
Abstract
A proportion of patients surviving severe traumatic brain injury (TBI) have symptoms suggestive of excessive sympathetic discharge, here termed paroxysmal sympathetic hyperactivity (PSH). The goals of this study were: (1) to describe the clinical associations and radiological findings of PSH, its incidence, and features in subjects with severe TBI in the intensive care unit (ICU); (2) to investigate the potential role of increased intracranial pressure in the pathogenesis of PSH; and (3) to determine the prognostic influence of PSH during the ICU stay, on discharge from the ICU, and at 12 months post-injury. A prospective cohort study was undertaken of all ICU admissions with severe TBI older than 14 years over an 18-month period. The PSH symptoms consisted of paroxysmal increases in blood pressure, respiratory rate, and heart rate; worsening level of consciousness; muscle rigidity; and hyperhidrosis. Subjects demonstrating PSH episodes were compared with a group of non-PSH consecutive subjects studied over the first 6 months of the study period. Data were recorded on the clinical variables associated with PSH episodes, early post-injury cerebral CT findings, and neurological status at 1 year. Of 179 severe TBI patients admitted over the study period, 18 (10.1%) experienced PSH. Injury severity-related variables (e.g., initial APACHE II score, admission coma level, and proportion with intracranial hypertension) were similar between the two groups. The PSH group had a longer ICU stay and a greater incidence of infectious complications. At 1 year post-injury, 20% of this group demonstrated ongoing PSH episodes. Over 18 months, 10.1% of admissions following severe TBI demonstrated PSH features in ICU. Subjects with PSH had a longer ICU stay and higher rate of complications, although this did not appear to compromise their long-term neurological recovery.
Introduction
A
The suggested pathophysiological mechanisms behind PSH have included epileptiform discharges in the diencephalon (Bhigjee et al., 1985), increased intracranial pressure (ICP) (Carmel, 1985; Goddeau, 2007; Talman et al., 1988), and disconnection syndromes with lesions of the inhibitory efferent pathways from cortical and/or subcortical areas (Blackman et al., 2004; Boeve et al., 1998; Bullard, 1987; Thorley et al., 2001). More recently, the excitatory-inhibitory ratio model suggests that a lesion in the mesencephalic region reduces descending inhibition, resulting in normally non-nociceptive afferent stimuli from the periphery becoming nociceptive, with resultant over-excitation of the peripheral sympathetic nervous system (Baguley, 2008).
Accordingly, the aims of this study were to: (1) describe the clinical associations and radiological findings of PSH, its incidence, and features in patients with severe TBI in the intensive care unit (ICU); (2) investigate the potential role of intracranial hypertension (ICH) in the pathogenesis of PSH; and (3) determine the prognostic influence of PSH in the ICU setting, on discharge from the ICU, and at 12 months post-injury.
Methods
Patient inclusion and exclusion
The study complied with the Data Protection and Patient Rights Law and was authorized and monitored by the hospital bioethics committee. Following the provision of informed consent (from the patient or their legal representative), consecutive ICU admissions following severe TBI (defined as a Glasgow Coma Scale [GCS] score of 8 or less following non-surgical resuscitation, or a score of 8 or less during the first 48 h after injury; Marshall et al., 1983) older than 14 years were assessed over an 18-month period. To maximize consistency within the results, ICU diagnostic and therapeutic protocols were not modified over the 18-month period. Subject numbers resulting from the selection process are shown in Figure 1. Thirty-two of 211 consented subjects were excluded, as they received infusion of drugs that could favor over-interpretation of the signs and symptoms of PSH, namely: (1) noradrenaline (NA) infusion at doses ≥0.5 μm/kg/min and/or dopamine at doses of ≥5 μm/kg/min; (2) systemic glucocorticoids before or during the ICU admission; and (3) thyroid replacement or inhibitor drugs.
