
Abstract
Despite negative neuroimaging findings in concussed athletes, studies indicate that the acceleration and deceleration of the brain after concussive impacts result in metabolic and electrophysiological alterations that may be attributable to changes in white matter resulting from biomechanical strain. In the present study we investigated the effects of sports concussion on white matter using three different diffusion tensor imaging (DTI) measures: fractional anisotropy (FA), mean diffusivity (MD), and axial diffusivity (AD). We compared a group of 10 non-concussed athletes with a group of 18 concussed athletes of the same age (mean age 22.5 years) and education (mean 16 years) using a voxel-based approach (VBA) in both the acute and chronic post-injury phases. All concussed athletes were scanned 1–6 days post-concussion and again 6 months later in a 3T Siemens Trio™ MRI. Three 2×2 repeated-measures analyses of variance (ANOVAs) were conducted, one for each measure of DTI used in the current study. There was a main group effect of FA, which was increased in dorsal regions of both corticospinal tracts (CST) and in the corpus callosum in concussed athletes at both time points. There was a main group effect of AD in the right CST, where concussed athletes showed elevated values relative to controls at both time points. MD values were decreased in concussed athletes, in whom analyses revealed significant group differences in the CST and corpus callosum at both time points. Although the use of VBA does limit the analyses to large tracts, and it has clinical limitations with regard to individual analyses, our results nevertheless indicate that sports concussions do result in changes in diffusivity in the corpus callosum and CST that are not detected using conventional neuroimaging techniques.
Introduction
A
Most conventional imaging techniques rarely reveal structural damage to the sports-concussed brain (Ellemberg et al., 2009; Johnston et al., 2001). However, the presence of metabolic disturbances in young adults, and electrophysiological anomalies found in both young adults and older, former athletes that can persist for months to several years after injury, suggest that there might be physical injury to the concussed brain, the consequences of which may extend beyond metabolic and electrophysiological alterations (De Beaumont et al., 2007a,2007b,2009; Henry et al., 2010; Vagnozzi et al., 2008,2010).
Peerless and Rewcastle (1967) specified the nature of these physical injuries as shear strain to white matter (WM) or diffuse axonal injury (Gentry, 1994), though the term “traumatic axonal injury” (TAI) is now used more frequently (Buki and Povlishock, 2006; Gennarelli, 1996). TAI is more commonly seen at gray-white matter junctions (Ducreux et al., 2005a,2005b; Huisman et al., 2004; Lee et al., 2006; Le et al., 2005; Okumura et al., 2005; Song et al., 2002), because the two tissue types differ in their respective rigidity (Barr, 2005; Holbourn, 1945) due to the myelin sheaths that surround WM axons. Shear strain injuries occur when local strains and strain rates exceed a critical threshold, at which axons are affected (Bain and Meaney, 2000; Gennarelli et al., 1989). They occur most often when the skull and brain are accelerated around the midline axis by a force vector that deforms the brain (Ommaya and Gennarelli, 1974). In landmark studies from the 1940s, Holbourn simulated the movement of the brain using gel models (1943,1945), when the significance of angular acceleration was first suggested. These studies were supported by animal work that showed very similar movement patterns in nonhuman primates, in which a clear plastic window was used to view the movement of the brain upon impact (Pudenz and Shelden, 1946).
Diffusion tensor imaging (DTI) provides information about the brain's microstructure by quantifying isotropic (typical of gray matter) and anisotropic (typical of WM) water diffusion. DTI measurements are based on the fact that the network of fibers within the brain is composed of a distinct microstructure that inherently constrains the flow of water molecules. Water diffuses primarily along the WM fibers, and is constrained in the direction perpendicular to them. DTIs numerically model this process via ellipses whose long axis is aligned with the most likely direction of the fiber in a voxel. One of DTI's main uses in neurology is detecting the presence of axonal injury (Toga and Mazziotta, 2002).
Indeed, there is increasing evidence to suggest that TAI is present in traumatic brain injury (TBI) across the severity spectrum, and that the extent of the damage is related to the severity of the injury as defined by the initial Glasgow Coma Scale score (Huisman et al., 2004). Likewise, Kraus and associates (2007) investigated TBI in adults across the severity spectrum using DTI, and also found the degree of TAI to be related to the severity of the injury, with severe TBI patients exhibiting the greatest extent of damage. The presence of axonal shearing in people with mild, moderate, and severe TBI alike suggests that the brains of concussed athletes undergo similar changes, though perhaps to a lesser extent than is observed in more severe TBI.
Few studies have focused on TAI in the acute post-injury phase (days to weeks); however, recent work has shown that damage can be detected within the first week of injury (Miles et al., 2008; Wilde et al., 2008). Several case studies using DTI on TBI patients have consistently noted reduced diffusion in the brain, especially around the corpus callosum, in adults soon after injury (Huisman et al., 2004; Lee et al., 2006). Furthermore, the axonal shearing observed in people with mTBI has functional consequences. Lee and colleagues (2006) noted that the brain areas affected by axonal injury corresponded to the types of neuropsychological dysfunction that patients exhibited.
