
Abstract
There are currently no international guidelines regarding treatment in the early rehabilitation phase for persons with severe traumatic brain injury (TBI), and only a few studies have investigated the effect of integrating rehabilitation into acute TBI care. The aim of the study was to evaluate whether a continuous chain of rehabilitation that begins with the acute phase could improve the functional outcome of severe TBI patients, compared to a broken chain of rehabilitation that starts in the sub-acute phase of TBI. A total of 61 surviving patients with severe TBI were included in a quasi-experimental study conducted at the Level I trauma center in Eastern Norway. In the study, 31 patients were in the early rehabilitation group (Group A) and 30 patients were in the delayed rehabilitation group (Group B). The functional outcomes were assessed 12 months post-injury with the Glasgow Outcome Scale Extended (GOSE) and the Disability Rating Scale (DRS). A favorable outcome (GOSE 6–8) occurred in 71 % of the patients from Group A versus 37 % in Group B (p=0.007). The DRS score was significantly better in Group A (p=0.03). The ordinal logistic regression analysis was used to quantify the relationship between the type of rehabilitation chain and the GOSE. A better GOSE outcome was found in patients from Group A (unadjusted OR 3.25 and adjusted OR 2.78, respectively). These results support the hypothesis that better functional outcome occurs in patients who receive early onset and a continuous chain of rehabilitation.
Introduction
D
Previously, the majority of patients in Norway with severe TBI received specialized inpatient TBI rehabilitation in the later phases, because of the belief that patients have to reach a specific level of responsiveness to benefit from the treatment, or because the demand exceeded the number of beds that were available. Therefore, patients have spent much time waiting to be admitted to specialized rehabilitation units (Shiel et al., 2001). Recommendations have been made by the Norwegian Health Authorities to reinforce the primary management and rehabilitation offered to these patients (
However, there are currently no accepted international guidelines for early rehabilitation treatment for severe TBI, and only a few studies have investigated the effect of integrating rehabilitation into the acute care of TBI in a Level I trauma center (Choi et al., 2008; Greenwood et al., 2004; Mackay et al., 1992). In a retrospective study of acute rehabilitation after TBI, Greenwood and associates (2004) compared the use of targeted resources in 92 patients who received multidisciplinary acute rehabilitation with patients who were transferred to their referring hospitals. According to the procedures, they were usually sent to the orthopedic or general surgical units. The conclusion of the study is that length of stay in the acute treatment program was not prolonged compared to that of patients who received the treatment-as-usual. In a recently published prospective study by Choi and associates (2008), 135 consecutive survivors of severe TBI were studied in a multimodal early rehabilitation unit at a Level I trauma center. Almost two thirds of the patients improved and had a good clinical outcome, and one third reached independence in the activities of daily living. The study concludes that early rehabilitation of patients with severe TBI had a beneficial effect. According to Choi and associates (2008), further investigation of the long-term outcomes after severe TBI and comparative studies of the concept of early rehabilitation in an ICU were needed.
The aim of this study was to evaluate whether the early onset of a continuous chain of rehabilitation starting in the acute phase could improve the functional outcomes of patients with severe TBI, as compared to a broken chain of rehabilitation starting in the sub-acute phase of TBI. Based on previous research, it was expected that patients who received early rehabilitation would show evidence of better functional outcomes 12 months post-injury.
Methods
This prospective cohort study was part of a larger TBI research project that included patients with acute TBI admitted to Level I trauma center for the southeast region of Norway (OUH) over a period of 2 years (2005–2007). The inclusion criteria were patients who 1) were aged 16–55 years, 2) resided in the southeast region of Norway, 3) were admitted with ICD-10 diagnoses S06.0–S06.9 within 24 h of injury, 4) had Glasgow Coma Scale (GCS) (Teasdale and Jennett, 1974) between 3 to 8 before intubation, 5) were in need of neurointensive care (i.e., neuromonitoring to optimize conditions for neuronal survival) for at least 5 days, and 6) survived the first year after the injury. We excluded patients with serious comorbidities that could interfere with the assessment of TBI-related disabilities, such as 1) previous neurological disorders, 2) associated spinal cord injuries, 3) intentional trauma, and 4) previously diagnosed psychiatric and substance abuse disorders.
