
Abstract
In the intensive care unit, dopamine agonists (DA) have been used in traumatic brain injury (TBI) patients to augment or accelerate cognitive recovery and rehabilitation. However, the efficacy and safety of DA in this population is not well established. We conducted a systematic review of randomized controlled trials (RCTs) examining the clinical efficacy and safety of DA in patients with TBI. We searched MEDLINE, EMBASE, and the Cochrane Central Register of Controlled Trials, comparing DA to either placebo, standard treatment, or another active comparator. There was no restriction for age, date, or language of publication. Sensitivity analyses were planned to evaluate the potential effect of timing of TBI, age, drugs, and year of publication on efficacy. Among the 790 citations identified, 20 RCTs evaluating methylphenidate, amantadine, and bromocriptine were eligible. Significant clinical heterogeneity was observed between and within studies, which precluded any pooling of data. Efficacy outcomes included mainly neuropsychological measures of cognitive functioning. A total of 76 different neuropsychological tests were used, but most of them (59%) only once. Only 5 studies systematically assessed safety. No trend could be drawn from the analysis of efficacy and safety. Important sources of bias in the studies were of major concern. Considering the absence of consensus regarding clinical outcome, the lack of safety assessment, and the high risk of bias in the included trials, more research is warranted before DA can be recommended in critically ill TBI patients.
Introduction
T
Neurotransmitters such as dopamine influence cognitive processes, movement control, and emotion (Bales et al., 2009; Thurman and Guerrero, 1999). Central dopaminergic pathway dysfunction may contribute to some of the neuropsychiatric sequelae in patients recovering from TBI (Bales et al., 2009). In the intensive care unit, step-down units, or on the ward, dopamine agonists (DA) are anecdotally used in patients recovering from TBI in an attempt to augment vigilance or accelerate cognitive recovery and rehabilitation. However, the efficacy and safety of DA in this population is not clear (Francisco et al., 2007; Siddall, 2005; Tenovuo, 2006). The aim of the present systematic review was to determine the clinical efficacy and safety of DA in TBI patients compared to placebo, active control, or standard treatment (Moher et al., 2009).
Methods
Search strategy
Randomized controlled trials (RCTs), were identified using both electronic and manual search strategies. In June 2010, we searched MEDLINE, EMBASE, and the Cochrane Central Register of Controlled Studies from the earliest accessible date. We combined terms defining the study treatment (DA) and the study population (TBI). A specific filter was applied to MEDLINE and EMBASE search strategies to identify RCTs (Lefebvre et al., 2009; Scottish Intercollegiate Guidelines Network, 2009). The bibliographies of all identified RCTs and the reviews retrieved were manually searched for additional studies. The search strategy was reviewed by a qualified librarian. The full search strategy for MEDLINE is presented in Appendix 1.
Eligibility criteria
We sought studies of TBI patients, without age restrictions, comparing the effect of the administration of a DA, including methylphenidate, bromocriptine, amantadine, levodopa, ropinirole, pramipexole, apo-morphine, cabergoline, and pergolide, to either placebo, standard treatment, or another active comparator. We included studies addressing clinical efficacy using any primary outcome measures and/or safety. There was no restriction for date or language of publication. We excluded unpublished studies, animal studies, and studies assessing dopamine agonists in any other type of brain injury. Studies of mixed populations with TBI representing more than 80% of patients, or for which data of TBI patients could be isolated, were included.
Study selection
Every study citation retrieved was evaluated by two independent reviewers (A.J.F. and S.K.), according to the previously described inclusion/exclusion criteria. Disagreements were resolved by consensus.
Data extraction and validity assessment
Each study was evaluated independently and in duplicate by two reviewers (A.J.F. and S.K., M.M.P., D.R.W., F.B., or Marie-Soleil Delisle). Any disagreement was resolved by a third independent reviewer. Information was collected using a standardized case report form that was revised after pilot testing on 5 studies by 5 different reviewers. Descriptive variables for each trial were collected, including language of publication, country of randomization, source of funding, sample size, and objectives. Information on the study design included the type of RCT, blinding, method of randomization, number of participating centers, and screening and enrolment of patients. Clinical variables including patient demographic data, past medical history, concomitant drugs permitted, timing of DA administration since the injury, description of the TBI (i.e., mechanism of trauma, severity of TBI, severity of global illness, and radiological findings), and evaluation of the pre-intervention level of functioning, cognitive function, and quality of life, were also collected if reported. Clinical outcomes included length of stay (intensive care unit [ICU] and hospital), mortality, side effects, functional scales, post-traumatic symptoms, and neuropsychological test outcomes.
Methodological quality was assessed using the rating instrument developed by the Cochrane Handbook for Systematic Reviews of Interventions (Higgins and Altman, 2008). In order to assess the carry-over effect in crossover studies, a washout period was considered appropriate when equal to at least 5 half-lives of the study drug from the last dose, when more than one dose was administered in the study. Based on clinical considerations, an a priori washout period of 2 days or more for a single-dose trial was considered suitable. In these crossover studies, we considered not reporting the results of baseline assessment after the washout period, and the inclusion of patients who dropped out after the first study period, as inappropriate (Higgins et al., 2008).
Data synthesis
Data related to study design, drug treatment, and patient demographics, were described for each study. Pre-morbid conditions were described using three categories: functional status, cognitive or psychological impairment, and quality of life, when available. Severity of TBI and illness was assessed using severity scales (Glasgow Coma Scale, Acute Physiology and Chronic Health Evaluation II, and Injury Severity Score), and radiological findings (computed tomography [CT] scan), when available. Clinical outcomes measured by neuropsychiatric questionnaires and scoring tools were categorized as either behavioral or cognitive outcomes. Cognitive outcomes were further categorized into the following domains: attention, speed of processing and reaction time, memory, and executive functioning, according to the predominant domain measured by the test (Patry and Mateer, 2006; Tsaousides, 2009). Sustained attention, focused attention, selective attention, alternating attention, and divided attention, were classified under attention. Clinical outcomes not falling into cognitive or behavioral categories were classified as “other outcomes.”
Sensitivity analyses were performed to evaluate the potential effect of the following sub-groups on efficacy: early versus late TBI, children versus adults (16 years of age or older), type of drugs, and year of publication. Year of publication was dichotomized into the following categories: before 1995, and 1995 and after, based on the increased use of computer-based neuropsychological tests after 1994. Patients were considered to have an early TBI if they were still in an acute care facility (ICU or ward). Patients recruited in rehabilitation centers or in the community were considered to have late TBI.
Safety was assessed by retrieving all adverse events reported. We specifically looked for information on predetermined side effects that were clinically relevant in the evaluation of DA administration safety in TBI, in addition to the reported findings. Information regarding how safety was assessed in the individual studies was also collected. Evaluation of side effects was considered appropriate, if (1) the authors were using a prospectively validated side-effect checklist or a pre-defined objectively measured endpoint; (2) if the method of assessing specific side effects was provided; and (3) if the timing for side-effect evaluation was provided and clinically relevant (Loke et al., 2008).