Diffusion alterations are also evident in the chronic post-injury phase (months to years). Several studies investigating mTBI using whole-brain DTI analysis techniques in adult samples taken from emergency departments have found diffuse WM differences in the corpus callosum (Wilde, et al., 2008), and the frontotemporal (Chu et al., 2010) and midbrain regions (Hartikainen et al., 2010), which manifest as changes in fractional anisotropy (FA), mean diffusivity (MD), radial diffusivity (RD), and axial diffusivity (AD). A study using tract-based statistics to investigate mTBI in adults found that symptom-free patients showed no differences in diffusion variables relative to controls, though symptomatic patients demonstrated higher MD values overall than both controls and asymptomatic patients in the corpus callosum, the right anterior thalamic radiations, the superior longitudinal fasciculus, the inferior longitudinal fasciculus and the fronto-occipital fasciculus bilaterally (Messé et al., 2010). A study investigating concussed college athletes who had been symptomatic for at least 1 month found no changes in FA, but did find that concussed athletes showed significantly increased MD in the left hemisphere (specifically parts of the inferior/superior longitudinal and fronto-occipital fasciculi, the retrolenticular part of the internal capsule, and posterior thalamic and acoustic radiations), using a WM skeleton in which only the middle of the tracts are analyzed (Cubon et al., 2011).
In the current study we sought to further investigate the presence of TAI in concussed athletes in the acute (2–6 days post-injury) and chronic (6 months post-injury) phases, using a whole-brain voxel-based method. We hypothesized that concussed athletes would demonstrate changes, either increases or decreases, in FA and MD as well as AD in concussed athletes relative to control athletes at both time points. We further hypothesized that the corpus callosum would demonstrate particular vulnerability, as is consistent with the extant literature (Ducreux et al., 2005a; Wilde et al., 2008), but that the corticospinal tract (CST) would also be found to be vulnerable to the effects of concussion, as has been suggested using other techniques such as transcranial magnetic stimulation (De Beaumont et al., 2007b,2009), and magnetic resonance spectroscopy (Henry et al., 2010).
Methods
Participants
All participants in this study were active male football players for university level intervarsity sports teams and were recruited with help from the team physician and physiotherapists. Athletes were excluded from participation if there was a history of alcohol and/or substance abuse; psychiatric illness; learning disability; neurological disorders (seizure disorder, central nervous system neoplasm, or brain tumor); and TBI unrelated to contact sports. None of the athletes who participated in this study were taking psychotropic medications at the time of testing. Concussion severity, determined by the team physician, varied from grade 1 (confusion for less than 15 min without amnesia or loss of consciousness) to grade 3 (loss of consciousness, duration either brief [seconds] or prolonged [minutes]), according to the parameters set out by the American Academy of Neurology Quality Standards Subcommittee and Neurology AAo (1997). The study was composed of one experimental group of 16 athletes who suffered a sports concussion examined at two different time points, and a control group (n=8) composed of athletes who had no history of head injury. The concussed (mean age 22.08 years, SD=1.72 years) and the control (mean age 22.81 years, SD=1.53 years) groups were statistically equivalent for age (p=0.29). Similarly, concussed athletes had a mean of 15.8 years (SD=2.16 years) of education, while control athletes had a mean of 16.08 years (SD=1.56 years) of education (p=0.75). Additionally, at the time of each scan symptom scores were calculated using the Post-Concussion Symptom Scale (PCSS), with symptoms rated on a Likert scale from 0 (non-existent) to 6 (very severe). Symptoms on the PCSS include headache, feeling pressure in the head, sensitivity to light, sensitivity to noise, dizziness, vision changes, feeling slowed down, feeling foggy, changes in sleep, fatigue, drowsiness, memory difficulty, concentration difficulty, increased irritability, increased sadness, emotional lability, anxiety, nausea, vomiting, and numbness or tingling. The symptom scores were calculated by adding the Likert scale ratings from each symptom as reported by each athlete.
All neuroimaging was performed at the Unité de Neuroimagerie Fonctionelle (UNF) of the Centre de Recherche de l'Institut Universitaire de Gériatrie de Montréal, using a Siemens Trio™ 3-T whole-body MRI system (Siemens, Erlangen, Germany). This study was approved by the research and community ethics boards at the UNF and the Université de Montréal, and done in compliance with the code of ethics as stated in the Declaration of Helsinki. All subjects gave informed consent following careful screening for MRI compatibility. None of the concussed athletes contacted for this study refused participation. Concussed athletes were scanned within the first 5 days of injury (mean=81.92 h, SD=46.74 h). The second scan took place 6 months after the initial scan for the concussed group (mean=6.375 months, SD=0.41 month), and 18 months after the initial scan for controls (n=8, mean=18.24 months, SD=10.29 months). Only athletes who were able to be scanned at both time points were included in the analyses. While the difference between follow-up scans was quite large, the work of Westlye and colleagues (2010) suggests that there were no detectable differences between participants of such a tight age range.
