
Abstract
This study evaluated the injury severity profile of unilateral, frontal penetrating ballistic-like brain injury (PBBI) on neurofunctional outcome, blood–brain barrier (BBB) permeability, and brain edema formation. The degree of injury severity was determined by the delivery of a water-pressure pulse designed to produce a temporary cavity by rapid (<40 ms) expansion of the probe's elastic balloon calibrated to equal 5%, 10%, 12.5%, or 15% of total rat brain volume (control groups consisted of sham surgery or insertion of the probe only). Neurofunctional assessments revealed motor and cognitive deficits related to the degree of injury severity, with the most clear-cut profile of PBBI injury severity depicted by the Morris water maze (MWM) results. A biphasic pattern of BBB leakage was detected in the injured hemisphere at all injury severity levels at 4 h post-injury, and again at 48–72 h post-injury, which remained evident out to 7 days post-PBBI in the 10% and 12.5% PBBI groups. Likewise, significant brain edema was detected in the injured hemisphere by 4 h post-injury and remained elevated out to 7 days post-injury in the 10% and 12.5% PBBI groups. However, following 5% PBBI, significant levels of edema were only detected from 24 h to 48h post-injury. These results identify an injury severity profile of BBB permeability, brain edema, and neurofunctional impairment that provides sensitive and clinically relevant outcome metrics for studying potential therapeutics.
Introduction
T
Penetrating ballistic-like brain injury (PBBI) has been established as a military-relevant model of TBI, and can be calibrated to simulate the leading pressure or shockwave to the brain from penetrating projectiles of low or high velocities (Williams et al., 2006b). The 10% unilateral, frontal PBBI rodent model has been well characterized and reproduces acute neuropathological aspects of penetrating brain injury seen in humans, including lacerated brain damage, intracerebral hemorrhage, increased intracranial pressure (ICP), axonal degeneration, upregulation of pro-inflammatory cytokines, electrocortical disturbances, and neurofunctional impairment (Lu et al., 2011; Wei et al., 2009; Williams et al., 2005, 2006a,b, 2007). We also recently demonstrated that 10% unilateral frontal PBBI produces long-term motor and cognitive impairment indicative of striatal asymmetry and frontal lobe syndrome with progressive histopathology (Shear et al., 2010).
It is important to note that the sensitivity of outcome metrics to different degrees of injury severity in any brain injury model is highly relevant to their potential capacity to detect therapeutic efficacy. For example, a task that fails to discriminate between injury severity levels, effectively resulting in an all-or-none effect, is unlikely to be sensitive to therapeutic interventions in that injury model. Conversely, behavioral tasks that provide a clear gradient across the full range of injury severity levels would likely provide a more sensitive and reliable drug screening platform. To this end, the current study assessed the sensitivity of our neurofunctional and neurocognitive testing platform across a range of PBBI injury severity levels operationally defined by the magnitude of the ballistic component of the injury (calibrated to equal 5%, 10%, 12.5%, or 15% of total rat brain volume).
This study also investigated the time course and injury severity profile of blood–brain barrier (BBB) permeability and brain edema formation in the unilateral frontal PBBI model. The BBB is a highly specialized structure crucial for maintaining homoeostasis of the central nervous system (CNS) and limiting exposure to damaging cells and molecules. BBB disruption is a pathological hallmark of severe TBI, which is associated with neuroinflammatory events contributing to brain edema formation and cell death (Adelson et al., 1998; Marmarou, 1994; Marmarou et al., 2000). Understanding the time course of BBB breakdown as it relates to brain edema formation in the PBBI model is important to establishing the optimal therapeutic window and in the histopathological assessment of therapeutic interventions.
Methods
Subjects
Male Sprague–Dawley rats (250–300 g; Charles River Labs, Raleigh, VA) were used in all experiments. All procedures were approved by the Walter Reed Army Institute of Research Institutional Animal Care and Use Committee. Research was conducted in compliance with the Animal Welfare Act and other federal statutes and regulations relating to animals and experiments involving animals, and adhered to the principles stated in the Guide for the Care and Use of Laboratory Animals, National Research Council (NRC) Publication, 1996 edition. Animals were housed individually under a 12-h light/dark cycle (lights on at 0600) in a facility accredited by the Association for Assessment and Accreditation of Laboratory Animal Care International.
