
Abstract
Clinical features can be used to identify which patients with minor brain injury need CT scanning. A systematic review and meta-analysis was undertaken to estimate the value of these characteristics for diagnosing intracranial injury (including the need for neurosurgery) in adults, children, and infants. Potentially relevant studies were identified through electronic searches of several key databases, including MEDLINE, from inception to March 2010. Cohort studies of patients with minor brain injury (Glasgow Coma Score [GCS], 13–15) were selected if they reported data on the diagnostic accuracy of individual clinical characteristics for intracranial or neurosurgical injury. Where applicable, meta-analysis was used to estimate pooled sensitivity, specificity and likelihood ratios. Data were extracted from 71 studies (with cohort sizes ranging from 39 to 31,694 patients). Depressed or basal skull fracture were the most useful clinical characteristics for the prediction of intracranial injury in both adults and children (positive likelihood ratio [PLR], >10). Other useful characteristics included focal neurological deficit, post-traumatic seizure (PLR >5), persistent vomiting, and coagulopathy (PLR 2 to 5). Characteristics that had limited diagnostic value included loss of consciousness and headache in adults and scalp hematoma and scalp laceration in children. Limited studies were undertaken in children and only a few studies reported data for neurosurgical injuries. In conclusion, this review identifies clinical characteristics that indicate increased risk of intracranial injury and the need for CT scanning. Other characteristics, such as headache in adults and scalp laceration of hematoma in children, do not reliably indicate increased risk.
Introduction
Clinical assessment of the patient with a minor brain injury involves identifying features of the clinical history and examination that are associated with an increased likelihood of intracranial injury, and therefore indicate a potential need for CT scanning. Clinical assessment may be undertaken in an unstructured manner, with clinicians using estimates of the diagnostic value of each feature to adjust their estimate of the probability of intracranial injury, or in a structured manner, with selected features being used to guide or mandate CT scanning according to a clinical decision rule. Whichever method is used, it will be helpful to have estimates of the diagnostic value of each clinical feature that could be used to identify intracranial injury, so that we know which features should influence unstructured assessment or be incorporated in a clinical decision rule.
We therefore undertook a systematic review and meta-analysis to evaluate the diagnostic value of clinical characteristics that can be used to identify intracranial injury (including the need for neurosurgery) in adults, children, and infants with minor brain injury.
Methods
The systematic review and meta-analysis was undertaken in accordance with the guidelines published by the Centre for Reviews and Dissemination for undertaking systematic reviews (Centre for Reviews and Dissemination, 2009) and the Cochrane Diagnostic Test Accuracy Working Group on the meta-analysis of diagnostic tests (Deeks et al., 2009; Leeflang et al., 2008).
Data sources and searches
Potentially relevant studies were identified through searches of 13 electronic databases including MEDLINE (1950 to April 2009; supplemented with an update to March 2010), EMBASE (1980 to April 2009), CINAHL (1981 to April 2009), and the Cochrane Library (2009, issue 2). The search strategy used free text and thesaurus terms and combined synonyms relating to the condition (e.g., head injury) with a search filter aimed at restricting results to diagnostic accuracy studies (used in the searches of MEDLINE, CINAHL, and EMBASE only). Language restrictions were not used on any database. Searches were supplemented by hand searching the reference lists of all relevant studies (including existing systematic reviews) and leading experts in the area of minor brain injury were contacted to identify additional published or other unpublished reports. Further details on the search strategy can be found in Table S1 (Supplementary Data are available online at
Study selection
Four reviewers (APa, APi, SG, and SH) independently assessed the inclusion of potentially relevant articles in three phases. In phase I, two authors (APa and SH) screened all titles to exclude obviously irrelevant articles (i.e., nonhuman, unrelated to minor brain injury). In phase II, the list of included abstracts that were identified as possibly relevant by title were divided equally between two pairs of authors (APa and APi, SG and SH) and assessed independently by each reviewer for inclusion. The full manuscript of all potentially eligible articles that were considered relevant by either pair of authors was obtained, where possible. In phase III, all relevant full text articles were independently assessed for inclusion (APa and SH, checked by APi and SG) and any disagreements in the selection process (within or between pairs) were resolved through discussion and included by consensus between the four reviewers.
