
Abstract
Rhino- and/or otoliquorrhea can be diagnosed by detecting beta-trace protein (β-TP) in nasal or ear secretions, as β-TP is found in high concentrations in cerebrospinal fluid (CSF) but not in serum. CSF fistulae following trauma or surgery can also occur at other anatomical sites, resulting in CSF leakage into the thoracic and abdominal cavities. By analogy, determination of ß-TP has also been used to diagnose CSF admixture in pleural effusions and ascites. However, no systematic study has yet evaluated the concentrations of β-TP in such fluids in the absence of CSF. To determine the validity of β-TP determination as a marker for the presence of CSF, we investigated β-TP concentrations in pleural effusions and ascites without CSF admixture. Patients from whom samples of ascites or pleural effusion and a paired plasma sample were available were investigated. One hundred sixty-four patients were prospectively recruited. ß-TP concentrations were determined by nephelometry. Mass spectrometric proteome analysis confirmed the presence of ß-TP in the samples. Median β-TP concentrations detected in ascites and pleural effusions (range, 0.014–26.5 mg/L, median 2.29 mg/L) exceeded the corresponding plasma concentrations 2.6-fold. According to cutoffs published to diagnose rhino- and otoliquorrhea, between 6.1% and 95.7% of the specimens would have been erroneously rated CSF-positive. Protein analysis confirmed the presence of β-TP in pleural effusion and ascites. Ascites and pleural effusion contain high concentrations of β-TP that exceed the levels in corresponding plasma. Therefore, β-TP is not a specific marker for the presence of CSF in these fluids.
Introduction
T
Beta-trace protein (β-TP), which has been identified as a lipocalin-like prostaglandin D synthase, is an abundant protein in CSF, but is present only at low levels in serum (Melegos et al., 1996) Impaired renal function results in an accumulation of β-TP in sera. Within the nervous system, β-TP is predominantly secreted by the choroid plexus and arachnoid trabecular cells (Blodorn, et al., 1996; Hoffmann, et al., 1993; Melegos et al., 1999).
Despite the consensus that nephelometric measurement of β-TP is suitable to detect CSF fistulae in rhino- and otoliquorrhea, a wide range of thresholds (from 0.35 to 6.0mg/L) has been reported (Arrer et al., 2002; Bachmann et al., 2002; Reiber et al., 2003; Risch et al., 2005; Schnabel et al., 2004). Others have suggested a concurrent determination of β-TP in serum to calculate a β-TP fluid/serum ratio (Kleine et al., 2000; Risch et al., 2005). β-TP has also been used as a marker to diagnose CSF fistulae at other anatomical sites, such as pleural effusions or ascites (Born et al., 2008). However, so far no study has systematically investigated the concentration of β-TP in these fluids. The current study was performed to test the hypothesis that the diagnostic approach used to identify CSF admixture in rhino- and otoliquorrhea could be extended to ascites and pleural effusions.
Methods
The study was performed prospectively from November 2007 to June 2008. All patients provided their fully informed written consent. The study was approved by the local ethics committee. Ascites, pleural effusion, the wound secretion from an extremity, and the aspirate of a thyroid cyst were obtained through percutaneous tap or sampling from drainage tubes. Specimens sent to the central laboratory were included consecutively if a paired plasma sample obtained on the same day was available. In addition, patient charts had to be reviewable to identify each patient's age, gender, concurrent diseases, and underlying cause of pathological fluid. Only the first sample obtained from each patient during the study period was included in the study.
β-TP was measured using the Prospec nephelometer and the N Latex β-TP® test (Siemens Diagnostics); the concentration of β-TP was calculated by Behring Nephelometer Analyzer software. All samples were centrifuged at 14,000×g for 10 min before β-TP measurement. Viscous secretions were diluted 1:100 with N dilution buffer®. Precision was monitored using N/T protein Control LC® (Siemens). The range for reliable measurements was 0.1–19.6 mg/L; the interassay coefficient of variation was<5.7%. The systematic deviation was from +1.9% to +4.75%. All samples were analyzed in duplicate.