Imaging parameters were: diffusion weighting gradients applied in 64 directions with b values of 0 and 700 sec/mm2 and four averages in each direction, repetition time of 12,800 msec, echo time of 101 msec, field of view of 256×256 mm2, matrix size of 128×128 with partial Fourier reconstructed to 6/8, slice thickness of 2 mm with 0.6-mm gaps, and 75 slices. 3D T1-weighted images of corresponding subjects were also acquired with an inversion recovery rapid gradient echo sequence using a 3T Trio Siemens MRI scanner. Acquisition parameters were as follows: TI/TR/TE=1500/2500/3.83 msec; flip angle=15 degrees; slice thickness=0.9 mm, with an acquisition matrix of 256×256×256. Total scan time was 28 min (4 min localizers, 9 min MPRage, and 15 min DTI).
Image preprocessing and registration
Extracerebral tissues were removed from the 3D structural MRIs using iMagic Pro 2.0 software (Neuronic S.A., 2007) followed by manual editing. Edited scans were linearly registered to a high-resolution single-subject brain template image using FLIRT software (Jenkinson and Smith, 2001). A minimal deformation target (MDT) was generated from the 26 subjects (using the method described in Kochunov et al., 2001), and each 3D structural image was warped to the MDT using a 3D fluid registration algorithm that allows large deformations while guaranteeing diffeomorphisms (Lepore et al., 2006,2008). Jacobian matrices representing local volume expansions or contractions relative to the template image were calculated from the deformation fields for each subject. From the diffusion-weighted images, voxel-wise diffusion tensors were generated with MedINRIA (
Deformation fields from the nonlinear registration of T1-weighted images were applied to the diffusion tensor images to warp them to a common space. The finite strain (FS) method was applied to compute the tensor rotations to the affine transformation matrix M (Alexander et al., 2001). We then applied a preservation of principal direction (PPD) algorithm on the higher-order transformation (Alexander et al., 2001; Zhang et al., 2006).
Voxel-wise statistics
The most common univariate anisotropy measure, FA, is defined in terms of the eigenvalues, λ
i
, i=1,2,3, of the diffusion tensor as:
with
We applied a voxel-wise 2×2 repeated-measures analysis of variance (ANOVA) using SPM8 to the derived scalar images (FA, AD, and MD), with a significance threshold of .01 divided by the number of derived scalar images computed for a final significance threshold of .003 in order to be conservative in our estimate of significant differences, and to account for the use of multiple comparisons. Because each cluster is composed of several voxels, each with its own F value, cluster results are reported as ≥or ≤0.003, along with the maximum F value in the cluster.
The mean FA values and standard deviation of each cluster shown in Figure 1 were recorded. Similarly, analogous areas from the opposite hemisphere were also included. In concussed athletes, a WM structure with an FA value increased by more than 2.5 SDs above the mean for that region of interest in the control group was considered damaged. The value of 2.5 SDs was chosen to be consistent with the work of Niogi and associates, who performed a similar analysis (2008). Such an individualized investigation of the concussed athletes was included to account for the heterogeneity of injury (see Fig. 1 for example FA maps).
