
Abstract
Decompressive craniectomy (DC) has been regarded as an ultima ratio measure in the treatment of refractory intracranial hypertension after brain injury. Most discussion about its benefits is based on studies performed in patients who are <65 years of age. The aim of this study was to identify patients aged ≥66 years who underwent DC after traumatic brain injury (TBI), in order to assess patient outcome and to correlate the values of potential predictors of survival on prognosis. From January 2002 to December 2009, 44 patients aged ≥66 underwent DC (follow-up, 12–102 months). Potential predictors of outcome were analyzed, including age, post-resuscitation Glasgow Coma Scale (GCS) score, presence of mass lesion, Simplified Acute Physiology Score (SAPS) II, Injury Severity Score (ISS), and timing of surgical decompression. Mortality was 48% at discharge from the intensive care unit (ICU), 57% at hospital discharge, and 77% at 1-year follow-up and at last follow-up. A bad outcome Glasgow Outcome Scale Dead-Vegetative State-Severely Disabled (GOS D-VS-SD) was observed in 36/44 patients both at hospital discharge and at 1-year follow-up. Mean SAPS II was 45.2 for patients who survived and 57.3 for patients who had died (p=0.0022). Patients who survived had a higher mean post-resuscitation GCS score (p=0.02). Logistical regression analysis indicated post-resuscitation GCS score as the only independent predictive factor for outcome. None of the 22 patients with a post-resuscitation GCS score of 3–5 had a good outcome, 2/10 (20%) patients with a post-resuscitation GCS score of 6–8 and 6/12 patients (50%) with a post-resuscitation GCS score ≥9 had a good outcome.
Introduction
R
In a previous article, we reviewed the studies in which elderly patients who underwent DC for traumatic brain injury (TBI) were analyzed (De Bonis et al., 2010). We concluded that in most published series, patients >30–50 years of age were excluded a priori and that in most of the studies that included older patients, the authors did not perform appropriate statistical analyses to assess differences in the outcome among age groups, or found no correlation between age and outcome.
In our institution, even after our previous report (showing that patients <40 years of age and aged 40–65 had no difference in outcome and that patients >65 years of age had a worse outcome), we have continued to perform DC in the elderly, because age has never been an exclusion criterion, for both ethical and cultural reasons (Pompucci et al., 2007).
The aim of this study was to identify patients ≥66 years of age who underwent DC after TBI, in order to assess patient outcome and to correlate the values of potential predictors of survival on prognosis.
Methods
Patient population
From January 2002 to December 2009, 1923 consecutive neurotrauma patients were admitted to our center. Eighty-nine out of 1923 patients (4.6%) underwent DC. For the purposes of this study, we only included 44 patients ≥66 years of age. The study cohort included 11 patients without focal lesions (in whom massive post-traumatic brain swelling—unilateral or bilateral—and therapy-resistant intracranial hypertension and/or clinical deterioration required DC) and 33 patients with a subdural hematoma/huge post-traumatic contusion/hemorrhage together with massive brain edema. These latter patients required DC following evacuation of the mass lesion.
Management prior to decompression
Patients were initially admitted to the Intensive Care Unit (ICU) and were treated according to the Guidelines for the Management of Severe head Injury (Maas et al., 1997; The Brain Trauma Foundation et al., 2000). Medical management included intubation, ventilation, oxygenation, 30–degree head elevation, fluid resuscitation, mild hyperventilation (Pco2 30–33 mm Hg), sedation (propofol 2–5 mg/kg/h, remifentanyl 0.1–0.2 μg/kg/min), normothermia (36–36.5°C), and normoglycemia. Osmotherapy with mannitol (1–2 g/kg/day) and hypertonic saline solution administration was the next step. Controlled ventricular drainage was used, when available, as a second-line instrument when maximal medical management alone was not able to control intracranial pressure (ICP) elevation (7 cases). Standard management included an admission CT scan. In cases in which an urgent surgical treatment was not required, CT scans were repeated every 6 h on the first day after trauma and then every 24 h, or after persistent ICP increase (>20 mm Hg). Seven patients received initial continuous intraventricular ICP monitoring and underwent DC after failure of maximal medical therapy for ICP control. The remaining 37 patients did not undergo preoperative placement of ICP monitoring. Patients in this group demonstrated rapid clinical deterioration immediately after admission, or had CT scans showing massive brain swelling and initial herniation requiring immediate surgery.