Because routine blood analysis in the clinical laboratory is implemented in plasma, a pre-test comparing β-TP concentrations in 30 paired plasma and serum samples was performed. The pre-test revealed no differences (mean serum value, 0.54 [range, 0.22–1.56]; mean plasma value, 0.57 [range, 0.27–1.58]; difference of means: p=0.34).
Total protein concentration and β-TP were measured in the pathological body fluids. β-TP, creatinine, and C-reactive protein (CRP) were quantified in the paired plasma samples. Total protein in the specimens was measured using the modified biuret method (Dimension RxL Max HM Clinical Chemistry System autoanalyzer, Siemens Diagnostics), creatinine was measured using the Jaffé kinetic method (Dimension RxL Max HM Clinical Chemistry System autoanalyzer, Siemens Diagnostics), and CRP was measured using the turbidometric immunoassay (Dimension RxL Max HM Clinical Chemistry System autoanalyzer, Siemens Diagnostics).
Proteome analysis
Two-dimensional (2D) gel electrophoresis and mass spectrometric peptide mass fingerprinting were performed as described. Briefly, after fractionated precipitation (Pecks et al., 2010), the total volume of the re-dissolved proteins from fraction IV was loaded onto a strip for isoelectric focusing (IEF) (Sinz et al., 2002). The first dimension, IEF, was conducted on 7-cm Immobiline Dry strips (pH 4-7; GE Healthcare/Amersham Biosciences, Freiburg, Germany) in an IPGphor system (GE Healthcare/Amersham Biosciences, Freiburg, Germany); focusing was completed when 8000 Vh were reached. Subsequently, strips were equilibrated twice (15 min each) in 5 mL equilibration buffer (50 mM Tris-HCl pH 8.8; 6M urea; 30% glycerol; 2% sodium dodecyl sulfate [SDS]) supplemented with 1% (w/v) dithiothreitol and 4% (w/v) iodoacetamide. For the second dimension, SDS polyacrylamide gels (12% t) were run for 1 h at 150 V in a Mini-PROTEAN 3 Dodeca Cell Vertical Electrophoresis System (BioRad, München, Germany) while applying the Laemmli continuous buffer system. Gels were fixed and stained with colloidal Coomassie Brillant Blue G-250. Stained gels were scanned with the Umax Mirage II Scanner (Umax Data Systems, Willich, Germany). The Progenesis PG200, version 2006 (Nonlinear Dynamics Ltd, Newcastle upon Tyne, UK) was used for image analysis. Protein spots of interest were excised manually. Excised gel plugs were subjected to in-gel digestion with trypsin (Promega, Madison, WI). A sample preparation of the peptide mixture was placed on an AnchorChipTM 600/384 target plate (Bruker Daltonik, Bremen, Germany) using α-cyano-4-hydroxycinnamic acid as matrix. Peptide mixtures were analyzed with a Reflex III matrix-assisted laser desorption/ionization-time of flight-mass spectrometer (MALDI-TOF-MS) (Bruker Daltonik, Bremen, Germany), which was equipped with the SCOUT source and delayed extraction and operated in positive ion mode using an acceleration voltage of 20 kV. Mass spectra were further processed and analyzed with FlexAnalysis 2.4 and BioTools 3.0 software (Bruker Daltonik, Bremen, Germany). Database searches were performed against an in-house SWALL database, which consists of Swiss-Prot release 56.8 and TrEMBL release 39.8, using Mascot version 2.2.03 software (Matrix Science, London, UK) (Kienbaum et al., 2009).
Statistical analysis
Statistical analysis was performed with SAS version 9.1 software (SAS Institute Inc., Cary, NC). Means were compared with the Wilcoxon two-sample test, and medians were compared with the median two-sample test. Categorical data were analyzed with the χ2 statistic. Spearman rank-sum correlation was used for continuous variables. A p-value <0.05 was considered statistically significant.
