
Abstract
Changes in the demographics, approach, and treatment of traumatic brain injury (TBI) patients require regular evaluation of epidemiological profiles, injury severity classification, and outcomes. This prospective multicenter study provides detailed information on TBI-related variables of 508 moderate-to-severe TBI patients. Variability in epidemiology and outcome is examined by comparing our cohort with previous multicenter studies. Additionally, the relation between outcome and injury severity classification assessed at different time points is studied. Based on the emergency department Glasgow Coma Scale (GCS), 339 patients were classified as having severe and 129 as having moderate TBI. In 15%, the diagnosis differed when the accident scene GCS was used for classification. In-hospital mortality was higher if severe TBI was diagnosed at both time points (44%) compared to moderate TBI at one or both time points (7–15%, p<0.001). Furthermore, 14% changed diagnosis when a threshold (≥6 h) for impaired consciousness was used as a criterion for severe TBI: In-hospital mortality was<5% when impaired consciousness lasted for<6 h. This suggests that combining multiple clinical assessments and using a threshold for impaired consciousness may improve the classification of injury severity and prediction of outcome. Compared to earlier multicenter studies, our cohort demonstrates a different case mix that includes a higher age (mean=47.3 years), more diffuse (Traumatic Coma Databank [TCDB] I–II) injuries (58%), and more major extracranial injuries (40%), with relatively high 6 month mortality rates for both severe (46%) and moderate (21%) TBI. Our results confirm that TBI epidemiology and injury patterns have changed in recent years whereas case fatality rates remain high.
Introduction
T
The stagnating mortality rates may be related to ongoing changes in epidemiology patterns of TBI. The higher age of the general population is mirrored in an increase in older patients with TBI (Maas et al., 2008). As older age is associated with poorer outcome (Hukkelhoven et al., 2003), this trend may neutralize effects of improved patient management. Other developments, such as the emergence of strict safety laws, probably also contribute to changing epidemiological profiles of TBI. For example, traffic accidents are decreasing and falls are increasing as causes of injury (Maas et al., 2008).
Comparing outcome among studies and over time is complicated by variability in injury severity classification. The definition of severe TBI varied considerably in different multicenter observational studies (Jennett et al., 1977; Marshall et al., 1983; Murray et al., 1999a,b; Myburgh et al., 2008; Rusnak et al., 2007). In addition, the accuracy of the Glasgow Coma Scale (GCS) as an instrument to grade injury severity has been challenged. A growing use of sedatives and neuromuscular blocking agents in the pre-hospital setting results in more patients with artificially low GCS scores at hospital admission (Stocchetti et al., 2004) and weakens the predictive value of the GCS score (Balestreri et al., 2004).
Trends as described here emphasize the importance of continuous evaluation of TBI epidemiology and outcome. In a multicenter prospective observational cohort study, we collected detailed data on demography, injury patterns, management, and outcome of moderate and severe TBI in the Netherlands. This article describes the epidemiological profile of the investigated cohort and findings are compared with earlier multicenter series to detect support for some of the trends in epidemiology and outcome suggested in the literature. In addition, we aimed to examine variability in injury severity diagnosis based on clinical evaluations at three different time points in relation to pre-hospital interventions, intracranial pathology, and outcome.
Methods
Study sites
The Prospective Observational COhort Neurotrauma (POCON) study was executed in 5 out of 11 specialized (Level I) trauma centers in the Netherlands. These hospitals are the only Dutch centers using helicopters to transport their mobile medical team (MMT).
In all participating centers, patients were assessed on emergency department (ED) admission according to Advanced Traumatic Life Support (ATLS®) principles. In each center, protocols were available for treatment of patients with severe TBI, based on international guidelines issued by the Brain Trauma Foundation (BTF) (Brain Trauma Foundation, 2007).
Inclusion criteria
Between June 1 2008 and May 31 2009, all patients with TBI and an ED admission GCS score ≤13 were included. When intubated at the injury scene, the GCS score obtained before intubation (≤13) was used as a qualifier to determine eligibility for study inclusion. Exclusion criteria were age<16 years and hospital admission>72 h after injury.
Data collection and definitions
Data were collected from medical records by trained research staff supervised by a physician. Data were (anonymously) entered into stand alone databases, available at each individual center. Demographic variables and injury characteristics included age, gender, medical history, injury mechanism, alcohol intoxication (yes=serum ethanol level ≥0.5% suspected=on clinical grounds), drug intoxication (yes=based on clinical observations, eye-witness reports, or confirmed by laboratory tests). Patient characteristics at injury scene and ED included: GCS score, pupil reactions (both reacting, one non-reacting, both non-reacting), hypotensive episode (yes=systolic blood pressure<90 mm Hg, suspected=on clinical grounds), hypoxic episode (at injury scene or ED, yes=SaO2<90% or PaO2<8 kPa, suspected=on clinical grounds), glucose (mmol/L), and hemoglobin (g/dL). Severity scores included the Injury Severity Score (ISS) and Abbreviated Injury Scores (AIS). Major extracranial trauma was defined as AIS ≥3 (injury requiring hospital admission) in one or more body regions other than the head.
