
Abstract
Traumatic spinal cord injuries (SCI) are rare but extremely costly. In order to improve the modelling of inclusion criteria for studies of SCI it is necessary to determine what epidemiological trends affect SCI.
Using the Rhone Registry, which contains all the casualties resulting from road crashes in the Rhône département of France and codes their injuries using the Abbreviated Injury Scale (AIS), we describe the epidemiological trends that affect spinal cord injury (SCI), major spinal trauma (MST) and severe injuries (AIS4+) to other body regions between two periods 1996–2001 and 2003–2008.
Although there has been a marked decrease (35%) in the incidence of casualties after a road traffic crash, and reductions of 22% in the incidence of MST and 33% in that of severe injuries (AIS4+) (p<0.001), for SCI the incidence rate and number of casualties have remained surprisingly stable. In the second period, there was no change in the incidence of SCI resulting from road traffic crashes, nor in the associated fatality, mortality and survival rates. The incidence for car users was significantly lower in the second period. This contrasts with the incidences for motorcyclists and for the group including pedestrians and cyclists which were respectively 47% and 77% higher in the second period. The median age of the casualties, the age-adjusted incidence of SCI and the number of associated injuries were also higher in the second period.
We have observed a marked reduction in the incidence of road trauma including the most severe injuries, but not SCI. The higher proportion of motorcyclists, the increase in the age of casualties and the greater presence of multiple injuries are new factors in the epidemiology of SCI after a road crash.
Introduction
T
However, in order to improve prevention and patient care, including the use of new therapies, it is crucial to be able to describe the trends affecting the incidence of SCI (O'Connor 2005; Pirouzmand 2010) and the survival of patients with the condition (DeVivo et al., 1999; Catz et al., 2002; van den Berg et al., 2010). This would make it possible to avoid overestimating the number of cases that could be included in future studies. The main goal of this observational study was to describe the trends that affect spinal cord injuries resulting from road crashes using the data in the Rhône Road Trauma Registry. To do this, we compared two six year observation periods with a gap between them (1996–2001 and 2003–2008). Very surprisingly, in spite of the extremely significant drop in road trauma, particularly in terms of the 35% fall in the number of casualties with the most severe injuries, there has been no change in the incidence and mortality of SCI.
Material
The Rhône Registry has been described elsewhere (Lieutaud et al., 2010; Laumon et al., 1997). Briefly, it covers the Rhône département (1.6 million inhabitants) and has been approved by the health authorities (Comité National des Registres) and the National Commission for Information Technology and Civil Liberties (CNIL) (Lieutaud et al., 2010). The Registry, which is funded by public grants, contains the demographic characteristics of each casualty as well as the features of the accident (type of road users, location, date, time of day), and a description of the injuries sustained. The inclusion criterion is a road traffic accident involving at least one vehicle, motorized or not, occurring in the Rhône département and requiring health care activity. Inclusion of a casualty in the Registry is the result of the cooperation of 245 healthcare structures which administer care to road traffic casualties. The collaboration of primary care teams and forensic medicine institutes means that the Rhône Registry also includes casualties who die at the scene of the accident. All the injuries were coded by the same doctor (Amina Ndiaya) using the Abbreviated Injury Scale (AIS version 90) (Association for the Advancement of Automotive Medicine, 1990).
“The AIS was developed to provide researchers with a simple numerical method of ranking and comparing injuries by severity, and to standardize the terminology used to describe injuries. First, the AIS is based on anatomical injuries which distinguishes it from other systems that depend on physiological parameters. Second, the AIS assigns scores to injuries and not the consequences of the injuries.
The AIS scale is a consensus-derived anatomically based system that classifies individual injuries by body region on a 6-point ordinary severity scale ranging from AIS 1 (minor) to AIS 6 (currently untreatable). Empirical data show that the AIS correlates with the probability of death for AIS ≥3. The Maximum AIS (MAIS), which is the highest single AIS code in a patient with multiple injuries, has been used to describe overall severity.
The Injury Severity Score (ISS) is the sum of the squares of the highest AIS scores for three different body regions. The ISS gives a much better fit between overall severity and the probability of survival.
Injuries are described as follows: R=body region (R=6 means the Spine) T=Type of anatomic structure (T=4 means the spinal cord, T=5 means the vertebras and disks) S=Specific anatomic structure (S=02, 04, 06 mean the cervical, thoracic and lumbar spine respectively).