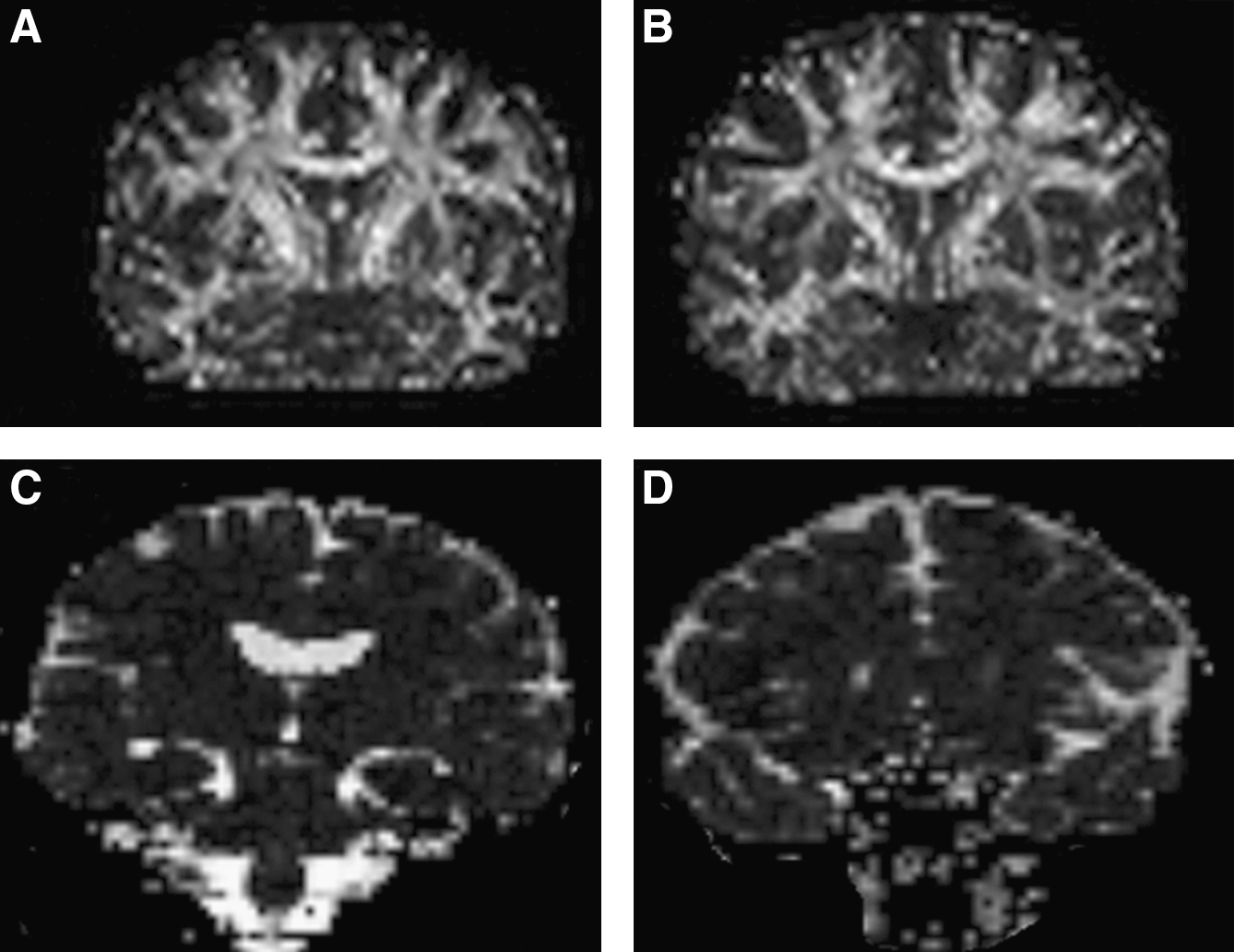
Example fractional anisotropy (FA) maps of one control athlete (
Results
Initially, three 2×2 repeated-measure ANOVAs were conducted, one for each dependent measure of DTI used in the study: FA, MD, and AD. All significant results represent voxel clusters with a p value of .003 or less. Averaged F values derived from each individual subject were then further calculated.
Prominent FA increases were detected in the corpus callosum, as well as throughout the CSTs in the concussed group [F(1,46)≥18.86, p<0.003]. Though not affected along the entire length, the corpus callosum showed augmented FA values at the genu and posteriorly in the body. Within the right hemisphere, underlying primary motor and sensory cortices continuing ventrally through the CST to the level of the thalamus demonstrated elevated FA values (Fig. 2). In contrast, the left hemisphere showed only sparse changes in FA in the dorsal regions immediately underlying the primary motor and sensory cortices, whereas more ventral regions remained statistically non-significant. There was no main effect of time from the acute phase to the chronic phase [F(1,46)≤9.7, p<0.003], nor was there a significant group×time interaction [F(1,46)≤9.7, p<0.003].

Differences in fractional anisotropy (FA) between control and concussed athletes. (
AD showed a more complex pattern of results (Fig. 3). There was a main effect of group at the dorsal end of the CST underlying the primary motor cortex in the right hemisphere in the same areas showing higher FA values. Concussed athletes showed greater AD values than control athletes [F(1, 46)≥23.77, p<0.003]. Unlike FA, there were no significant AD differences in the corpus callosum, nor were there areas within the left hemisphere that demonstrated significant differences between the two groups. There was no main effect of time and no significant group×time interaction, demonstrating the stability of both groups across time [F(1,46)≤9.7, p<0.003].

Differences in axial diffusivity (AD) between control and concussed athletes. (
MD demonstrated significant differences along the CST and corpus callosum (Fig. 4). Though there were no significant group×time interactions [F(1,46)≤13.23, p<0.003], there was a main effect of group seen in the body of the corpus callosum, where MD values were lower in concussed athletes relative to their control counterparts [F(1,46)≥9.8, p<0.003]. Group effects were also seen within ventral portions of the CST, where again concussed athletes showed lower MD than controls [F(1,46)≥9.8, p>0.003]. Similarly to what was seen with respect to the FA and AD data, there was no effect of time [F(1,46)≤9.7, p>0.003; Tables 1 and 2], which underscores the stability of the control and concussed groups, not only across time, but also across the diffusion parameters used in the current study.
