
Abstract
Studies of spinalized animals indicate that some pharmacological agents may act on receptors in the spinal cord, helping to produce coordinated locomotor movement. Other drugs may help to ameliorate the neuropathological changes resulting from spinal cord injury (SCI), such as spasticity or demyelination, to improve walking. The purpose of this study was to systematically review the effects of pharmacological agents on gait in people with SCI. A keyword literature search of articles that evaluated the effects of drugs on walking after SCI was performed using the databases MEDLINE/PubMed, CINAHL, EMBASE, PsycINFO, and hand searching. Two reviewers independently evaluated each study, using the Physiotherapy Evidence Database (PEDro) tool for randomized clinical trials (RCTs), and the modified Downs & Black scale for all other studies. Results were tabulated and levels of evidence were assigned. Eleven studies met the inclusion criteria. One RCT provided Level 1 evidence that GM-1 ganglioside in combination with physical therapy improved motor scores, walking velocity, and distance better than placebo and physical therapy in persons with incomplete SCI. Multiple studies (levels of evidence 1–5) showed that clonidine and cyproheptadine may improve locomotor function and walking speed in severely impaired individuals with incomplete SCI. Gains in walking speed associated with GM-1, cyproheptadine, and clonidine are low compared to those seen with locomotor training. There was also Level 1 evidence that 4-aminopyridine and L-dopa were no better than placebo in helping to improve gait. Two Level 5 studies showed that baclofen had little to no effect on improving walking in persons with incomplete SCI. There is limited evidence that pharmacological agents tested so far would facilitate the recovery of walking after SCI. More studies are needed to better understand the effects of drugs combined with gait training on walking outcomes in people with SCI.
Introduction
Strategies to improve walking after SCI can be roughly grouped into two categories: those that attempt to harness and potentiate neural pathways underlying locomotor control, or those that attempt to minimize or counteract the secondary sequelae of SCI to allow locomotion. Pharmacological agents that target one or both of these approaches could theoretically provide a way to facilitate walking function after SCI.
Since the early 20th century, there has been a great deal of progress in our understanding of the neural control of locomotion. Early studies in spinally-transected cats showed that the spinal cord, isolated from all supraspinal and peripheral input, was capable of generating alternating flexion and extension activity, and a model for a spinal locomotor network capable of producing the basic locomotor rhythm was proposed (Brown, 1911). Although there is only indirect evidence for such spinal locomotor networks in humans (Calancie et al., 1994; Dimitrijevic et al., 1998), a great deal of work has been dedicated to understanding and characterizing the spinal mechanisms underlying locomotion in the hopes of finding appropriate strategies to facilitate recovery of walking after SCI.
Cat models have been very useful for understanding the contribution of different neurotransmitter systems on spinal locomotor network activity (Rossignol et al., 2001). This has led, in turn, to investigations of the effects of various pharmacological agonists or antagonists of different neurotransmitter systems on locomotor activity (Rossignol et al., 2001). The seminal work of Jankowska and associates (Jankowska et al., 1967a,1967b) linked the noradrenergic neurotransmitter system to neuronal pathways that could underlie this locomotor-like rhythmicity in acute spinal cats. Noradrenaline (norepinephrine) acts as a hormone and a neurotransmitter within the central and sympathethic nervous systems, and it is synthesized by a series of enzymatic reactions that include the noradrenergic precursor L-DOPA (L-3,4-dihydroxyphenylalanine) and dopamine. In fictive (non-behaving) spinal cats, in which the spinal cord is isolated from all supraspinal and sensory input, intravenous application of L-DOPA elicits rhythmic alternating activity (Grillner and Zangger, 1979). In behaving spinalized cats, the administration of clonidine or tizanidine (both are agonists of the α2 adrenergic receptor) has been shown to facilitate expression of locomotion if the animal is supported over a moving treadmill belt (Barbeau and Rossignol, 1991; Chau et al., 1998b; Forssberg and Grillner, 1973). Clonidine has also been shown to potentiate locomotor training in acute spinal cats (Chau et al., 1998a), and modulate the timing of muscle activity (Barbeau and Rossignol, 1991). The dopamine precursor L-DOPA has been shown to induce locomotion in spinalized cats (Grillner and Zangger, 1979), but this effect is likely mediated via noradrenergic pathways in the acute preparation since DOPA's effects on the spinal cord are mediated by inducing the production and release of noradrenaline (Anden et al., 1966). In the chronic state, however, dopaminergic pathways are implicated in the modulation of ongoing locomotor activity in spinalized cats, particularly in increasing flexor burst amplitude (Barbeau and Rossignol, 1991).