PBBI surgery
Unilateral (right) frontal PBBI was performed using a computer-controlled simulated ballistic injury device (Mitre Corp., McLean, VA) attached to a specially designed stainless steel probe (Popper & Sons Inc., New Hyde Park, NY). The probe was constructed from a 20-gauge stainless steel tube, with fixed perforations along one end that were sealed by airtight elastic tubing. Rats were anesthetized (isoflurane; 5% induction, 2% maintenance) and positioned in a stereotaxic frame (Kopf, Tujunga, CA) for probe insertion. The scalp was incised along the midline and a 4 mm diameter burr hole was created to expose the right frontal pole of the brain (+4.5 mm anteroposterior, +2 mm mediolateral from bregma). The PBBI probe was mounted to a stereotaxic arm and fixed at an angle of 50 degrees from the vertical axis and 25 degrees counter-clockwise from the anterior–posterior axis. The probe was then manually advanced through the cranial window, along the axis described previously, penetrating into the right frontal hemisphere to a distance of 1.2 cm (from dura). The ballistic component of the injury was induced by a rapid (<40 ms in duration) calibrated water pressure pulse designed to inflate the elastic tubing and form an elliptical-shaped balloon calibrated to equal 5%, 10%, 12.5%, or 15% of total rat brain volume. Following PBBI, the probe was retracted, the cranial window sealed with sterile bone wax, and the incision closed with wound clips. Control groups consisted of rats receiving sham surgeries with or without insertion of the probe (i.e., probe and sham controls). All behavioral testing and histological analyses were conducted by trained laboratory personnel who were blinded to the experimental conditions.
Neurobehavioral assessments
Neurobehavioral assessments were conducted on the following six groups: sham (n=10), probe (n=10), 5% PBBI (n=10), 10% PBBI (n=10), 12.5% PBBI (n=10), and 15% PBBI (n=8). The outcome metrics included neuroscore, forelimb asymmetry, rotarod, and Morris water maze (MWM) tasks. Histological end-points for these groups consisted of lesion reconstruction using H&E-stained sections.
Neuroscore
The modified neurological examination (Bederson et al., 1986) was used. This test was originally designed to assess cardinal features of focal ischemia, and is particularly sensitive to unilateral striatal damage, which is the primary lesion tract following unilateral, frontal PBBI (Shear et al., 2010). Neurological deficits were evaluated at 1, 3, and 7 days post-PBBI. Neurological scores (NS) were based on a 12-point sliding scale ranging from 0 (normal) to 3 (severely impaired) composed from the following four neurological tests that measured: 1) contralateral forelimb flexion during tail suspension, 2) shoulder adduction (body upward curling behavior) during tail suspension, 3) impaired resistance to lateral push, and 4) open-field circling behavior. Maximum composite score for all 4 tests combined equaled 12.
Forelimb asymmetry task
The forelimb asymmetry task assessed sensorimotor function by quantifying the animal's use of forelimbs to brace itself during vertical exploration (or rearing activity) (Bland et al., 2000). At 7 days post-injury, PBBI rats were individually placed in a Plexiglas® cylinder (20 cm diameter×30 cm high) for 5 min and videotaped for data analysis. The number of times the animal placed either its right (ipsilateral to the injury), left (contralateral to the injury), or both forelimbs on the wall of the cylinder, during rearing episodes, was scored. Data were normalized for statistical comparison using the following formula: Index of Asymmetry (IA)=(ipsi+½ both)/(ipsi+contra+both).
Rotarod task
The Rotamex-5 rotarod apparatus (Columbus Instruments, Columbus, OH) was used to measure motor coordination and balance. Prior to PBBI surgery, all rats were handled for 2 days (10 min per day) and then trained to criteria on a fixed-speed version of the rotarod task (Shear et al., 2010). One day prior to injury (baseline measures) and at 7 days post-injury, the ability of animals to remain balanced on the rotating rod was assessed at sequential fixed-speed increments of 10, 15, and 20 rpm for a maximum of 60 sec each trial (2 trials/speed; 60-sec ITI).
MWM task
A dark, blue polyurethane MWM pool (75 cm deep; 175 cm diameter) was filled with clear water (maintained at 22±1°C) to a depth of 60 cm. A clear Plexiglas platform was submerged to a depth of 1 cm from the water surface and placed ∼ 35 cm from the wall of the pool in the center of the northwest (NW) quadrant. The position of the platform remained constant throughout each experiment.
Animals were given four trials per day for 5 consecutive days (30-min ITI) from 10 to 14 days post-PBBI. For each trial, animals were placed in the MWM, with their nose facing the pool wall, at one of four pseudo-randomly determined starting points (e.g. north, south, east, and west) and given 90 sec to locate the hidden platform. Once an animal found the platform, it was allowed to rest for 10 sec before being removed to its home cage. Animals that could not locate the platform within the allotted time were gently guided to the platform and allowed to rest for 10 sec. Between trials, animals were placed back in their home cages, which were kept warm via the use of water-circulating warming blankets. All trials were recorded with a digital video-tracking system (Noldus EthoVision XT). Primary outcome measures included: 1) latency (sec) to find the hidden platform, 2) swim distance (cm) to the hidden platform, and 3) swim speed (cm/sec).