The ethical justification for randomizing patients seemed untenable for researching the acute care of patients with severe TBI (Kompanje, 2007). Therefore, we used a quasi-experimental study design, including all patients fulfilling the inclusion criteria. In general, the capacity (available bed principle) determined the assignment to whether the patients were admitted to ERSICU (group A) or not (group B). The admission of patients with severe TBI is unpredictable. Hence there may have been periods when several patients competed for the beds available. Although no formal selection criteria were given, we could not rule out selection biases related to advanced age and comorbidity. Hence, we applied narrow inclusion criteria in order to reduce the selection bias in the study design (described previously).
Patients in Group A received early comprehensive rehabilitation in the ERSICU during acute TBI hospitalization. The ERSICU was based on collaboration between the departments of intensive medicine, neurosurgery, and rehabilitation. When the patients' medical conditions were sufficiently stable, they were transferred directly to Sunnaas Rehabilitation Hospital (eastern region) or to Rehabilitation Clinic in Kristiansand (southern region) for further sub-acute brain injury rehabilitation (continuous chain of treatment). The primary aim of early rehabilitation after severe TBI was to offer treatment that focused on reducing the extent of the brain injury, preventing complications, and promoting functional recovery through multisensory stimulation performed by an interdisciplinary rehabilitation team integrated in acute care. The early rehabilitation program was based on three different concepts that were originally proposed by Affolter (organization of sensory input) (Affolter, 1981), Bobath (stimulation of normal movement, function and control) (Bobath, 1959) and Coombes (retraining functions of the face and mouth) (Coombes, 2001) which were also called the ABC components. As reported by Kleffelgard and associates (2008), Affolter guiding was the most time-consuming component used for a mean of 45 min per day. A mean of 30 min was used for the other two components.
Patients in Group B did not receive early comprehensive rehabilitation, but received either inpatient brain injury rehabilitation in sub-acute rehabilitation departments after a waiting period at a local hospital or nursing home, or received no inpatient rehabilitation at all (broken chain of treatment). The primary aim of specialized inpatient rehabilitation in the sub-acute phase of TBI was to reduce impairment, increase functional independence, restore social participation, and minimize the distress of the patient as well as of the caregivers. There was a particular focus on the personal and domestic activities of daily life. As described in another study, all of the patients received a minimum of 2–3 h of daily individual treatment included physiotherapy, occupational therapy, speech therapy, cognitive training, nutrition, dietary services, and psycho-social support (Sandhaug et al., 2010).
A flow chart of the inclusion is presented in Figure 1. In all, 132 patients were assessed for eligibility. Eleven percent refused participation in the study, 15% were excluded because of comorbid conditions, 17% died, and 8% were excluded because they did not need a minimum of 5 days of neurointensive care. The remaining 49 % of the patients were included in the study. Three patients dropped out of the study before the 12-month follow-up. Therefore, 61 patients were assessed in the study (31 patients were in Group A and 30 were in Group B).