Indications for surgery and surgical technique
Criteria for DC were the appearance of diffuse unilateral or bilateral brain swelling on the CT scans with correlating clinical deterioration; massive brain swelling with loss of subarachnoid space in the basal cisterns; or initial herniation. Delayed surgical decompression was performed in patients who experienced persistent intracranial hypertension (ICP>30 mm Hg) and failed to respond to the maximal conservative therapy, or patients with delayed intracranial hypertension caused by late brain contusion development or increase in edema. Contraindications to craniectomy included primary fatal brainstem damage (bilaterally fixed and dilated pupils).
In patients on whom surgery was performed to treat diffuse cerebral edema without a mass lesion, a wide unilateral hemicraniectomy was performed, including removal of bone in the frontal, temporal, and parietal regions ipsilateral to the hemisphere in which the greatest swelling was observed on CT scans. The craniectomy was performed from the temporal bone to the floor of the middle fossa, to maximize the extent of decompression at the level of the basal cisterns. The dura mater was then widely opened in a stellate fashion to the extent of bone decompression, and a dural graft was placed to increase the available volume before closure. The bone flap was stored in sterile conditions with cryopreservation. In the absence of a mass lesion, the side chosen for the craniectomy was determined based on the presence of midline shift, swollen hemisphere, asymmetry of basal cisterns obliteration, nonsurgical brain contusions, and left or right-handedness. In these cases, a large hemicraniectomy allowed us to obtain a good ICP control. When a mass lesion was present, a similarly wide craniectomy incorporating the mass lesion was performed. A subdural catheter for postoperative ICP monitoring was placed in all patients.
The craniectomy limits were: anterior, frontal to the midpupillary line; posterior, 3–6 cm posterior to the external acoustic meatus; superior, 1–4.5 cm from the midline; and inferior, at level of the middle cranial fossa floor at the origin of the zygomatic arch. The mean anteroposterior diameter of the bone flap was 15 cm (range 13.5–17cm).
Data collection and statistical analyses
The following patient data were collected (Table 1): preoperative data (age; date-hour of trauma and date-hour of surgery; mechanism of the injury; post-resuscitation Glasgow Coma Scale [GCS] score—intubated patients were assigned an implied verbal score of 1-; Marshall score at preoperative CT scans; Injury Severity Score [ISS] and Simplified Acute Physiology Score [SAPS] II); intraoperative data (length of surgery, colloids and crystalloids administration); postoperative data (mannitol administration; ICP values; days of mechanical ventilation; percentage of patients with pneumonia; percentage of patients receiving antibiotics; percentage of patients who underwent tracheostomy; duration of ICU stay; duration of hospitalization; complications).
ISS, Injury Severity Score; SAPS, Simplified Acute Physiology Score; GCS, Glasgow Coma Scale; DC, decompressive craniectomy; EVD, external ventricular drainage; VP, ventriculo-peritoneal; ICU, intensive care unit; t-stu, Student t-test.
Outcome was assigned according to the Glasgow Outcome Scale (GOS). Patients were followed up as outpatients 1 month after hospital discharge, then every 3 months for the first year. Then, phone surveys were used to ascertain patients' vital status and clinical conditions. Follow-up ranged from 12 to 102 months for patients who were still alive. GOS score was determined at ICU discharge, at hospital discharge, at 1-year follow-up and at last follow-up. No patients were lost to follow-up. Patient outcome was used as the dichotomous dependent variable: bad outcome (GOS score Dead-Vegetative State-Severely Disabled [D, VS, SD]) or good outcome (GOS score Good Recovery-Moderately Disabled) at hospital discharge and at last follow-up. Potential predictors of outcome were analyzed, including age, post-resuscitation GCS score, presence of mass lesion, SAPS II, and timing of surgical decompression. The independent contribution of predictive factors to outcome was studied using logistical regression analysis. Student t-test was used to compare means. Fisher's exact test was used to compare categorical variables. Variables with p values <0.05 were considered statistically significant.