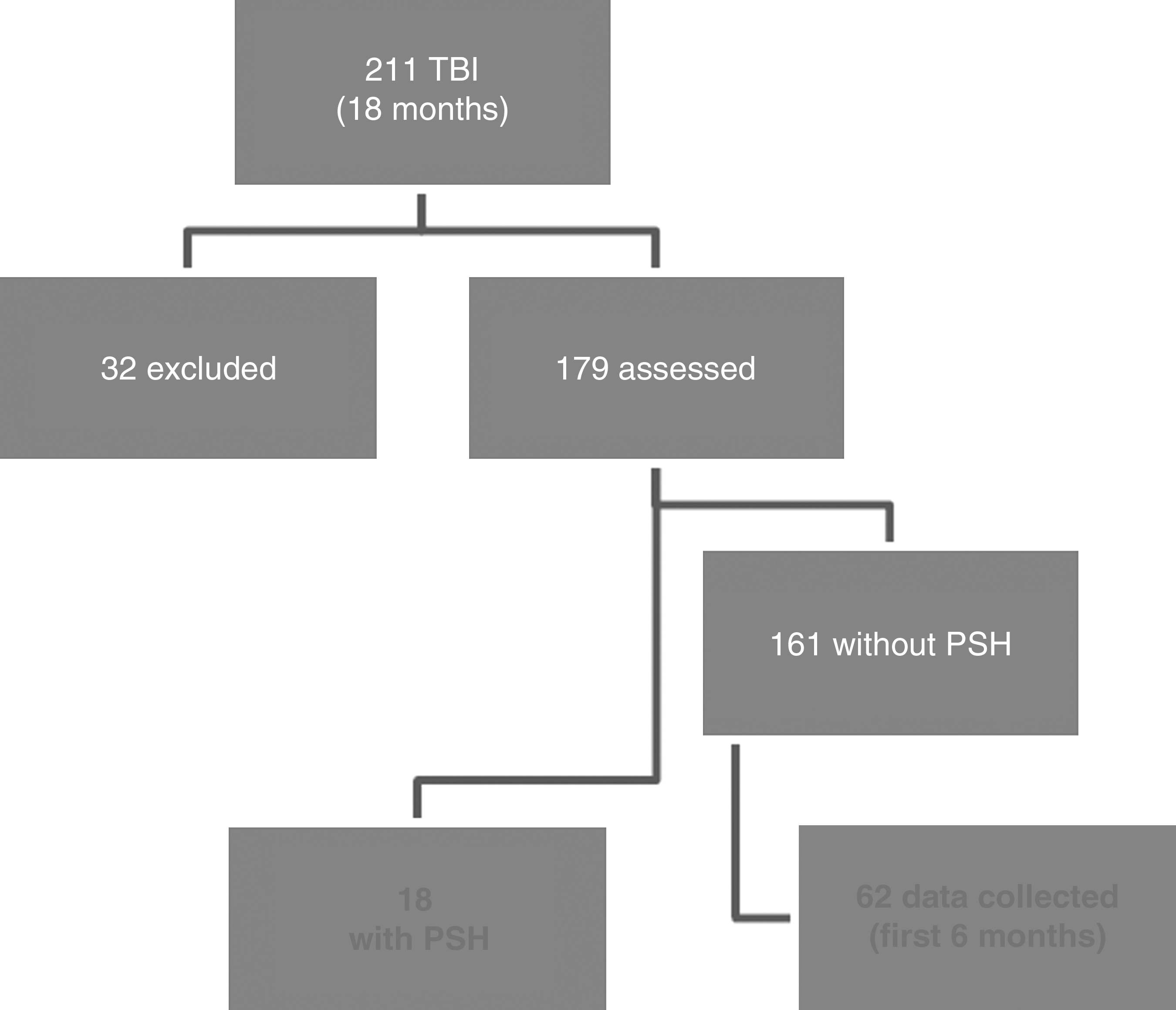
Selection process for the two study groups (PHS, paroxysmal sympathetic hyperactivity; TBI, traumatic brain injury).
All remaining subjects were assessed for the development of PSH during their ICU admission using a previously published protocol (Fernandez-Ortega et al., 2006), namely, short episodes of at least 5 of the 8 following signs and symptoms: (1) tachycardia; (2) arterial hypertension,; (3) tachypnea; (4) reduced level of consciousness; (5) muscle rigidity; (6) fever; (7) hyperhidrosis; and (8) pupillary dilation. These parameters had to be abrupt and simultaneous, and not otherwise explainable. Episodes that could be related to an intercurrent disorder (e.g., fever in cases of sepsis according to the criteria of the American College of Chest Physicians, Society of Critical Care Medicine [Bone et al., 1992], pupillary dilation in cases of brain herniation, or arterial hypertension and tachypnea as a result of the abrupt withdrawal of sedative drugs) were not included. The PSH group was compared to a control group consisting of consecutive admissions without PSH during the first 6 months of the 18-month study period. In the control group, we chose patients from the first 6 months to make the two groups similar in size. Over the 18-month study period, there were no changes in the treatment protocols or in admission strategy, and the demographic and clinical characteristics of patients did not change.