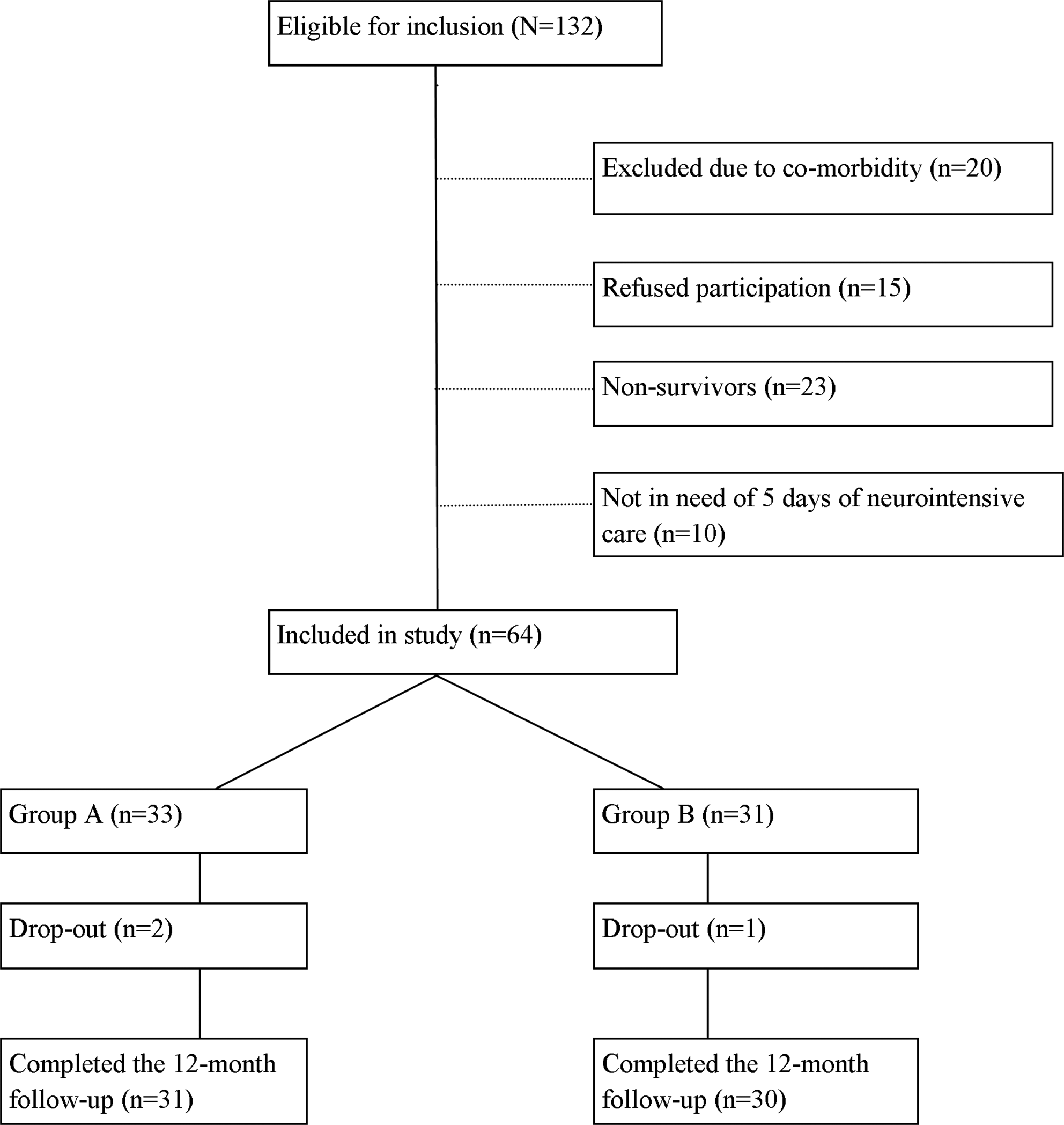
Flow chart for patients (age 16–55 years) included in the study.
The study was approved by the Regional Committee for Medical Research Ethics, East Norway and the Norwegian Data Inspectorate.
Procedure
Demographic variables (age, gender, education, marital status, employment) and clinical features (GCS, pupils, oxygen saturation, and mean arterial pressure before intubation), Injury Severity Score (ISS) (Baker et al., 1974), head CT scan, and the rates of intracranial pressure (ICP) monitoring and intracranial surgeries were collected during acute TBI admission. The severity of the injury was based on structural brain damage found on a CT scan according to the Marshall classification (Marshall et al., 1992) and ISS. At 12-month follow-up, patients were interviewed and examined by the first author in the outpatient clinic or in the rehabilitation hospital, where they had been admitted for a clinical follow-up assessment.
Structural brain damage
The patients were examined by head CT scan shortly after acute admission. A second head CT scan was performed within 6 to 24 h after injury. Findings from the first and second head CT scans were categorized according to the procedures in Marshall and associates (Marshall et al., 1992). Scores from the worst head CT scan were used in this study. A single neuroradiologist reviewed the CT findings. The original Marshall classifications range from 1 to 6, with separate categories for any lesion that was surgically evacuated and any non-evacuated mass lesions. For the purposes of the study, the head CT findings were divided into two groups: less severe brain injury (no intracranial injuries and small lesions, Marshall score 1–2) and more severe brain injury (significant intracranial abnormalities, Marshall score 3–6).