Results
Study selection
The search strategy identified 790 citations. Twenty studies were included in the systematic review (Fig. 1). Demographics of the study are listed in Table 1. One study published in Chinese only provided descriptive results that were impossible to analyze with regard to the objectives of this study and was therefore rejected. Among those included, 14 evaluated methylphenidate, 4 evaluated amantadine, and 2 evaluated bromocriptine. No study evaluating the use of levodopa, apo-morphine, ropinirole, pramipexole, cabergoline, or pergolide in TBI was identified.
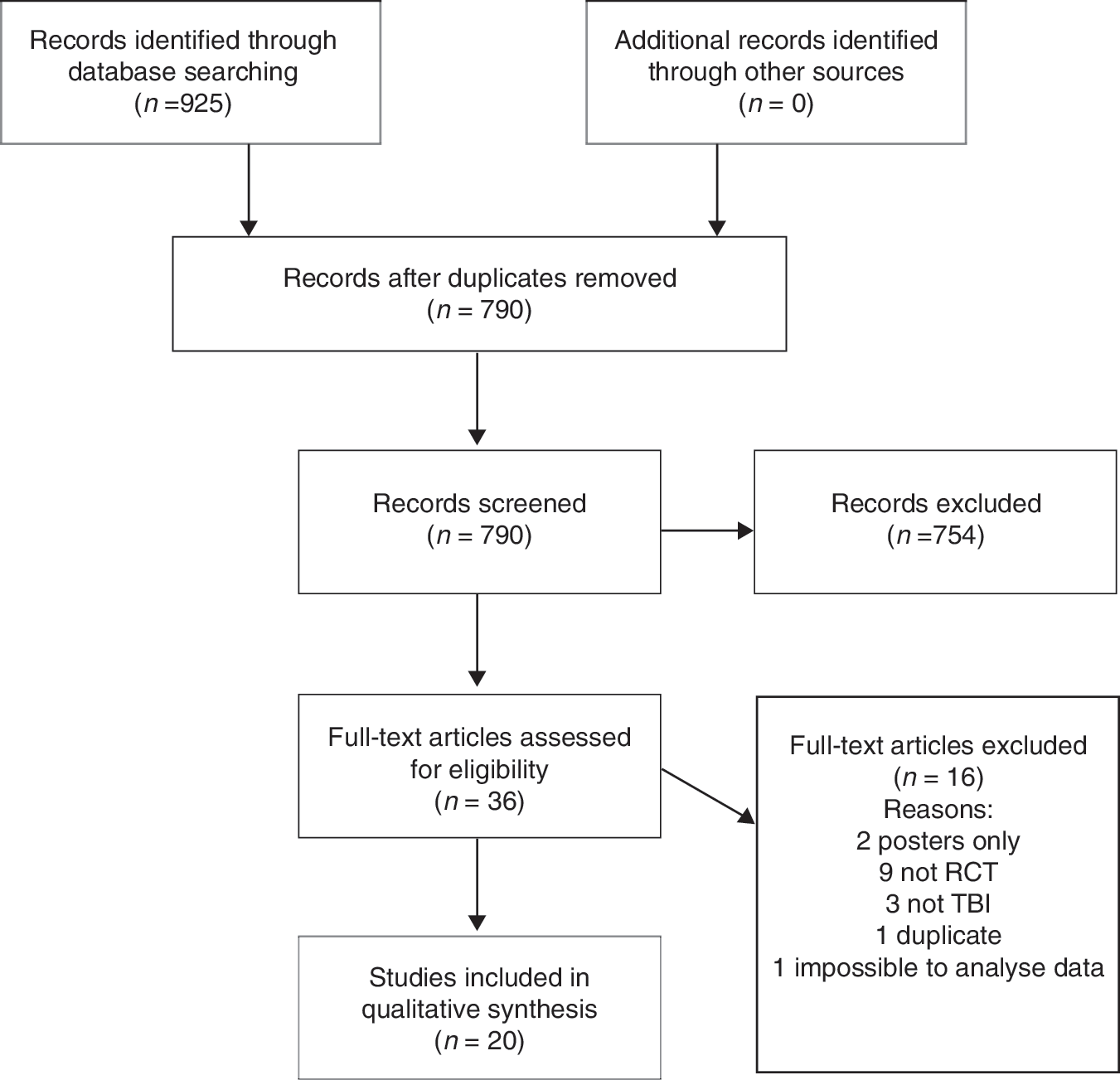
Flow chart of the study (RCT, randomized controlled trial; TBI, traumatic brain injury).
RCT, randomized controlled trial; MPH, methylphenidate; AM, amantadine; B, bromocriptine; PTA, post-traumatic amnesia; GCS,
Glasgow Coma Scale; LOC, loss of consciousness; TBI, traumatic brain injury; N/A, not applicable.
Adults are defined as≥16 years old.
Study characteristics
Twenty studies evaluated the administration of a DA in TBI, including a total of 480 patients (Alban et al., 2004; Beers et al., 2005; Gualtieri and Evans, 1988; Kim et al., 2006; Lee et al., 2005; Mahalick et al., 1998; McDowell et al., 1998; McMahon et al., 2009; Meythaler et al., 2002; Moein et al., 2006; Mooney and Haas, 1993; Plenger et al., 1996; Schneider et al., 1999; Speech et al., 1993; Whyte et al., 1997,2004,2008; Williams et al., 1998; Willmott and Ponsford, 2009; Willmott et al., 2009; Table 1). Dopamine agonists were compared to placebo in all but 2 studies (Beers et al., 2005; Kim et al., 2006). One these studies reported a comparison between amantadine and standard care (Beers et al., 2005). Sertraline was used as a comparator to methylphenidate in the other study (Kim et al., 2006). Of the 20 included studies, 14 (70%) used a crossover design, 5 (25%) used a parallel design, and 1 (5%) used a time series analysis. The majority of studies (80%) were single-center studies. All studies were published in English, and the majority was from the U.S.A. Other countries represented were Iran, Australia, and Korea.
Dosage regimen
Dosage did not vary much among the methylphenidate studies (0.3–0.6 mg/kg per day for adults). However, duration of treatment and follow-up period ranged from 1 day to 1 month. A similar observation can be drawn regarding the doses of amantadine that were used (200–300 mg/kg/d in adults, and 4–6 mg/kg/d in children). Duration of treatment among the studies using amantadine varied from 2 to 12 weeks. A higher variation of dosing was seen among the 2 studies using bromocriptine (2.5–10 mg/d). One study used a single dose (McDowell et al., 1998), and the other study followed patients for 4 weeks (Whyte et al., 2008).
Patient characteristics
Seven of the 20 studies included children (Beers et al., 2005; Gualtieri and Evans, 1988; Mahalick et al., 1998; McDowell et al., 1998; McMahon et al., 2009; Whyte et al., 1997; Williams et al., 1998), 3 of them exclusively (Beers et al., 2005; Mahalick et al., 1998; Williams et al., 1998). No study included patients over 65 years old, although age was not always mentioned as an exclusion criterion. Some information on baseline level of functioning and psychological and cognitive conditions was available in 12 of 20 studies (Alban et al., 2004; Beers et al., 2005; Gualtieri and Evans, 1988; Kim et al., 2006; Lee et al., 2005; McMahon et al., 2009; Meythaler et al., 2002; Mooney and Haas 1993; Whyte et al., 1997,2004,2008; Willmott and Ponsford, 2009).