Results
Our series included 26 men and 18 women (mean age 76.6±5.8 years, age range 66–94 years). Patients' characteristics are summarized in Table 1.
Mortality was 48% at ICU discharge (21 patients), 57% at hospital discharge (25 patients) and 77% (34 patients) at 1-year follow-up and at last follow-up. A bad outcome (GOS D, VS, SD) was observed in 36/44 patients (82%) both at hospital discharge and at 1-year follow-up. Subgroup analysis revealed that the percentage of patients with a bad outcome was 82% both for patients with a mass lesion (27/33) and for patients without a mass lesion (9/11). The eleven patients discharged with an SD or in a VS either died (9 patients) or did not improve (2 patients) at 1-year follow-up. Thirty-nine patients had a controlled ICP (<20 mm Hg) after surgery. All patients (5 cases) with sustained postoperative intracranial hypertension (ICP ≥20 mm Hg) died in the ICU. SAPS II for patients who survived was 45.2±11.9 and was 57.3±10.6 for dead patients (p=0.0022), with a risk of death of 34.7% and 61.2% respectively. SAPS II was 60.3±8.8 and 52.4±11.9, with a risk of death of 68% and 50.7% (p=0.04) for patients who died in the ICU and for patients who died after ICU discharge, respectively. Student t-test showed that patients who survived had a higher mean post-resuscitation GCS score (p=0.02) (Table 1). Living and dead patients did not differ in terms of age, Marshall score, ISS, medical treatment during and after surgery, length of surgery, rate of patients with pneumonia (66% of all patients), or rate of patients who underwent tracheostomy (62% of all patients) (Table 1).