ISS
The ISS is an anatomical scoring system that provides an overall score for patients with multiple injuries (Baker et al., 1974). Each injury was assigned an Abbreviated Injury Scale (AIS) score that classified individual injuries according to body regions with a 6-point ordinal severity scale (Association for the Advancement of Automotive Medicine, 1998). The ISS scores ranged from 1 to 75 (best to worst) and were calculated from the sum of the squares of the highest AIS scores in the three most injured body regions. An ISS of ≥15 was universally accepted as the definition for a major trauma. AIS and ISS scores were determined from the hospital's trauma register (Skaga et al., 2006).
Outcome measures
The primary outcome measure was the Glasgow Outcome Scale Extended (GOSE) (Wilson et al., 1998), which was assessed 12 months post-injury. The GOSE divided patients into the following outcome categories: 1=dead, 2=vegetative state, 3=lower severe disability and complete dependence on others, 4=upper severe disability and some dependence on others, 5=lower moderate disability and working at a lower level of performance, 6=upper moderate disability and returning to previous work with some adjustments, 7=lower good recovery with minor physical or mental deficits, and 8=upper good recovery. The GOSE outcomes were split into: unfavorable (2–5) and favorable (6–8). The GOSE was administrated in a structured face-to-face interview conducted by the first author.
The secondary outcome measures included the Disability Rating Scale (DRS) (Rappaport, 2005), the patient's employment status and the living situation 12 months post-injury. The DRS scale measured the levels of arousal, awareness, and responsiveness (including eye opening, communication ability, and motor response); cognitive ability for self-care activities (such as feeding, using the toilet, and grooming); dependency on others (level of functionality); and psychosocial adaptability (employability). The scores on the DRS items included values from 0 to 29 (low to high level disability) and were categorized by the following disability categories: 0=none, 1=mild, 2–3=partial, 4–6=moderate, 7–11=moderately severe, 12–16=severe, 17–21=extremely severe, 22–24=vegetative state, and 25–29=extreme vegetative state. Both categorized and dichotomized DRS (dichotomized at the median value) were used. The first author scored the DRS.
Employment status at 12 months post-injury was dichotomized into: full- or part-time work versus not working. Students were regarded as full or part-time employees. Living situations were categorized as: living at home without assistance, living at home with assistance or living in a nursing home.
Statistical analyses
Descriptive data were presented using the proportions and mean values with standard deviations (SD), or the median with the interquartile range (IQR) (for the 25th and 75th percentile values). The Mann–Whitney U test was used to compare differences between Group A and Group B regarding gender, length of hospital stays, and post-traumatic amnesia (PTA). T tests were used for analyzing differences in age, GCS, AIS, ISS and DRS. The χ2 test with contingency tables was applied to study associations between categorical independent variables.
Ordinal logistic regression analyses (proportional odds) were used to evaluate the relationship between early rehabilitation and functional outcome 12 months post-injury. The two groups of patients that were studied were entered as an explanatory variable and analyzed separately (unadjusted OR) against the dependent variable GOSE. For the purpose of this analysis, GOSE was reclassified into a variable of three categories: severe disability (GOSE score 2–4), moderate disability (GOSE score 5–6), and good recovery (GOSE score 7–8). Possible confounding variables were studied with multivariate regression analysis (adjusted OR). These variables were age, severity of structural brain injury, and length of rehabilitation stay. Head CT scans were classified as less severe versus more severe brain injury by using the Marshall classification. The model was controlled by the proportional odds assumption test. The Pearson and deviance goodness-of-fit statistics were computed. Before conducting the logistic regression analysis, possible multicollinearity was examined. All statistical tests were two-sided, and the 5% significance level was used. Statistical analyses were performed using SPSS for Windows, version 15 (SPSS Inc, Chicago, IL).