Histopathology
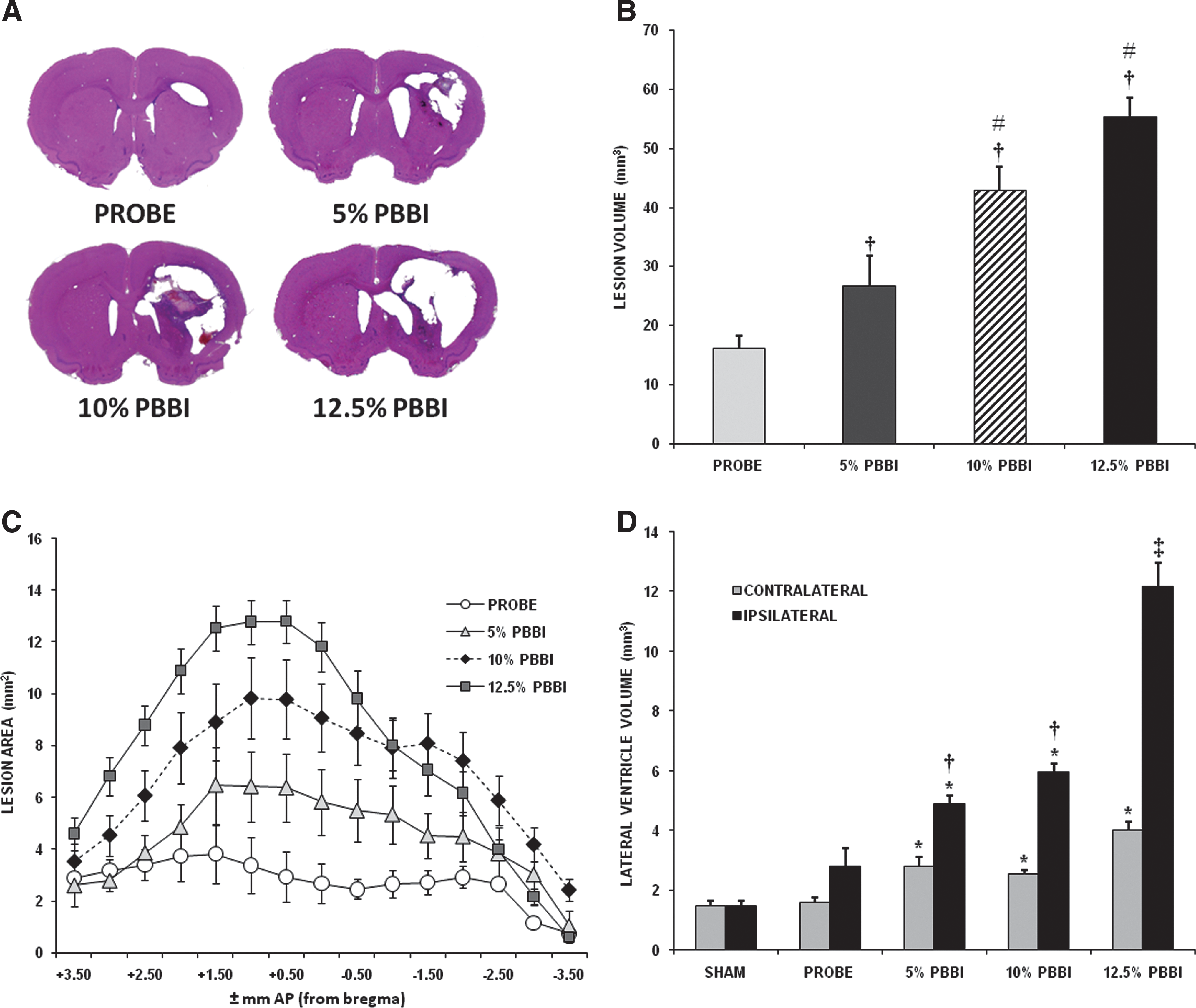
At 3 weeks post-injury, animals were fully anesthetized with ketamine/xylazine (70 and 6 mg/kg, i.p., respectively) and perfused with 4% paraformaldehyde. Coronal brain sections (40 μm thick) were cut from +4.0 to −7.0 mm anteroposterior (AP) from bregma. Serial sections (22 per rat) collected at 500-μm intervals were processed using H&E staining for analysis of lesion volume (FD Neurotechnologies, Baltimore, MD). All brain tissues used for lesion volume quantification were digitally imaged using a light microscope (Olympus BH-2) under a 0.5×objective lens and then imported into a computer-based image analysis system (Loats Assoc., Westminster, MD). Total lesion volume was calculated by summing a distance-weighted average of sequential lesion areas according to the principles of Cavalieri. Sequential lesion areas were defined by tracing the perimeter of the lesion cavity (including injured penumbra) across 15 serial sections (+3.50 to −3.50 mm AP from bregma). Similarly, volumetric measurements of the lateral ventricles were quantified from five serial brain sections (∼+1.50 to −0.50 from bregma). Mean lesion cavity volume and lateral ventricle volumes from PBBI groups at each injury severity level were used for statistical comparison.