The level of functioning prior to randomization was assessed using different scales, including the Disability Rating Scale (Alban et al., 2004; Whyte et al., 1997,2004,2008), the Glasgow Outcome Scale (Gualtieri, 1988; Gualtieri and Evans, 1988; Mooney and Haas, 1993), and the Rancho Los Amigos Scale (Gualtieri and Evans, 1988). Patients were described as severely disabled in 2 studies (McMahon et al., 2009; Meythaler et al., 2002), moderately disabled in 3 studies (Alban et al., 2004; Whyte et al., 1997,2004), and mildly to moderately disabled in 2 studies (Gualtieri and Evans, 1988; Mooney and Haas, 1993).
Patients were described as having significant behavioral or cognitive deficits in 3 studies (Beers et al., 2005; Meythaler et al., 2002; McMahon et al., 2009), one of them including only comatose patients (McMahon et al., 2009). Other studies reporting cognitive status included patients with intellectual quotient within normal range (Alban et al., 2004; Gualtieri and Evans, 1988; Speech et al., 1993; Whyte et al., 2004; Williams et al., 1998; Willmott and Ponsford 2009; Willmott et al., 2009), or with mild cognitive impairment (Kim et al., 2006; Lee et al., 2005). No study reported quality of life prior to randomization.
Severity of TBI
Location of patients at randomization can be found in Table 1. Of note, only 3 studies included patients in a critical care setting (intensive care unit, trauma unit, or emergency department). Heterogeneity among and within studies arises for the most part from the time elapsed from trauma to randomization, varying from less than 48 h to 34.2 years post-TBI. Information on global severity of illness at the time of injury (e.g., Abbreviated Injury Scale, Injury Severity Score, or Acute Physiology and Chronic Health Evaluation II) was not available in any of the studies. Only 7/20 (35%) studies reported CT scan findings (Alban et al., 2004; Lee et al., 2005; Mahalick et al., 1998; McDowell et al., 1998; Moein et al., 2006; Schneider et al., 1999; Whyte et al., 2004), and it was not possible to calculate a Marshall or Rotterdam score (Saatman et al., 2008). Severity of TBI was assessed using 3 different tools: loss of consciousness after injury, presence of post-traumatic amnesia, and the Glasgow Coma Scale. Nine studies (45%) included exclusively patients suffering from severe TBI (Alban et al., 2004; Gualtieri and Evans, 1988; Meythaler et al., 2002; Mooney and Haas, 1993; Whyte et al., 1997,2004,2008; Willmott and Ponsford, 2009; Willmott et al., 2009).
Studies describing the mechanism of trauma included only blunt TBI, except for 2 patients with penetrating TBI (McDowell et al., 1998), 1 aneurysm (McDowell et al., 1998), 1 stroke (McMahon et al., 2009), 1 cerebral anoxia (McMahon et al., 2009), and 1 suspected assault with unknown lesions (McDowell et al., 1998). These patients were included in the analysis since it was not possible to exclude them from the data provided.
Efficacy outcomes
Pooled estimates of outcome measures were planned, but were not calculated due to the inconsistent outcome measures used. Efficacy outcomes included mostly neuropsychological tests. Only one study used length of stay as a primary outcome, and showed both reduced hospital and intensive care unit stays with methylphenidate (Moein et al., 2006).
Neuropsychological assessment
A total of 76 different neuropsychological tests were used to assess efficacy outcomes (see Figs. 2 –7). Of these, 45 (59%) tests were only used in one study. Of note, individual results of tests were not provided in 31 out of 128 assessments (24%). The tests were categorized into cognitive- and behavioral-predominant domains, except for 4 tests (Selective Attention Task, Symbol Digit Modalities Test, Sustained Arousal and/or Attention Task 50/50 or 20/80, and Wisconsin Sorting Card Test), that were included in 2 domains.
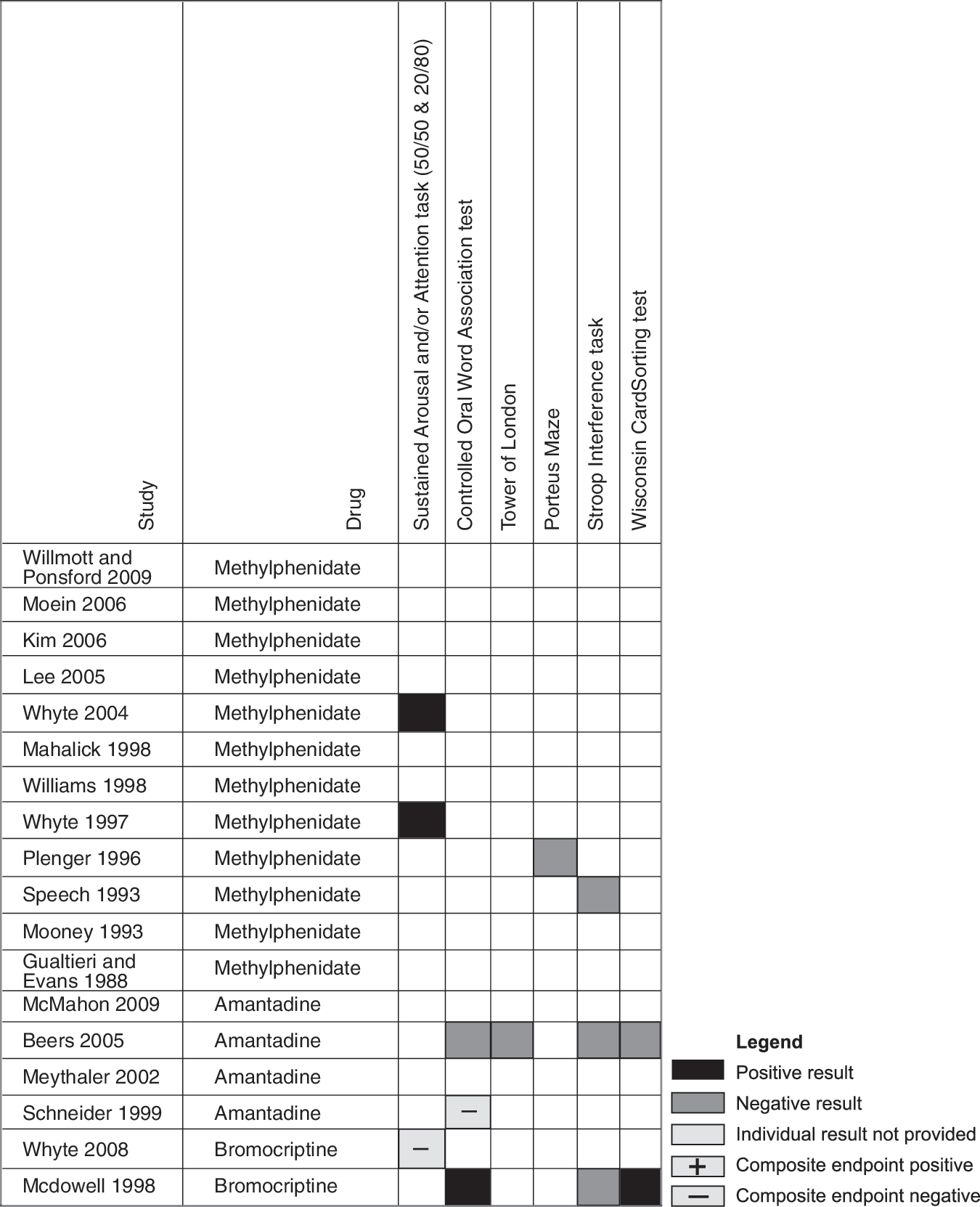
Tests assessing executive functioning.