Results
Demographics, injury characteristics, and clinical features
The demographic and injury characteristics of Groups A and B are listed in Table 1. There were no statistically significant differences between the groups regarding demographics, cause of injury, clinical characteristics observed at the site of the injury (before intubation), and structural brain injury assessed by CT scans. However, patients in Group A were more frequently treated with intracranial surgery because of mass lesions in the brain (p=0.09). The length of stay in the ICU at OUH was similar in both groups (the Group A median was 12 days versus 13.5 days in Group B) as shown in Table 1. Early rehabilitation in Group A began at a median of 12 days after the injury (IQR 8). The median length of stay in the ERSICU was 14 days (IQR 8.5) for Group A. The median length of stay in a local hospital was 39 days (IQR 35) for Group B. In Group B, the waiting time for inpatient brain injury rehabilitation ranged from 6 to 57 days. In Group A, the total length of stay in acute hospitals had a median that was 17 days shorter than the stays for Group B. The total length of inpatient rehabilitation stay had a median that was 29 days shorter in Group A, but this difference did not reach statistical significance.
Substance use: n=60; Group A n=30, Group B n=30.
PTA n=51; Group A n=27, Group B n=24.
IQR, interquartile range; ICU, Intensive Care Unit.
Functional level 12 months post-injury
The mean GOSE in the study was 5.4 (SD 1.3) and the median was 6 (range 2–8). Of all the patients, 16.4% achieved good recovery levels (GOSE 7–8), 64% had moderate disability (GOSE 5–6), 18% had severe disability (GOSE 3–4) and 1.6% was in a vegetative state (GOSE 2). Of all the patients, 54% had a favorable functional outcome (GOSE 6–8) 12 months post-injury. One patient in Group A was in a vegetative state and two were at the lower level of severe disability. In contrast, none of the patients in Group B remained in a vegetative state, but five patients were at the lower severe disability level. Better global functioning, assessed by GOSE, was found in Group A (χ2 13.9, df 6, p=0.03), (Fig. 2). A favorable outcome (GOSE 6–8) was found in 71% of the patients in the early rehabilitation group (Group A) and 37% in group B (χ2 7.22, df 1, p=0.007).

Global functional outcome of patients with early rehabilitation (Group A) and patients with delayed rehabilitation (Group B) at 12 months post-injury as measured by Glasgow Outcome Scale Extended (GOSE).