Studies were considered eligible for inclusion if they met the following criteria: 1) diagnostic cohort study (prospective or retrospective) of adults and/or children (of any age; minimum 20 subjects) with minor brain injury (defined as blunt head injury with a GCS of 13 to 15 at presentation; 2) studies describing any individual clinical characteristics to identify patients at risk of any intracranial injury or need for neurosurgical intervention, and included a proportion of the cohort undergoing imaging; and 3) provided data that allowed true positive (TP), true negative (TN), false positive (FP) and false negative (FN) numbers to be extracted or calculated. Studies that recruited patients with a broad range of brain injury severities were only included if >50% of the patients had minor brain injury. Full-text non-English language citations were excluded from this review because of limited resources for translation.
Data extraction and quality assessment
Data relating to study design, quality, and results were extracted by one reviewer (SH) into a standardized data extraction form and independently checked for accuracy by a second (APa). Any discrepancies were resolved through discussion to achieve agreement. Where differences were unresolved, a third reviewer's opinion was sought (SG or APi). Where multiple publications of the same study were identified, data were extracted and reported as a single study.
Although all clinical variables were considered, we selected 32 clinical characteristics (Tables 1 –5) for data extraction on the basis of having reasonably consistent definitions and being relevant to routine clinical practice. Other characteristics, such as confusion, lethargy, and irritability were considered too ill-defined for consistent recording. Of note, intoxication was defined as alcohol or drug intoxication; visual symptoms was defined as any visual disturbances, changes, symptoms or blurred vision; persistent vomiting was defined as repeated vomiting (≥2 episodes); retrograde amnesia was defined as amnesia >30 min before impact; basal skull fracture was defined as any clinical signs suggestive of a base of skull fracture; and radiological skull fracture was defined as any skull fracture diagnosed on an imaging modality, such as CT or radiography.
GCS, Glasgow Coma Scale; LOC, loss of consciousness; CI, confidence interval; NLR, negative likelihood ratio; PLR, positive likelihood ratio.
Pooled estimates based on the following: data from one study only - observed data; data from two studies - a fixed effects meta-analysis conducted using the method of DerSimonian and Laird (1986); data from three or more studies - a full Bayesian meta-analysis conducted using the bivariate random effects method of Reitsma et al. (2005).
Credible interval if more than three studies meta-analyzed.
Significant heterogeneity, p-value<0.05.
GCS, Glasgow Coma Scale; LOC, loss of consciousness; CI, confidence interval; NLR, negative likelihood ratio; PLR, positive likelihood ratio.
Pooled estimates based on the following: data from one study only - observed data; data from two studies - a fixed effects meta-analysis conducted using the method of DerSimonian and Laird (1986); data from three or more studies - a full Bayesian meta-analysis conducted using the bivariate random effects method of Reitsma et al. (2005).
Credible interval if more than three studies meta-analyzed.
Significant heterogeneity, p-value<0.05.
GCS, Glasgow Coma Scale; LOC, loss of consciousness; CI, confidence interval; NLR, negative likelihood ratio; PLR, positive likelihood ratio.
Pooled estimates based on the following: data from one study only - observed data; data from two studies - a fixed effects meta-analysis conducted using the method of DerSimonian and Laird (1986); data from three or more studies - a full Bayesian meta-analysis conducted using the bivariate random effects method of Reitsma et al. (2005).
Credible interval if more than three studies meta-analyzed.
Significant heterogeneity, p-value<0.05.
GCS, Glasgow Coma Scale; LOC, loss of consciousness; CI, confidence interval; NLR, negative likelihood ratio; PLR, positive likelihood ratio.
Pooled estimates based on the following: data from one study only - observed data; data from two studies - a fixed effects meta-analysis conducted using the method of DerSimonian and Laird (1986); data from three or more studies - a full Bayesian meta-analysis conducted using the bivariate random effects method of Reitsma et al. (2005).
Credible Interval if more than 3 studies meta-analyzed.
Significant heterogeneity, p-value<0.05.
GCS, Glasgow Coma Scale; LOC, loss of consciousness; CI, confidence interval; NLR, negative likelihood ratio; PLR, positive likelihood ratio.
Pooled estimates based on the following: data from one study only - observed data; data from two studies - a fixed effects meta-analysis conducted using the method of DerSimonian and Laird (1986); data from three or more studies - a full Bayesian meta-analysis conducted using the bivariate random effects method of Reitsma et al. (2005).
Credible interval if more than three studies meta-analyzed.
Significant heterogeneity, p-value<0.05.