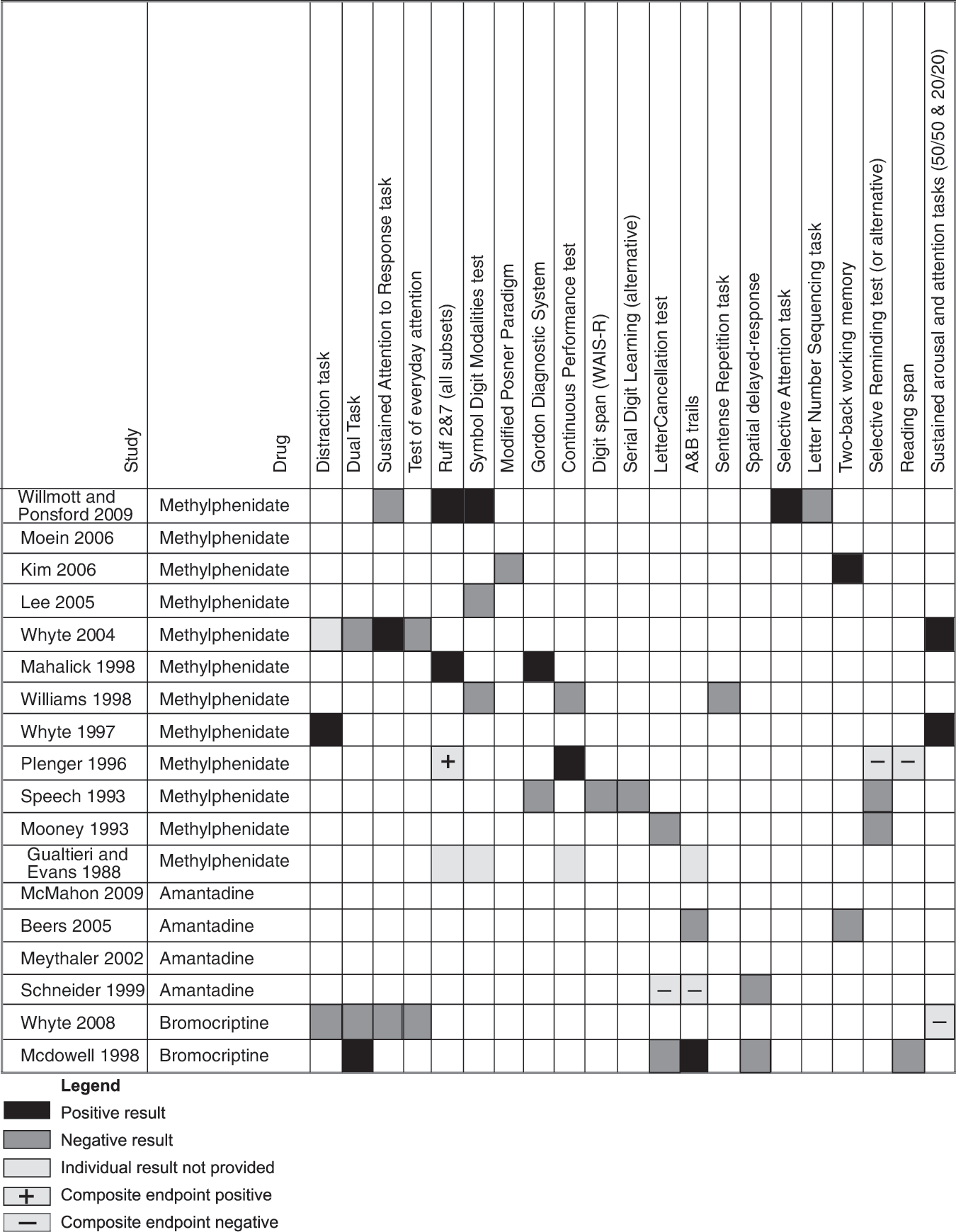
Tests assessing attention (WAIS-R, revised Wechsler Adult Intelligence Scale).
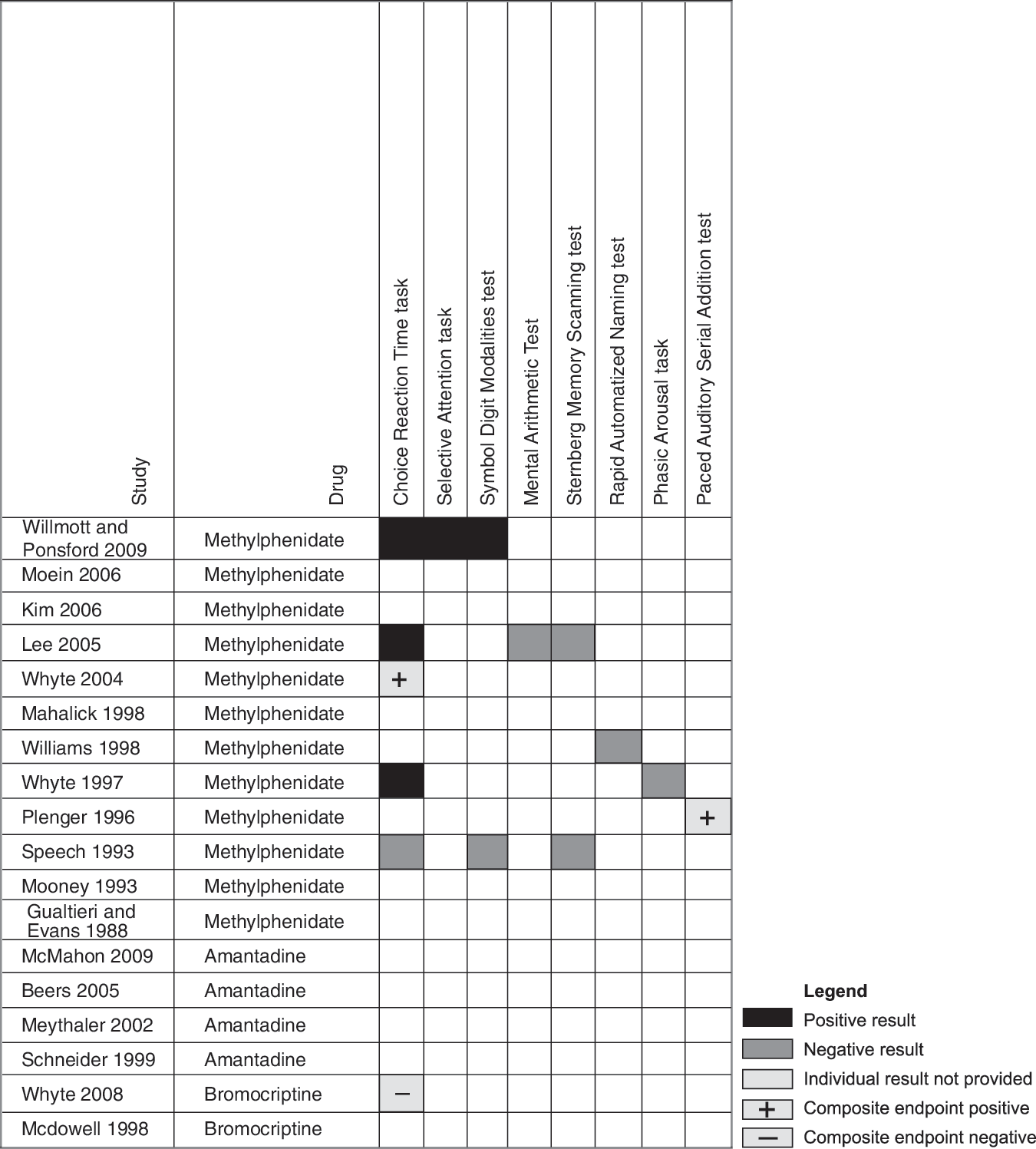
Tests assessing processing speed and reaction time.