Data collection
Data were recorded for the 18 PSH and 62 non-PSH subjects. Data included epidemiological and injury characteristics, including age, sex, GCS score, Injury Severity Score (ISS), pre-hospital hypoxia or hypotension, non-CNS organ involvement, clinical management data (Acute Physiology, Age, and Chronic Health Evaluation II [APACHE II] scores during the first 24 h), computed tomography (CT) findings during the first 48 h, the need for surgical intervention (e.g., continuous ICP monitoring, emergency neurosurgery, or tracheostomy), the presence of ICH, number and type of infections, and GCS score at the time of ICU discharge. Cerebral CT scans were undertaken on admission and again at least once during the first 48 h. Radiological findings were considered to be the sum of the two imaging studies. The validated Gennarelli classification system (Gennarelli et al., 1982) was selected, as it affords a combination of clinical and imaging data. Scoring was undertaken by a single observer unaware of the identity of the subject. Radiological findings were aggregated into focal and diffuse groups to improve statistical power, the former corresponding to lesions of grades 1 to 4, and the latter to grades 5 to 7.
The characteristics of PSH episodes were recorded as the number and duration of episodes per day, the 24-hour mean values for physiological variables and GCS scores, and as a categorical “yes/no” response for the presence of muscle rigidity, fever, hyperhidrosis, and pupillary dilation. Clinical outcome 1 year post-injury was assessed using the Glasgow Outcome Scale (GOS; Becker et al., 1977), which was obtained by telephone interview with either the patient or a first-degree relative. Consistent with research done over the last 3 decades (Jiang et al., 2002; Robertson et al., 1999; Saul and Ducker, 1982). GOS data were dichotomized into those with a favorable GOS score (GOS score 4 or 5), or an unfavorable score (GOS score 2 or 3) for subjects surviving to discharge from the ICU.
Statistical analysis
Study variables were recorded in a computerized database and analyzed with SPSS v 15.0 for Windows (SPSS Inc., Chicago, IL). Outcome at ICU discharge and at 12 months were analyzed after excluding subjects who died in the ICU to reduce underestimation of variables such as ICU stay, tracheotomy, and infection rates. Between-group comparisons were performed with parametric or non-parametric techniques as appropriate. The quantitative variables are expressed as means±standard deviation (mean±SD). The qualitative variables are expressed as frequency or percentage of incidence. The comparison between groups was done with the Student's t-test for quantitative variables. To compare the means of independent samples, we used the Levene test to analyze homoscedasticity, or the non-parametric Mann-Whitney U test (for admission APACHE II score, ISS, number of organ systems affected, neurological severity data, and ICU and hospital stay). In the case of categorical variables, between-group comparisons were done with the chi-square test or Fisher's exact test. In all cases, significance was set at p<0.05. Multiple linear regression (MLR) was used to delineate the length of ICU stay and the period of mechanical ventilation after excluding patients who died.
Based on the variable of interest (ICU-stay), the sample size used in our study ensured a power of 80%, assuming a 95% confidence interval.
Results
Demographic data and severity parameters
The results of the demographic variables and the parameters of general and neurological severity for both groups are shown in Table 1. The age, sex, ISS and APACHE II scores at admission were similar in controls and PHS patients during the 18 months of the study (data not shown). Subjects with PSH were younger and more likely to be male, but there were no other statistically significant differences for the other clinical variables. In the control group (without PSH), the ratio of males to females was also significant (p<0.001). In addition, the percentage of males without PSH was similar between the control group and the total group (75.8% versus 72.3%). Our ICU has an established sedation protocol for TBI patients. This includes an opiate of short duration and propofol, both given via perfusion, to obtain the desired level of consciousness.
Data are presented either as mean and standard deviation (SD) or as frequency counts.
NS, not significant; GCS, Glasgow Coma Scale; ICP, intracranial pressure; ICH, intracranial hypertension; APACHE II, Acute Physiology, Age, and Chronic Health Evaluation II; PSH, paroxysmal sympathetic hyperactivity.
Table 2 shows the results of cerebral CT data based on the Gennarelli scale. While the PSH group tended to have more focal lesions than the non-PSH group, this result did not reach significance.