The methodological quality of each included study was assessed using a modified version of the Quality Assessment of Diagnostic Accuracy Studies (QUADAS) tool (Whiting et al., 2003), a generic, validated, quality assessment instrument for diagnostic accuracy studies. A summary score estimating the overall quality of an article was not calculated, because the interpretation of such summary scores is problematic and potentially misleading (Juni et al., 1999; Whiting et al., 2005). The quality assessment items in QUADAS include the following: spectrum composition, description of selection criteria and reference standard, disease progression bias (this item was not applicable to this review as the reference standard was defined as CT or MRI within 24 h of admission), partial and differential verification bias, test and reference standard review bias, clinical review bias, incorporation bias (this item was not applicable to this review as the reference standard was always independent of the index test), description of index and reference test execution, study withdrawals, and description of indeterminate test results.
Data synthesis and analysis
Indices of test performance were extracted or derived from data presented in each primary study of each test. Two-by-two contingency tables of TP cases, FN cases, FP cases, and TN cases were constructed. Data from cohorts of children were analyzed separately. Data from cohorts of adults, mixed cohorts, and cohorts with no clear description of the age range included were analyzed together.
Individual clinical characteristics data that had been defined in a reasonably homogeneous and clinically meaningful way were selected and analyzed using three different approaches, where applicable. If data from only one study was available, no meta-analyses were undertaken, and the analysis produced estimates of sensitivity, specificity, negative likelihood ratio (NLR) and positive likelihood ratio (PLR), and corresponding 95% confidence intervals (CI). The latter were calculated assuming the statistics were normally distributed on the logit scale (sensitivity, specificity) and on the logarithm scale (NLR, PLR). The PLR is the proportion with the outcome (neurosurgery or intracranial injury) given the risk factor is “positive”, divided by the proportion without the outcome given the risk factor is “positive”, that is, the PLR is the odds for having the outcome, given a positive risk factor. By a similar argument, the NLR is the odds for having the outcome given a negative risk factor (Deeks and Altman, 2004). Therefore, the PLR and NLR are two potentially useful clinical diagnostic measures, depending upon whether a patient is risk factor-positive or risk factor-negative.
If there were data from two studies, a fixed effects meta-analysis was conducted using the DerSimonian and Laird method (DerSimonian and Laird, 1986), weighted by the inverse of study variance estimate, and, as before, estimates of sensitivity, specificity, NLR, PLR, and corresponding 95% CI. Note that the correlation between outcomes cannot be taken into account in this case as there was insufficient data.
For data from three or more studies, a full Bayesian meta-analysis was conducted. The bivariate random effects method of Reitsma and associates (2005) was used. The Bayesian approach was chosen because the between-studies uncertainty can be modelled directly, which is important in any random effects meta-analysis where there are small numbers of studies and potential heterogeneity. Correlation between sensitivity and specificity was modelled at the logit level and the correlation was modelled separately. In addition to the estimated sensitivity, specificity, NLR, PLR, and corresponding 95% credible intervals (CrI), results also included estimated heterogeneity (Q) statistics and corresponding p-values for sensitivity and specificity, calculated using a fixed-effects approach.