Logistical regression analysis indicated post-resuscitation GCS score as an independent predictive factor for outcome (Table 2). Sex, age, presence of a mass lesion, SAPS II score, and time interval between trauma and surgery were not statistically significantly associated with outcome in our population.
Comparing outcome among three groups (GCS scores 3–5; 6–8; ≥9), we observed that none of the 22 patients with a post-resuscitation GCS score of 3–5 had a good outcome (Fig. 1). Only 2/10 (20%) patients with a post-resuscitation GCS score of 6–8 and 6/12 patients (50%) with a post-resuscitation GCS score ≥9 had a good outcome (Fig. 1).
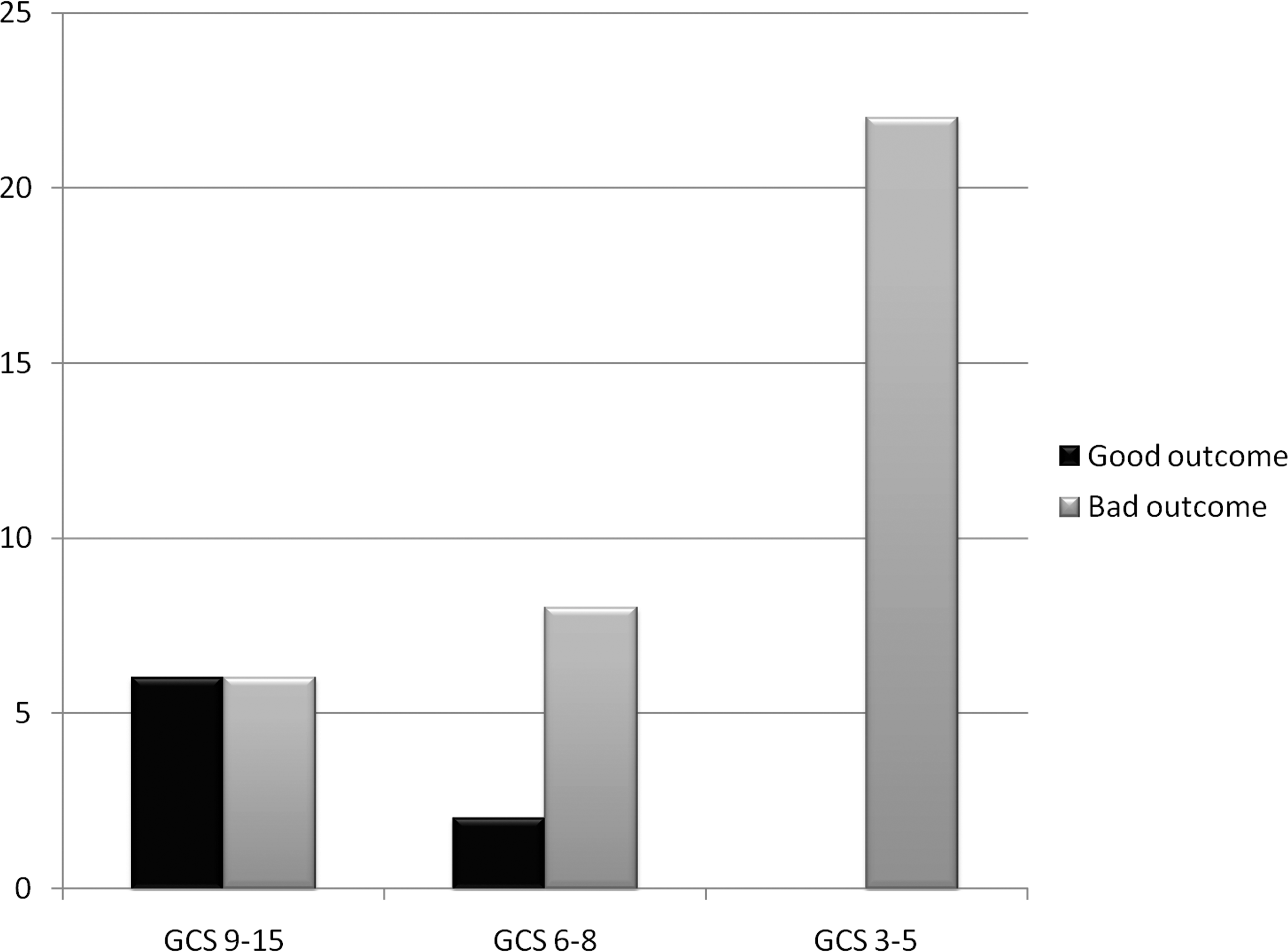
Graph showing outcome according to Glasgow Coma Scale (GCS) (p=0.001).
Discussion
GCS score and age are important prognostic indicators in patients with severe TBI (Hukkelhoven et al., 2003; Maas et al., 2007). There have been numerous studies demonstrating the bad outcomes of elderly patients after TBI when compared with those of younger patients. Elderly patients with TBI have increased lengths of hospital stay as well as an increased need for rehabilitation at hospital discharge (Mosenthal et al., 2004; Richmond et al., 2011) Several studies have demonstrated an increase in mortality in elderly patients who sustain TBI compared with that of younger patients. In almost all clinical studies and in all trials for the treatment of severe TBI, patients >65 years of age were excluded (De Bonis et al., 2010; Slieker et al., 2008). The recent DECRA study, which concluded that in adults with post-traumatic refractory intracranial hypertension caused by brain swelling, DC was associated with more unfavorable outcomes than was medical treatment, only included patients between the ages of 15 and 59 years (Cooper et al., 2011).