BBB permeability
A time course for BBB permeability was assessed using Evans blue (EB) extravasation (Uyama et al., 1988). EB dye (2% solution in phosphate buffered saline; pH 7.4) was injected intravenously (4 mL/kg) at 4 h, 24 h, 48 h, 72 h, or 7 days post-injury and allowed to circulate for 30 min prior to perfusion. Groups consisted of animals receiving sham, probe, 5% PBBI, 10% PBBI, and 12.5% PBBI (n=5 per group/time point). At assigned time points, the animals were anesthetized with ketamine/xylazine (70/6 mg/kg, i.p.) and perfused with saline until the fluid from the right atrium was clear. The meninges and outer vessels were removed and the brains were placed in a brain-block device and cut into coronal (4 mm) sections. Each section was then cut in half along the anatomic midline and the 4-mm samples from the peri-contusion area (∼+2.60 to −1.40 mm AP from bregma) of the ipsilateral and corresponding contralateral hemisphere were stored at −80° C until processed. For EB processing, brain samples were minced, weighed, and placed in 50% trichloroacetic acid solution (volume=2.0 mL). Following homogenization and centrifugation (30 min at 5,000g), the absorbance of the extracted dye in supernatant at 610 nm was recorded and EB values were expressed as μg/g of brain tissue against a standard curve.
Brain edema formation
Animals were randomly assigned to one of five groups (n=6 per group/time point): sham, probe, 5% PBBI, 10% PBBI, and 12.5% PBBI, and brain edema measurements were taken at 4 h, 24 h, 48 h, 72 h, 5 days, 6 days, and 7 days post-PBBI. At each post-injury time point, animals were euthanized with CO2 followed by rapid decapitation. The same anatomical regions of the ipsilateral and contralateral brain hemisphere as described previously for the BBB study were collected and quickly placed in pre-weighed microcentrifuge tubes, which were then immediately capped to prevent further evaporation (the brain surface was exposed for no more than 90 sec). After the wet weight of the brain sections was obtained, the cap was removed and the open tubes were placed in a vacuum oven (60°C). After drying for 5 days, the containers were removed from the oven, immediately capped, and reweighed. All weighing was done on the same balance and all weights were recorded three times each. The percentage of water content was calculated for each hemisphere using the following formula: % water=[(wet weight – dry weight)/wet weight]×100.
Statistical analysis
Histopathological and behavioral end-points were compared by independent samples t tests or analysis of variance (ANOVA) followed by Fisher Projected Least Significant Difference (PLSD) post hoc and paired t test analyses when appropriate. All data are presented as the mean±standard error of the mean (S.E.M), p values<0.05 were considered significant. For all experiments, trained investigators performing behavioral and neuropathological assessments were blinded to the experimental groups.
Results
Neurobehavioral assessments
Behavioral assessments could not be performed on 15% PBBI animals (n=8) because none of these animals survived; five died immediately from prolonged apnea and the remaining three died within 24 h post-injury. Because 15% PBBI resulted in 100% mortality in this experiment, this group was not included in the subsequent BBB or edema experiments. No mortality was observed following 5%, 10%, or 12.5% PBBI.
Neuroscore
A mixed-factorial (5 groups×3 time points) ANOVA on neuroscore assessments showed a significant between-group effect (F 4,45=82.03, p<0.01). Compared to normal (zero) scores for sham-operated animals, significant neurological deficits were detected by 24 h post-injury in all PBBI animals and remained elevated out to 7 days post-injury (Fig. 1A; sham data not shown). However, more severe deficits were evident following 10% and 12.5% PBBI.

Graphs show results of
Forelimb asymmetry task
Sham animals had an IA score of 52.55±3.07 indicating normal (nonpreferential) use of both forelimbs during cylinder exploration. ANOVA results (F 4,45=5.05, p<0.05) showed that all injury severities (including probe) produced a similar degree of sensorimotor dysfunction in the contralateral limb on this task at 7 days post-injury compared to sham animals (Fig. 1B).
Rotarod task
Prior to PBBI, all groups had achieved a stable, baseline level of performance. The mixed-factorial (5 groups×3 speeds) ANOVA showed that all injured groups (including probe-inserted controls) displayed significant motor deficits at 7 days post-injury (F 4,45=12.05, p<0.05), with more severe motor impairment evident following 10–12.5% PBBI (Fig. 1C).
MWM Task
MWM data were analyzed using the repeated-measures (5 groups×5 days) ANOVA for each outcome metric. Results showed that PBBI produced significant cognitive impairment in all injured groups (except for probe controls) evidenced by longer latencies (F 4,45=22.05, p<0.01; Fig. 1D) and longer swim distances (F 4,45=11.62, p<0.01) to the hidden platform. Post hoc analysis revealed the PBBI-induced cognitive impairment was directly ranked by the degree of injury severity, with 12.5% PBBI causing the greatest impairment and 5% PBBI causing the least significant cognitive deficits (albeit still significantly higher than control animals). No significant between-group differences were detected on swim-speed measures.
Histopathology
At 3 weeks post-injury, ANOVA results on lesion volume measures showed significant and progressive between-group differences (F 3,36=26.08, p<0.01) that corresponded to the degree of PBBI severity. Post hoc analysis showed that although 5% PBBI caused significantly more damage than insertion of the probe alone, this was not as severe as the damage caused by 10% and 12.5% PBBI (Fig. 2B). Likewise, significant between-group differences were detected on volumetric measurements of the lateral ventricle both ipsilateral (F 4,45=37.27, p<0.01) and contralateral (F 4,45=9.46, p<0.01) to the injured hemisphere. Significant ventricular enlargement was detected in both the ipsilateral and contralateral hemispheres following 5%, 10%, and 12.5% PBBI (Fig. 2D), but this effect was much greater in the injured hemisphere than in the uninjured hemisphere (p<0.05 ipsilateral compared to contralateral). Insertion of the probe alone resulted in a small but not significant increase in lateral ventricle volume (p>0.05).