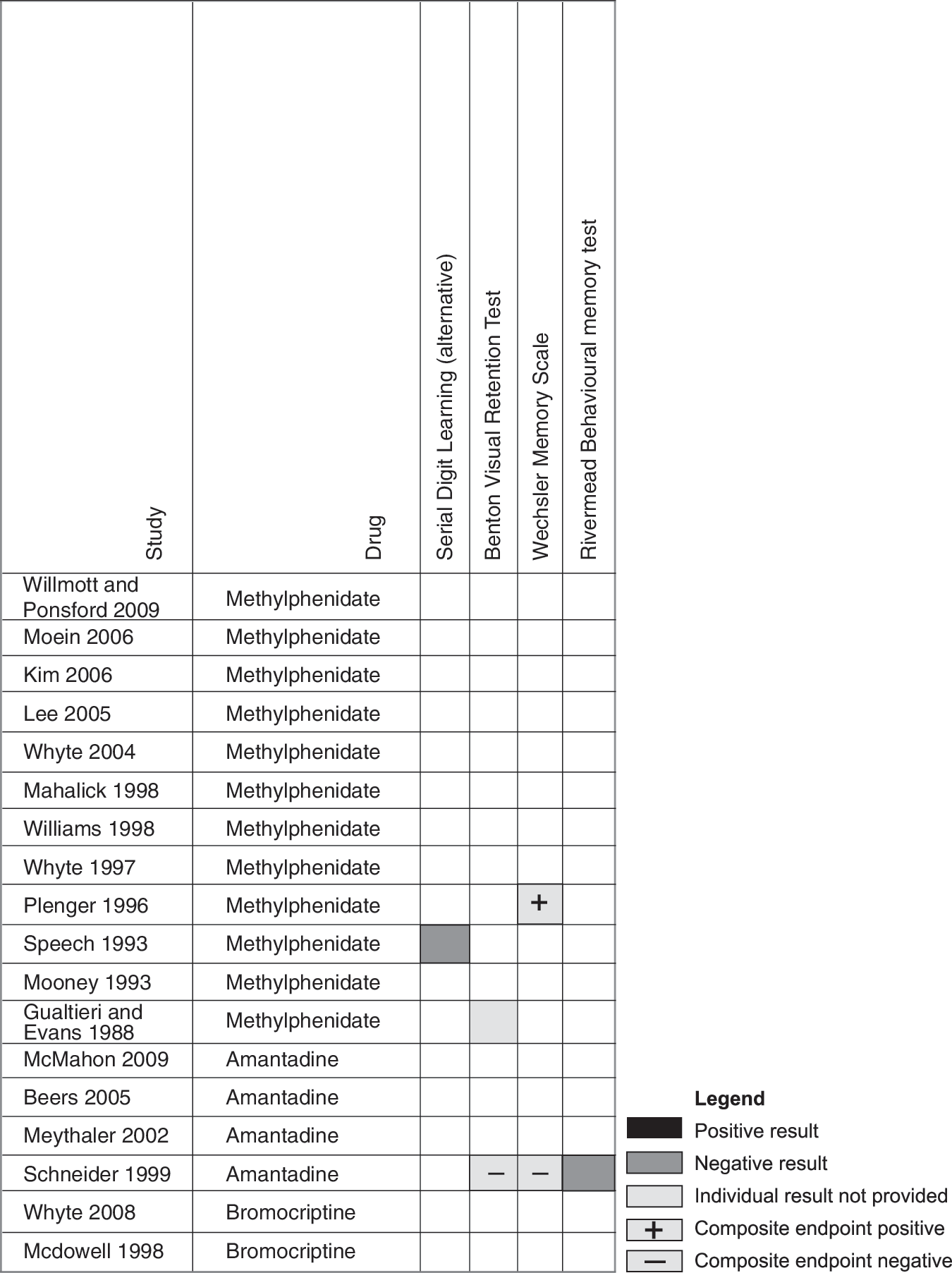
Tests assessing memory.