The mean DRS score in the study was 4.7 (SD 5.6) and the median was 3 (IQR 4.5). Of all the patients, 11.5% had no disability and 20% had severe disability at the 12-month follow-up. The functional level, as measured by DRS, was significantly better in Group A (p=0.03), (Fig. 3). The median DRS in Group A was within the range of partial disability (2.0), whereas the median in Group B was within the range of moderate disability (4.0) (p=0.03).
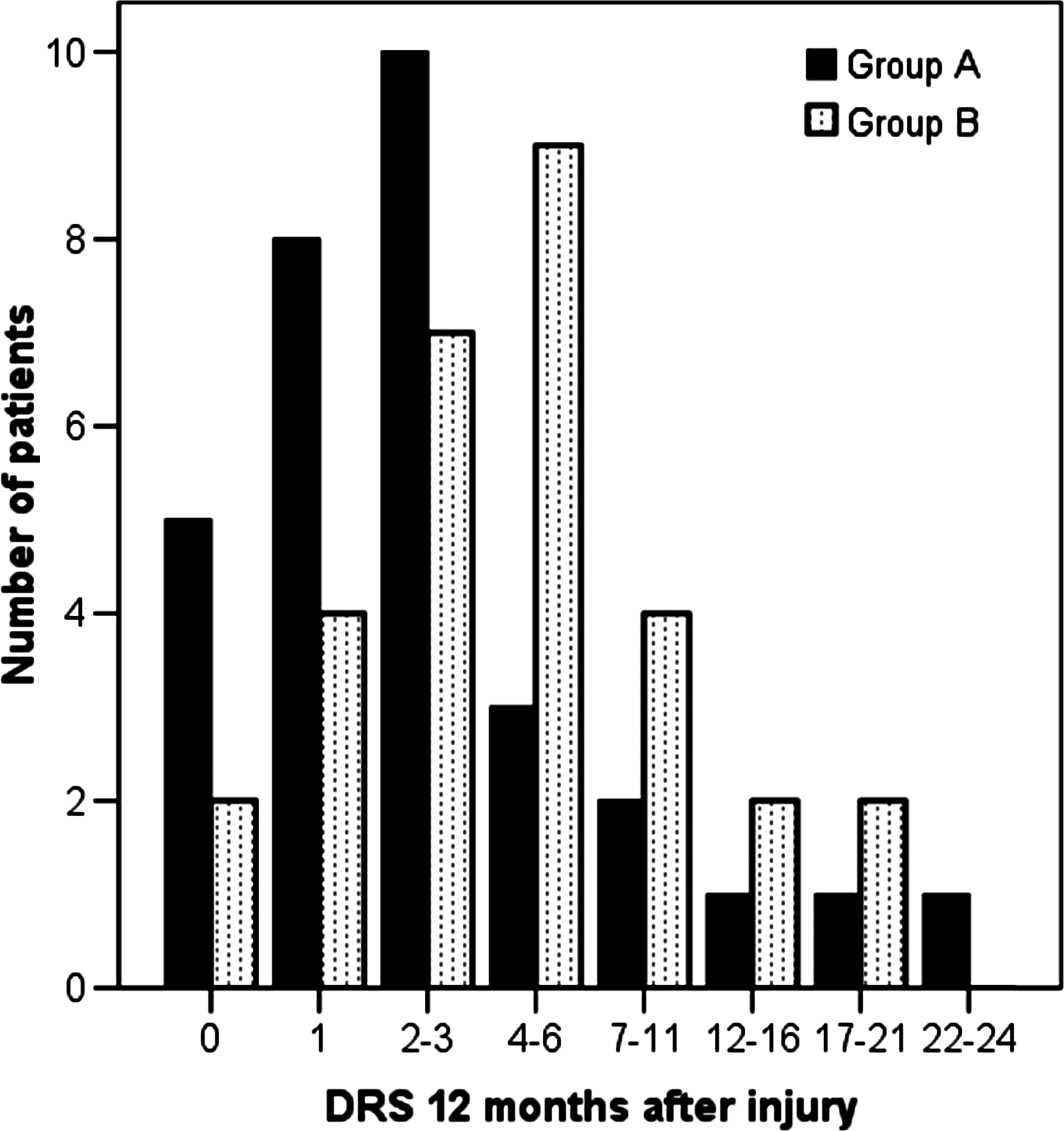
Functional level of patients with early rehabilitation (Group A) and patients with delayed rehabilitation (Group B) at 12 months post-injury as measured by Disability Rating Scale (DRS).
Of all the patients, 67% were living at home with no assistance from the community, and 15% were living at home with assistance. Eighteen percent of the patients were residing in nursing homes 12 months post-injury with severe disability, according to GOSE (score 2–4). In Group A, 81% of patients were living at home and 13% were living in nursing homes. In Group B, 53% were living at home, and 23% were living in nursing homes (χ2 5.56, df 2, p=0.06).
Thirty-four percent of the patients had returned to work 12 months post-injury (14% full time and 20% part time). Of those who achieved a GOSE level that indicated good recovery, 80% returned to work. The frequency of returning to work was 39% in Group A (16% in full-time work), and 27% in Group B (6% in full-time work).
Association between early rehabilitation onset and functional outcome 12 months post-injury
The ordinal logistic regression analyses included all the patients (Table 2). In the unadjusted regression model, Group A had a significantly increased probability of a better global functional outcome (unadjusted OR 3.25; 95% CI [1.08-9.87], p=0.03). The trend of the increased probability of a better outcome in Group A was also upheld when the model was adjusted for age (OR 2.85) and in the final regression model adjusted for age, severity of the structural brain injury, and length of the stay in rehabilitation hospitals (OR 2.78). Test of the parallel lines indicated that we had not violated the proportional odds assumption of the final model (p=0.24). The p-value for the Pearson goodness-of-fit test (p=0.76) indicated that the model fit well.
Group A: early rehabilitation group; Group B: delay rehabilitation group; Severe disability: GOSE score 2-4; Moderate disability: GOSE score 5-6; Good recovery: GOSE 7-8; OR: (odds ratio). OR>1 increases the probability of favorable functional outcome. OR<1 decreases the probability of favorable outcome.
Better outcomes in Group A were also found with an ordinal logistic regression analysis that used DRS as a dependent variable as well as the same covariates used in the GOSE model (results not shown).