The following treatment and hospital stay variables were collected: referral (direct or secondary), intubation (at injury scene, in ED, or before operation), length of hospital and intensive care unit (ICU) stay, operations (both intra- and extracranial surgery), insertion of an ICP-monitor, sedation, and mechanical ventilation at the intensive care unit (ICU). Brain specific treatments: osmotherapy (mannitol or hypertonic saline), vasopressive medication to maintain CPP (not registered if administered for systemic blood pressure support), hyperventilation (yes if PaCO2≤4 kPa or no if PaCO2>4 kPa, treatment was registered when documented in medical records as ICP treatment), cerebrospinal fluid (CSF) drainage, hypothermia (body temperature<35°C), and use of barbiturates. Increased ICP was defined as any period with a measured ICP>20 mm Hg.
The first acquired CT scan was assessed. If not available, the second CT scan was scored, provided that it was obtained within 6 h after the initial scan and prior to neurosurgical interventions. Each CT scan was scored by one of three raters (T.M.J.C.A, B.J., P.E.V.) using a standardized data sheet described before (Jacobs et al., 2010a, b, 2011). For each scan, the TCDB CT classification and the Rotterdam CT score were determined (Maas et al., 2005; Marshall et al., 1991a) and the following individual variables were recorded: subdural hematoma (SDH), epidural hematoma (EDH), contusions, hemorrhagic contusions, intraparenchymal hematoma, subarachnoid hemorrhage (SAH), microbleeds (maximum diameter of 5 mm), diffuse edema, midline shift, and the status of the ambient cisterns and the fourth ventricle.
Injury severity classification
Clinical injury severity was based on the GCS score at admission to the ED of the participating hospital and defined as severe (GCS 3–8) or moderate (GCS 9–13). To address the question if the diagnosis depended upon the moment of assessment, we also classified injury severity at the injury scene (severe=GCS 3–8 at scene, mild/moderate=GCS 9–15, unknown=GCS unavailable) and by the moment of return to consciousness (severe=≥ 6 h, moderate=< 6 h or GCS never ≤8). Time to return to consciousness was calculated from the moment the patient scored a GCS ≤8 until the moment of obeying commands (GCS motor score >5) or producing words (GCS verbal score >2).
Guideline compliance
We assessed BTF guideline compliance for intubation and ICP monitoring. Pre-hospital endotracheal intubation is advised in patients with a pre-hospital GCS score ≤8 (Badjatia et al., 2008). Monitoring of ICP is recommended in patients with severe TBI when a CT reveals intracranial pathology, or in the presence of two or more of the following criteria: age >40 years, unilateral or bilateral motor posturing (here defined as an ED Motor score ≤3), or systolic blood pressure<90 mm Hg (Bratton et al., 2007).
Outcome assessment
In-hospital mortality and the discharge location were collected from medical files. Six and 12-month outcome was assessed with the Glasgow Outcome Scale Extended (GOSE), an 8-point scale classifying functional outcome from 1 (dead) to 8 (good recovery). GOSE scores were determined through a postal questionnaire or structured telephone interviews. Both methods have been validated (Wilson et al., 1998, 2002).
Protocol approval and patient consent
The study protocol was approved by the ethics committee of the coordinating hospital (Radboud University Nijmegen Medical Center). The other participating hospitals all provided a feasibility statement. After discharge, surviving patients (or their proxy) received a letter providing information about the study, inviting patients to contact the centers' local physician or the study coordinator if they had any objections against being contacted for follow-up. For follow-up through telephone interview, oral informed consent was obtained, and in case of outcome assessment through postal questionnaires, we gained written informed consent.
Statistical analysis
Data were analyzed using SPSS version 16.0. Mostly descriptive data will be presented. Differences in mortality rates and in the proportion of abnormal CTs between different categories of injury severity were calculated using Pearson χ2 tests. A p<0.05 was considered significant. The International Mission for Prognosis and Analysis of Clinical Trials in TBI (IMPACT) prediction rule was used to calculate the probability of death at 6 months post-injury. Where possible, the full laboratory model was used. In case of insufficient data, probability of death was calculated using either the extended or the core model (Steyerberg et al., 2008).
Results
Demography, injury severity, and CT findings
We included 508 patients (70% male, mean age 47.3 years), 335 (67%) with severe and 169 (34%) with moderate TBI (Fig. 1). Patient and injury characteristics are shown in Table 1. The average age of patients involved in a road traffic accident (RTA) was lower (mean 42.8, SD 20.0 years) compared to falls (mean 55.8, SD 19.0 years). More than one-third (38%) of the falls were from the stairs. Falls from>3 m were the most common injury mechanism in work-related accidents (n=22, 69%).