The serotonergic system has also been implicated in the spinal control of locomotion in both spinal cat and rat models. Unlike the noradrenergic system, serotonergic agonists modulate established locomotor patterns, but are not able to initiate locomotion in spinal cats (Barbeau and Rossignol, 1990,1991). The application of serotonergic agonists has an excitatory effect on the amplitude of ongoing muscle activity, particularly in the extensor muscles (Barbeau and Rossignol, 1990,1991). The excitatory effect of serotonergic agonists sometimes manifests as spasms or clonus, interfering with the locomotor pattern in spinal cats (Barbeau and Rossignol, 1990). Indeed, serotonergic agonists also potentiate the response to cutaneous nerve stimulation (Barbeau and Rossignol, 1990), and serotonergic pathways have been implicated in hyperactive reflex responses to electrical stimulation (Carlsson et al., 1963; Marley and Vane, 1967), or mechanical stretch or vibration (Carp and Rymer, 1986). However, there is evidence that quipazine, a serotonergic agonist, can help to improve locomotor function in adult spinal cats. Barbeau and Rossignol (1990) showed that quipazine improved joint angle excursion, foot clearance, and step length, and in another study this drug increased step cycle duration, lateral stability, and rhythmic stepping (Brustein and Rossignol, 1999). In adult spinalized rats, serotonin or serotonin agonists help to improve alternating stepping patterns, foot placement (Antri et al., 2002), step shape consistency, the number of steps executed (Fong et al., 2005), interlimb coordination, and electromyographic amplitudes during stepping (Feraboli-Lohnherr et al., 1999). It has also been shown in the in vitro neonatal rat spinal cord that serotonin improves left-right and flexor-extensor rhythmicity during fictive locomotion induced by N-methyl-D-aspartate (NMDA; Pearlstein et al., 2005). More recently, Courtine and colleagues showed that serotonergic agonists used in combination with epidural electrical stimulation and locomotor training in spinalized rats led to kinematics and electromyography (EMG) during full weight-bearing stepping that were similar to those pre-injury (Courtine et al., 2009). Together, this evidence suggests that serotonin and serotonergic agonists, likely in combination with other therapies, may potentially facilitate the lumbosacral spinal circuits used in walking after spinal cord injury in humans.
In addition to the potential contribution of pharmacological agents to the activation of spinal locomotor centers, drugs may also be used to ameliorate neuropathological changes associated with SCI that interfere with functional recovery. Spasticity is one of the most common secondary complications of SCI (Levi et al., 1995; Noreau et al., 2000), and is associated with deleterious effects on ambulation and mobility, among other activities of daily living (Adams and Hicks, 2005; Lundqvist et al., 1991). Spasticity is a complex condition that has been defined as a velocity-dependent increase in stretch reflexes, but also has encompassed other signs such as clonus and muscle spasms by various authors (Adams and Hicks, 2005; Elbasiouny et al., 2010). There are several techniques for reducing spasticity, including pharmacological agents. Baclofen, a derivative of gamma aminobutyric acid (GABA) and a GABAB receptor agonist, is commonly used to treat spasticity after SCI with the intent to enhance motor function. Spasticity has been typically associated with a reduction in presynaptic inhibition (Iles and Roberts, 1986), although other changes in motor neuron properties are also implicated (Elbasiouny et al., 2010). The main effect of baclofen is thought to be presynaptic, by reducing neurotransmitter release and thereby reducing the excitability of synaptic inputs into motor neurons (Li et al., 2004).
Another neuropathological change that negatively impacts locomotor function following SCI is demyelination, which is present following contusion injuries (Guest et al., 2005). In this situation, nerve fibers may remain continuous across the injury site, but varying degrees of demyelination will affect axonal conduction (Nashmi and Fehlings, 2001; Waxman 1989). The low density of sodium channels in the internodal regions of the axon, along with the presence of fast potassium channels in these areas, contribute to the reduced electrical excitability of demyelinated axons (Nashmi and Fehlings, 2001; Waxman 1989). The blockage of the fast potassium channel currents using 4-aminopyridine (4-AP) has been shown to prolong action potentials and facilitate axonal conduction (Blight, 1989; Sherratt et al., 1980) and increase synaptic transmission (Smith et al., 2000) in demyelinated neurons. In animal models of SCI, administration of 4-AP has been associated with improved motor and sensory function (Blight and Gruner, 1987; Blight et al., 1991). There is also vigorous work being done to address the effects of demyelination using cell-transplant strategies (Keirstead et al., 2005; McDonald and Belegu, 2006; Nistor et al., 2005; Reubinoff et al., 2001; Tetzlaff et al., 2010; Wu and Ren, 2009).