Results
Trial flow
Figure 1 summarizes the process of identifying and selecting relevant literature. Of the 8003 citations identified, 71 cohort studies met the inclusion criteria. Of these, 66 studies provided data for meta-analysis (40 studies provided data for adult brain injuries and 26 provided data for child and/or infant brain injuries)
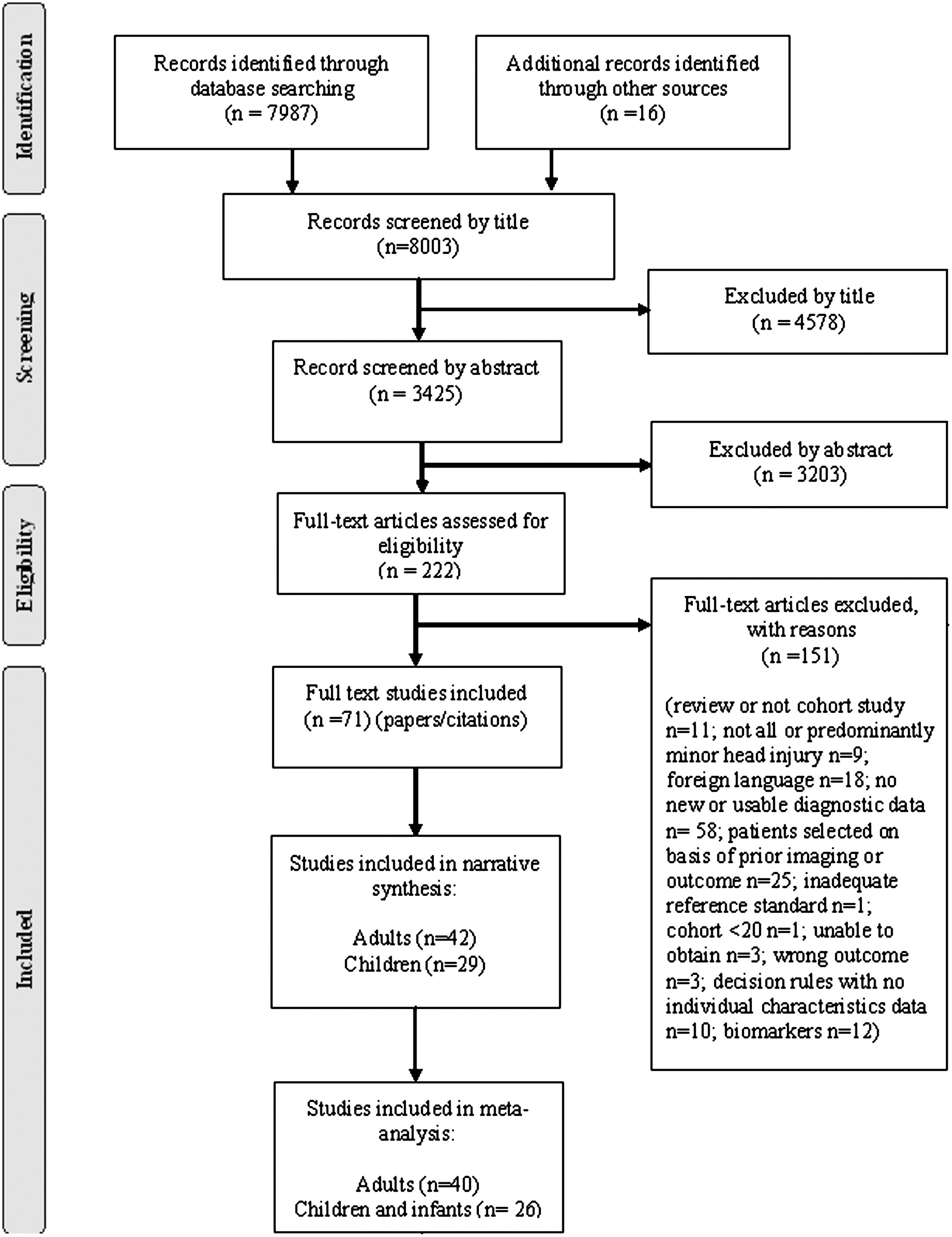
Diagnostic accuracy review–PRISMA (adapted) flow chart.
Study and patient characteristics
Full details of the 71 included studies are presented in Table S2 (Supplementary Data are available online at
Quality assessment
The overall methodological quality of the 71 included studies is summarized in Figure 2 (further details can be found in Table S3; Supplementary Data are available online at
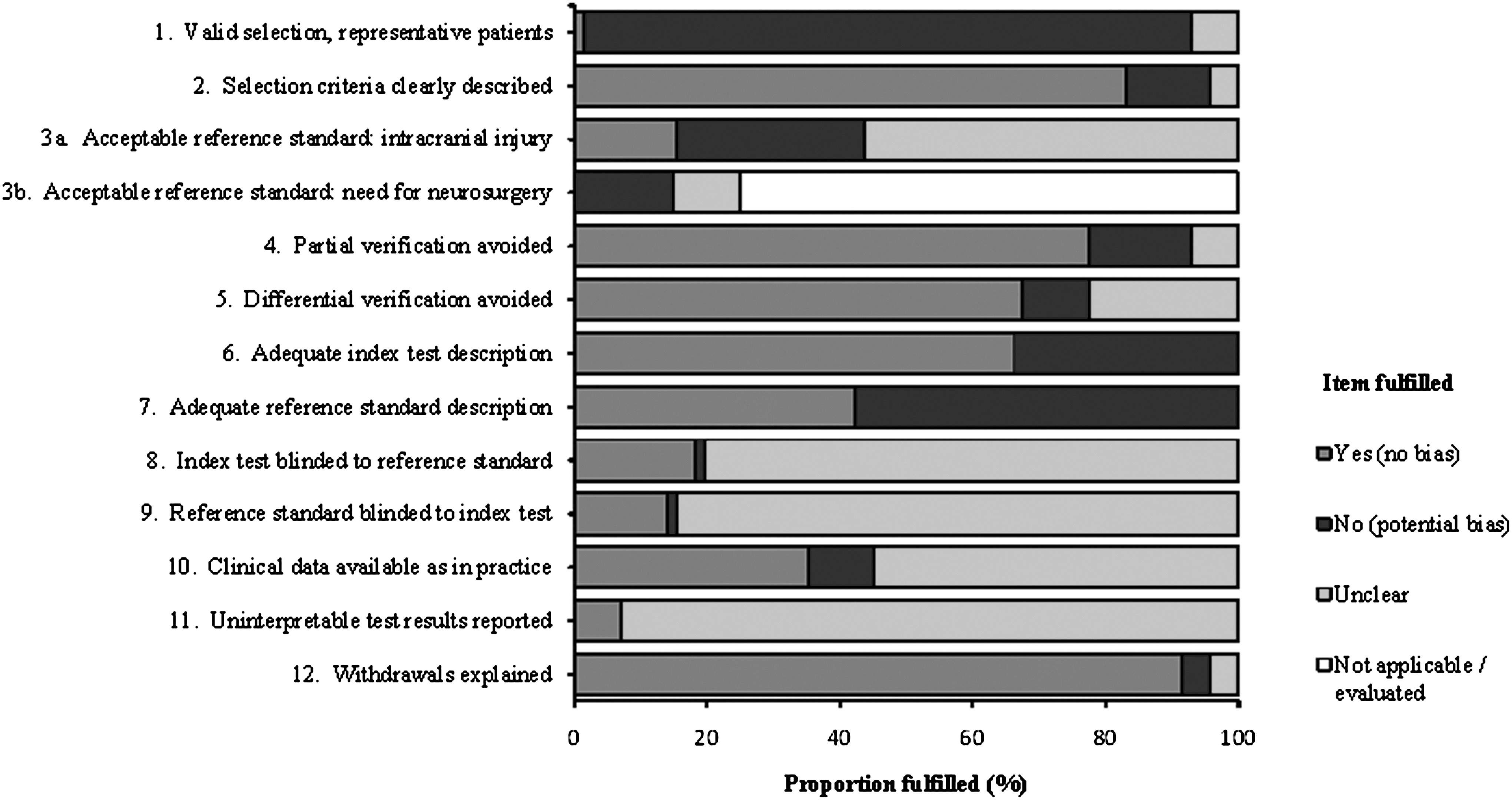
Summary of quality of 71 studies assessed by using the modified QUADAS tool (Whiting et al., 2003).
Diagnostic performance of individual characteristics
The results are summarized separately for adults, children and infants (data from individual studies are available from the authors).
Adults