The Gennarelli classification categorizes severe TBI based on the Glasgow Coma Scale (GCS) (a: GCS 3–5, b: GCS 6–8) and the type of CT injury, corresponding to focal lesions 1–4 (extradural, subdural, and other focal lesions), and diffuse brain injury 5–7.
PSH, paroxysmal sympathetic hyperactivity.
Clinical characteristics of the PSH episodes
The onset of clinical episodes of PSH occurred a mean of 5.9 days (SD 3.7 days) post-injury. On two occasions, the subject's PSH only became manifest once the infusion of neuroblocking agents was ceased. Table 3 details the clinical manifestations of the subjects in the PSH group during and between episodes. Mean episode duration was 30.8 min (range 15–50 min) for an average of 5.6 (range 3–8) episodes per day. PSH episodes were observed to be triggered by external stimuli in 13 subjects (72%). All subjects in the PSH group continued to experience paroxysms on discharge from the ICU, with 80% of these resolved at the 12-month review. ICP was measured during and between episodes in 8 subjects, with no subject showing an elevation in ICP during the PSH crisis. Sixteen patients (89%) received treatment with a combination of clonidine (83%), beta blockers (33%), and opiates (55%), depending on individual physician preference.
Data are presented as mean and standard deviation (SD) or as frequency counts.
PSH, paroxysmal sympathetic hyperactivity.
Prognostic course of PSH and non-PSH groups
Details of the clinical progress and follow-up data of the two groups are shown in Table 4. No deaths were recorded in the PSH group. The 15 deaths in the control group all occurred during the first 96 h of admission to the ICU. Of these, 6 resulted from brain death secondary to the TBI, and 9 were due to trauma-related non-CNS injuries. Consequently, 12-month follow-up data were sought for 47 subjects in the non-PSH group.
Notes: data is presented either as mean and standard deviation (SD) or as frequency counts.
PSH, paroxysmal sympathetic hyperactivity; GCS, Glasgow Coma Scale; LOS, length of stay; GOS, Glasgow Outcome Scale; NS, not significant; ICU, intensive care unit.
The clinical course of the PSH group was characterized by more time on mechanical ventilation, more infections and tracheotomy placement, and longer ICU stay and a greater total period of hospitalization. Despite these differences, no significant differences were seen between the two groups in terms of GCS score at discharge from ICU or 12-month GOS status.
The subgroup of patients with chest trauma had a longer period of mechanical ventilation than patients without chest trauma (11 versus 6.4 days, p=0.019). There were no differences in the period of mechanical ventilation related to the presence or absence of abdominal trauma. The presence of PSH and the presence of chest trauma were independently associated with days on mechanical ventilation (p=0.021 for chest trauma and p=0.001 for PSH), and ICU stay (p=0.002 for chest trauma and p=0.001 for PSH).
Discussion
This prospective cohort study recruited consecutive ICU admissions with severe TBI over an 18-month period to compare subjects with PSH to a non-PSH group recruited over the first 6 months of the same period. Subjects in both groups were young, a finding typical of patients with severe TBI (Centers for Disease Control and Prevention, 1997). However, the PSH group was significantly younger than the control group, a finding consistent with most (Baguley et al., 1999; Cuny et al., 2001; Rabinstein 1997), but not all previous studies (Baguley, 2007). Also in keeping with previous TBI research, there was a 3:1 ratio of males to females in the non-PSH group (Suárez-Álvarez et al., 1995). However, it was notable that only males were identified with PSH (p<0.05), consistent with previous research by our group (Fernández-Ortega et al., 2004). The predominance of males across our two series may be related to the relatively low number of subjects in our studies, or may be a consequence of putative sex differences in TBI recovery (Slewa-Younan, 2008), as they relate to the pathophysiological mechanism underlying PSH. However, there is currently no rational basis to explain the over-representation of males experiencing PSH.
The 10.1% incidence of PSH seen in this study is consistent with previous estimates of 8% (Baguley et al., 2007) and 10.5% (Hendricks et al., 2007) in similar cohorts following TBI. However, other studies have reported incidence rates up to 30% (Dolce et al., 2008; Rabinstein, 2007). The pathophysiology of PSH has yet to be precisely defined, especially in terms of its clinical manifestations and pattern of acute neurological damage. Blackman and associates proposed alternative criteria to diagnose the PSH complex, in what they termed “paroxysmal autonomic instability with dystonia” (Blackman et al., 2004). The criteria were very similar to those proposed by Hendricks and colleagues (Hendricks et al., 2007), while Rabinstein and co-workers (Rabinstein, 2007) required four simultaneous criteria for the diagnosis. Thus the wide range in incidence is likely to be due to the different methodologies and diagnostic criteria employed (Perkes et al., in press).