Finally, there has been a great deal of effort in SCI research to find therapies that can afford neuroregenerative effects, promote neural plasticity, or provide neuroprotective effects (Kwon et al., 2011a,2011b; Tetzlaff et al., 2010). There are currently numerous clinical trials testing the effects of different neuroregenerative or neuroprotective compounds and the SCI community is anxiously awaiting the results. Outcomes from two large multi-center clinical trials investigating the neuroprotective effects of methylprednisolone (Bracken et al., 1992,1998) and GM-1 ganglioside (Geisler et al., 2001) have already been completed more than a decade ago. Methylprednisolone is a synthetic glucocorticoid steroid with known neuroprotective effects, likely through its anti-inflammatory effects and ability to attenuate lipid peroxidation (Bracken et al., 1992). Gangliosides are naturally-occurring glycosphingolipids found in the cell membranes of the brain and spinal cord and are thought to have neuroprotective and neurotrophic effects (Mocchetti, 2005).
Therapies to improve walking function after SCI have received considerable attention from researchers advancing various rehabilitation therapies and those targeting pharmacological interventions. While there has been much focus on the effect of rehabilitation therapies (Lam et al., 2008; Mehrholz et al., 2008), we also need to understand what has been the effect of pharmacological agents on walking outcomes, especially as clinical trials of new drugs move forward (Baptiste and Fehlings, 2008). Hence, we undertook this targeted systematic review to understand the current evidence for the efficacy of pharmacological agents on functional ambulation in people with SCI in order to understand what lessons we may apply towards future clinical research to improve walking after SCI. This work was part of the Spinal Cord Injury Rehabilitation Evidence project (
Methods
The methods for this systematic review have been described in detail elsewhere (Eng et al., 2007), but will be briefly summarized here. A keyword literature search using multiple databases (MEDLINE/PubMed, CINAHL®, EMBASE, and PsycINFO) was used to identify all relevant articles published from 1980–2009. The following keywords were used in the search: spinal cord injury/paraplegia/quadriplegia/tetraplegia, drug therapy/pharmacological agents/4-AP/clonidine/cyproheptadine/GM-1 ganglioside/L-dopa/baclofen, and ambulation/gait/walking/locomotion. Studies were only included if they specifically reported outcome measures associated with gait (e.g., walking speed, endurance, spatiotemporal data, and gait kinematics). The reference lists of the studies were also hand searched for additional relevant studies. Articles were excluded from the review if they were animal studies, they were not in English, less than half the reported population had a spinal cord injury, or there were no measurable outcomes associated with the intervention. We did not require a minimum sample size because of the resultant limited number of publications.
Quality assessment tools and determination of level of evidence
The rigor and quality of each study were assessed by two of the authors (A.D. or T.L.), using either the Physiotherapy Evidence Database (PEDro) scale (Moseley et al., 2002), or a modified version of the Downs & Black tool (Downs and Black, 1998). Discrepancies in scoring were resolved by discussion. We extracted data from the reviewed studies and summarized the findings in the tables (Tables 1 –4). When possible, drug dosage and adverse effects were also extracted.
RCT, randomized clinical trial; PEDro, Physiotherapy Evidence Database; SCI, spinal cord injury; EMG, electromyography.
EMG, electromyography.
RCT, randomized clinical trial; PEDro, Physiotherapy Evidence Database; SCI, spinal cord injury; ASIA, American Spinal Injury Association.
RCT, randomized clinical trial; PEDro, Physiotherapy Evidence Database; EMG, electromyography; AIS, American Spinal Injury Association (ASIA) Impairment Scale.
RCT, randomized clinical trial; PEDro, Physiotherapy Evidence Database; SCI, spinal cord injury.
FIM, Functional Independence Measure; SCI, spinal cord injury.
We used the PEDro tool to assess the quality of studies that were randomized controlled trials (RCTs). This scale evaluates the internal and external validity of a study based on an 11-item scale, with a maximum score of 10. Higher scores represent greater methodological quality (9–10=excellent; 6–8=good; 4–5=fair;<4=poor; Foley et al., 2003).
A modified version of the Downs & Black tool was used to assess all other studies. This tool evaluates quality based on 27 items, assessing reporting, external validity, and internal validity (bias and confounding) of the study. The maximum score for this tool is 28, with higher scores indicating better methodological quality.
After each study was individually assessed, we determined the level of evidence of all of the studies collectively using a modified scale developed by Sackett and colleagues (Sackett et al., 2000). We collapsed Sackett's levels of evidence into 5 categories. Level 1 evidence corresponded to studies that were “good” to “excellent” RCTs, or a PEDro score≥6. Level 2 was the rating for evidence that included RCTs with a PEDro score≤5, non-randomized prospective controlled studies, and cohort studies. Level 3 corresponded to evidence from case-control studies. Evidence from pre-post/post-test/case series and observational/case report studies were rated Level 4 and 5, respectively. Any study that did not include statistical analysis for the walking outcome measure were automatically rated Level 5.