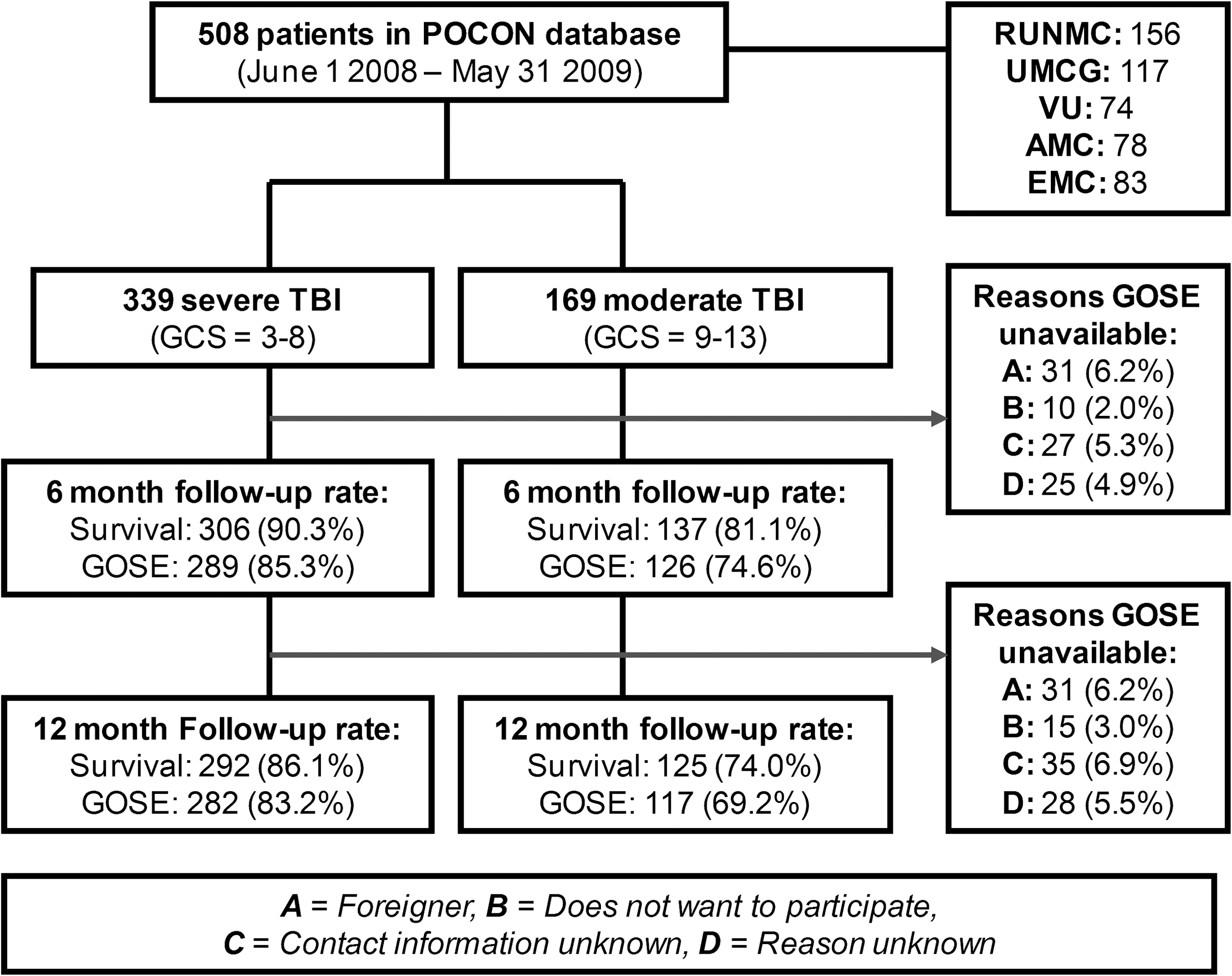
Patient inclusion and follow-up rates. POCON, Prospective Observational COhort Neurotrauma; AMC, Academic Medical Center, University of Amsterdam; EMC, Erasmus Medical Center Rotterdam; GCS, Glasgow Coma Scale; GOSE, Glasgow Outcome Scale Extended; RUNMC, Radboud University Nijmegen Medical Center; TBI, traumatic brain injury; UMCG, University Medical Center Groningen; VU, VU University Medical Center Amsterdam.
Values are reported as n (%) or mean (sd).
Brain injury resulting from medical insults such as cardiac event or epileptic seizure.
GCS scores at the ED were available in all patients, but 20% of the injury scene scores were missing (Table 2). Almost half (47%) of the patients with severe and 24% with moderate TBI had major extracranial injury. Episodes of hypotension or hypoxia during the pre-hospital phase or at the ED were present or suspected in 20% of the patients.
Values are reported as n (%) or median (interquartile range).
ED, Emergency Department; GCS, Glasgow Coma Scale; ISS, Injury Severity Score.
Untestable, for example because of severe facial swelling.
CT scans were assessed in 95% of the patients (Table 3). Intracranial pathology was detected in 81% in severe TBI and in 56% in moderate TBI. In twenty-six patients (5%) the CT revealed injuries to the vault, skull base, or face without any intracranial abnormalities. SAH and SDH were the most frequent types of intracranial pathology, detected in 43% (SAH) and 39% (SDH) of the patients.
Values are presented as n (%) or median (interquartile range).
Includes both mass lesions (≥25 mL) and smaller lesions ≤25 mL.
CT, computed tomography; TCDB, Traumatic Coma Data Bank.
Patient management and guideline compliance
Most patients (86%) were directly referred to the participating centers and more than 90% were admitted to the hospital (ICU or medical ward) (Table 4). Pre-hospital endotracheal intubation was performed in 69% of the patients with severe and in one patient with moderate TBI. During the pre-hospital phase, 276 patients had a GCS score ≤8. In agreement with BTF guideline recommendations, 192 (70%) of these patients were intubated at the injury scene. In 20% we were unable to assess guideline compliance as the injury scene GCS score was missing.
Values are reported as n (%) or median (interquartile range);
Presented as n (% all patients/% ICU admitted patients); bPatients were intoxicated and were discharged after monitoring at the ED; c12 moderate and 84 severe TBI patients died during ICU admission; d17 moderate and 104 severe TBI patients died during hospital admission (excluding patients deceased at ED/OR).