In the present study, Major Spinal Trauma (MST) was defined on the basis of (R=6, T=4 or 5, AIS ≥2) and included spinal luxations and/or fractures and/or spinal cord injuries. This excluded minor spinal trauma without radiological signs of trauma (by either plain film, CT or magnetic resonance imaging) and isolated nerve root injuries with no fracture or dislocation. Spinal cord injuries were defined as injuries resulting in permanent neurological deficit: R=6, T=4, AIS≥4. Any other injured body regions were described for AIS ≥4 injuries.
Temporary paraparesia or tetraparesia (coded AIS=3) were not included in the study. In the case of casualties with a persistent complete deficit, cervical SCI was coded AIS 5 and thoracic or lumbar SCI was coded AIS 4.
All the patients in the Registry with SCI also had MST. The AIS cannot differentiate between different levels of incomplete neurological deficit. That is to say that no distinction was made between classes B, C, D of the American Spinal Injury Association/International Spinal Cord Society neurological standard scale, all of them being included in the AIS 4 score.
Road users were categorized as car occupants, motorcyclists (which includes the users of any motorized two wheeled vehicle), cyclists, pedestrians, truck occupants, bus occupants and others (in-line skaters, roller-skaters, and quad bike user).
This study is based on a registry that covers this fairly urbanized area of France between 1 January 1996 and 31 December 2008. We used the January 2011 safeguard of the Registry. The study period was divided into two six-year-periods, 1996–2001 and 2003–2008. The study avoided 2002 because, in that year, the incidence of road traumas was intermediate between two relatively homogeneous periods.
Statistical Analysis
With regard to the first goal of this study, we calculated the incidence and fatality rates of SCI during the periods 1996–2001 and 2003–2008. Adjustment for age was performed on the basis of the population of the Rhône Département in 2002, which is the median year of the period under study. In a post hoc analysis, we then determined the road user types involved and the other injuries that were significantly linked to SCI during each period. Statistical analysis was performed using the SAS software. P<0.05 was deemed to be significant.
Results
Incidence and mortality rates
Although there has been a marked decrease (35%) in the incidence of casualties after a road traffic crash and reductions of 22% in the incidence of MST and 33% in that of the most severe injuries (AIS4+) (p<0.001), in the case of SCI, the incidence rate and number of casualties has remained surprisingly stable (Table 1).
Although the population was higher in the second period, the numbers and incidences of casualties, particularly for the most severe injuries (AIS4+) and major spinal trauma, decreased significantly but the numbers and incidences of spinal cord injury remained constant.
Spinal cord injuries accounted for a percentage of the most severe injuries that rose from 5.5% to 7.8%, but this difference does not achieve significance due to the small number of AIS 4+ spinal cord injuries.
Between the two periods, the mortality of SCI casualties and the number who deceased during prehospital and intrahospital care did not change, while the number and the mortality of the most severely injured road crash casualties (AIS4+) decreased significantly (Table 2). Consequently, the number of crash survivors with SCI fell.
With regard to spinal cord injury sustained in a road crash, there was no significant change between the two periods in the incidence, the number of fatalities, the fatality rates, mortality rates, or survival rates.
The majority of fatalities occurred at the scene of the accident, although the proportion was significantly lower in the later period (respectively 32/34 vs 31/42, p=0.04).
Demographic data
The sex ratios in the two periods for all the casualties in the Registry were 1.6 and 1.7 respectively. The sex ratios were much higher in the case of SCI: 4.9 and 3.8 for the two periods, this reduction not being significant. As shown previously (Lieutaud et al., 2010), the sex ratio for SCI casualties increased in both periods with the severity of the injury and the use of a motorcycle or a bicycle (data not shown).
The mean age of the casualties with spinal cord injuries was significantly higher in the more recent period, rising from 32±16 to 38±17 years (p=0.04). However, this increase was observed only among survivors (mean age from 31±14 to 38±15 years, p=0.01) not fatalities, whose mean age did not change. Moreover, analysis of the distribution of age classes revealed a significant decrease in the second period in the number of casualties aged under 40 years while the number of casualties aged over 40 years increased (p=0.02). The drop was particularly marked for the youngest age group (under 10 years) and teenagers. (Figure 1A). The same phenomenon was observed for age-adjusted incidences (Figure 1B).