Table 1 presents a summary of the pooled sensitivity, specificity, PLR, and NLR for each individual clinical variable for diagnosing intracranial injury in adults. Depressed, basal, or radiological skull fracture and post-traumatic seizure each substantially increased the likelihood of intracranial injury (PLR >10). Focal neurological deficit, persistent vomiting, decrease in GCS, and previous neurosurgery all markedly increased the likelihood of intracranial injury (PLR 5–10). However, the latter was only assessed in three studies (Arienta et al., 1997; Fabbri et al., 2005; Ibanez et al., 2004), was subject to significant heterogeneity, and had a CI for the PLR crossing 1. Fall from a height, coagulopathy, chronic alcohol use, age >60, pedestrian motor vehicle accident (MVA), seizure, vomiting, retrograde amnesia, and GCS<14 or GCS<15 moderately increased the risk of intracranial injury (PLR 2–5). Meanwhile, loss of consciousness and headache (even if severe) appear to be of little value in diagnosing intracranial injury. However, loss of consciousness is sometimes used as an inclusion criterion for studies; therefore, its diagnostic value may be underestimated. Only a few studies reported data specifically for neurosurgical injuries. Consequently, the results should be treated with caution; however, the diagnostic value of individual characteristics to diagnose neurosurgical injury does not appear to differ markedly from those of intracranial injury (Table 2).