The current study utilized a more comprehensive procedure for measuring and analyzing PSH than many previous studies, identifying significant increases in heart rate and respiratory rate and reduced GCS scores during PSH episodes compared to between-episode values. The increase in heart rate and respiratory rate did not respond to a low blood pressure or an increase in CO2, but were an independent response that did not improve the physiological parameters of perfusion or ventilation. In addition, muscle rigidity, sweating, fever, and pupillary dilatation were significantly more frequent during PSH paroxysms. This approach excludes non-paroxysmal rises potentially due to other etiological causes. In addition to the clinical manifestations that constitute the syndrome, other characteristics of the syndrome were identified: its paroxysmal nature, a physiologically recordable over-reactivity to non-nociceptive stimuli (Baguley et al., 2009), the number of presentations during the day, and its time of onset in relation to the TBI. We believe these characteristics are all determining elements for diagnosis.
In this series, PSH onset was usually around the fifth day post-TBI, except for two cases receiving prolonged intravenous perfusion of neuroblocking agents, in whom the onset occurred later. This is consistent with other studies that have examined patients from the time of hospital admission (Baguley et al., 1999; Goddeau et al., 2007; Hendricks et al., 2007; Wang and Manley, 2008). Conversely, studies within the subacute TBI rehabilitation phase report greater onset latencies (Baguley et al., 2008). Once established, subjects presented with a mean of 5.6 episodes daily, lasting for a mean of 30 min. To date, most publications have omitted this information, instead providing qualitative data of the self-limiting and repetitive nature of the episodes throughout the day (Baguley et al., 1999,2009; Boeve et al., 1998). Where data have been reported, episode durations have been reported to be a few minutes (Srinivasan et al., 2007) up to 2 h (Goddeau et al., 2007). In our ICU a protocol of sedation is used in patients with severe TBI, and is similar in patients with or without PSH. These episodes, therefore, are not likely to be attributable to changes in or withdrawal of sedative medications. While PSH episodes continued in all subjects on discharge from the ICU, the episodes had resolved in 80% of subjects by 12-month follow-up, supporting the observation of the spontaneous disappearance of paroxysms over time (Baguley et al., 1999). Further research is required to better quantify the frequency, severity, and duration of paroxysmal episodes.
This study adds data to the debate regarding the pathophysiology of PSH. Previous evidence suggests that an epileptogenic etiology for PSH is unsupported (Baguley et al., 2008). In the current study we assessed the potential role that ICH may play in the pathogenesis of PSH. The PSH subjects in this series did not demonstrate a greater frequency of ICH compared to non-PSH subjects, nor was there an increase in ICP observed during PSH episodes in this group. These findings are consistent with and extend the findings of Klug and associates (Klug et al., 1984). Consequently, it appears unlikely that ICH and ICP play a role in the pathogenesis of PSH.
Data in this study were less helpful regarding the potential impact of intracerebral pathology and the development of PSH. This is particularly relevant, as the third group of pathophysiological theories of PSH suggest that intracerebral lesions could alter neuroendocrine modulation. However, there were no significant associations between CT data and PSH onset in this study. Consistent with previous studies (Rabinstein, 2007), there was a non-significant tendency for there to be more focal lesions in the PSH group. However, other studies have reported a significant presence of diffuse lesions in PSH (Baguley et al., 1999, 2008), or very heterogeneous lesions in both intra- and extracerebral structures (Baguley et al., 2007). Recent research suggests that almost all TBI patients have a degree of diffuse injury regardless of the presence of focal structural lesions (Jing Zang et al., 2010). Hypothetically, many disconnection theories invoke a pathophysiological link with diencephalic damage (Diesing and Wijdicks, 2006), and MRI may help localize the functional mechanism that triggers these symptoms, as it is more sensitive for the detection of skull-base lesions than CT (Lv et al., 2010). Furthermore, more sophisticated imaging tools such as diffusion tensor imaging, functional MRI, or positron emission tomography, may have a role in providing evidence of the causality of PSH.