CPP, cerebral perfusion pressure; CSF, cerebrospinal fluid; ED, Emergency Department; ICP, intracranial pressure; ICU, Intensive Care Unit; MMT, mobile medical team; OR, operating room.
Of the patients admitted to the ICU, 96% required mechanical ventilation and 86% received sedatives. An ICP monitoring device (intraparenchymal or ventricular catheter) was placed in 38% of severe and 8% of moderate TBI patients and raised ICP (>20 mm Hg) was measured in half (moderate) to two-thirds (severe) of the patients with ICP monitoring. According to BTF criteria, 269 patients required ICP monitoring of whom 123 (46%) actually received a monitoring device.
Osmotherapy was administered in 26% of the ICU-admitted patients, with mannitol as the most frequently administered agent. Hypertonic saline was used in two centers and HyperHAES® in one center. Therapeutic hypothermia (n=10) and barbiturates (n=3) were rarely used.
Thirty-three subjects with severe TBI were directly admitted to the medical ward. Approximately half (n=14) of these patients died shortly after admission, comprising a group of patients considered “unsalvageable”. The remaining patients showed a fast improvement in their GCS score and were therefore not admitted to the ICU.
Observed and predicted outcome
A total of 140 (46%) patients with severe TBI and 29 (21%) with moderate TBI had died at 6 months post-injury: 143 (85%) patients died during ED or hospital admission and 25 (15%) between hospital discharge and 6-month follow-up. One patient died between the 6 and 12-month follow-up. Most patients died during ICU admission (57%). Three quarters (76%) died as a result of the head trauma, 11% died as a result of extracranial injury, in 6% the cause of death was not trauma related, and in 7% the cause of death was unknown. Discharge locations were: 177 (49%) home, 101 (28%) other hospital, 56 (15%) rehabilitation center, and 31 (9%) nursing home or residential care facility.
Predicted mortality (calculated with the IMPACT rule) was compared with observed mortality in 369 patients. Patients with a GCS of 13 (n=62) were excluded, as the IMPACT prediction rule is validated for patients with a GCS ≤12. In 31 patients there were insufficient data to apply the IMPACT rule and in 46 patients, 6-month survival data were unavailable. For the remaining patients (n=369), the full laboratory model was used in 317 (86%), the extended model in 17 (5 %,) and the core model in 35 (9%). In severe TBI, observed mortality (46%) was comparable to the median predicted mortality (46% [IQR: 16–61%]). In moderate TBI however, observed mortality (22%) was higher than the median predicted mortality (11% [IQR: 6–22%])
Figure 2 shows the 6 and 12-month outcome in patients who survived the first year after the accident and for whom both outcome measures were available (n=218). Two patients were in a vegetative state at 6 months post-injury and one was in a vegetative state at 1 year post-injury (one patient had died and is therefore not shown in Fig. 2). The proportion of patients with good recovery (GOSE 7–8) increased between the 6 and 12-month follow-up from 38% to 46% in severe TBI and from 48% to 55% in moderate TBI.
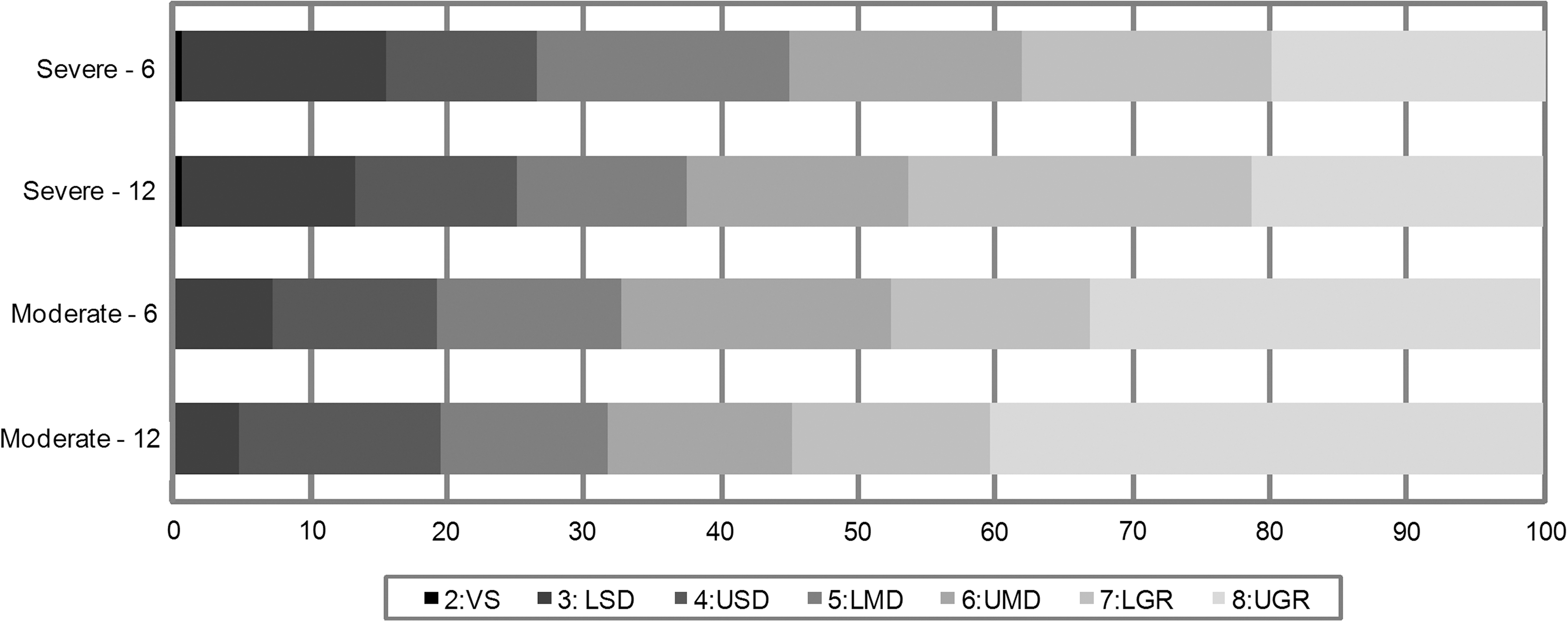
Cumulative percentages of 6 and 12-month outcome in patients surviving the first year after injury. VS, vegetative state; LSD/USD, lower/upper severe disability; LMD/UMD, lower/upper moderate disability; LGR/UGR, lower/upper good recovery.
