 7 ICU days, as well as improving clinical outcome at 1 month post-injury. These benefits of early EN on the neurological recovery of sTBI patients may be only because of the supply of calories and nitrogen, but also because of the ability of early EN to maintain gastrointestinal tract capability and integrity and control blood glucose, and to reduce septic complications and infection (Braunschweig et al., 2001; Hadley, 1996; Kudsk et al., 1992; Moore et al., 1992; Suchner et al., 1996). In the present study, the incidence of septic complications was slightly lower in the EN group than in the non-EN group (4.8% vs. 5.9%), excluding the incidence of aspiration pneumonia, which is a major symptom of EN intolerance. It has been suggested that another benefit of early EN is to stimulate mesenteric blood flow, thereby inhibiting bacterial translocation and systemic inflammation, rather than meeting energy and nutrient requirements (Cook et al., 2008; Kattelmann et al., 2006; Roberts et al., 1999).
The significantly improved survival rate for sTBI patients with initial GCS scores from 6 to 8 (Group A) compared with those with initial GCS scores from 4 to 5 (Group B) was observed over 7 ICU days. This result may be explained by recent studies suggesting that initial GCS score is strongly correlated with fatality and could be a good prognostic factor for brain-trauma outcomes (Marmarou et al., 2007; Martins et al., 2009; Scavarda et al., 2010). Although GCS scores over 7 ICU days seemed to rise for sTBI patients with both levels of severity, the GCS variation was different when combining initial severity and nutritional support. In our study, GCS scores of non-EN patients in Group A were gradually decreased and became similar to those in Group B on the 7th ICU day. However, GCS scores for patients receiving EN in Group A were increased significantly compared with both the EN patients in Group B and the non-EN patients in Group A. Nevertheless, the initial condition of patients in Group B may be too serious to enable them to recover even though EN was supplied for them early. Therefore, we suggest that, in this study, improved GCS scores for patients with initial GCS scores of 6–8 may be attributed to early EN.
There are several strengths and limitations that need to be considered when interpreting the results of this study. One strength was the collaboration between the hospitals in Taiwan that manage the large, unselected, brain-trauma samples and the regular meetings for standardization of the recorded data. A limitation of this study was that the reasons for non-EN treatment for the 152 patients in the control group over 7 ICU days were not always recorded in the medical records. However, the injury severity and operative status were collected and showed similar initial conditions between EN and non-EN groups. Another limitation was the limited number of patients supplied with EN from the 3rd to the 7th ICU days. Hence, our data were not heterogeneous enough to examine the correlation between EN treatment times after trauma and outcome of sTBI patients.
Conclusion
In conclusion, we propose that providing EN for sTBI patients within 48 h after trauma definitely has benefits for survival and GCS score recovery compared with non-EN treatment, especially in those with an initial GCS scores between 6 and 8. The effect and mechanism of early EN at different times on the neurological recovery of sTBI patients requires further investigation by a prospective randomized trial.
Footnotes
Acknowledgments
We thank the sTBI patients from 18 hospitals in Taiwan for their dedication to this study. We also thank the research staff in Taipei Medical University and relevant hospitals for their assistance in assembling and sorting the medical records.
This study was supported by the National Health Research Institutes grant NHRI-EX100-9707PI, the Department of Health, Executive Yuan grant DOH100-TD-B-111-003, and the National Science Council, Executive Yuan grant NSC98-2321-B-038-003-MY3 from the Taiwanese government.
Author Disclosure Statement
No conflicting financial interests exist.