Effect sizes
We calculated effect sizes and 95% confidence intervals using the Cohen's d estimate with Hedges adjustment for sample size (Devilly, 2004) for studies that measured changes in walking speed, either during pre- and post-treatment, or placebo and experimental treatment. To calculate effect size for the pre-post studies, the mean pre-test walking speed was subtracted from the mean post-test walking speed and divided by the weighted average of the standard deviations for both time points. To calculate effect size for the controlled studies, the change in walking speed from baseline in both the experimental and placebo groups was calculated. The difference in the mean changes was then divided by the weighted average of the standard deviations of all of the changes. We also calculated effect sizes for 4 different locomotor training studies that had walking speed as an outcome measure (Field-Fote and Roach, 2011; Gorassini et al., 2009; Winchester et al., 2009; Wirz et al., 2005) for comparison using the same methods.
The results were displayed in a forest plot. An effect size of 0.2–0.5 is considered small, 0.5–0.8 medium, and≥0.80 large (Cohen, 1977). When walking speed data from the articles were illustrated in graphical form, we scanned the image to a computer file and extracted the data from these graphical plots using a custom-written MATLAB software program (GRABIT, J. Doke; MathWorks, Inc., Natick, MA). The changes in walking speed for subjects using body weight support in the Norman study were not included in this analysis because the amount of body weight support may have changed between each evaluation (Norman et al., 1998). In addition, because multiple drugs were tested in each subject, data were only extracted from this study when the drug was immediately preceded by a period when no medication was given and was used for the pre-to-post comparison. This study also reported the effects of baclofen or the combination of cyproheptadine and clonidine on walking, but these results were not included in the forest plot because there was data for only one subject, and the effect sizes could not be calculated (Norman et al., 1998).
Results
The literature search resulted in 696 articles related to pharmacological interventions and gait after SCI. Eleven studies met our criteria and were evaluated using either the PEDro tool for RCTs, or the modified Downs & Black tool for all other studies. Six studies examined the effects of monoaminergic drugs (clonidine, cyproheptadine, and L-dopa) on gait after SCI, three studies examined the effects of 4-AP, two studies examined the effects of baclofen, and one studied the effects of GM-1 ganglioside. Most but not all subjects had incomplete spinal cord injuries.
Monoaminergic agents
Six studies examined the effects of monoaminergic drugs on walking after complete or incomplete SCI (Tables 1A–D, total n=51). Reported side effects in each study are also included in each of the tables. In most studies, the effects of each drug were studied individually with the exception of one study by Fung and associates (Fung et al., 1990), in which subjects were given a combination of cyproheptadine and clonidine in addition to the baclofen they were already taking before the experiment began.
Clonidine
Our literature search resulted in three studies examining the effects of clonidine (Norman et al., 1998; Rémy-Néris et al., 1999; Stewart et al., 1991; Table 1A, total n=29; 8 months to 10 years post-injury). Two of the studies (Norman et al., 1998; Stewart et al., 1991) used the oral form of clonidine, while a third study administered the drug intrathecally via lumbar puncture in order to minimize side effects (Rémy-Néris et al., 1999). In a small RCT (n=9, no statistical analysis), improvements were only noted in one of the three subjects with incomplete SCI, in whom the subject progressed from being unable to walk to walking over ground with an assistive device (Stewart et al., 1991). This particular subject was more severely impaired than the other incomplete SCI subjects, and had the shortest amount of time post-injury (1 year post-injury). The other studies (1 pre-post [Norman et al., 1998] and 1 non-randomized controlled study [Rémy-Néris et al., 1999]) similarly showed that more severely impaired subjects benefited more from the administration of clonidine. In addition, the pre-post study by Norman and colleagues showed that the effects of clonidine persisted after washout of the drug (Norman et al., 1998).
Cyproheptadine
Cyproheptadine is a serotonergic antagonist and an antihistamine drug. Two studies examined the effects of this drug on walking in patients with SCI (Norman et al., 1998; Wainberg et al., 1990; Table 1B, total n=20; 1–15 years post-injury). Subjects took up to 24 mg of cyproheptadine daily in the form of oral tablets in both studies.
One Level 5 cross-over study (Wainberg et al., 1990), and one Level 5 post-test study (Norman et al., 1998), both without statistical analysis, described the effects of cyproheptadine on gait patterns after SCI. The prospective controlled trial showed that maximum comfortable walking speed increased 8–34% in all 6 ambulatory subjects with the medication (Wainberg et al., 1990). In addition, the two patients that required body weight support during treadmill walking while taking the placebo medication were able to make stepping movements with full weight bearing while taking cyproheptadine. Muscle coordination was improved and clonus was reduced in the patients. Norman and associates (Norman et al., 1998) similarly reported that the administration of cyproheptadine was associated with increased treadmill speed, as well as reduced ankle clonus.