Injury severity classification at different time points
Figure 3 shows how injury severity classification varied depending upon the time point the GCS score was obtained (i.e., at the injury scene or at ED admission). At the ED, 260 (77%) patients classified as having severe TBI had already been intubated, either during the pre-hospital phase (n=234) or at the first hospital before transportation to the participating hospital (n=26). In contrast, three patients with an ED admission diagnosis of moderate TBI were intubated before GCS evaluation. In 77 patients (15%), fluctuations in the GCS resulted in a change in injury severity category. In-hospital mortality rates were significantly higher (χ2[3]=42.8, p<0.001) for patients classified as having severe TBI at both the injury scene and the ED (S–S, 44%), than for patients improving from severe TBI to moderate TBI (S–M, 7%), those with mild/moderate TBI deteriorating to severe TBI (M–S, 14%), and those with mild/moderate TBI at the injury scene and moderate TBI at the ED (M–M, 15%). No significant differences existed in mortality rates between these latter three categories. Similarly, the proportion of intracranial CT abnormalities was significantly higher (χ2[3]=21.7, p<0.001) in S–S patients (86%) than in those in the S–M (69%), M–S (67%), and M–M (65%) categories.
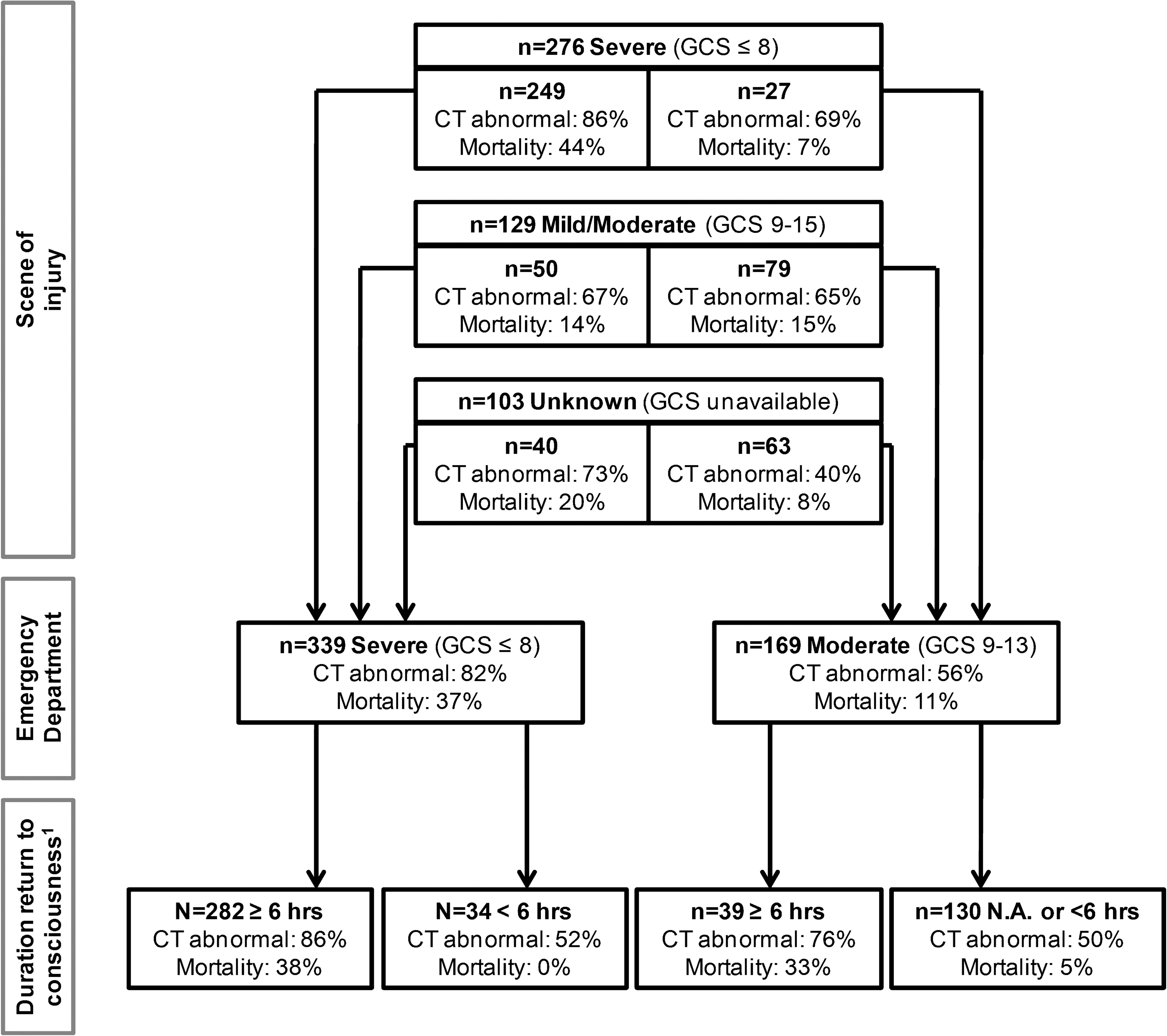
Injury severity based on clinical parameters at different time points. 1Six-hour threshold could not be determined in 23 patients (died within 6 h before regaining consciousness [n=20], discharged to other hospital within 6 h [n=2], missing data [n=1]). CT, computed tomography; GCS, Glasgow Coma Scale; N.A., not applicable (GCS was never ≤8). CT abnormal, the first available CT scan reveals intracranial pathology.