Discussion
This study evaluated two different types of rehabilitation approaches in the early phase of severe TBI with a quasi-experimental study design. The results indicated that there was a better functional outcome for patients who received the combination of early rehabilitation and a continuous chain of treatment. Patients who received early care in other institutional settings and delayed admission to inpatient brain injury rehabilitation centers had poorer outcomes.
Demographics, injury characteristics, and clinical features
The demographic variables of all the included patients were comparable to other studies of severe TBI (Lippert-Gruner et al., 2007a). No statistically significant differences were found in the demographic variables between Groups A and B. The groups were also comparable for injury severity variables such as GCS, pupil condition, hypoxemia, hypotension, AIS head, ISS, intracranial pathologies on the worst CT scan findings within 24 h, and the rate of ICP monitoring/intracranial surgery.
Patients who received early rehabilitation in this study (Group A) had a shorter stay in both the acute (17 days) and rehabilitation hospitals (29 days) as well as a shorter total hospital stay (35 days). However, these results were not statistically significant, most likely because of the small sample size.
The median length of stay in the ICU/ERSICU was shorter than the lengths of stay reported in previous studies (Greenwood et al., 2004), which probably occurred because of the efficiency of both the neurointensive care and the integrated chain of treatment. Delays in in-hospital rehabilitation in Group B ranged from 6 to 57 days, which was considerably lower than the waits before 2005 when patients had delays of 3–6 months before receiving inpatient rehabilitation. This reduction in the waiting period was probably the result of the reinforced rehabilitation efforts in specialized rehabilitation hospitals according to recommendations by the Norwegian Health Authorities.
Functional level 12 months post-injury
Global functioning, as measured by the mean value of GOSE 12 months post-injury, was within the moderate disability range. The proportion of patients with favorable outcomes (75%) was slightly lower in our study than in a German study of patients who received multidisciplinary early rehabilitation treatment (84%) (Lippert-Gruner et al., 2007a). However, 87% of the patients in Group A showed good recovery/moderate disability 12 months post-injury, which was similar to the findings in the German study (Lippert-Gruner et al., 2007a).
The functional level 12 months post-injury, as measured by DRS, was within the range of moderate disability for all of the patients. At the group level, there was a significant advantage in the early rehabilitation group. The proportion of partial disability (DRS scores 2–3) shown in Group A (33 %) was similar to a previous Italian study on early rehabilitative treatment in patients with severe TBI (Mammi et al., 2006).
The living situations and employment status of the patients 12 months post-injury reflected their functional levels. Better outcomes occurred in Group A for both the return to work rates and living situation. However, the rates of work re-entry were considerably lower when they were compared to the employment rate at the time of injury. The results were roughly comparable to other studies of severe TBIs at the 12-month follow-up point (Lippert-Gruner, et al., 2007a; Mammi et al., 2006). In a Danish study (Blicher et al., 2007), 4 % of patients returned to their regular occupation 12 months post-injury, in contrast to 16 % of patients in Group A who returned to work.
Early rehabilitation and functional outcome
We hypothesized that the patients who had received early rehabilitation would show evidence of better functional outcomes 12 months post-injury. As expected, better functional outcomes were found at a 12-month follow-up in the group that received early rehabilitation. There was also increased probability of a better outcome in Group A, when the model was controlled for variables that could affect the results (age, severity of injury, and total length of rehabilitation). The age variable negatively influenced functional outcome, in agreement with other studies (Maas et al., 2008). Neither brain injury severity nor the length of rehabilitation stays confounded the results in the adjusted logistic regression model, and additional tests revealed that the model was a good fit. We used head CT scans to determine the brain injury severity variable through the assessment of structural brain damage. To note, CT scans are not influenced by state of consciousness, unlike GCS, which might be obscured in acute settings because of substance use at the time of injury, medical sedation, or paralysis (Maas et al., 2008).