Combination of cyproheptadine+clonidine
There are two Level 5 post-test studies that examined the effect of the combination of cyproheptadine and clonidine (Table 1A and 1C, total n=4; 8 months to 2 years post-injury; Fung et al., 1990; Norman et al., 1998). In the study by Norman and associates (Norman et al., 1998), the combination of cyproheptadine and clonidine resulted in increased maximal treadmill speed and decreased assistance with stepping in 2 subjects. In the study by Fung and colleagues (Fung et al., 1990), subjects also underwent locomotor training. The subjects were first stabilized on the combined medication for 2 weeks (in addition to the baclofen they were already taking before the study started), before commencing the combined drug therapy in addition to intense locomotor training (body-weight-supported treadmill training, 3–5 sessions/week for 3–8 weeks). Treadmill-based gait assessments demonstrated improved lower limb muscle activity and joint kinematic patterns following medication and locomotor training. Muscle activity became more phasic during walking and the subjects experienced less clonus. Subjects were able to walk over ground while on medication, and they showed further improvement in functional ambulation with the addition of locomotor training.
Levodopa
One study has examined the effect of L-dopa in incomplete SCI (Maric et al., 2008; Table 1D, n=12, 4–16 weeks post-injury). Subjects underwent a randomized cross-over trial in which 6 weeks of placebo was followed by 6 weeks of L-dopa (or vice versa), combined with locomotor training (45 min, 5 days/week). This study provides Level 1 evidence that there is no difference between L-dopa and placebo combined with locomotor training on changes in voluntary muscle strength, walking function, and activities of daily living, in sub-acute SCI.
4-Aminopyridine
The effects of 4-AP on gait after SCI has been studied in two Level 1 RCTs (DeForge et al., 2004; van der Bruggen et al., 2001), and one Level 4 pre-post study (Segal and Brunnemann, 1998; Table 2, total n=44, 1–56 years post-injury). Although an earlier pre-post trial showed promising results (36% improvement in gait speed; Segal and Brunnemann, 1998); later controlled trials did not support this result (DeForge et al., 2004; van der Bruggen et al., 2001). Level 1 evidence showed that there was no benefit from 4-AP over placebo for gait parameters in chronic incomplete SCI (DeForge et al., 2004; van der Bruggen et al., 2001). The varied dosages used in the three reviewed studies (10-mg 4 times daily in the DeForge study, between 15 and 45 mg daily in the van der Bruggen study, and a 10-mg single dose in the study by Segal and Brunneman)) complicates interpretation of the outcomes and makes it difficult to draw clear conclusions from the available evidence.
GM-1 ganglioside
One study reported the effects of GM-1 on walking after SCI (Walker and Harris, 1993; Table 3, n=9, 1–13 years post-injury). Subjects were given GM-1 ganglioside intravenously or intramuscularly in conjunction with physical therapy, and was compared to placebo via cross-over design. This study provides Level 1 evidence that shows that GM-1 ganglioside is beneficial for the recovery of walking in chronic SCI (Walker and Harris, 1993). The levels of injury (i.e., on the American Spinal Injury Association [ASIA] Impairment Scale [AIS] classification or functional level) of the subjects were not clearly described by the authors, but all subjects were chronic wheelchair users at the start of the study. Subjects had significantly higher motor scores with GM-1 ganglioside, with no placebo effect. All but one subject increased walking speed and walking distance with GM-1 ganglioside. The subject who did not improve in gait speed or distance did, however, switch from long-leg bracing to below-knee bracing.
Baclofen
There is limited evidence that baclofen may improve walking after SCI. Two Level 5 pre-post studies that examined the effects of baclofen on gait (Table 4, total n=21, 0.5–27 years post-injury; Azouvi et al., 1996; Norman et al., 1998). The study by Avouzi and associates (Azouvi et al., 1996) showed there was increase in the Functional Independence Measure (FIM) walking scores in 5 of 18 patients, and 2 people acquired the ability to climb stairs when using baclofen. Subjects in the study by Norman and colleagues (Norman et al., 1998) only showed minor changes in walking when using this drug.
Effect sizes
Figure 1 is a forest plot of the effect sizes for all studies from which we were able to extract data on changes in walking speed. Effect sizes were small for the majority of the studies (d<0.20) for which we were able to extract walking speed data (Fig. 1). One randomized cross-over study examining at the effects of 4-AP actually resulted in slower walking speeds (van der Bruggen et al., 2001). The cross-over study that investigated the effects of 4-AP on walking speed (DeForge et al., 2004) had a medium effect size (d=0.564 for maximum walking speed).