The bottom part of Figure 3 shows the proportion of patients who remained unconscious for>6 h. Of the 169 patients diagnosed as moderate at ED evaluation, 39 (24%) deteriorated to a GCS ≤8 and remained unconscious for>6 h. Patients with impaired consciousness for>6 h had significantly higher in-hospital mortality rates (38% in severe and ≥6 h, 33% in moderate and ≥6 h, 0% in severe and<6 h and 5% in moderate and<6 h, χ2[3]=68.4, p<0.001), and significantly more often revealed intracranial CT abnormalities (86% in severe and≥6 h, 76% in moderate and ≥6 h, 52% in severe and<6 h and 50% in moderate and<6 h, χ2[3]=61.2, p<0.001) compared to patients with no or<6 h unconsciousness.
Comparison with earlier multicenter studies
In Table 5, our data are compared with previous observational multicenter series of severe TBI. Differences between our study and previous ones will be commented on in the Discussion.
Int. Databank, International data bank full series; TCDB, The USA National Traumatic Coma Data Bank; GB4, The British Four Center Study; EBIC, European Brain Injury Consortium Survey of Head Injuries; ATBIS, Australian Traumatic Brain Injury Study; AUSTRIA, Austrian Severe Traumatic Brain Injury Study; POCON, Prospective Observational Cohort Study Neurotrauma. AUT, Austria, AUS, Australia, CT, computed tomography, ED, Emergency Department, EML, evacuated mass lesion, GB, Great Britain, GCS, Glasgow Coma Scale, GOS, Glasgow Outcome Scale, GR, good recovery, ICP, intracranial pressure, MD, moderate disability, NEML, non-evacuated mass lesion, NLD, Netherlands, NSU, Neurosurgical Unit, NZL, New Zealand, NR, not reported, SAH, subarachnoid hemorrhage; SD, severe disability, sd, standard deviation, USA, United States of America, VS, vegetative state.
If NSU admission GCS was unavailable, the GCS had to be ≤8 at the injury scene, first hospital (in case of secondary referral) and at post-resuscitation. bPatients were admitted to ICU or died at ED or operating room. cOnly operations within 24 h. dPre-ICU admission. eData available in 415 (84.3%) patients. fAssessed 11–1199 days post-injury. g3% classified as good/moderate recovery (not shown here). hAssessed 90–360 days post-injury. i85% follow-up for GOSE and 90% follow-up for survival. jAdditional analyses on datasets done in (Murray et al., 1999a).
Discussion
This multicenter observational cohort study in 508 consecutive moderate and severe TBI patients admitted to five Level I trauma centers, shows different case fatality rates between severe (46%) and moderate (21%) TBI. At 1 year post-injury, 45% of moderate and 52% of severe TBI survivors still experienced disability (GOSE ≤6). Compared to earlier observational multicenter series executed over the last four decades, our cohort of severe TBI patients reveals a higher mean age, a higher rate of patients with diffuse injury (i.e. TCDB I–II), more major extracranial injury, and relatively high mortality rates. In addition, our study shows that injury severity diagnosis is influenced by the moment at which the GCS score is obtained. Interestingly, combining clinical information from the injury scene and the ED appears to be useful for outcome prediction. In-hospital mortality rates in patients with a diagnosis of severe TBI at both time points (44%) is three times higher than mortality in patients diagnosed as moderate TBI at one or both time points (7–15%). Furthermore, our study confirms that duration of impaired consciousness remains an important predictor of mortality (Gennarelli et al., 1982). Patients who were in coma for>6 h had significantly higher mortality rates (33–38%) than patients with a duration of<6 h of impaired consciousness (0–5%), independent of their diagnosis on evaluation at the ED.
Demography and injury causes
Mean age in the current TBI cohort (46 years in severe and 50 years in moderate TBI) is among the highest of all multicenter series, which is in line with the reported trend of increasing age in the TBI and general trauma population (Maas et al., 2008; Nijboer et al., 2007). However, precise comparison with previous studies is difficult, as we included patients ≥16 years whereas some other studies included patients of all ages.