Our results support other studies that suggest that early rehabilitation is broadly beneficial for severely brain injured patients (Choi et al., 2008). However, the studies included in the Cochrane review by Turner-Stokes and associates (2005) failed to address the impact of early rehabilitation. This could be partially explained by ethical problems of randomizing patients from vulnerable populations such as patients with severe TBI. There is a general lack of evidence for establishing the causal effect of early rehabilitation on promoting the recovery of a damaged brain (Zhu et al., 2007). Biochemical and anatomical plasticity of the brain and natural recovery provide the foundation for rehabilitation interventions to enhance the functional recovery in patients with brain injuries (Elliott and Walker, 2005). Experimental studies of animals (Oliff et al., 1998) and studies of patients with stroke (Liepert et al., 2000) demonstrated that brain plasticity is activity driven, and that the potential to enhance brain plasticity and improve functional recovery is greater in the early stages of recovery after injury (Zhu et al., 2007). Motor activity can positively influence the expression of brain-derived neurotrophic factor (BDNF), which has a neuroprotective influence on the damage of the neurons as well as on neuronal survival (Oliff et al. 1998). An experimental early rehabilitation model showed that types of housing that provided animals with an enriched environment led to a clear functional increase in neuromotor function and reduced neural loss compared to animals in standard housing (Lippert-Gruner et al., 2007b). Another study evaluated the effects of acute and delayed exercises following experimental TBI in rats (Griesbach et al., 2004). The results suggested that voluntary exercise can endogenously upregulate BDNF and enhance recovery after TBI (14–20 days after). However, when exercises were administrated too soon after TBI (0–6 days after) the molecular response to exercise was disrupted and the recovery was delayed.
In our study, early rehabilitation integrated with ICU treatment and administered from a median of 12 days post-injury might have influenced brain plasticity and sped up the recovery process. Furthermore, this study indicated that early rehabilitation led to shorter hospital stays and better functional outcomes 12 months after the injury (Zhu et al., 2007). Hoffman and Von Wild demonstrated that early rehabilitation in combination with intensive care treatment contributes to preserving the rehabilitation potential of the brain (Hoffmann and von Wild, 2002).
Different programs for early rehabilitation after TBI have been previously studied including multimodal early onset stimulation (Gruner and Terhaag, 2000) and multimodal early rehabilitation (Choi et al., 2008). However, there is still uncertainty regarding which component(s) of these programs that are the most important (Borg et al., 2011). The results of this study support a clinical management model integrating both acute and sub-acute care of subjects with severe TBI, and providing neurointensive care and comprehensive early rehabilitation ensuring continued treatment in the later stages of the rehabilitation process. This program design reflects the current trends in the organization of rehabilitation services after moderate and severe TBI in Scandinavia (Borg et al., 2011).
Several limitations should be considered when interpreting the results of this study. First, this was an age-selected cohort study of a severe TBI population (16–55 years). Second, a quasi-experimental study design cannot eliminate the possibility of confounding bias caused by unmeasured confounders. However, the groups are equal with respect to the most important well-known predictors for outcome in TBI, thus lending support to the validity of our findings. Third, we excluded patients with comorbidities that interfered with the assessment of TBI-related disabilities (such as previously diagnosed neurological, psychiatric, and substance abuse disorders) to reduce the possible bias of the clinician selection approach; hence, results may not be generalized to these patients. Fourth, the small sample size in this study limited the number of covariates that could be controlled for in a multiple regression analyses, but also the distinction among the different degrees of severity within severe TBI. Nevertheless, our study is one of the few prospective studies in this field that has investigated early rehabilitation in the acute care of TBI patients at a Level I trauma center, and provided a comparison of two different treatment approaches.
Conclusion
The results of this study support the hypothesis that severe TBI patients who received early comprehensive rehabilitation in a continuous chain of treatment had better functional outcomes 12 months post-injury. Further studies on the long-term outcomes and cost effectiveness of early rehabilitation after severe TBI are required. In addition, studies of the effectiveness of specific rehabilitation efforts are needed.
Footnotes
Acknowledgments
The authors thank all the patients for their participation. Special thanks are given to Tone Jerstad (neuroradiologist, Oslo University Hospital, Ulleval) for the CT assessments and Morten Hestnes (Trauma Register, Oslo University Hospital, Ulleval) for the extraction of trauma scores. This study was supported by grants from the Norwegian Health South-East Authority.
Author Disclosure Statement
No competing financial interests exist.