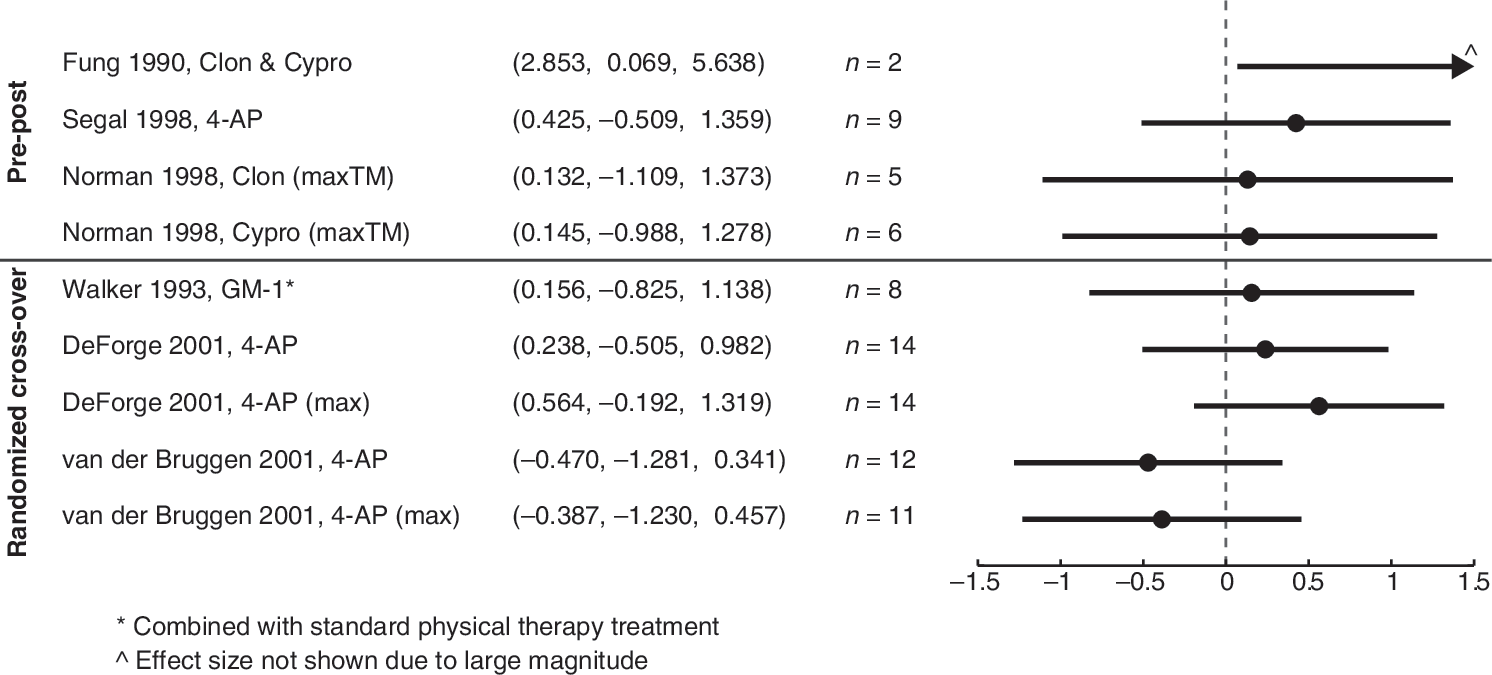
Forest plot displaying effect sizes and 95% confidence intervals using the Cohen's d estimate with Hedges adjustment for sample size for each study that reported changes in walking speed. Pre-post studies are separated from randomized cross-over trials. All effect sizes are for over-ground walking speed or for treadmill walking speed (TM). (Clon, clonidine; Cypro, cyproheptadine; GM-1, GM-1 ganglioside; 4-AP, 4-aminopyridine).
Health and drug screening
Few of the studies presented in this review reported that health screenings of other organ systems (e.g., liver function) were performed to ensure that the subjects were healthy enough to properly metabolize the drugs. Only one of the studies (DeForge et al., 2004) stated that blood count and liver function tests were performed. Two of the studies involving clonidine (Norman et al., 1998; Stewart et al., 1991) measured blood pressure when increasing dosage because of its hypotensive effects. Possible drug-drug interactions were also not addressed. Six studies stated that subjects were taking other drugs at entry to the study (DeForge et al., 2004; Fung et al., 1990; Norman et al., 1998; Stewart et al., 1991; van der Bruggen et al., 2001; Wainberg et al., 1990), but only three specifically listed what these drugs were (DeForge et al., 2004; Fung et al., 1990; Norman et al., 1998).
In the study by Norman and associates, one subject continued to take anticonvulsant medication (divalproex sodium) and an antidepressant (imipramine) throughout the study, and another subject took an anxiolytic medication (bromazepam) occasionally during the study to aid with sleeping (Norman et al., 1998). In the study by DeForge and colleagues of 4-AP, 6 of 15 subjects had been stabilized on medication for spasticity. Three of these subjects were taking clonidine, two were taking baclofen, and one was taking cyproheptadine (DeForge et al., 2004). Subjects in the study by Fung and associates were also taking baclofen in addition to the combination of clonidine and cyproheptadine throughout the study (Fung et al., 1990). In the study by van der Bruggen and colleagues of 4-AP, subjects were asked to maintain stable doses of prescribed medications throughout study, but the types of drugs that were taken or the number of subjects taking other drugs were not reported (van der Bruggen et al., 2001). Anti-spasticity medications were also taken by three subjects in the study by Stewart and associates of clonidine (Stewart et al., 1991). Subjects in the study by Wainberg and colleagues were stabilized on their medications for spasticity for at least 3 months before they started the study with cyproheptadine (Wainberg et al., 1990).