EB extravasation
The injury severity profile of PBBI-induced BBB disruption was assessed over a 1-week time course by measuring the extravasation of EB dye into the brain parenchyma. Two time points for the sham groups were used: 4 h and 24 h post-injury. Data from PBBI groups euthanized at 4 h post-PBBI were compared to sham data at 4 h post-injury. Data from PBBI groups euthanized at 24 h to 7 days post-injury were compared to sham data at 24 h post-injury.
PBBI produced in an injury-severity-dependent gradient of BBB leakage in the ipsilateral (injured) hemisphere that occurred in two temporal phases (Fig. 3A). An initial increase in EB dye extravasation was detected in the ipsilateral hemisphere of all injured animals (including probe) at 4 h post-injury (F 4,21=15.47, p<0.05) that appeared to resolve by 24 h post-injury (F 4,23=2.17, p>0.10). A second increase in EB extravasation was detected in the injured hemisphere at 48 h (F 4,23=4.10, p<0.05) and 72 h post-injury (F 4,24=9.22, p<0.05) that remained elevated out to 7 days post-injury following 10–12.5% PBBI (p<0.05). Notably, significant BBB leakage was also detected in the injured hemisphere of probe-inserted control animals at 4 h and 72 h post-PBBI. The whole brain and coronal sections pictured in Figure 3 show the pattern and distribution of EB dye extravasation at the different injury severities at 4 h post-PBBI (Fig. 3C) and across the different time points at 10% PBBI (Fig. 3D).
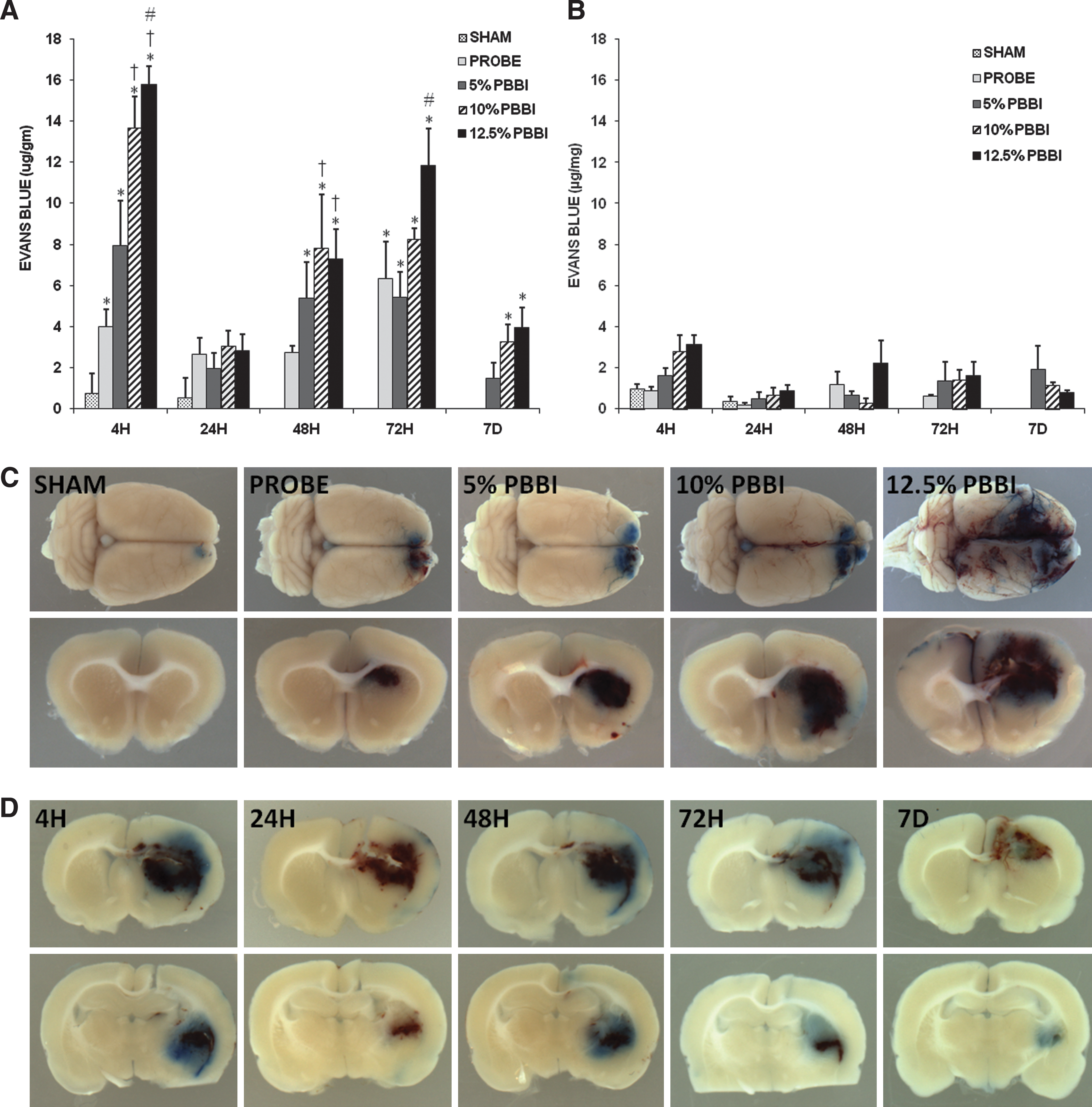
Measurements of Evans blue (EB) extravasation in the ipsilateral (injured) hemisphere
Brain edema formation
Brain edema formation was analyzed as percent brain water content in the 1) ipsilateral (injured) and 2) contralateral hemispheres, and as 3) the percent increase in brain water content in the ipsilateral vs. the contralateral hemisphere (Fig. 4). Two time points for the sham groups were used: 24 h and 7 days post-injury. Data from PBBI groups euthanized between 4 h and 5 days post-PBBI were compared to sham data at 24 h post-injury. Data from PBBI groups (10% and 12.5% PBBI) euthanized at 6 or 7 days post-injury were compared to sham data at 7 days post-injury.