Children
Table 3 presents a summary of the pooled sensitivity, specificity, PLR, and NLR for each individual clinical variable for diagnosing intracranial injury in children. The most useful clinical characteristics were depressed or basal skull fracture and focal neurological deficit (PLR >10). Coagulopathy, post-traumatic seizure, and previous neurosurgery (albeit in only one study with >20,000 children) (Dunning et al., 2006) all markedly increased the likelihood of intracranial injury (PLR 5–10). Visual symptoms, bicycle and pedestrian MVA, seizure, loss of consciousness, persistent vomiting, severe or persistent headache, anterograde or post-traumatic amnesia, GCS<14, GCS<15, intoxication, and radiological skull fracture all moderately increased the likelihood of intracranial injury (PLR 2–5). Meanwhile, headache (other than severe or persistent), scalp hematoma, and scalp laceration were not diagnostically useful. Only four studies (Hahn and McLone, 1993; Haydel and Shembekar, 2003; Schunk et al., 1996; Stein and Doolin, 1995) reported data (and examined a limited range of characteristics) for neurosurgical injuries. A summary of the results are presented in Table 4; however, the data should be treated with some caution. Although the absence of radiological skull fracture had some value for ruling out neurosurgical injury (NLR=0.504), GCS<14, seizure, headache, and vomiting each moderately increased the likelihood of neurosurgical injury (PLR 2–5).
Infants
Table 5 presents a summary of the pooled sensitivity, specificity, PLR, and NLR for each individual clinical variable for diagnosing intracranial injury in infants. Despite the limited number of heterogeneous studies, a depressed skull fracture or focal neurological deficit indicated a substantially increased risk of intracranial injury (PLR >10), whereas meta-analytical data suggested that radiological skull fracture, GCS<15 and any loss of consciousness moderately increased the likelihood of intracranial injury (PLR 2–5). More importantly, the failure to show diagnostic value for some characteristics may reflect the limitations of the data rather than a genuine lack of value. No studies reported data for neurosurgical injuries in infants with minor brain injury.
Discussion
This systematic review and meta-analysis found that most of the clinical characteristics we examined had some value (PLR >2) for diagnosing intracranial injury. Most notably, a depressed skull fracture, basal skull fracture, radiological skull fracture, post-traumatic seizure, focal neurological deficit, decrease in GCS, or persistent vomiting all indicated a markedly increased risk of intracranial injury in adults (PLR >5). Similarly, a depressed skull fracture, basal skull fracture, focal neurological deficit, coagulopathy or post-traumatic seizure markedly increased risk of intracranial injury in children and depressed skull fracture or focal neurological deficit in infants. Clinical characteristics of limited diagnostic value included loss of consciousness and headache in adults and scalp hematoma and scalp laceration in children. The failure to demonstrate diagnostic value of many characteristics for diagnosing neurosurgical injury probably reflects the limited data available for this outcome and should not be interpreted as showing that individual characteristics are of limited value. There are good theoretical reasons to anticipate that characteristics that are useful for diagnosing any intracranial injury will also be valuable for diagnosing specifically neurosurgical injury. Frequently used clinical characteristics, such as loss of consciousness, headache and vomiting, have been widely studied, although not always clearly defined. This may be important because clinical characteristics appeared to be more diagnostically useful when they were clearly defined and specified (for example, persistent vomiting as opposed to any vomiting). Other clinical characteristics, such as decreasing GCS, visual symptoms and specific mechanisms of injury, have been less widely studied. As a result, conclusions from only two or three studies should be treated with caution, particularly when the findings are inconsistent.
Certain limitations are inherent in meta-analysis (Higgins and Green, 2009), of which the most important relates to the synthesis of data from studies that may be heterogeneous. In our meta-analysis, a large amount of heterogeneity was found between the studies. This may be due to the prevalence of intracranial injury, which varied widely between studies and is likely to be caused by differences in the inclusion criteria, adequacy of reference standards, and definitions of intracranial injury. It could be argued that it is inappropriate to calculate a pooled LR in the presence of significant heterogeneity. However, not reporting a pooled estimate can make interpretation difficult and reduce the clinical value of a systematic review. The pooled LR estimate should therefore be regarded as a very general estimate of the diagnostic value of a characteristic that may actually vary substantially between settings and populations. Although an extensive literature search was conducted, it is possible that some relevant studies may have been missed. However, such omissions are likely to have been minimal, as the search included all identifiable publications in the gray literature (including contact with clinical experts in the field). Although two previous meta-analyses determined the relative risks of 23 clinical characteristics in adults (Dunning et al., 2004b) and 7 clinical characteristics in children (Dunning et al., 2004a), our analysis updates and expands the number of characteristics analyzed and presents the findings as LRs as they provide more clinically useful information (e.g., indicate the value of individual clinical features for ruling in or ruling out intracranial injury) and may help refine clinical judgement (e.g., help the clinician to assimilate clinical information during history-taking and examination, and estimate the risk of intracranial injury for the individual patient in a way that is potentially more flexible than the rigid application of a clinical decision rule) (Grimes and Schulz, 2005).