Level of injury
Although the number and incidence of casualties with major spinal trauma, which includes fractures and dislocation of the spine, decreased significantly for injuries at all levels (cervical thoracic or lumbar), there was no decrease in spinal cord injuries at the cervical level (+5%) (Table 3). Moreover, the proportion of cervical spinal cord injuries with complete neurological deficit was significantly higher in the more recent period (45/52) than in the earlier period (33/47) (p<0.05).
Characteristics of the accidents
Car users sustained significantly fewer SCI than other road users during the more recent period whatever their position in the car (driver or passenger) (p=0.01) (Figure 2). This result is also due to a 47% increase in SCI among motorcyclists (p=0.02) and a 77% increase in SCI among users of “green” modes, i.e. pedestrians and cyclists (p=0.04).
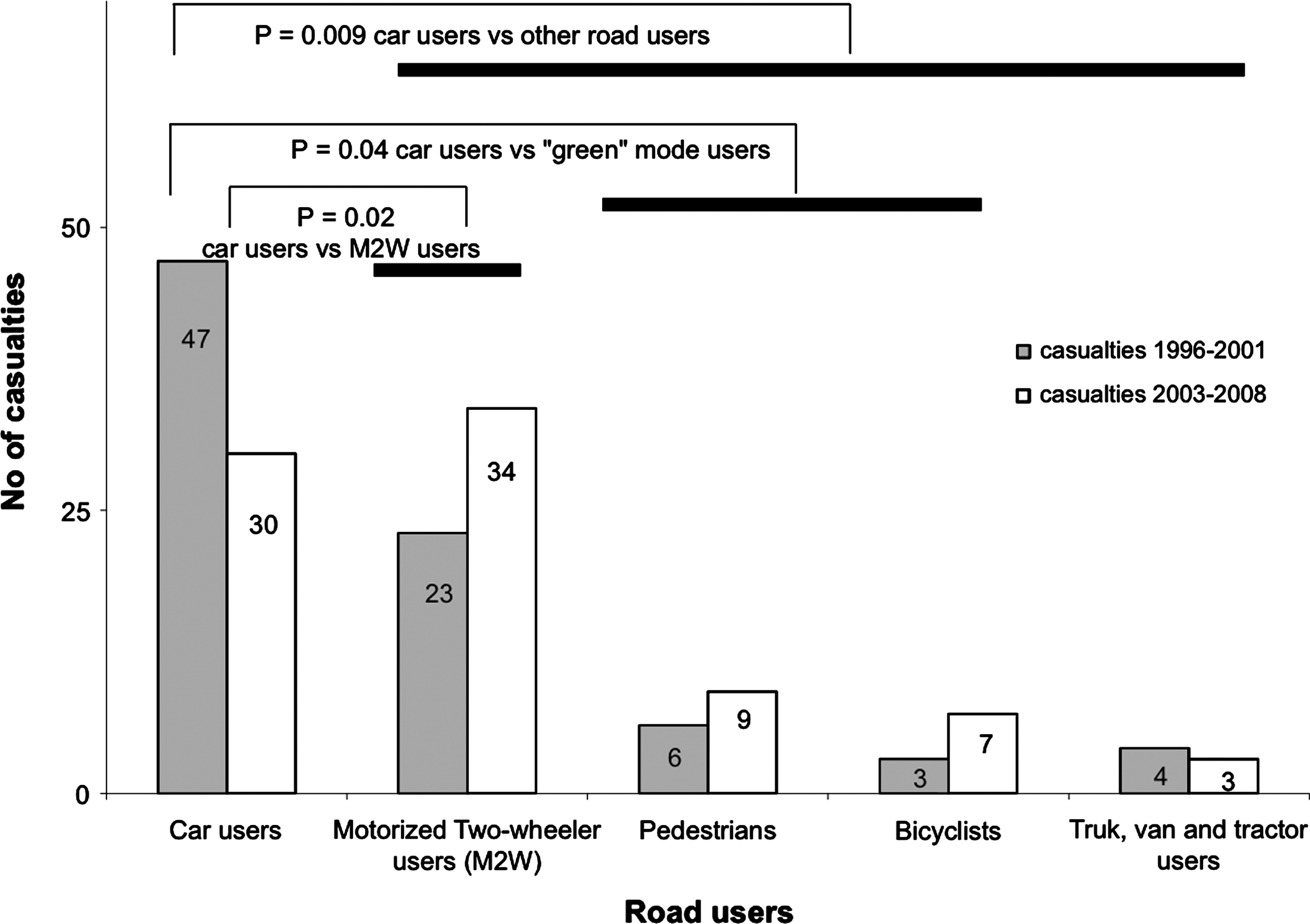
Distribution of types of road user among casualties with spinal cord injuries sustained in a road traffic accident in the two studied periods. There were significantly fewer car occupants in the more recent period but an increased number of motorcyclists (in particular), pedestrians and cyclists.