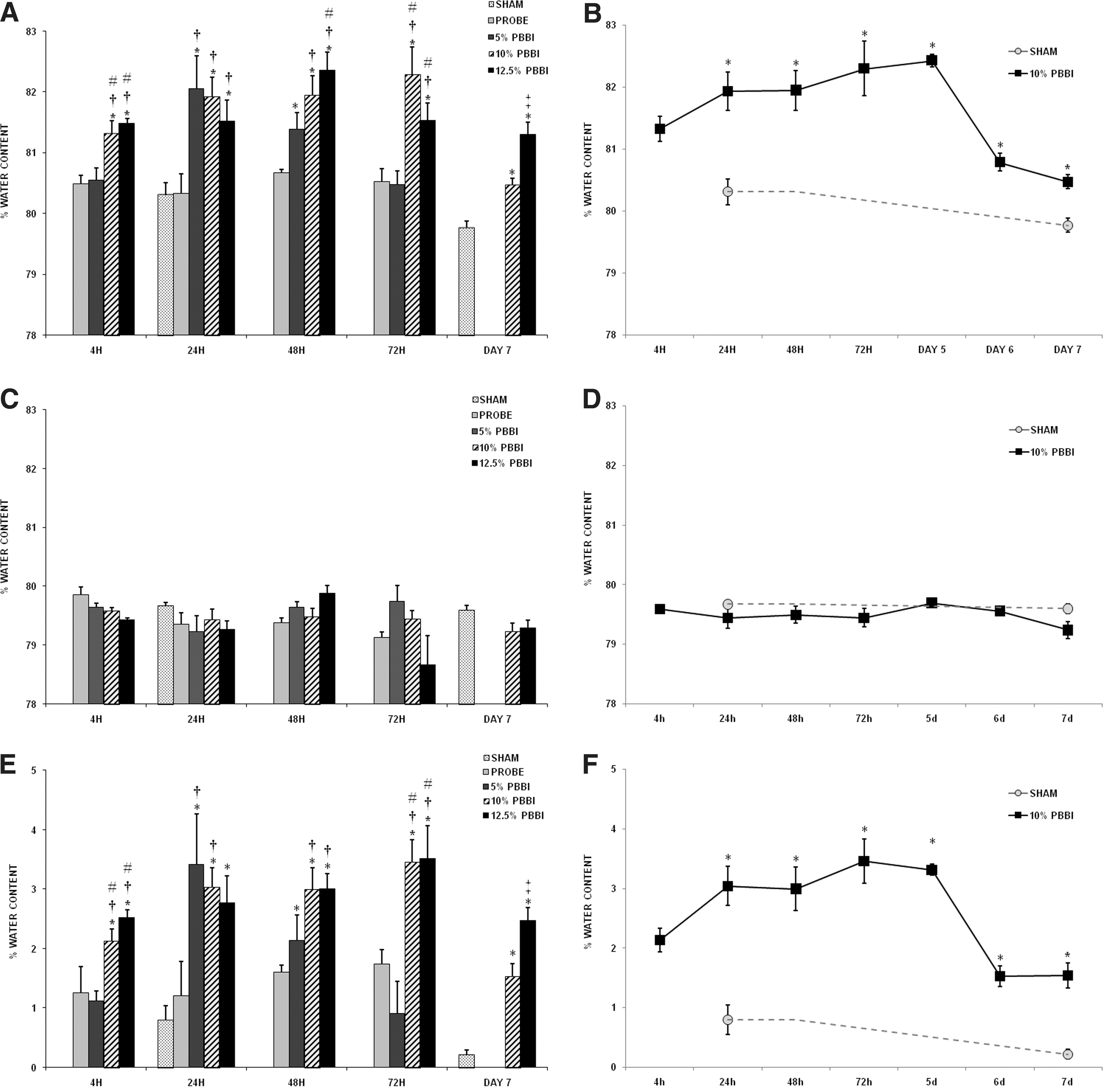
Measurements of edema formation in the ipsilateral (injured) hemisphere
Following PBBI, an injury-severity-dependent pattern of brain edema formation was detected in the ipsilateral (injured) hemisphere. Significant increases in edema levels were apparent by 4 h post-injury (F 4,21=9.01, p<0.01) at the two highest injury severity levels (10% and 12.5%), which remained elevated out to 7 days post-PBBI (F 2,16=21.63, p<0.01). In contrast, following 5% PBBI, significant increases in edema levels were not detected until 24 h post-injury (p<0.01) and only remained elevated to 48 h post-injury (p<0.01). No significant edema was detected following insertion of the probe alone, nor was any significant edema detected in the contralateral (uninjured) hemisphere (Fig. 4C). Figure 4E shows the results normalized as the percent increase in brain water content in the ipsilateral vs. the contralateral hemisphere.