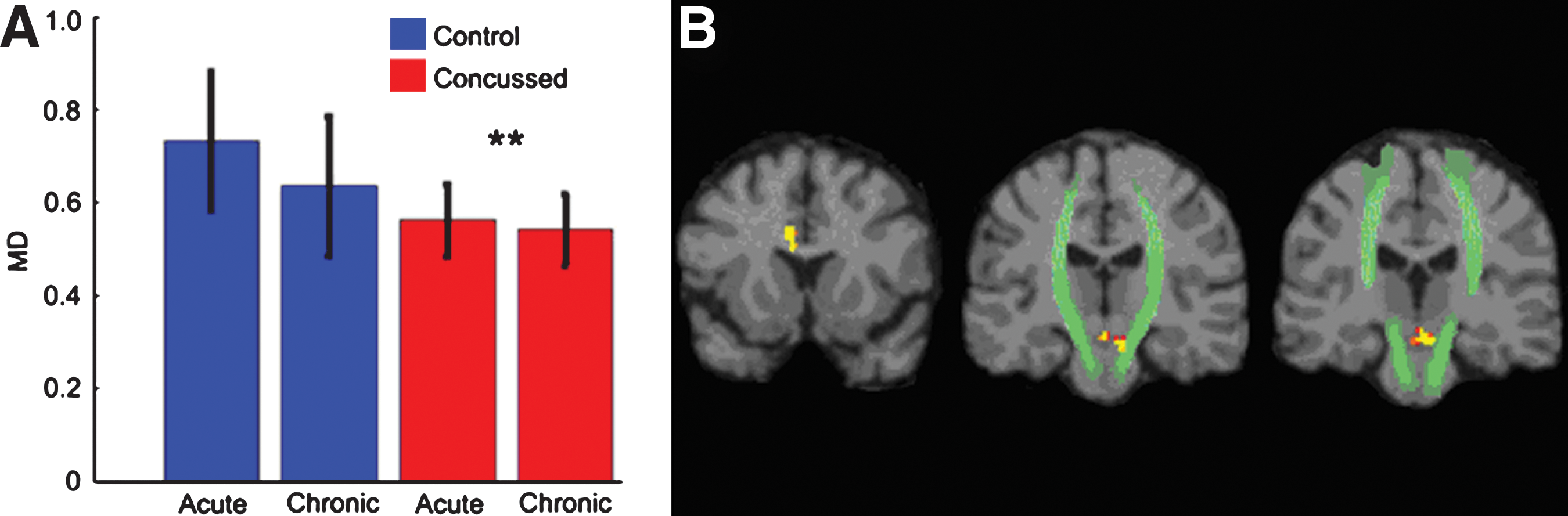
Differences in mean diffusivity (MD) between control and concussed athletes. (
Concussed athletes compared to the control mean FA in brain regions showing significant differences at the group level and their opposite hemisphere homologues. The structure was noted as damaged if the FA was 2.5 standard deviations greater than the average FA of 8 healthy control subjects in either hemisphere. The total number of subjects showing FA below which a structure was considered to have a traumatic axonal injury lesion is listed in the final row. The final column shows the number of structures in which each subject showed altered FA values at either time point (T1=acute phase, T2=chronic phase). The adjoining two columns depict the total number of symptoms reported at the time of the first scan, and the number of total concussions sustained according to self-report, respectively.
CST, corticospinal tract.
Concussed athletes compared to the control MD mean in brain regions showing significant differences at the group level. No opposite hemisphere homologues were added, as the regions are either midline (corpus callosum), or spanned each hemisphere (right and left CST). The structure was noted as damaged if the MD was 2.5 standard deviations less than the average MD of 8 healthy control subjects in either hemisphere. The total number of subjects showing MD above which a structure was considered to have a traumatic axonal injury lesion is listed in the final row (T1=acute phase, T2=chronic phase). Only areas within the corpus callosum showed MD differences at the individual level.
CST, corticospinal tract.
Results of the individual analyses show that while every concussed athlete showed increased FA in at least one area, some athletes were more affected than others, according to the number of clusters affected. Also, more concussed athletes had elevated FA at the second cluster along the CST (nearest the corpus callosum) at both time points. Though non-significant at the group level, some athletes appear to also have elevated levels along the right CST. Such different findings at the individual level further underscore that while the biomechanical mechanisms do bear similarities between individuals, there are also differences that are lost in group-based analyses. One-way ANOVAs were conducted to investigate whether the number of regions showing alterations differed according to either the number of reported symptoms, or the total number of concussions reported. The number of regions showing elevated FA levels did not differ with respect to the total symptom score [F(2,13)=1.072, p=0.484]. However, the number of regions showing elevated FA values differed significantly according to the number of concussions reported [F(2,13)=6.95, p=0.009; Fig. 5]. Further post-hoc analyses revealed that this effect was only significant in those subjects who had a history of three concussions (p=0.005), but not for those who reported one (p=0.804) or two (p=0.804) concussions. The individual analyses for MD did not reveal any significant differences between the control group and the concussed athletes along the CST. However, within the corpus callosum concussed individuals did show elevated MD. Furthermore, one-way ANOVAs between the total symptoms reported [F(2,13)=1.072, p=0.297], and the total number of concussions [F(2,13)=1.48, p=0.264] were not significant.