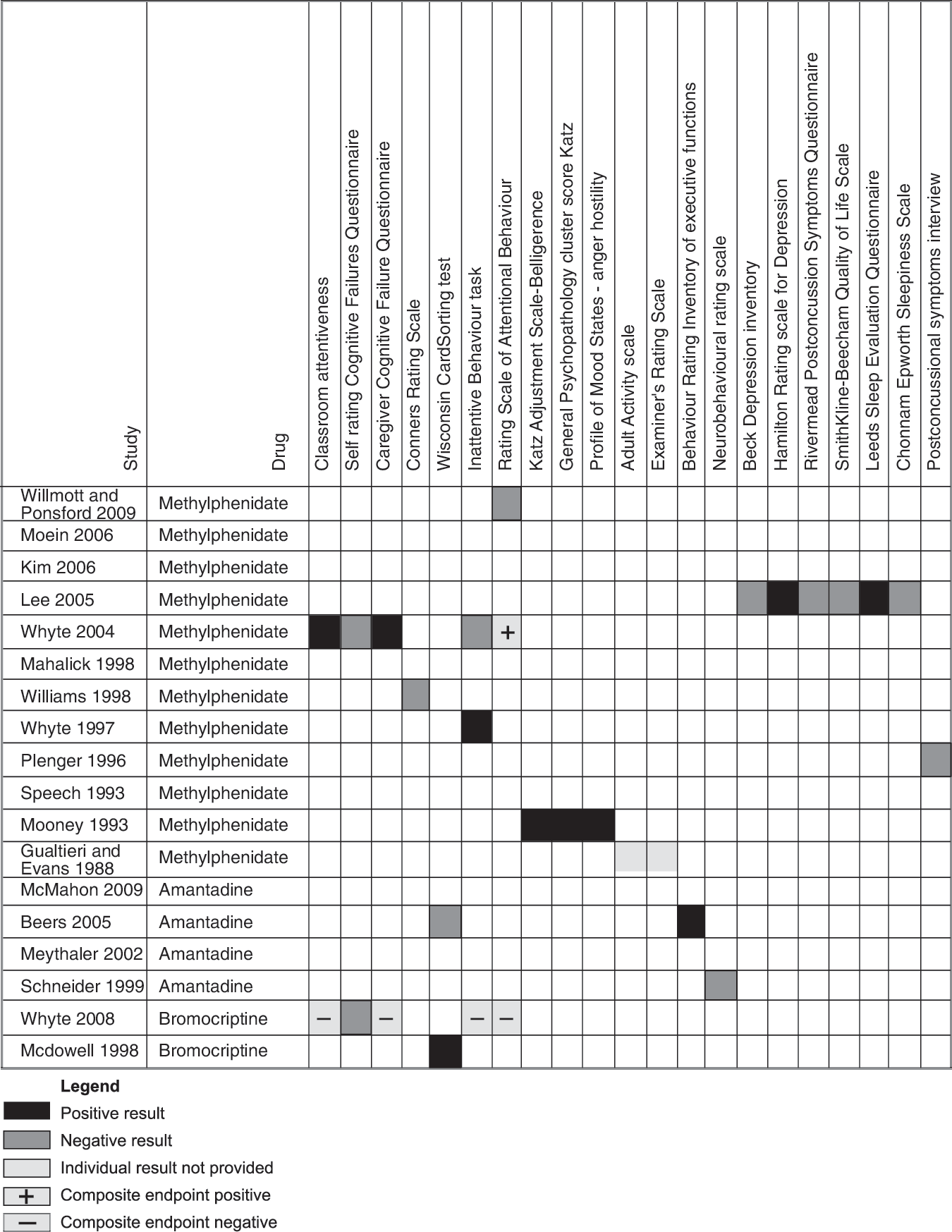
Tests assessing mood and behavior.
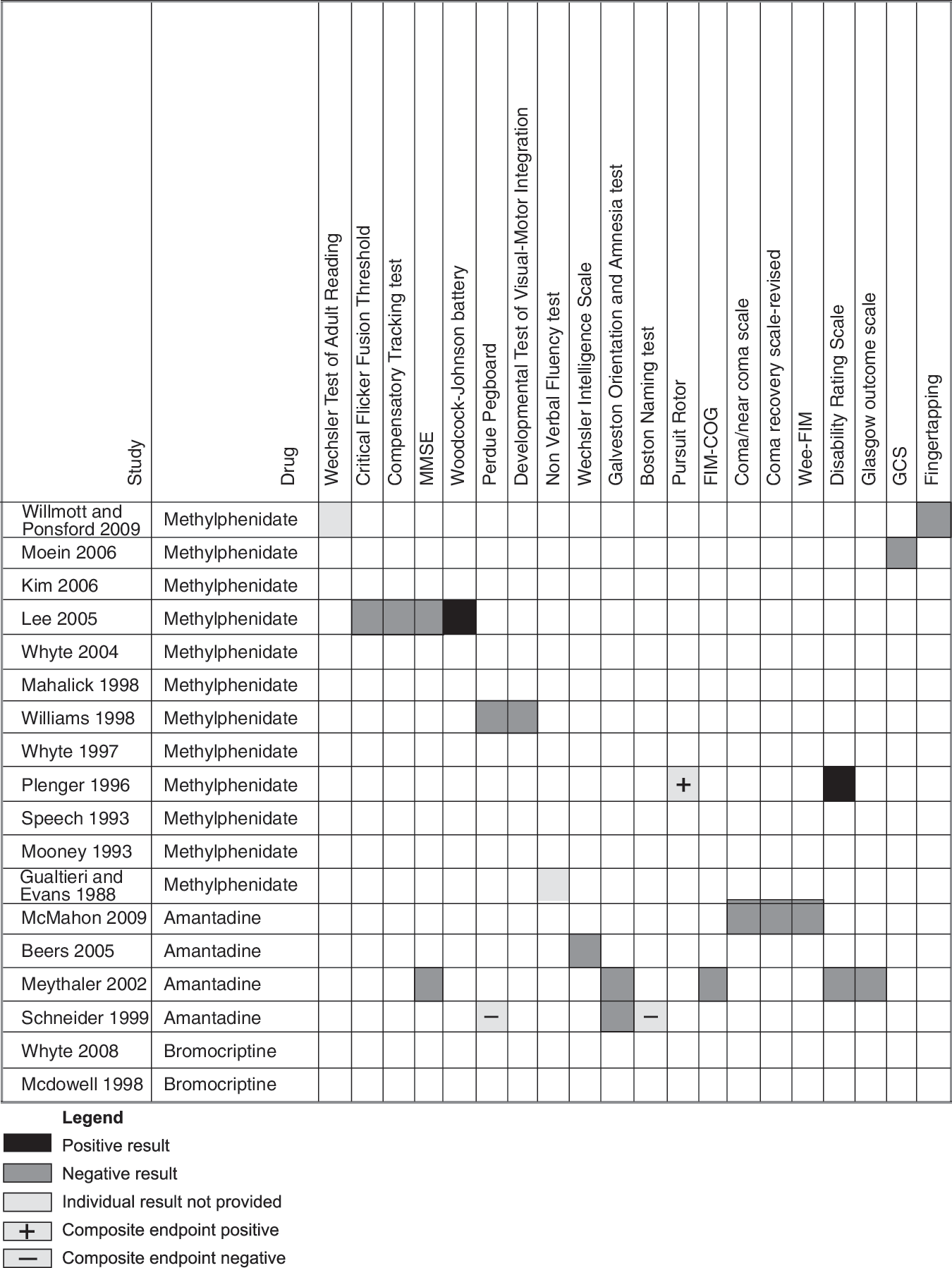
Other tests (MMSE, Mini-Mental State Examination; FIM-COG, Functional Independence Measure trademark-cognitive; Wee-FIM, Functional Independence Measure for Children; GCS, Glasgow Coma Scale).
Executive functioning
Executive functioning was assessed by a total of 6 tests in 8 studies. Three tests showed statistically positive results in at least one study (Fig. 2). Only “Sustained Arousal” and “Attention tasks,” an experimental test, showed positive results in two different studies (Whyte et al., 1997,2004). These two studies evaluated methylphenidate in rehabilitating severe TBI.
Attention
A total of 21 tests were used to evaluate attention in 15 studies (Fig. 3). Of these, 10 tests (48%) yielded statistically positive results in at least one study. Two tests (Ruff 2&7 and Sustained arousal and attention tasks) had statistically significant positive results confirmed by two different studies (Mahalick et al., 1998; Whyte et al., 1997,2004; Willmott and Ponsford, 2009). All these studies evaluated methylphenidate in a heterogeneous population including mild to severe TBI. Out of the 21 tests, 9 (43%) were experimental measures.