Significant (>50%) reductions in brain edema were detected in 10% and 12.5% PBBI brains between 72 h and 7 days post-injury. In order to accurately pinpoint the time frame when edema began to subside following PBBI, additional edema measurements were taken at 5 and 6 days post-injury (10% PBBI rats only). Results showed that significant (54±5%) resolution of edema occurred between 5 and 6 days post-PBBI (Fig. 4B and F), although edema levels in 10% PBBI brains remained significantly higher than sham at both 5 (t 10=9.25, p<0.05) and 6 days post-injury (t 10=5.61, p<0.05).
Discussion
In the current article, we assessed the sensitivity of our neurobehavioral testing platform and characterized the time course profile of BBB permeability and brain edema formation across different injury severity levels in the PBBI model. Neurobehavioral measures revealed motor and cognitive deficits related to the degree of injury severity on all testing parameters except for the forelimb asymmetry (cylinder) task. Histopathology measures identified a biphasic pattern of BBB permeability and a time course of brain edema formation following PBBI, both of which were closely related to the degree of injury severity.
Neurobehavioral assessments
The neurological examination used in the present study was based on a neurological grading system originally developed by Bederson and colleagues (1986) for use in experimental stroke models. In the present study, PBBI produced various degrees of neurological dysfunction indicative of striatal asymmetry, which were more prominent following 10% and 12.5% PBBI than following 5% PBBI or insertion of the probe alone.
The cylinder task has been widely used to evaluate motor abnormalities and therapeutic efficacy in other models of CNS injury (Choi-Lundberg et al., 1998; Schallert et al., 2000; Tillerson et al., 2001). We previously reported that 10% unilateral, frontal PBBI produces deficits on this task that appear more comparable to what has been reported in focal injury models that produce extensive cortico-striatal damage (Clausen et al., 2009; Shear et al., 2010). In the current study, the cylinder test failed to discriminate between any injury severity levels (including probe alone), which suggests that this task would not provide a sensitive outcome metric in the PBBI model, and is therefore not viable for drug testing studies. In part, because the cylinder task is a test of spontaneous, unskilled limb use, the failure of this task to detect differences between the probe-insertion alone and the different PBBI injury severity levels may be caused by a lack of motivation to use the impaired limb.
The Rotarod test represents one of the most commonly used behavioral assessments, and has been described as a sensitive index of injury-induced motor dysfunction in TBI models (Hamm et al., 1994). We have previously demonstrated that 10% unilateral, frontal PBBI results in motor deficits on a fixed-speed Rotarod task that remain evident out to 4 weeks post-injury, which supported the use of the fixed-speed testing paradigm in our longitudinal neurofunction platform for the PBBI model (Shear et al., 2010). PBBI caused motor deficits at all injury severities (including probe) but there was a clear segregation between the lower (probe and 5% PBBI) and higher (10% and 12.5% PBBI) magnitudes of injury severity indicating that ≥10% PBBI is required for drug testing.
At its inception, the MWM task was designed to assess hippocampal-dependent spatial learning and memory mechanisms (Morris, 1984). However, a strength of this task is that the testing platforms can be exquisitely sensitive to abnormalities in cognitive function caused by damage to many different brain areas, not just the hippocampus (De Leonibus et al., 2003; Devan and White, 1999; Devan et al., 1999; Lyeth et al., 1990; Shear et al., 1998a,b; Whishaw and Jarrard, 1996; Whishaw et al., 1987). In the current study, the observation of a clear gradient in cognitive performance across the full range of injury severity levels provides further support for this task as being a sensitive and reliable drug-screening platform in the PBBI model.
