
Abstract
Near-infrared transcranial laser therapy (TLT) has been found to modulate various biological processes including traumatic brain injury (TBI). Following TBI in mice, in this study we assessed the possibility of various near-infrared TLT modes (pulsed versus continuous) in producing a beneficial effect on the long-term neurobehavioral outcome and brain lesions of these mice. TBI was induced by a weight-drop device, and neurobehavioral function was assessed from 1 h to 56 days post-trauma using the Neurological Severity Score (NSS). The extent of recovery is expressed as the difference in NSS (dNSS), the difference between the initial score and that at any other later time point. An 808-nm Ga-Al-As diode laser was employed transcranially 4, 6, or 8 h post-trauma to illuminate the entire cortex of the brain. Mice were divided into several groups of 6–8 mice: one control group that received a sham treatment and experimental groups that received either TLT continuous wave (CW) or pulsed wave (PW) mode transcranially. MRI was taken prior to sacrifice at 56 days post-injury. From 5–28 days post-TBI, the NSS of the laser-treated mice were significantly lower (p<0.05) than those of the non-laser-treated control mice. The percentage of surviving mice that demonstrated full recovery at 56 days post-CHI (NSS=0, as in intact mice) was the highest (63%) in the group that had received TLT in the PW mode at 100 Hz. In addition, magnetic resonance imaging (MRI) analysis demonstrated significantly smaller infarct lesion volumes in laser-treated mice compared to controls. Our data suggest that non-invasive TLT of mice post-TBI provides a significant long-term functional neurological benefit, and that the pulsed laser mode at 100 Hz is the preferred mode for such treatment.
Introduction
T
Low-level laser therapy (LLLT) has been found to modulate various biological processes, such as increasing mitochondrial respiration and ATP synthesis, facilitating wound healing, and promoting the process of skeletal muscle regeneration and angiogenesis in injured ischemic organs (Conlan and Cobb, 1996; Karu, 2007; Oron, 2006; Streeter et al., 2004). LLLT has also been shown to modulate processes in the nervous system. Anders and associates (2004) reviewed the beneficial effects of LLLT on functional recovery of injured peripheral nerves. Light-emitting diodes were also shown to regulate cytochrome C oxidase, leading to increased energy metabolism in vitro in visual neurons that had been functionally inactivated by toxin (KCN) (Wong-Riley et al., 2005). It was also demonstrated that infrared transcranial laser therapy (TLT) applied 6 h post-embolic stroke in rabbits (Lapchak et al., 2004), and 24 h post-ischemic stroke in rats (De Taboada et al., 2006; Oron et al., 2006), caused a significant improvement in neurological scores compared to sham-operated experimental animals. In another study, the beneficial effect of TLT in a rabbit stroke model suggested an extended therapeutic window and some advantages of using pulsed wave (PW) laser mode over continuous wave (CW) laser mode (Lapchak et al., 2007). The beneficial effect of TLT for stroke was also evaluated in a rabbit model in combination with thrombolytic activity and was found to be effective (Lapchak et al., 2008). Furthermore, it was found that TLT significantly elevated ATP levels in the intact brains of rabbits (Lapchak and DeTaboada, 2010). The safety and effectiveness of TLT for acute stroke patients was also seen in two randomized clinical trials (Lampl et al., 2007; Zivin et al., 2009), in moderate to moderately severe stroke patients, but not in very severe stroke patients (Stemer et al., 2010; Zivin et al., 2009).
In a previous study we have shown that TLT given at 4 h post-TBI in mice significantly reduced neurological deficits up to 28 days (Oron et al., 2007). The use of various laser modes for TLT in TBI has not been investigated previously, nor has the therapeutic window of TLT for TBI been explored. The aim of the present study was to evaluate the long-term effect of TLT, as assessed by neurobehavioral outcome and histologic brain lesions, at different treatment time points post-injury, and with different laser treatment modes (CW versus PW) and power density.
Methods
Animals
A total of 45 male (2-month-old) Sabra mice (Hebrew University strain) weighing 25–35 g were used in this study. They were housed in groups of six per cage, under a 12-h:12-h, light:dark reversed light cycle. Food and water were provided ad libitum.
The study was performed according to the guidelines of the Institutional Animal Care Committee at The Hebrew University, Jerusalem, Israel.
Trauma model
Trauma to the head was induced under ether anesthesia. Ether anesthesia was confirmed by testing loss of pupillary and corneal reflexes before induction of trauma to the head. Closed-head injury (CHI) was induced using a weight-drop device as previously described (Chen et al., 1996; Yatsiv et al., 2002). This specific model was recently described as “a clinically-relevant model of closed head injury” (Flierl et al., 2009). Following a sagittal scalp incision, the mice were manually immobilized, and a tipped Teflon cone was placed 2 mm lateral to the midline and 1 mm caudal to the left coronal suture. Following this, a metal rod (94 g) was allowed to free fall onto the cone from a pre-calibrated height. This procedure does not cause a skull fracture if the height of the falling metal rod is well controlled and the head is stabilized (Flierl et al., 2009). The lesion in the brain due to the procedure is focal as described by us previously (Oron et al., 2007) using histological methods and MRI images (Beni-Adani et al., 2001), and in the current study.