Reaction time
Processing speed and reaction time was evaluated in 8 studies, using a total of 8 different tests (Lee et al., 2005; Plenger et al., 1996; Speech et al., 1993; Whyte et al., 1997, 2004, 2008; Williams et al., 1998; Willmott and Ponsford, 2009; Fig. 4). Five of them were experimental. Positive results were shown by 3 tests. Choice reaction time task, a test used in all 8 studies, yielded positive results in 50% of subjects (Lee et al., 2005; Whyte et al., 1997; Willmott and Ponsford, 2009). Studies showing positive results evaluated methylphenidate in mild and severe TBI, with duration of treatment varying from 6 days to 4 weeks.
Memory
Memory was assessed by only 4 studies (Gualtieri and Evans, 1988; Plenger et al., 1996; Schneider et al., 1999; Speech et al., 1993), using a total of 4 tests (Fig. 5). All tests are published. Only 2 studies report individual test results, both not showing any statistically significant difference.
Mood and behavior
A total of 21 tests were used to evaluate mood or behavior (Fig. 6). No trend can be drawn from the analysis of the results. A total of 6 studies showed positive results on a behavioral measure (Beers et al., 2005; Lee et al., 2005; McDowell et al., 1998; Mooney and Haas, 1993; Whyte et al., 1997,2004), but none of these positive results were replicated in another study.
Other measures
A total of 20 tests could not be classified as either a cognitive domain measure or a behavior measure, and are thus classified as other measures (Fig. 7). Of these, the Woodcock-Johnson battery, measuring general intellectual ability, specific cognitive abilities, scholastic aptitude, oral language, and achievement, showed positive results in one study (Lee et al., 2005). The Disability Rating Scale, which measures general functional changes over the course of recovery from TBI, yielded positive results in one study (Plenger et al., 1996), which were not corroborated by a second (Meythaler et al., 2002).
In summary, no clear beneficial effect could be drawn in any of the predefined categories of outcome (see Figs. 2 –7). Predetermined sensitivity analyses did not provide additional information.
Safety outcomes
Twelve of 20 studies reported evaluation of adverse events (Alban et al., 2004; Beers et al., 2005; Lee et al., 2005; McMahon et al., 2009; Meythaler et al., 2002; Moein et al., 2006; Mooney and Haas 1993; Plenger et al., 1996; Schneider et al., 1999; Whyte et al., 2008; Williams et al., 1998; Willmott et al., 2009). However, only 5 studies (Alban et al., 2004; McMahon et al., 2009; Plenger et al., 1996; Williams et al., 1998; Willmott et al., 2009) systematically assessed safety using pre-defined objective measures or a tool for at least one side effect.
Two RCTs evaluating methylphenidate reported results of side effects in a second publication as a primary outcome: Whyte and associates (2004) in Alban and associates (2004), and Willmott and Ponsford (2009) in Willmott and associates (2009). Although both studies mentioned a statistically significant increase in blood pressure and heart rate, their clinical significance was not described. Among the 10 remaining studies using methylphenidate, 5 reported the evaluation of side effects (Table 2). No study reported systematic measures of aggressive behavior, agitation, or delirium. All four studies using amantadine reported side effects. Most side effects were reported as minor, and resolved spontaneously upon discontinuation of the study drug.
?=total number of events impossible to calculate since data were not provided by at least one study.
All side effects were predetermined except for side effects listed in the “others” section.
Itching and tremors were the most common side effects reported among patients on bromocriptine. However, the incidence did not differ significantly from placebo.
Five patients were withdrawn from the study because of either probable or possible side effects (Beers et al., 2005; Schneider et al., 1999; Whyte et al., 2008). These included vomiting, dizziness, and elevated blood pressure, light-headedness and behavioral agitation, and rash and seizure.
Risk of bias
The analysis of risk of bias revealed that the majority of studies did not provide enough information on sequence generation and allocation concealment to assess their appropriateness (Table 3). All but one study (Mooney and Haas, 1993) were double-blinded, but the efficacy of randomization was rarely assessed. Of note, in 2 studies, the majority of patients or caregivers correctly guessed their attrition (Speech et al., 1993; Willmott and Ponsford, 2009). None of the studies had a published version of their protocol. Therefore, the selective reporting item could not be evaluated. Other sources of bias could be found in the majority of studies, and are described in Table 3. Based on the Cochrane Handbook for Systematic Reviews, crossover design was considered appropriate if the randomized population included only stable patients (Higgins et al., 2008). Based on this criterion, crossover design was considered inappropriate in all studies. The most common bias retrieved in parallel design studies was selection bias. A lack of information did not allow comparison of groups to determine the efficacy of randomization.
U, uncertain risk of bias; H, high risk of bias; L, low risk of bias; MPH, methylphenidate; B, bromocriptine; AM, amantadine.
Discussion
In this systematic review, we identified 20 RCTs evaluating the effect of DA on different functional outcome measures. However, considering the important clinical inconsistencies, a meta-analysis of the included studies could not be performed. As an effect, we could not draw meaningful conclusions regarding the efficacy of dopamine agonists in the patient recovering from TBI. The main factors contributing to our inability to pool data were the lack of consistency concerning patient severity of trauma, timing from injury, pre-randomization psychological and cognitive condition, and most importantly, the wide range of clinical outcome measures used in the different studies. While other systematic reviews of pharmacological therapies including dopamine agonists exist (Fleminger et al., 2006; Sivan et al., 2010; Writer and Schillerstrom, 2009), this is the first to focus on the use of these drugs specifically in patients suffering from TBI, and to evaluate both cognitive and behavioral outcomes in addition to other meaningful clinical outcomes from an acute care point of view. Methodological limitations of other reviews include the use of a unique database, inclusion of non-randomized trials, an incomplete search strategy description, language restriction, and lack of rigorous evaluation of bias (Sivan et al., 2010; Writer and Schillerstrom, 2009).
The impressive number of different tests used to assess neuropsychological outcomes in the included studies may be due to different reasons, such as the lack of a gold standard, the broad range of year of publication, the familiarity with a particular battery of tests available, and the resources available to researchers in different settings. Many studies used non-validated or experimental tools to assess outcomes. Moreover, clinical interpretation of statistically significant results was often difficult due to a lack of effect size and reliable change index reporting, the use of composite measures, and the lack of reproducibility of the neuropsychological tests among the patients. Choice of outcome measures and their analysis in TBI is still a matter of debate (Bagiella et al., 2010; Maas et al., 2010). Heterogeneity in outcome measures precludes any comparison between studies, and consequently from drawing conclusions regarding the efficacy of DA in TBI. Different groups have proposed various validated outcome combinations, including quality of life, neurobehavioral and neuropsychological status, and global functional outcome, but none has reached the status of a gold standard (Shukla et al., 2011). Future studies should aim at evaluating outcomes that are well described in the literature, validated, appropriate for international use, have well established normative data, are applicable to a broad spectrum of TBI, and are easy to administer (Wilde et al., 2010). Consequently, the Traumatic Brain Injury Outcome Workgroup has proposed selected outcomes evaluating different domains according to those recommendations in both adults and pediatric populations (McCauley et al., 2011; Wilde et al., 2010). Perhaps these recommendations should guide future studies regarding the efficacy of DA in TBI.