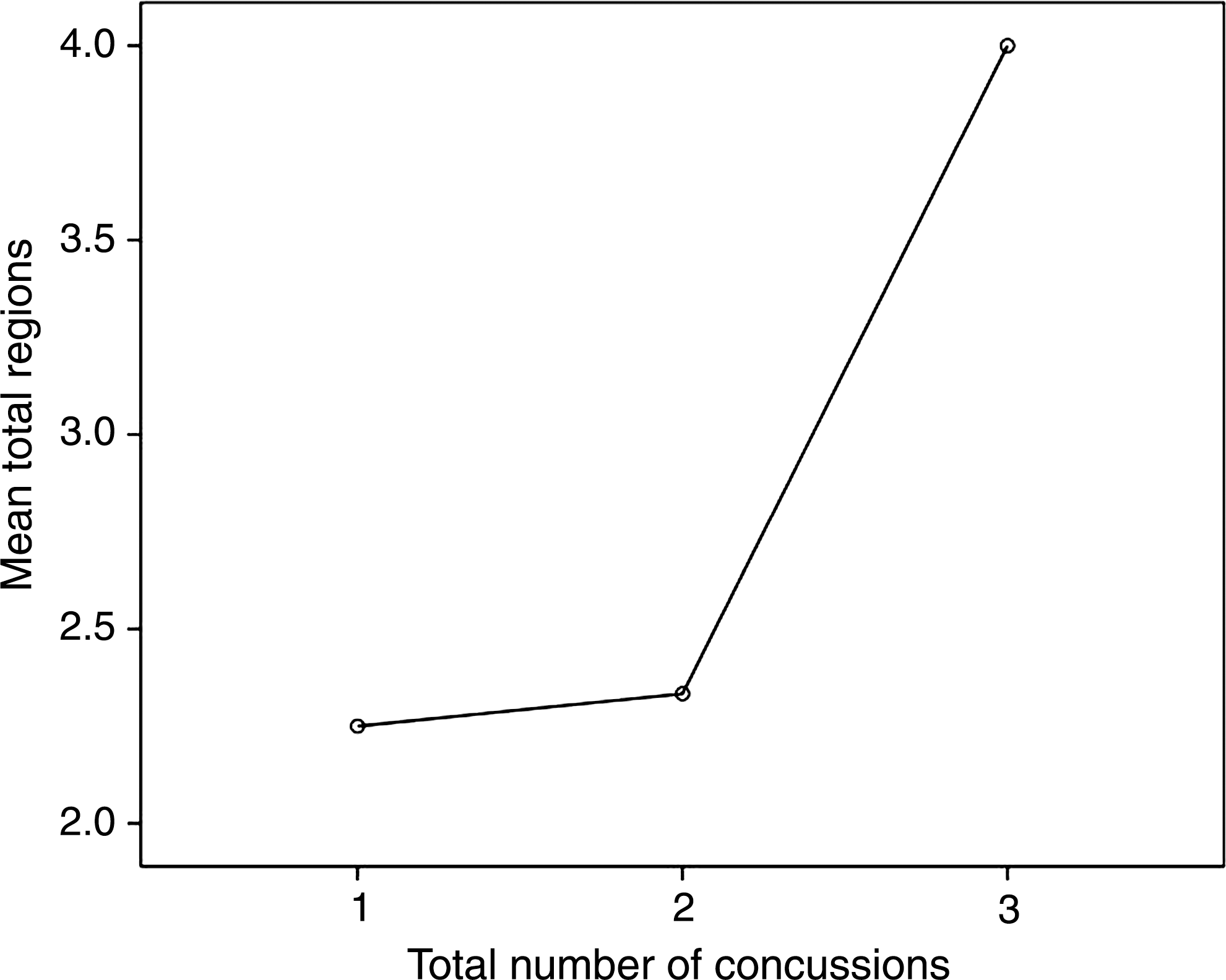
Plot demonstrating the relationship between the number of regions showing altered fractional anisotropy (FA) and the number of concussions reported by athletes in the concussed group. The analysis of variance demonstrates a significant difference between the number of concussions sustained and the number of damaged areas.