Results
None of the recruited patients were suspected of having a CSF fistula or were hospitalized for trauma of the spine. One hundred sixty-four patients were included: 83 received taps of the abdominal cavity, and 81 received taps of the pleural cavity. The mean age was 69.3 years (range, 24–93 years) and 63% of the cohort were male. β-TP was detectable in all fluid samples; the β-TP concentration ranged from 0.014 to 26.5 mg/L (median 2.29 mg/L). In plasma, β-TP concentrations ranged from 0.64 to 21.4 mg/L (median 0.88 mg/L). In all but 25 samples, β-TP levels exceeded the corresponding plasma level. The median concentration in the pathological fluids was 2.6-fold the concentration of β-TP in the plasma samples (Table 1).
As expected, there was an overall linear association between β-TP plasma concentrations and plasma creatinine (r=0.86, p<0.0001). When the thresholds from the literature for CSF detection in rhino- and otoliquorrhea were applied to the samples in this study, a significant percentage of false positive results occurred (Table 2).
The wound secretion from a tibia and the fluid of a thyroid gland cyst also contained high concentrations of β-TP (1.61 mg/L and 3.9 mg/L, respectively), which exceeded the corresponding plasma levels.
To test whether β-TP detected by nephelometry could reflect nonspecific values caused by antibody cross-reactivity, 2D gel electrophoresis with subsequent mass spectrometry was performed. This analysis confirmed the presence of β-TP in our fluid samples (Fig. 1).
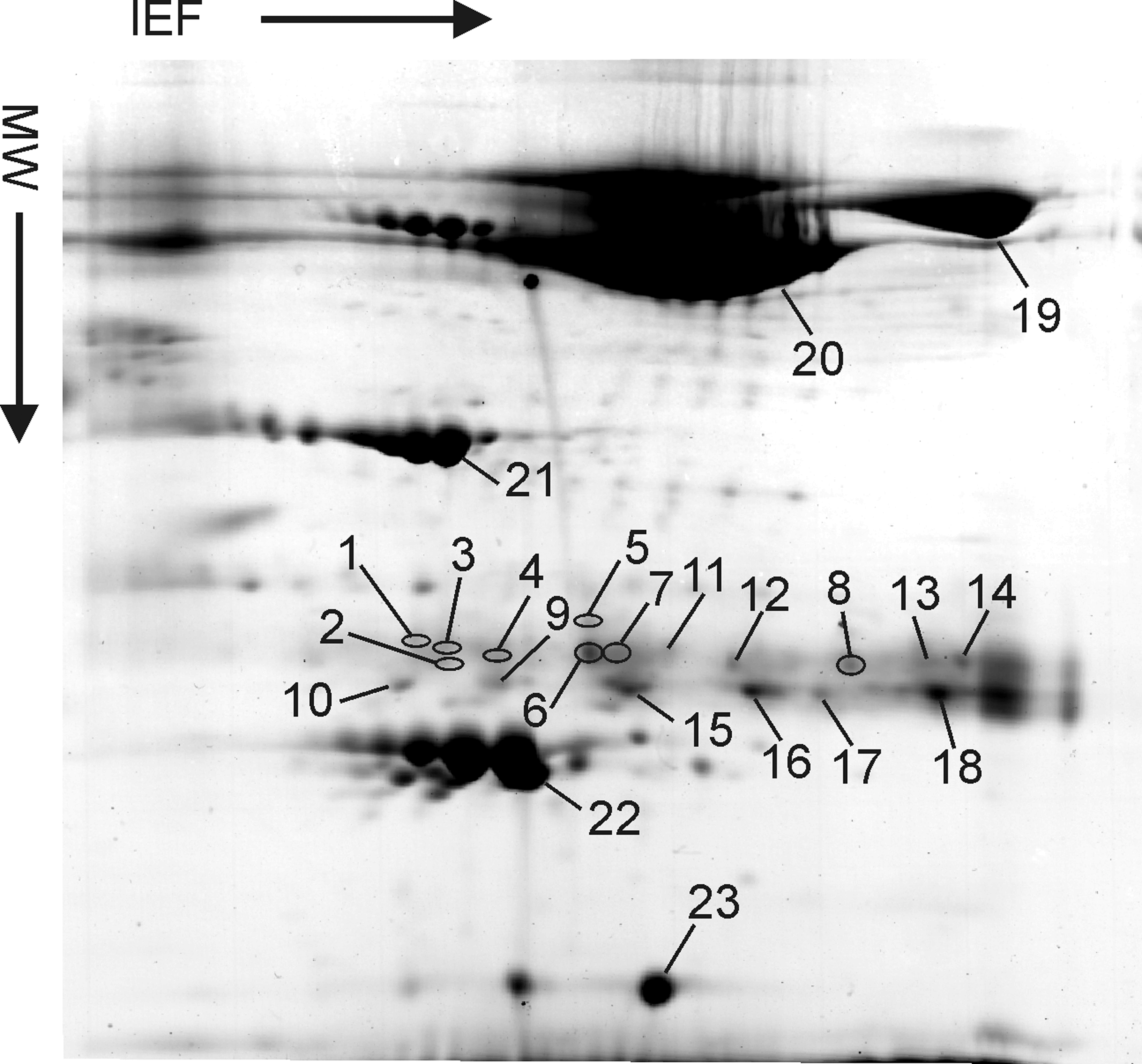
Two-dimensional gel image of proteins from an ascites sample after fractionated precipitation. Circled spots (spots 1–8) contain ß-TP (prostaglandin-H2 D-isomerase; UniProt accession number: P41222). Other spots in the vicinity (spots 9–18) are derived from immunoglobulin light chains, λ chains (e.g., Q6PJA3), and κ chains (e.g., Q8NEK0). For orientation, locations of serotransferrin (spot 19; P02787), serum albumin (spot 20; P02768), apolipoprotein A-IV (spot 21; P06727), apolipoprotein A-I (spot 22; P06727), and transthyretin (spot 23; P02766) are indicated. IEF: pH 4-7 (left to right). SDS-PAGE molecular weight (MW) separation: approximately. 110–10 kDa (top to bottom). Colloidal Coomassie Blue staining.