Clinical decision rules for minor brain injury are based upon individual clinical characteristics, with the presence of a criterion indicating the need for CT scanning (or hospital admission prior to the widespread use of CT). There is substantial variation in the criteria used by each rule (Harnan et al., 2011; Pickering et al., 2011) and it is interesting to examine the diagnostic value of each item, as estimated in our meta-analysis. Most adult rules use GCS<15, focal neurological deficit, loss of consciousness, vomiting, and amnesia. Our meta-analysis of these individual characteristics suggested that loss of consciousness has little diagnostic value, although this may reflect its use as a selection criterion in many studies. The other four criteria were supported by our meta-analysis, although vomiting was only useful if it was persistent, and most rules did not specify that vomiting had to be persistent. Many rules do not include suspected basal or depressed skull fracture, age, seizure, decreasing GCS, mechanism of injury, or coagulopathy as criteria. Our meta-analysis suggested that these could be useful criteria (or, at least, falling from a height and bicycle or pedestrian MVA were useful with regards to mechanism of injury). Conversely, several rules used headache as a criterion, whereas our meta-analysis suggested this was of limited diagnostic value.
Most rules for children use loss of consciousness, GCS<15, skull fracture, vomiting, headache, and visible injury as criteria. Our meta-analysis of the individual characteristics supported the use of loss of consciousness, GCS<15, skull fracture, vomiting, and headache (if severe or persistent), but suggested that scalp laceration/hematoma or an undefined headache were of little diagnostic value. Many rules do not use focal neurological deficit, amnesia, seizures, mechanism of injury, or coagulopathy as criteria. However, our meta-analysis suggested that these criteria were all potentially diagnostically useful. Overall the The Children's Head Injury Algorithm for the prediction of Important Clinical Events (CHALICE) (Dunning et al., 2006) and National Emergency X-Radiography Utilization Study II (NEXUS II) (Mower et al., 2005) rules appeared to be most consistent with the findings of our meta-analysis, in terms of including criteria that are diagnostically useful and excluding those that are not.
Conclusion
In conclusion, we have identified the clinical features that are most useful for identifying intracranial injury in adults, children, and infants with minor brain injury. These features can be used by clinicians to select patients for CT scanning and can be included in clinical decision rules used to guide decision making. We have also identified clinical features, such as headache in adults and scalp laceration or hematoma in children, which have little diagnostic value and therefore do not (if uncomplicated and an isolated finding) indicate a need for CT scanning.
Footnotes
Acknowledgments
We thank Fiona Lecky, Tim Coats, Jake Timothy, and David Hughes for providing clinical advice, Alex Sutton for providing statistical advice, and Joanne Turner for clerical assistance.
This project was funded by the United Kingdom National Institute for Health Research (NIHR) Evaluation, Trials and Studies Coordinating Centre (NETSCC) Health Technology Assessment (HTA) programme (grant number 07/37/08) as part of a larger review of management strategies for minor brain injuries. The views and opinions expressed therein are those of the authors and do not necessarily reflect those of the United Kingdom Department of Health.
Abdullah Pandor (APa) coordinated the review. Steve Goodacre (SG) was responsible for conception and design. Angie Rees (AR) developed the search strategy, undertook searches, and organized retrieval of articles. APa, SG, Susan Harnan (SH), and Alastair Pickering (APi) were responsible for the acquisition, analysis, and interpretation of data. Patrick Fitzgerald (PF) provided statistical support and undertook the meta-analyses. SG and APi helped interpret and provided a methodological, policy, and clinical perspective on the data. APa wrote the drafts of the manuscript, which were subsequently revised and approved by all authors. APa is the guarantor.
Author Disclosure Statement
No conflicting financial interests exist
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.