Discussion
This systematic review found 11 articles that examined the effects of pharmacological agents on walking outcomes after SCI. The median PEDro score for the RCTs was 7 out of 10 (first quartile=6, third quartile=7; two studied the effects of 4-AP, one studied L-dopa, one studied clonidine, and one studied GM-1 ganglioside), showing that these studies were of good quality. The non-RCTs that were reviewed were of lower quality, with the median Downs & Black score for these studies being 12 out of 28 (first quartile=1, third quartile=15.25).
Studies show small effects
Where over-ground walking speed data were available, we calculated and compared the effect sizes of each reviewed study. Most studies showed small to negative effects on walking speed (d=–0.470 to 0.564), with only one study showing a medium effect size (DeForge et al., 2004; Fung et al., 1990; Segal and Brunnemann, 1998; van der Bruggen et al., 2001; Walker and Harris, 1993). To determine how these effect sizes compared to changes in walking speed following physical rehabilitation alone, we looked at the results from four studies in which subjects with chronic incomplete SCI underwent different forms of gait training and walking speed was an outcome measure (Field-Fote and Roach, 2011; Gorassini et al., 2009; Winchester et al., 2009; Wirz et al., 2005). Our calculated effect sizes from these studies were 0.1–0.62 (n=10–30; mean±SD: d=0.32±0.16), indicating that locomotor training will result in as good, or more likely better, gait outcomes than using any of the drugs presented in this review.
It is striking that few of the studies we examined combined intensive locomotor training with pharmacological agents. Only two studies (Fung et al., 1990; Maric et al., 2008) employed intensive task-specific gait training techniques in conjunction with the drug therapy. Two other studies reported that subjects underwent regular therapy sessions that appeared to consist largely of non-specific range-of-motion and strengthening exercises, with some gait training (Wainberg et al., 1990; Walker and Harris, 1993). Given the importance of task-specific training on functional recovery (Edgerton and Roy, 2009; Harkema, 2001; Ichiyama, et al., 2008), it will be important to understand the combinatorial effects of rehabilitation along with pharmacological interventions.
Only a fraction of patients were able to improve their walking speed with clonidine or cyproheptadine. The subjects that typically benefited from the medications were more severely impaired and had higher levels of spasticity, but also had a minimum level of function (could stand or walk with assistance). This suggests that these drugs may be more useful in helping individuals with more severe impairments as a way to initiate or facilitate locomotor training, particularly through their effect in reducing severe spasticity and clonus (Norman et al., 1998; Stewart et al., 1991). In addition, there is evidence that clonidine has deleterious effects on walking in cats with partial spinal lesions (Rossignol et al., 2001), so it may not be surprising that this drug did not greatly improve walking in humans with incomplete SCI.
Another possible reason that minimal gains in walking were seen with the monoaminergic drugs may have to do with the drugs' side effects. Subjects with SCI may already have low tolerance to changes in blood pressure or heart rate due to abnormal cardiovascular control (Krassioukov and Claydon, 2006), and therefore may be more sensitive to the medications that have hypotensive effects, such as clonidine, than the general population. Also, because clonidine is an α2-receptor agonist that inhibits the release of norepinephrine and decreases sympathetic tone (AHFS Drug Information, 2011), it could cause a decrease in the general excitability of the nervous system. Cyproheptadine is an anti-serotonergic drug (a CNS depressant) and is also an antihistamine drug. Side effects of antihistamine medications are drowsiness and fatigue, which may have an obvious detrimental impact on walking outcomes. Thus the side effects of these drugs may have outweighed the desired effects of the medication.
There may be several explanations as to why L-dopa did not improve locomotor function in persons with SCI. Maric and colleagues hypothesized that the locomotor spinal circuitry would be facilitated during walking training in the presence of a noradrenergic drug (Maric et al., 2008). However, animal studies have shown that noradrenergic terminals degenerate within a week after SCI (Anden et al., 1964), and in chronic spinalized cats, L-dopa modulates muscle activity in ongoing locomotion through dopaminergic receptors, not noradrenergic receptors (Barbeau and Rossignol, 1991). There is also a reduction in the capacity of the spinal cord to synthesize dopamine from L-dopa in acutely injured rats (10 days post-injury), although this capacity recovers to normative values by the time the animals are 100 days post-injury (Commissiong, 1985). The participants in the study by Maric and associates (2008) had a SCI between 4 and 16 weeks' duration, and the administration of L-dopa occurred over a 12-week period. Thus, changes in the capacity for dopamine synthesis during this sub-acute injury phase could have confounded the results. The authors also justified the use of this drug in persons with SCI because it improved motor function in stroke in combination with exercise training (Scheidtmann et al., 2001). However, the mechanisms underlying the recovery of walking function in stroke could be quite different than what occurs in SCI. These factors may have contributed to the lack of effect of L-dopa on walking outcomes in persons with SCI (Maric et al., 2008).