Discussion
We observed significantly higher FA and AD values and lower MD values along the CST and in the corpus callosum in concussed than in nonconcussed athletes at both the acute and chronic time points. Though there were some differences in the precise locations along the CSTs, there was continuity in terms of where in the coronal plane the differences were observed. Specifically, the WM underlying the primary motor and primary sensory cortical areas exhibited the most damage. Similarly, the corpus callosum showed alterations in areas thought to be connected to premotor and motor areas (Hofer and Frahm, 2006). Our results are consistent with those of other studies that employed DTI in the investigation of mTBI (Chu et al., 2010; Mayer et al., 2010; Wilde et al., 2008), in that in the current study we found anisotropic changes. As in previous studies, we found the corpus callosum to be affected by TAI; furthermore, the current study identified the CST as being particularly vulnerable.
In the current study we found consistently increased FA values in concussed athletes in both the acute and chronic post-injury phases. Most studies report the inverse, citing disruption to the organizational structure of the tissue, axonal degeneration, and demyelination as pathological hallmarks of TBI (Arfanakis et al., 2002; Kumar et al., 2009; Miles et al., 2008; Newcombe et al., 2007,2008; Wilde et al., 2010; Wozniak and Lim, 2006; Wozniak et al., 2007). However, all of the aforementioned studies with two exceptions (Miles et al., 2008; Wozniak et al., 2007) included mixed TBI samples, for which the decrease in FA was thought to stem from wallerian degeneration and subsequent massive cell loss (Arfanakis et al., 2002; Wilde et al., 2010; Wozniak and Lim, 2006). The seemingly contrary increase in FA is thought instead to be reflective of subtle cytotoxic edema and a localized inflammatory response due to compressed intracellular space along the CST and corpus callosum, and is more reflective of milder injuries. The subsequent restriction of diffusion then results in increased directionality of the fibers. These results are consistent with other studies in which mTBI was studied exclusively (Chu et al., 2010; Mayer et al., 2010; Wilde et al., 2008).Within the chronic phase, we also report persistently elevated FA values, which may still be characterized by volume loss and myelin degeneration (Bigler, 1999; Meythaler et al., 2001). Such an interpretation may also seem counterintuitive, as increasing the interstitial space between cells is thought to decrease anisotropy. However, a loss of crossing fibers could result in increased anisotropy (Pfefferbaum and Sullivan, 2003), potentially accounting for the increased FA seen in the chronic phase. Suffice it to say that the increased FA values observed in the acute phase and those observed in the chronic phase may have the same net result, but result from different processes (Hurley et al., 2004).
AD quantifies the diffusion along the axon parallel to the predominant fiber orientation. Increases in AD are thought to be reflective of damage to the axon itself, as opposed to radial diffusivity, which is thought to measure damage to the myelin (Song et al., 2002). The acceleration and deceleration forces that characterize concussion cause defects to myelin lamellae and axolemmas, which results in axonal swelling with the release of large amounts of Ca2+ (Buki and Povlishock, 2006; Maxwell et al., 1988), consistent with what is known about the metabolic cascade that follows a concussive blow (Giza and Hovda, 2001). The fact that AD is not reduced may in fact be an encouraging sign, as a decrease is thought to reflect a structural change to the axon (axotomy), whereas an increase may simply mean that while there is swelling, the axonal structure, though affected, is more or less intact (Newcombe et al., 2007). To that end, the AD and FA values may still normalize over the course of 2–13 months (Chappell et al., 2006), well inside the 6-month time frame employed in the current study.
MD is the average molecular diffusion and is thought to be affected by cellular size and integrity (Pierpaoli et al., 1996; Toga and Mazziotta, 2002). Overall, the literature points to cytotoxic edema and inflammation due to homeostatic membrane dysfunction. There is also some evidence that damaged neurons may potentially repair their damaged membranes, rather than progressing to axotomy (Farkas et al., 2006). Other researchers investigating ischemic brain injury have speculated that decreased MD values in conjunction with elevated FA values reflect basic alterations in cerebral microstructure (Bhagat et al., 2006; Green et al., 2002). The metabolic changes observed in concussion (Giza and Hovda, 2001; Henry et al., 2010) support the notion that both membrane dysfunction and altered microstructure are driving the lowered MD values seen in the current study. This corresponds well with the current study's findings, for which apparent cellular edema normalizes in the chronic post-injury phase, as cellular edema is thought to be an acute phenomenon (Chu et al., 2010; Wilde et al., 2008).
The results of the individual analyses support the group findings. The clusters along the CST were greater than 2.5 standard deviations above the mean of the control group in the majority of the concussed athletes, with the exception of the dorsal-most cluster (left CST cluster 1). Perhaps most clinically relevant, the number of affected regions was significantly higher in athletes who sustained three concussions than in athletes who had only one or two concussions. Such a finding, though certainly preliminary, adds to the ever-growing body of evidence about the deleterious effects of multiple concussions (Bruce and Echemendia, 2009; De Beaumont et al., 2007a; Gaetz et al., 2000; Guskiewicz et al., 2003; Theriault et al., 2010).