The poor methodological quality of the included studies was another concerning finding. The majority of studies used a crossover design, which may be appropriate when high inter-patient heterogeneity is likely, such as in a TBI population. However, patient condition should be stable in order to avoid the natural evolution of the condition to account for the benefit or harm. Evolution and brain recuperation from a TBI may continue to occur up to several years after injury and is not predictable (Lammi et al., 2005). A crossover design also mandates a washout period between treatments, which has to be long enough to avoid a carry-over effect. It has been shown that dopamine receptors can downregulate during treatment and upregulate following cessation of therapy in patients suffering from Parkinson's disease (Thobois et al., 2004). In the studies identified, the washout period was often not long enough to avoid a carry-over effect. The use of a parallel design, which would overcome the carry-over problem, is limited by the heterogeneity of the TBI population, which poses a methodological challenge. Similarity of the study groups seen in this population is often impossible to achieve unless large sample sizes are used, and pre-specified covariate adjustments are made (Maas et al., 2004,2010).
Assessment of safety was not consistent between studies, and a lack of rigor in the methodology of side-effect evaluation was considered a major limitation. Although some studies did use a questionnaire or a standardized tool to assess side effects, they often relied on self-reporting of symptoms. The studies also often failed to look prospectively for potentially concerning side effects in a TBI population. Neurological and psychiatric adverse reactions such as seizures, delirium, hallucinations, and insomnia should be targeted as key safety outcomes, since they are clinically relevant in the TBI population, and are associated with the use of dopamine agonists in other human populations and animal models (Barone et al., 1992; Wood, 2010). A lack of information regarding diagnosis of these side effects was also an issue.
Despite the results of our review, the dopaminergic system is an obvious target for research of cognitive impairments in TBI. Dopamine receptors are known to be present in many areas of the brain important to cognition, and are often damaged post-TBI (the hippocampus, striatum, and frontal cortex; Bales et al., 2009). The role of dopamine receptors in cognitive domains such as attention, working memory, executive functioning, and speed of processing is still a matter of debate (Nieoullon, 2002). However, some observations in humans showing impairment in visuospatial, executive, and verbal fluency tests related to induced parkinsonism lead one to think that dopamine participates in cognition (Burruss et al., 2000; Nieoullon, 2002; Stern et al., 1990). Radioimaging studies in patients with Parkinson's disease, schizophrenia, and attention-deficit/hyperactivity disorder provides supporting evidence (Bruck et al., 2001; Duchesne et al., 2002; Heilman et al., 1991; Tanaka, 2006).
The influence of dopaminergic drugs on neuronal plasticity, a concept of brain adaptation to injury over time, is also a concerning feature (Ampuero et al., 2010; Larson and Zollman, 2010). Dysfunction of the molecular processes influencing neuronal plasticity in the hippocampus may be a potential cause for temporal and spatial memory impairment seen in TBI (Ampuero et al., 2010; Falo et al., 2006). The role for dopamine pathways in this process is unclear, but some data suggest that a modification of plasticity occurs with the exposure of various neurotransmitter agonists and antagonists, including dopamine (Bales et al., 2009; Meintzschel and Ziemann, 2006). For example, benzodiazepines and haloperidol have been incriminated as possible causes of adverse effects on neuronal plasticity (Ampuero et al., 2010; Falo et al., 2006). Proper safety evaluation of dopamine agonists in TBI is therefore warranted.
Conclusion
This systematic review is the first to evaluate the effect of the administration of dopamine agonists on different domains of cognition, behavior, and safety in TBI patients. Because of the significant clinical heterogeneity in the outcome measures used in the different studies, pooled analyses could not be performed, and consequently clear conclusions about the efficacy or safety of dopamine agonists in TBI patients are difficult to draw. Despite the low incidence of adverse events reported, most studies did not systematically screen for them. In summary, our systematic review does not support the use of dopamine agonists as part of the treatment regimen for improving functional outcome measures in either the acute or sub-acute phases of care in TBI patients. Future studies should first aim at standardizing and validating a neuropsychological battery of tests in TBI. A clinical trial of dopamine agonists in TBI could then be designed using standardized outcome measures with clear clinical significance, including a validated neuropsychological battery of tests. It should also use a parallel design in a large sample with predefined covariates, and should systematically screen for potential side effects.
Footnotes
Acknowledgments
The authors would like to thank Ms. Marie-Soleil Delisle, Ms. Marie Frenette, and Ms. Jodi Peters for their help with this study.
Author Disclosure Statement
No competing financial interests exist.
| 1 | head trauma.mp. | 9919 |
| 2 | head injury.mp. | 36681 |
| 3 | head injuries.mp. | 11177 |
| 4 | brain trauma.mp. | 2421 |
| 5 | “brain injuries”.mp. or expBrain Injuries/ | 105383 |
| 6 | cerebral trauma.mp. | 998 |
| 7 | cerebral injury.mp. | 2592 |
| 8 | cerebral injuries.mp. | 666 |
| 9 | “craniocerebral trauma”.mp. or exp Craniocerebral Trauma/ | 211373 |
| 10 | craniocerebral injury.mp. | 920 |
| 11 | craniocerebral injuries.mp. | 1008 |
| 12 | brain injury.mp. | 81937 |
| 13 | Traumatic brain injury.mp. | 24215 |
| 14 | Traumatic brain injuries.mp. | 1275 |
| 15 | 1 or 2 or 3 or 4 or 5 or 6 or 7 or 8 or 9 or 10 or 11 or 12 or 13 or 14 | 234953 |
| 16 | exp Dopamine Agonists/ | 134451 |
| 17 | dopamine agonist$.tw. | 11285 |
| 18 | bromocriptine.tw. | 12227 |
| 19 | amantadine.tw. | 5300 |
| 20 | levodopa.tw. | 14134 |
| 21 | methylphenidate.tw. | 8292 |
| 22 | apomorphine.tw. | 15887 |
| 23 | ropinirole.tw. | 1058 |
| 24 | pramipexole.tw. | 1367 |
| 25 | pergolide.tw. | 2025 |
| 26 | cabergoline.tw. | 1591 |
| 27 | exp Dopamine Agents/ | 298400 |
| 28 | or/16-27 | 312593 |
| 29 | 15 and 28 | 3630 |
| 30 | Randomized controlled trial.pt. | 572709 |
| 31 | Controlled clinical trial.pt. | 160808 |
| 32 | randomized.ab. | 548100 |
| 33 | placebo.ab. | 338077 |
| 34 | Drug therapy.fs. | 1393362 |
| 35 | randomly.ab. | 359540 |
| 36 | group.ab. | 2580745 |
| 37 | trial.ab. | 506749 |
| 38 | 37 or 36 or 35 or 34 or 33 or 32 or 31 or 30 | 4626546 |
| 39 | 38 and 29 | 925 |
| 40 | remove duplicates from 39 | 790 |