The ICU admission characteristics of the PSH and non-PSH groups were similar in terms of neurological group severity at the time of admission. Likewise, extra-neurological severity, percentages of extra-neurological organs affected, and percentages of abdominal trauma were all similar, as was the percentage of chest trauma. When considering subjects who survived to discharge from the ICU, the PSH group evidenced greater ICU morbidity, as measured in terms of longer duration of mechanical ventilation, higher prevalence of infections, greater mean length of stay, and a higher tracheotomy rate. The subgroup with chest trauma required more prolonged mechanical ventilation than the patients without chest trauma. After multiple linear regression analysis, both the presence of PSH and chest trauma were independently associated with mechanical ventilation and ICU stay. These results are very similar to research published in other acute TBI settings (Baguley et al., 1999,2007; Hendricks et al., 2007). While all 15 deceased subjects were in the non-PSH group, the deaths occurred prior to the possible onset of PSH, and so it cannot be ruled out that non-PSH subjects who died soon after admission might have developed PSH had they survived. We are unable to determine other reasons to explain the worse initial course of these patients apart from the presence of PSH.
No significant differences were observed between the two groups in terms of level of consciousness at discharge from ICU or GOS status at 12 months. At the time of discharge from the ICU, mean GCS scores were similar between groups; however, the PSH group had a poorer neurological evolution. Slower neurological recovery has been reported in the subacute setting, in which the PSH group took considerably longer to reach a similar degree of functional recovery compared to the non-PSH group (Baguley et al., 1999). At 12 months, dichotomized neurological recovery was similar in the two groups, with around 75% of subjects attaining a favorable outcome. Our results contrast with those of other researchers (Baguley et al., 1999; Srinivasan et al., 2007), who found a similar initial evolution in the two groups, and worse medium- and long-term evolution in PSH-affected patients. The reasons for the observed between-study differences in subacute outcome have yet to be adequately explored.
Strengths of this study include the consecutive nature of case selection and the use of published diagnostic criteria to identify cases of PSH. Furthermore, this study is one of a limited number of studies that have used a control group to examine the prognostic impact of PSH episodes (Baguley et al., 1999; Fernández-Ortega et al., 2004; Hendricks et al., 2007; Rabinstein, 2007). The relative rarity of PSH limited the overall sample size, which in turn may have reduced the already low sensitivity of the GOS score as an outcome tool. Furthermore, the use of the Gennarelli classification system and CT data potentially reduced the study's capacity to identify patterns of PSH-causative lesions.
Limitations of this study include the exclusion of patients without PSH after the first 6 months. This was done to make both groups similar in size because of the rarity of PSH. The 99 patients admitted between months 7 and 18 had a similar age, sex, APACHE II score, and ISS at admission as the patients admitted during the first 6 months. However, although the treatment protocols remained unchanged throughout the entire 18-month period, it is not possible to confirm the similarity of the groups. We did not analyze the effects of different treatments for PSH because this study was not interventional, and furthermore, we believe that no effective drugs are available to treat this complication. Drugs used include bromocriptine (Russo and O'Flaherty, 2000), morphine, and baclofen, but no definitive results about their usefulness are available. Further studies will therefore be necessary to seek the best treatment for this complication. The number of patients with PSH was reduced, which is a limitation with regard to the drawing of conclusions about the anatomical localization of lesions that produce the PSH episodes. The use in the future of MRI or positron emission tomography to study this complication, or multi-center studies to increase the number of recruited patients, could help determine the pathophysiology of PSH and help develop new treatment strategies. Finally, with a larger number of patients, we could use different measures of quality of life, and thus determine whether these patients have a similar prognosis 1 year after TBI.
In conclusion, PSH after severe TBI is a poorly-understood syndrome, with an incidence of around 10%. In the ICU, episodes were approximately 30 min in duration and occurred 5.6 times a day. The diagnosis of PSH requires general parameters such as a history of severe TBI, time and sequence of presentation, and clinical manifestations of sympathetic and motor overactivity. Data from this study suggest that elevated ICP is not associated with PSH episodes, and no specific radiological features were found to be associated with the occurrence of PSH. There is general agreement between studies that PSH is associated with a worse course during the initial weeks after a severe TBI; however, the impact of PSH on late outcomes after severe TBI is less clear. The capacity to quantify PSH episodes presents an opportunity to assess treatment efficacy in future research.
Footnotes
Author Disclosure Statement
No competing financial interests exist.