Regarding the type of journey, of the 87 casualties aged between 16 and 64 years for which information was available for both periods, 10 (12%) were injured in the course of a work-related journey. This rate was the same in both periods.
Spinal cord injury severity and other associated injuries (AIS4+)
A significant difference was apparent between the two periods with regard to the severity of the SCI, the age of the casualties, the injury severity score and the number of severe associated injuries for each body region. Although the ISS was lower, the age of the casualties and the number of associated injuries was higher in the second period.
The severity of the spinal injuries (MAIS spine score) was slightly but not significantly higher in the second period (Table 4). Among the SCI fatalities, there was a significant decrease in the median ISS score (p<0.001). Conversely, the ISS among survivors was higher in the second period, but not significantly so.
£ indicates statistically significant difference vs survivors in the period 1996–2001.
$ indicates a casualty may have injuries to several body regions.
MAIS, Maximum Abbreviated Injury Score; SD, Standard Deviation.
The number of body regions with severe (AIS4+) injuries associated with SCI was significantly higher (by 50%) in the later period and such injuries affected survivors more often than the deceased (p=0.007). The highest incidence was for thoracic injuries, which was significantly higher among survivors (p=0.006), followed by head injuries.
SCI among road users
There were fewer spinal cord injuries among car occupants in the second period, at all levels (cervical, thoracic, lumbar). In contrast, there were twice as many cervical injuries among the group including motorcyclists, pedestrians and cyclists (p=0.03) (Table 5).
Cervical injuries increased significantly among motorcyclists, cyclists and pedestrians.
Between the two periods, the numbers of casualties with severe injuries in other body regions increased from 8 to 22 motorcyclists and from 5 to 10 “green” mode users whereas they remained stable among car users (from 21 to 20).
To conduct a more detailed examination of motorcyclists, which was the subgroup which exhibited the greatest increase in the more recent period, we attempted to describe the body regions that sustained associated injuries at the time of the road crash. The motorcyclists sustained significantly more thoracic injuries (p=0.04) in the more recent period, and these increased in exactly the same proportion as fatalities (p=0.04) (Table 6). Similarly, the number of head injuries more than doubled in the more recent period, without achieving statistical significance.
The number of fatalities and individuals with severe injuries to the head or thorax was higher in the second period.
Discussion
This study set out to observe changes in the incidence of spinal and spinal cord trauma and the associated survival rates in a given geographical zone during a fairly short period after a road crash. Like Pirouzmand (2010), we found that the incidence not of only spinal trauma but of all trauma including the most severe, was lower in the more recent period. But, unlike that author, we did not find that this reduction was accompanied by a significant reduction in the incidence of spinal cord trauma. A large number of publications have described the changes in the survival of patients with an SCI, which, in developed countries, is not far from that of the general population (Catz et al., 2002; van den Berg et al., 2010). In a similar way, unlike Devivo et al., we found no improvement in immediate survival in the more recent period compared with the earlier one (DeVivo et al., 1999). This may be due to the fact that the research teams in question did not include SCI casualties who died soon after sustaining the injury who, in our view, represent almost 40% of the SCI casualties in the period 1997–2006 (Lieutaud et al., 2010), with this figure remaining almost the same (38%) in the more recent period between 2003 and 2008 described in this paper.