BBB permeability and brain edema formation
In human patients, BBB disruption has been related to worse neurological outcome following stroke (Lorberboym et al., 2003) and more recently, to the development of post-traumatic epilepsy following TBI (Lorberboym et al., 2003; Tomkins et al., 2011). Brain edema is one of the most important clinical complications following trauma to the brain, and falls into two major categories; cytotoxic and vasogenic edema. Cytotoxic edema is caused by metabolic disturbances and occurs rapidly following TBI, resulting in acute intracellular swelling and necrotic cell death (Bakay et al., 1986a,b; Beaumont et al., 2000; Kimelberg, 1992). In contrast, vasogenic edema is thought to occur as a result of BBB breakdown, which allows blood plasma and solutes to leak into the brain's extracellular space, causing water to diffuse to the site of higher solute concentration, and contributing to a net volume increase in the brain, resulting in increased ICP and reduced cerebral blood flow (CBF) (Beaumont et al., 2000; Klatzo, 1985).
In the current study, we detected a biphasic pattern of BBB permeability in the ipsilateral (injured) hemisphere consistent with what others have reported in TBI and ischemic injury models (Baldwin et al., 1996; Baskaya et al., 1997; Belayev et al., 1996; Zhao et al., 2007). The first opening was evident at 4 h post-injury at all injury severity levels (including probe) and corresponded to increased edema levels following 10% and 12.5% PBBI. However, acute EB dye leakage subsided by 24 h post-injury, whereas edema levels remained elevated at the higher injury severity levels (10% and 12.5% PBBI). Moreover, post-injury levels of edema continued to rise in 5% PBBI brains, reaching significant levels by 24 h post-injury. The observation of sustained and progressive brain edema formation at 24 h post-PBBI, in the absence of EB dye extravasation, supports previous work indicating that the manifestation of brain edema in the acute post-injury phase is predominately cytotoxic (Beaumont et al., 2000). With respect to this, the acute (4 h) post-injury EB dye leakage may be at least partly the result of a combination of factors, including mechanical disruption of the microvascular system resulting in leakage from torn blood vessels (Dietrich et al., 1994; Lotocki et al., 2009) and/or poor clearance from damaged blood vessels (Louin et al., 2006). As such, these results should be interpreted with caution regarding acute BBB permeability in the PBBI model.
A second peak phase of EB dye extravasation was detected between 48 and 72 h post-injury at all injury severity levels, which remained evident out to 7 days post-PBBI in the brains of 10% and 12.5% PBBI animals. This delayed profile of EB dye extravasation coincides with the delayed neuroinflammatory response in the PBBI and other brain injury models (Morganti-Kossmann et al., 2007; Wei et al., 2009; Whalen et al., 1999; Williams et al., 2007) and therefore may provide a more genuine indication of injury-induced BBB breakdown. Notably, the injury-severity-dependent profile of brain edema levels appeared to recede in parallel with the secondary phase of BBB resolution, although both edema and EB dye levels remained evident at 7 days post-injury in the brains of 10% and 12.5% PBBI rats. This may indicate that the acute post-injury edema shifted to more vasogenic profile as a result of secondary neuroinflammatory events, BBB disruption, and elevated ICP (Wei et al., 2009; Williams et al., 2007).
One of the primary mechanisms for edema resolution involves the bulk flow of edemic fluid into the ventricles. This suggests the PBBI-induced ventricular enlargement detected at 3 weeks post-injury in the current study may have been a symptom of post-traumatic hydrocephalous, a frequent and serious complication of TBI that can contribute to the development of post-traumatic seizure disorders, including epilepsy (Blatter et al., 1997; Marmarou et al., 1996; Mazzini et al., 2003). In further support of this, it has recently been demonstrated that acute post-injury manifestation of non-convulsive seizures is directly related to the degree of injury severity in the PBBI model (Lu et al., 2011). Therefore, to the extent that PBBI-induced ventricular enlargement is indicative of post-traumatic hydrocephalus; it may represent an important therapeutic target in the PBBI model.
Summary and Conclusions
In the present study, we demonstrated an injury severity profile of motor and cognitive abnormalities in the PBBI model and provided further validation for several sensitive, clinically relevant outcome metrics for studying potential therapeutics. In addition, we identified an injury-severity-dependent profile of BBB permeability and brain edema formation that further defined the therapeutic window in this brain injury model.
In TBI, the therapeutic windows created by delayed, secondary complications are the principal target for therapeutic intervention. However, acute therapeutic benefits, which often serve as a foundation for chronic studies, may not always translate to improved behavioral outcome, particularly if the treatment is withdrawn prematurely (Shear et al., 2002).
Importantly, others have demonstrated a gradient effect of BBB permeability following injury (Lotocki et al., 2009; Zhao et al., 2007) indicating that BBB breakdown following CNS injury is not an all-or-none event. Future work using small molecule tracers is warranted to further identify the temporal gradient of BBB breakdown in the PBBI model.
Footnotes
Acknowledgments
This material has been reviewed by the Walter Reed Army Institute of Research. There is no objection to its presentation and/or publication. The opinions or assertions contained herein are the private views of the authors, and are not to be construed as official, or as reflecting the views of the Department of the Army or the Department of Defense.
Author Disclosure Statement
No competing financial interests exist.