Conflicting evidence exists regarding the benefits of GM-1 ganglioside on the recovery of locomotion after SCI. In the reviewed study, GM-1 ganglioside combined with physical therapy improved motor scores, walking distance, and walking speed in a small RCT with chronic SCI (Walker and Harris, 1993). Later, a large multi-center RCT in patients with acute SCI (n=760) showed that although GM-1 ganglioside treatment accelerated initial recovery during the first 8 weeks of treatment, it was no different than placebo by the end of the trial (26 weeks; Geisler et al., 2001). However, specific walking-related outcomes were not reported in this larger trial. This supports the idea that treatment effects tend to be exaggerated in smaller, non-controlled trials, and that larger trials are needed to evaluate the effectiveness of therapeutic interventions.
Intrathecal baclofen showed slightly better results (an increase in the walking component of the FIM score in 5 of 18 patients; Azouvi et al., 1996) than oral baclofen (only minor changes were seen in walking; Norman et al., 1998). This is consistent with the evidence on the effects of baclofen on spasticity. A systematic review showed that intrathecal baclofen is effective in reducing spasticity compared to controls, while oral baclofen had no effects (Taricco et al., 2000). Currently, there are investigations into using other drugs to target spasticity through different neural mechanisms (serotonergic or noradrenergic pathways; Rank et al., 2007).
Methodological limitations of the reviewed studies
There are several possibilities as to why the studies evaluated in the present review had small or even negative effects on walking, many of which may be related to the variability of subject characteristics, and in the differences in testing protocols among studies. In addition to the small sample sizes in many of the studies, the subject groups may have been too heterogeneous in injury chronicity, level and severity, participant age, or too small in number to show a strong effect on the outcome measures. The dose and frequency of the different medications varied within and between studies, creating even more variability in study design. It is also possible that the subjects tested had impairments that would have resulted in only minimum benefits from these drugs. In addition, it was reported that some of the subjects in the reviewed studies were taking other medications. The presence of other drugs may have led to drug-drug interactions that may have ultimately affected locomotor outcomes.
Varied outcome measures were used in the reviewed studies, making the results difficult to compare. There was a lack of measurable functional ambulation outcomes in most of the studies. Quantitative and accurate functional outcome measures are essential to SCI clinical trials (Steeves et al., 2007). In addition, the relatively weak level of evidence for the effects of these drugs on walking is due to the fact that more than half of the studies reviewed were not randomized or blinded, which may exaggerate the actual treatment effects (Carlson and Schmidt, 1999; Lipsey and Wilson, 1993).
In most studies, it was unknown whether subjects had organ systems healthy enough to metabolize the drugs they were given. For example, impairments in liver or kidney function could limit drug metabolism, distribution, and excretion. Liver function and blood count tests were reported in only one study (DeForge et al., 2004). Clonidine, 4-AP, and baclofen dosages should be adjusted according to the degree of renal function (AHFS Drug Information, 2011), yet none of the studies involving these drugs reported that they tested renal function of the subjects.
Future directions
Although the studies done to date of the effects of pharmacological agents on walking outcomes in SCI have been disappointing, there could be potential in investigating combinatorial strategies. Although it had a small sample size, the study by Fung and associates suggested that cyproheptadine and clonidine in combination with locomotor training improved gait patterns and over-ground walking speed (Fung et al., 1990). There are other promising combinations of multiple therapeutic interventions currently under study. One new drug combination (Spinalon), which consists of L-dopa, the 5-HT agonist buspirone, and carbidopa, has been shown to facilitate reflex stepping during treadmill training by activating spinal locomotor networks (Guertin et al., 2010). A recent case study testing safety has shown that this combination had no significant side effects in a subject with incomplete SCI (Guertin and Brochu, 2009). Combining pharmacological agents with active rehabilitation therapy may also be promising. In spinalized rats, combining pharmacological agents with locomotor training and electrical stimulation led to reorganization of central pattern generator circuits, enabling full weight-bearing stepping (Courtine et al., 2009). Future studies should also benefit from a combination of expertise of clinical pharmacologists along with neuroscientists and rehabilitation specialists.
Footnotes
Acknowledgments
This work was supported by the King Saud University–International Twinning Program. We thank the Rick Hansen Man-in-Motion Foundation and the Ontario Neurotrauma Fund for their support of the Spinal Cord Injury Rehabilitation Evidence (SCIRE) project. T.L. was supported by a New Investigator Award from the Canadian Institutes of Health Research. J.J.E. is a Michael Smith Foundation for Health Research Senior Scholar.
Author Disclosure Statement
No competing financial interests exist.