Change in the incidence and mortality of spinal and spinal cord trauma
Very surprisingly, and in marked contrast to the findings of Australian and American studies (O'Connor, 2005; DeVivo et al., 1999; Saunders et al., 2009; O'Connor and Brown, 2006), when we compared a recent six year period with another six year period very slightly before it, we were unable to demonstrate any change in the incidence of spinal cord trauma in spite of the fact that the incidence of severe AIS4+ injuries sustained in road crashes fell by 35%. A possible explanation for this is that O'Connor's findings related to two six year periods between 1986 and 1997 (O'Connor, 2005) while our study relates to a more recent period that takes in the very marked strengthening in 2002 of the legislation with a view to improving road safety. Similarly, and in contrast to the data published by most authors, the fact that our study also includes clinical data on the 40% of SCI casualties who died before arrival at hospital (Lieutaud et al., 2010) reveals that SCI mortality has been and is still underestimated and also remains stable over time. The survival rates reported by authors are consequently too high because inclusion in epidemiological studies is often based on hospital data which eliminates SCI casualties who died at the scene of the crash before the arrival of the emergency services or during the 24 hours immediately after injury (DeVivo et al., 1999; Ankarath et al., 2002). Some studies have applied exclusion criteria of 30 days after the injury, and sometimes even longer (O'Connor and Brown, 2006; Thurman et al, 1995; Tchvaloon et al., 2008; Lidal et al., 2007). There has, however, been no change in the early care administered to patients in our region in the two periods in question, involving prehospital medical care and immediate transfer of all cases to a trauma centre then to a neurosurgery department as soon as the patient's life-threatening injuries have been stabilized. Nevertheless, we still observed that slightly more than half the patients who were included in the second period died in the 30 days following the accident, which is very much higher than the rate of 4% to 16% reported among SCI patients observed during the acute phase (Ankarath et al., 2002; Kattail et al., 2009; Macias et al., 2009) and the 36% reported during observation studies conducted during rehabilitation and after (Lidal et al., 2007). In our study, even if the incidence of early death among SCI patients was non-significantly higher in the more recent period, the number of SCI patients who died at the scene before the arrival of the emergency services has tended to fall (31/32 vs 33/42; p=0.048). This is linked to a reduction in the severity of the injuries sustained by all the road crash casualties in the registry, in particular in the case of those with the most severe injuries (AIS4+) whose median ISS was lower in the second period, falling from 30 (IQ25–75: 21–45) to 26 (IQ25–75: 20–36) (p<0.001). However, when we make a comparison with other studies (O'Connor 2005), although the ratio between the number of SCI and the number of AIS4+ injuries is of the same order of magnitude (3‰ in the case of O'Connor and Brown, 2006 (O'Connor and Brown, 2006) vs 1.4‰ for the entire period covered by our study), we have not observed any improvement in the more recent period, and have even revealed a slight tendency for the situation to deteriorate as the ratio between the number of SCI and the number of AIS4+ injuries increased slightly from 1.3‰ in the period 1996–2001 to 1.6‰ in the more recent period. Similarly, we observed a ratio of SCI to MST of 1/12, which differs markedly from that observed by other authors (from 1/3 to 1/6) (Pirouzmand, 2010; Tchvaloon et al., 2008). However, our recruitment was complete and included patients with less severe spinal trauma than these two studies. The differences can be explained by the way Pirouzmand's study included only patients with an ISS of over 12, which applied to only 83% of our patients. In Baaj’ study, hospitalization was required, which was not necessarily the case for our patients. Thus, the selected populations in the various studies that deal with the ratio of SCI toMST are different, and most of the time cannot be easily compared (Baaj et al., 2010).
Contrary to Tchvaloon et al. (2008), we have thus observed a 56% increase in the number of associated organ injuries per casualty, while like them, we have observed little difference between the two periods in the levels of spinal and spinal cord deficit. However there is a marked but non-significant upward trend (relative risk 1.23; IC95 0.99–1.53) in the number of cervical injuries with complete as opposed to incomplete neurological deficit, which is frequently associated with mortality (Lieutaud et al., 2010; DeVivo et al., 1999; Ankarath et al, 2002).
Road users and demography
We have identified several reasons for this absence of change in the mortality and incidence of SCI: there has been a significant increase both in the proportion of SCI casualties who are motorcyclists and the overall number of motorcyclist casualties, in contrast to all other groups of road users (Gadegbeku et al., 2010). An analysis of the period 1996–2001 concurs with Australian data for the period 1987–1995 which revealed that among SCI casualties, car occupants predominated over motorcyclists (O'Connor, 2002). However, during the period 2003–2008, the ratio between motorcyclists and car occupants was reversed in France, and motorcyclists are now the dominant group among SCI casualties (34/23 in the more recent period vs 29/47 for car users; p<0.02). This is mainly the outcome of a 50% reduction in SCI sustained in a road crash among car occupants (OR 2.32). This change in the type of road users and, in particular, the increase in pedestrians and cyclists is associated with an increase in the proportion of older people in the study as the number of SCI casualties falls in all age categories up to the age of 40 years after which it increases. This has a non-negligible impact on the patient's expected neurological recovery as it has been shown that recovery from a neurological deficit and survival after SCI is better before 50 years of age than after (DeVivo et al., 1999; Catz et al., 2002; Tchvaloon et al., 2008; Penrod et al., 1990; Roth et al., 1992).