We conducted a multiple regression analysis that included the following parameters: fluid β-TP, fluid total protein, plasma β-TP, plasma CRP, and plasma creatinine. The analysis revealed a correlation between β-TP concentrations in plasma and pathological fluids (p<0.001, r=0.54, β=0.99). There was no correlation of total protein with β-TP concentration in the body fluid.
Discussion
This study is the first to systematically investigate whether nephelometric measurement of β-TP in fluids derived from the abdominal or thoracic cavity is suitable to detect CSF admixtures resulting from a CSF fistula. Our data demonstrate that this approach will result in a high proportion of false positive results. In patients without any suspicion of CSF fistula, the majority of samples obtained from the abdominal and pleural cavities contained β-TP concentrations that exceeded the corresponding plasma level. These data are in contrast to the findings with respect to nasal or otogenic secretion, in which several studies have demonstrated that β-TP is a highly specific and sensitive assay with which to detect liquorrhea (Bachmann and Petereit, 2004; Deisenhammer et al., 2009; Melegos et al., 1996). 2D gel electrophoresis and mass spectrometry were used to confirm the identity of the protein detected in ascites and pleural effusion, thereby ruling out that the high concentrations of β-TP in ascites and pleural effusion observed in the nephelometric assay were solely caused by cross-reacting proteins. Although the source of β-TP in the fluids remains unknown, it is of interest that the β-TP levels in ascites and pleural effusion correlate with renal impairment, as has been previously demonstrated for plasma β-TP concentrations (Melegos et al., 1999).
We are aware of the limitations of the current study. Because no samples from patients with confirmed CSF leakage were available as a positive control, we cannot provide data regarding the sensitivity and specificity of β-TP concentrations in ascites or pleural effusions to detect such fistulas. Nevertheless, our data suggest that the use of β-TP as a diagnostic marker for CSF fistulas should remain limited to nasal and otogenic secretions. The diagnosis of CSF fistulae in other locations requires support by other methods, such as radionuclide tracing studies or imaging methods.
Footnotes
Acknowledgments
We thank Uwe K Zettl for his helpful comments and Mrs. Weihrauch and Mrs. Schmidt for their contributions during data collection.
Author Disclosure Statement
No competing financial interests exist.