As a result of the aging TBI population, it has been suggested that falls emerge increasingly frequently as a cause of injury (Maas et al., 2008). In our study, traffic accidents (51%) still rank first, with falls constituting the second most common cause of TBI (38%). Analysis of trends in injury causes is complicated by variability in injury mechanism coding among studies. In line with recent recommendations to record common data elements (Maas et al., 2010), we registered detailed information on the injury mechanism, location, and intent: relevant data from an epidemiological perspective and for identification of areas for prevention. Patients who fell were older than patients involved in traffic accidents, but compared to studies with available data on falls, no apparent increase in the percentage of falls can be observed in our study, nor is there an increase in the proportion of falls under the influence of alcohol.
Injury patterns and treatment
In our cohort of severe TBI patients, 50% of the initial CT scans was rated as demonstrating no injury (TCDB I) or diffuse injury without large focal lesions (TCDB II). This finding is comparable with only one study from 2000 (Myburgh et al., 2008) but higher than the 25–37% reported in multicenter studies from before 1995 (Marshall et al., 1991b; Murray et al., 1999a). An increase in patients without (major) intracranial pathology may be related to developments in pre-hospital management. Sedation and intubation are becoming more common and may result in more patients with artificially low GCS scores (Stocchetti et al., 2004). However, other factors, such as selection bias, may also play a role. For example, secondary referrals often consist of patients with CT abnormalities at risk for deterioration or patients requiring neurosurgical intervention. In our study, 85% were directly admitted to one of the participating hospitals whereas this was the case in only 12–61% in other multicenter studies (Foulkes et al., 1991; Murray et al., 1999a; Leitgeb et al., 2007; Myburgh et al., 2008).
More than 80% of our severe TBI cohort was admitted to the ICU. Craniotomy was performed in 23% of severe TBI patients compared to 37–67% in previous series (Foulkes et al., 1991; Jennett et al., 1977; Leitgeb et al., 2007; Murray et al., 1999a,b; Myburgh et al., 2008). The relatively low proportion of patients undergoing neurosurgery may be explained by the high percentage of primary referrals, the site of inclusion (i.e., the ED rather than the ICU or neurosurgical unit) and the high degree of patients without signs of brain swelling or raised ICP (i.e., TCDB score I and II) in our study. Alternatively, the findings may represent a more conservative approach toward patient management. In our study, adherence to BTF guidelines for ICP monitoring was only 46%, although comparable rates of guideline compliance (43–57%) have been reported by others (Mauritz et al., 2008a; Shafi et al., 2008). In addition, the frequency of use of brain-specific therapies in our cohort was strikingly lower than in a recent Austrian observational study (Mauritz et al., 2007) but in line with a second study executed in Australia and New Zealand (Myburgh et al., 2008). For example, in our study, osmotherapy was used in 30% of ICU-admitted severe TBI patients compared to 31–62% in previous studies, brief hyperventilation was used in 10% (vs. 6.1–64%) and barbiturates were given in 1% (vs. 8.7–39%). Variety in “treatment aggressiveness” may be related to the scarcity of high-level evidence based treatment options (most are class II or III) on which current recommendations in the available guidelines are based (Maas et al., 2008). Consequently, despite implementation of structured protocols, differences in opinions continue to exist on how treatment options should be applied in the various stages of the disease.
Thus far, moderate TBI has received relatively little clinical research attention. We show that a significant proportion of patients with moderate TBI require ICU admission (43%) and craniotomy (11%), and mortality is as high as 21%, highlighting the potential severity of the injury and the need for a high level of care for a considerable subsection of these patients. The multicenter design of our study allows for future comparison of patient management across hospitals and its potential effect on outcome (i.e., comparative effectiveness research) (Maas et al., 2011). This may be especially relevant for moderate TBI patients for whom management guidelines currently do not exist.
Injury severity
We investigated the course of injury severity at three different moments in time. Three-quarters of the patients diagnosed with severe TBI based on the ED admission GCS score was intubated at the moment of clinical assessment, complicating a reliable neurological evaluation. Initial injury scene GCS scores are less biased, as they are obtained before any treatment is applied. Although this seems advantageous, the reliability (Zuercher et al., 2009) and prognostic value of pre-hospital GCS scores have been questioned (Winkler et al., 1984). Interestingly, in at least 15% of our cohort, diagnosis changed between injury scene and ED. Corroborating previous reports (Davis et al., 2006; Murray et al., 1999a; Winkler et al., 1984), our study suggests that combining information from both the injury scene and ED admission may have additional value for injury severity classification and outcome prediction. A diagnosis of severe TBI at both time points was associated with more intracranial pathology and worse outcome than a diagnosis of moderate TBI at one or both time points.
In some studies, coma for>6 h was an additional diagnostic criterion for severe TBI (Gennarelli et al., 1982; Jennett et al., 1977). In our study, 10% of the patients with an ED diagnosis of severe TBI regained consciousness within 6 h and none of these patients died during hospital stay. Hence, setting a minimal threshold for duration of unconsciousness may be a valid method to differentiate patients with temporarily low GCS scores, as a result of early interventions or alcohol or drug intoxication, from patients with “really” severe TBI. However, from a clinical perspective, setting a 6-h threshold for diagnosis of TBI is not feasible, as TBI usually requires earlier decisions on patient treatment.
1-year outcome
At 6 months, 46% of the severe and 21% of the moderate TBI patients had died. In surviving patients, 52% with severe and 45% with moderate TBI experienced some level of disability (GOSE 2–6) at 1 year post-injury, emphasizing the serious and long-term consequences of the disorder.