Last, the change in road users has also led to a significant increase in the proportion of complete or incomplete cervical spinal cord injuries compared with thoracic or lumbar injuries. This increase in cervical injuries, which are the main cause of early mortality (Lieutaud et al., 2010), may have been partly responsible for our failure to observe a reduction in mortality among SCI casualties in the more recent period (Lieutaud et al., 2010; DeVivo et al., 1999; Catz et al., 2002).
Limits of the study
One of the limits of the study is that it only considers spinal cord injuries that are caused by road traffic accidents. This problem is counterbalanced by the internationally recognized quality of the Registry as a result of its exhaustive coverage of a geographical zone. However, one cannot exclude the possibility that some patients died later, after returning home or in specialized centres, which would result in a slight underestimation of mortality. In western countries, such an underestimation would probably be very small as, with the exception of patients with cervical spinal injuries, once patients with spinal cord injuries have survived the initial phase, their longevity is practically identical to that of other individuals belonging to the same age group at the time of the accident (DeVivo et al., 1999; van den Berg et al., 2010; Tchvaloon et al., 2008). However, the fact that the population of individuals with SCI for us to study has a marked tendency to become older may partly explain the greater frequency of death after SCI.
The blood alcohol status of casualties with SCI sustained in road crashes was not recorded, but no further proof is required of the danger associated with intoxication of any type. The principal purpose of the Registry is not to demonstrate the obvious but to identify new factors that society can act on. However, knowledge of the blood alcohol status could have informed us about a need for a prevention policy that targets motorcyclists, whom we can now consider to be the group most at risk of serious spinal and spinal cord injuries.
Changes in behavior on the road: the reduction in average speeds
The fact that road safety policies have failed to have a visible effect on SCI raises a number of issues. One hypothesis about the reduction in road accidents is that it is due to lower average speeds. In France, studies have shown that the average speed of passenger cars fell by approximately 5 km/h on all types of road between 2002 and 2008 (ONISR, 2009). Likewise, in 2002, the percentages of car and motorcycle users exceeding the speed limits by 10% were 35% and 55% respectively. These figures dropped to 10% and 35% respectively in 2008. In 2008, motorcyclists still had higher mean speeds than motorists (86 vs 80 km.h−1).
The deployment of speed cameras since 2003 may have played a role in this reduction in mean speeds, not only near the cameras but also at a distance from them (Wilson et al., 2010). However, although the introduction of speed cameras and the changes in the legislation have played a significant role in reducing severe road trauma (casualties with AIS4+ injuries), the increase in traffic density may also have increased SCI. Greater traffic density may have led to a change in the types of vehicle used, with drivers attempting to avoid congestion by switching to a motorcycle because of its ability to move more freely in urban areas. Although the information on work-related accidents is frequently absent from the Registry, we failed to observe an increase in the rate of work-related accidents. Moreover, the other items of data (period of the year, time of day of the accident) have remained unchanged which gives the impression that motorcycle crashes still mostly occur during leisure trips, as reported in the majority of studies (Farmer and Williams, 2005).
Conclusion
The findings of this study confirm the quality of the primary prevention policies that target children, young adults or their parents, revealing a major reduction in crashes with SCI in the period between 2003 and 2008. However, quite unexpectedly in view of the fact that road trauma was approximately 35% lower in the more recent period and spinal trauma has fallen by 22%, we have not observed any significant reduction in the incidence and mortality of SCI sustained in road traffic accidents. Even more worryingly, we have observed an increase in multiple trauma and a deterioration in clinical outcomes for these casualties linked to a change in the road users that are affected and the ageing of the groups sustaining SCI. These findings confirm that although the incidence of road trauma is in general tending to fall in developed countries, the situation needs to be monitored continually. This study highlights the fact that if research that focuses on road casualties with SCI is conducted, in particular with a view to improving neuroprotection, it should, of course, target patients with a spinal cord injury, but also take account of the fact that the patients tend to be older than in the past and more frequently have associated multiple trauma.