Magnetic resonance spectroscopy (MRS) captures unique information about WM pathology through the detection and quantitation of several brain metabolites in vivo. We, along with others, have previously reported metabolic alterations in the primary motor cortex in the acute phase (Henry et al., 2010; Vagnozzi et al., 2008), as well as in the chronic phase (Henry et al., submitted). The metabolic results support the DTI results with remarkable consistency, as the MR regions of interest were seen in the CSTs underlying the motor cortex, precisely where the diffusion changes were manifesting FA and AD abnormalities. The acutely and chronically diminished concentrations of N-acetylaspartate (NAA; Henry et al., submitted), and increased phosphocreatine (Gasparovic et al., 2009) concentrations, are related to disrupted consumption and production of ATP in the injured neuron to regain homeostatic equilibrium and repair (Giza and Hovda, 2001; Henry et al., 2010; Vagnozzi et al., 2008). It is possible that the restorative metabolic process results in increased intracellular water retention (Mayer et al., 2010). Such a hypothesis is confirmed by looking at cellular mechanisms of osmotic regulation at different time points after injury. While ions are called upon to regulate osmotic pressure in the acute phase (Lang et al., 1998; Strange, 1992), other metabolites that do not alter the electrophysiological balance of the cell like myoinositol are called upon to regulate the osmotic pressure over the long term (Lang et al., 1998). Such a metabolic alteration would fit with the current study's DTI findings, for which MD is decreased due to cellular edema in the acute phase, and through metabolic alteration in the chronic phase. In other words, the mechanisms of osmotic regulation seen after sustaining a concussion, though different between the acute and chronic phases, may underlie the initial and continued alterations in MD. Transcranial magnetic stimulation (TMS) studies have demonstrated chronic subclinical motor system dysfunction specific to intracortical inhibition, which was exacerbated in young athletes who had suffered more severe and/or multiple injuries (De Beaumont et al., 2007b). More alarmingly, similar anomalies were found in retired athletes, who were decades removed from their last concussion (De Beaumont et al., 2009). In another study, de Beaumont and colleagues found the same intracortical inhibition problems in concussed athletes, in addition to neurophysiological and behavioral markers of subclinical motor dysfunction (De Beaumont et al., accepted). The exact link between the current study's DTI findings and the motor system dysfunction documented using TMS is not clear, but the fact that both point to the motor cortex and the underlying CST indicate that this brain area is particularly vulnerable.
The current study is not without limitations. Because mTBI is such a diffuse and heterogeneous injury, a VBA approach may lack the sensitivity to identify all alterations, because only those injured brain areas that are common to the experimental group will be detected. Likewise, from a clinical standpoint, it has not been established that VBA has enough statistical power for legitimate single-subject analysis. From a technical standpoint, VBA requires spatial normalization, which can introduce error if it is inaccurate, leading to false-positive results due to poor alignment (Shen et al., 2007). Also, because VBA requires spatial smoothing to allow each subject's brain to fit into a common space, there is further loss of sensitivity, leaving only changes in large tracts detectable. However, employing a VBA approach provides certain advantages. For example, VBA is fully automated, data-driven, and ideal for group-based analyses. Furthermore, VBA does not require a priori hypotheses about where changes in the brain might be occurring, and it can be used in an exploratory fashion whereby the whole brain can be examined, which is important in mTBI due to the heterogeneity of the injuries.
Overall, the results of the current study suggest that there is WM damage after a sports concussion in the acute and chronic post-injury phases, in the form of increased FA and AD values and decreased MD values, primarily along the CST, and to a lesser extent in the corpus callosum. These results are consistent with those of other studies that have investigated WM changes after mTBI (Chu et al., 2010; Mayer et al., 2010; Wilde et al., 2008), but are contrary to TBI studies showing decreased FA and increased MD (Arfanakis et al., 2002; Kumar et al., 2009; Miles et al., 2008; Newcombe et al., 2007,2008; Wilde et al., 2010; Wozniak and Lim, 2006; Wozniak et al., 2007), which may be due to the use of more severely injured participants, different imaging techniques, and the different time intervals used in these studies. Regardless of the nature of the findings, the emerging pattern of findings demonstrates WM injury after mTBI, including sports concussions, as demonstrated in the current study. The precise nature of the ensuing pathology must be further documented to better understand the time course of WM damage, and the possibility of recovery after a concussion. Future research should also concentrate on delineating the nature of diffusion changes resulting from moderate and severe TBI versus more mild injuries, as there appears to be different processes at work that are not explained by the degree of injury severity.
Footnotes
Author Disclosure Statement
No competing financial interests exist.