Recently, Brazinova et al. investigated the outcomes of patients with TBI who had GCS scores of 3 or 4 and were ≥66 years of age (Brazinova et al., 2010). In that series, 76/100 patients died at the ICU and 24 patients were discharged alive from the ICU (11 with ‘‘favorable’’ and 13 with ‘‘unfavorable’’ outcomes). At 12 months after trauma, 20 patients (20%) were still alive; 11 of them had favorable outcomes (11%). The authors then concluded that confirmed factors predicting poor prognosis for this group of patients were closed basal cisterns and midline shift >15 mm on the first CT scan. Factors possibly related to favorable outcomes were female gender, lower trauma severity, open or partially open basal cisterns, and no midline shift on the first CT scan. In that series, the surgical treatment was not specified (70 patients underwent a neurosurgical procedure, 41 patients underwent ICP monitoring).
To the best of our knowledge, no study has specifically investigated the outcomes of older patients who underwent DC after TBI.
In our series, we observed a mortality rate of 48% at ICU discharge and of 77% at 1-year follow-up, with a very high rate (82%) of patients with a bad outcome at 1-year follow-up. Mortality rate of the 22 patients with post-resuscitation GCS scores of 3–5 was 100%. Most patients who died had had a controlled ICP after surgery and no surgery-related complications. Nonetheless, the number of dead patients progressively increased after ICU discharge, confirming that older patients show a greater decline over the first 5 years after TBI than do younger patients (Marquez de la Plata et al., 2008). These results support the hypothesis that the adult brain has a decreased capacity for recovery as it ages (Carlsson et al., 1968). The brain's greater exposure to minor repetitive (often sub-clinical) insults as age increases, together with the presence of systemic comorbidities (e.g., vasculopathies, neuropathies) are also most likely contributors to the brain's reduced capacity for recovery and may therefore have a great impact on prognosis. Most of our patients died following infection, which is almost unavoidable in these patients, because of critical clinical conditions, prolonged bed stay and hospitalization, tracheostomy, and age-related comorbidities.
Interestingly, whereas we had already reported a correlation between increasing age and bad outcome in our previous report, in this series outcome didn't correlate with age, probably because we had exceeded the “age threshold” after which patients have a very low probability of a good outcome.
In this series, neither the severity of injury (measured with the ISS), nor the severity of CT findings (measured with Marshall score) correlated with outcome. None of the analyzed factors other than GCS score was associated with outcome at multivariate analysis.
SAPS II score was designed to measure the severity of disease for patients admitted to ICUs, taking into account physiological and anamnestical data during the first 24 h of the ICU admission. The value of the score is used as a mortality prediction model using a validated algorithm: the higher the score, the higher the predictable ICU mortality (PM) (Le Gall et al., 1993).
Older age and low GCS score at admission lead to a higher SAPS-II score. SAPS II score was high, as easily predictable, in the overall population (52.55) with PM of 50.7%. We found a high correlation between predicted (50.7%) and observed (48%) ICU mortality rate in this series.
Conclusion
In conclusion, patients >65 years of age treated with DC have a bad outcome in the great majority of cases. DC may probably prolong survival for days or a few months, as patients do not die from elevated ICP (and subsequent brainstem damage caused by herniation), but DC “does not reverse the primary brain injury associated with traumatic brain injury” (Polin et al., 1997). This damage, the “trauma” of surgery, the frequent comorbidities, the postoperative infections, and the brain's reduced capacity for recovery, predict a bad outcome in the vast majority of these patients.
All of this evidence could lead to a policy not to treat older patients with a low GCS score as aggressively as younger patients. One should balance the risk of not doing enough against the risk of an aggressive surgical treatment, such as DC, with the result of bad neurological outcomes, and to reserve surgery for cases with a higher probability of a good outcome, i.e., for patients with a high post-resuscitation GCS score. Finally, our results give rise to ethical questions in relation to the treatment with DC of patients >65 years of age with GCS score >5.
Footnotes
Author Disclosure Statement
All authors disclose any commercial/financial, actual or potential associations that might create a conflict of interest in connection with submitted manuscripts, according to the policy of the journal.