Findings with regard to improvements in road safety are not always uniform for all injuries and there is now a need to strengthen preventive measures in relation to the populations that are most at risk of sustaining SCI in a road crash, be they motorcyclists, cyclists or pedestrians.
Footnotes
Acknowledgments
We wish to thank the following people for having participated in the data collection and data recording, within the Rhône road trauma registry Association (ARVAC, president E Javouhey), and within the INRETS-UMRESTTE research unit (B Laumon, scientific adviser and A Ndiaye, medical coordinator): Ait Idir T, Ait Si Selmi T, Alloatti D, Amoros E, Andrillat M, Artru F, Asencio Y, Assossou I, Auzaneau F, Bagès-Limoges F, Bagou G, Balogh C, Banssillon G, Banssillon V, Barnier N, Barth X, Basset M, Bec JF, Bejui J, Bel JC, Bérard E, Bérard J, Bernard JC, Berthet N, Bertrand JC, Besson L, Biot B, Biot V, Blanc C, Blanchard J, Boeuf C, Boisson D, Bonjean M, Bost J, Bouchedor C, Bouletreau P, Boyer M., Boyer V, Breda Y, Brilland R, Bussery S, Cabet N, Caillot L, Caillot JL, Cannamela A, Caregnato B, Carre M, Catala Y, Chagnon PY, Chambost M, Chantran C, Chardon P, Charnay P, Chatelain P, Chattard S, Chauvin F, Chavane H, Chazot G, Chettouane I, Chevreton N, Chevrillon E, Chevrillon S, Chiron M, Chotel P, Cochard P, Combe C, Contamin B, Coppard E, Cot T, Crettenet Z, Cristini A, Cunin V, Dailler F, Dal Gobbo B, David JS, De Angelis MP, Decourt L, Delfosse A, Demazière J, Deruty R, Desjardins G, Devaux J, Dohin B, Drouet A, Emonet A, Escarment J, Evrard AS, Eyssette M, Fallavier L, Fanton L, Felten D, Feuglet P, Fifis N, Figura J, Fisher G, Fischer LP, Flocard B, Floret D, Fournier G, Fraisse P, Fredenucci JF, Freidel M, Fuster P, Gadegbeku B, Galin L, Gaillard P, Gallon M, Garnier N, Garzanti A, Gaussorgues P, Gautheron V, Genevrier M, Gibaud F, Gillet Y, Gilly F, Goubsky A, Granger M, Grattard P, Gueniaud PY, Guenot C, Guérin AC, Guignand M, Guillaumée F, Haddak M, Hamel D, Haouas T, Heckel T, Herzberg G, Ho-Van-Truc P, Jacquemard C, Joffre T, Kohler R, Lablanche C, Lafont S, Lagier C, Lapierre B, Laplace MC, La Rosa C, Laurent R, Lebel M, Leblay G, Le-Xuan I, Lieutaud T, Lille R, Linné M, Lucas R, Machin B, Maiello E, Malicier D, Mangola B, Marduel YN, Marie-Catherine M, Martin JL, Martin YN, Martinand G, Marty F, Mazouzi S, Menard B, Messikh C, Meyer F, Meyrand S, Molard S, Monneuse O, Morel-Chevillet E, Mioulet E, Minjaud F, Mollet C, Monnet J, Moyen B, Neidhart JP, Ngandu E, Ny S, Ould T, Paget P, Paillot JC, Paris D, Patay B, Pauget P, Peillon D, Perrin G, Perrin-Blondeau D, Petit P, Piriou V, Piton JL, Plantier M, Pornon P, Pramayon C, Quelard B, Rakaa A, Raquin L, Remy C, Rezig M, Ricard A, Richard A, Rigal F, Robert D, Rode G, Romanet JP, Rongieras F, Roset C, Rousson A, Roussouli P, Roux H, Ruhl C, Salamand J, Salord F, Sametzky P, Sayegh K, Sayous P, Sbraire N, Scappaticci N, Schiele P, Schneider M, Simonet C, Sindou M, Soldner R, Soudain M, Stagnara J, Stamm D, Suc B, Supernant K, Taesch MC, Tasseau F, Tell L, Thomas M, Tilhet-Coartet S, Tissot E, Toukou JC, Trifot M, Tronc F, Vallee B, Vallet G, Vancuyck A, Vergnes I, Verney MP, Voiglio EJ, Vourey G, Vuillard J, Westphal M, Willemen L.
Author Disclosure Statement
None of the authors declare having conflict of interest about this study.