In earlier multicenter series, 6-month mortality ranged between 32% and 49% in severe TBI (Jennett et al., 1977; Murray et al., 1999a,b; Myburgh et al., 2008; Rusnak et al., 2007) and between 16% and 19% in moderate TBI (Compagnone et al., 2009; Murray et al., 1999a). The high mortality rate in our study may be, first, related to the fact that we included an unselected cohort at the ED and did not correct for early mortality at the ED or in the first 24 h. Second, we classified patients based on their ED admission GCS scores whereas others used clinical parameters obtained at other time points. As we described previously, temporal fluctuations in the GCS may result in variability in injury severity classification, and consequently in outcome rates. In addition, other sources of variance among the study cohorts were observed that may have interacted with patient outcome. For example, mean age of our cohort was high and 47% of the patients with severe and 24% of those with moderate TBI had sustained major extracranial injuries, and both factors are associated with worse outcome (Ho et al., 2010; Hukkelhoven et al., 2003; Perel et al., 2008; Steyerberg et al., 2008).
The IMPACT prediction rule (Steyerberg et al., 2008) was used to assess the probability of death based on a range of admission characteristics. In severe TBI patients, median predicted probability of dying was as high as the observed case fatality rates, indicating that indeed variance in baseline characteristics may have played a role in the relatively high mortality in our study. In moderate TBI, however, predicted probability of death was lower (11%) than the observed mortality, again indicating the need for more research into management and outcome after moderate TBI.
An even greater discrepancy in outcome data can be observed between our observational study and data from patients enrolled into clinical trials, where mortality rates after severe TBI are usually<30% (Clifton et al., 2001; Edwards et al., 2005; Marshall et al., 1998). Currently, several initiatives—including the above mentioned IMPACT study—are investigating predictors of patient outcome by combining data from inconclusive clinical trials. Although this results in large multicenter patient cohorts that allow for advanced statistical analyses, the differences in outcome between observational studies and clinical trials underline the high level of selection that occurs before patients are enrolled in RCTs and demand for caution in generalizing results to unselected cohorts.
It may be proposed that the relatively low guideline compliance and the subsequent limited use of ICP-targeted treatment play a role in the observed mortality rate in our cohort. In a retrospective study among 34 academic trauma centers in the United States, mortality was lower in aggressive (ICP monitor placement >50%) than in non-aggressive centers (Bulger et al., 2002). However, other studies have reported no effect of ICP monitoring on outcome (Cremer et al., 2005; Mauritz et al., 2008a; Salim et al., 2008). Furthermore, it is interesting to note that in the earlier mentioned Austrian study (Mauritz et al., 2007), treatment was applied up to 39 times more often (barbiturates) (Mauritz et al., 2007) but the 6-month mortality rate (44%) was comparable to that in our study. The effect of patient management and center variation on outcome deserves further investigation, but requires careful consideration of variability in case mix (i.e., more severe patients are more likely to receive specific treatment). These analyses are currently underway.
Finally, regional differences have been reported as a source of variation in TBI epidemiology and outcome (Hukkelhoven et al., 2002; Mauritz et al., 2008b) further complicating comparison among studies. Nonetheless, even when we take into account the complexity of comparing patient outcomes across studies, we conclude that our data do not suggest a considerable decrease in mortality from studies executed in the last 40 years. This is in accordance with a recent meta-analysis that concluded that TBI mortality rates have not changed since 1990 (Stein et al., 2010).
Limitations
Some study limitations need to be addressed. The specialized status of the participating hospitals may have introduced bias toward inclusion of more severely injured patients. In addition, missing data were prominent in the pre-hospital phase and at outcome follow-up. Problems in pre-hospital documentation have been reported before (Murray et al., 1999a; Myburgh et al., 2008) and the follow-up rates in our study are similar to those of other studies (Compagnone et al., 2009; Murray et al., 1999a; Rusnak et al., 2007). Loss to follow-up was partially explained by a relatively large group of foreigners (6.2%) included in our study; most of these patients had returned to their home country at time of 6-month follow-up. Another source of loss to follow-up was the absence of contact information (5.3%), which was also not available to the patient's family physician, who was contacted if named in the medical documents.
As stated previously, comparing studies from different geographical areas with different inclusion criteria complicates assessment of trends in TBI epidemiology, and outcome. Longitudinal studies over an extended period are preferred. In addition, much effort is currently directed toward standardization of data collection across studies (Maas et al., 2011). Although our study was executed before recommendations on common data collection were available, it appears to be in line with much of this advice.
Conclusion
Our interdisciplinary multicenter study on the epidemiology of moderate and severe TBI demonstrates a clearly different case mix from earlier series (older age, more diffuse injuries, more major extracranial injuries) but with comparably high mortality rates. Fluctuations in GCS scores complicate diagnosis and injury profiling of TBI. Combining information from more than one time point and application of a threshold for impaired consciousness may advance injury severity diagnosis and outcome prediction. The quantity of data collected in our study allows for further evaluation of modifiers of patient outcome, such as guideline compliance, between-hospital variability, and availability of post-acute care facilities.
Footnotes
Acknowledgments
The POCON study is funded by the Dutch Brain Foundation (Hersenstichting - HSN-07-01). The authors express their gratitude to Dick Drost, Annemiek Coers, Annelou van der Veen, Joshua Field, Vivian de Ruijter, and Heleen Biersteker for their help with data collection. Amon Heijne is thanked for his help with development and maintenance of the POCON database.
Author Disclosure Statement
No competing financial interests exist.