Neurological Severity Score
Motor function and reflexes of the traumatized mice were evaluated at different time points post-CHI using the Neurological Severity Score (NSS), which was modified to emphasize motor functions (Beni-Adani et al., 2001). The neurological tests are based on the ability of the mice to perform 10 different tasks that evaluate the motor ability, balance, and alertness of the mouse, as described previously (Oron et al., 2007). One point is given for failing to perform each of the tasks; thus a normal uninjured mouse scores 0. The severity of injury is defined by the initial NSS, evaluated 1 h post-CHI (NSS1), and is a reliable predictor of the late outcome (Tsenter et al., 2008). Thus, fatal or near-fatal injury is defined in mice having an NSS1 of 9–10, severe injury with an NSS1 of 7–8, moderate injury with an NSS1 of 5–6, and mild injury with an NSS1 of 4 or less. The term dNSS represents the difference between NSS1 for an individual mouse and its NSS at a certain time point post-CHI. Thus a higher dNSS value indicates greater neurological recovery. After an initial NSS was performed on all of the mice, the mice were divided into experimental groups of eight, such that the mean NSS in each group was similar to ensure comparable severity of injury in all groups.
Laser treatment
All mice were subjected to CHI and assigned to control or laser-treated groups as detailed in the results section.
The laser device was a Ga-Al-As 808-nm wavelength laser with a maximal power output of 200 mW (Photothera, Inc., Carlsbad, CA), equipped with a rigid flat glass fiberoptic tube covered with a metal cylinder (3 mm in diameter and 3 cm long) with a bare glass distal tip. The laser was applied by placing in full contact the distal tip of the fiberoptic probe on a point in the midline of the skull (sagittal suture) located 4 mm caudal to the coronal suture of the skull, after the skin had been removed in that region by a small longitudinal incision. The rigid fiberoptic probe was placed on the skull perpendicular to the horizontal plane of the mouse's body. In preliminary experiments the entire cortical part of a fresh skull was excised from a mouse 4 h post-TBI. The distal tip of the fiberoptic probe of the laser was placed on the same location on the skull as described above. The power density of the laser post-transmission through the skull was measured by placing the probe of a laser power meter (Ophir Inc., Jerusalem, Israel) under the dura. Based upon prior measurements, this location was chosen as being sufficient to illuminate the entire brain (1.2 cm beam diameter as measured by an infrared viewer) due to dispersion of the laser beam by the skull. The laser power output at the tip of the fiberoptic probe (in full contact with the skull bone) was 21 mW. This delivered a power density of 10 mW/cm2 to the brain's cortical surface. Laser irradiation was delivered for 2 min at this power density (10 mW/cm2) so that the fluency at the cortical surface of the cerebrum was 1.2 J/cm2. The power and energy density of the laser were chosen based on preliminary experiments with various parameters of the laser applied in the CHI mouse model and our previous study (Oron et al., 2007).
In the first experiment there were three groups as follows: two groups that received TLT at a dose of 10 mW/cm2 CW at 6 h (n=6) or 8 h (n=7) post-CHI, while a third group (n=7), serving as sham-operated controls, underwent the same procedure as the laser-treated group but did not receive actual laser treatment. In the second experiment four groups were used and the laser was applied 4 h post-CHI: two groups received TLT at a dose of 10 mW/cm2 (peak power) PW at 100 Hz (n=7), or 600 Hz (n=6), a third group received TLT at a dose of 10 mW/cm2 CW (n=6), and the fourth group served as control sham-operated group (n=6) as in the first experiment. All mice from both experiments were sacrificed at 56 days post-CHI.
Magnetic resonance imaging
The mice were scanned in a 7T/30 spectrometer (Bruker, Karlsruhe, Germany) under ∼1.5% isoflurane anesthesia with a quadrature head coil. The MRI protocol included a conventional T2-weighted protocol utilizing the multi-slice multi-echo (MSME) sequence acquired with TR of 3000 msec and multi-TE of 60 msec. Geometric parameters were: 12 coronal slices with resolution of 0.075×0.120×1 mm3 (FOV of 19.2 mm2 and matrix of 256×160) were acquired. The images were reconstructed to final image dimensions of 256×256 with a resolution of 0.075×0.065×1 mm3.
Quantitative analysis of lesion volume from the MRI of mice was performed on 5 control and 6 laser-treated (3 CW and 3 PW, 100 Hz) mice chosen at random from the surviving mice. The lesion volume as a percentage of the total volume of each brain was calculated using Sigma Scan Pro software (Sigma, St. Louis, MO).
Statistical analysis
Data were analyzed using one-way analysis of variance (ANOVA) followed by the Student Neuman-Keuls test (using Sigma stat software). Data are presented as mean±standard deviation (SD). A value of p<0.05 was regarded as statistically significant.
Results
Neurobehavioral function
The NSS1 scores of the mice in the present study ranged between 4 and 6, indicating a mild-to-moderate trauma. The first experiment was designed to evaluate the optimal therapeutic window within which to treat with TLT post-CHI. The second experiment aimed to assess the effect of various PW modes of the laser versus CW mode on the neurological behavior and brain lesions of the traumatized mice.
In the first experiment, a slight increase in functional recovery, as assessed by dNSS, was found in the control non-treated mice only between days 17 and 28 post-CHI, and no further recovery was noted even at 56 days post-CHI (Fig. 1). However, when laser was applied either at 6 or 8 h post-CHI, the dNSS was significantly higher than in control animals, and this improvement gradually increased with time post-CHI. The improvement in the dNSS occurred at a faster rate and extent for those mice that had been treated 6 h post-CHI than those treated at 8 h post-CHI (Fig. 1). At 56 days post-CHI the dNSS of the mice that had laser energy applied at 6 h post-CHI was 3.3±0.6. This was significantly higher (p<0.05) than the dNSS of the mice with laser energy applied 8 h post-CHI (1.8±0.6), and also significantly higher (p<0.05) than the control group (1.0±0.2). These differences comprised a 3.4- and 1.8-fold increase in dNSS for the laser energy applied 6 and 8 h post-CHI, respectively, as compared to the control non-laser-treated mice. From 28 days post-CHI up to 56 days post-CHI there was no statistically significant difference in the dNSS between the control group and the group that had laser energy applied at 8 h post-CHI.
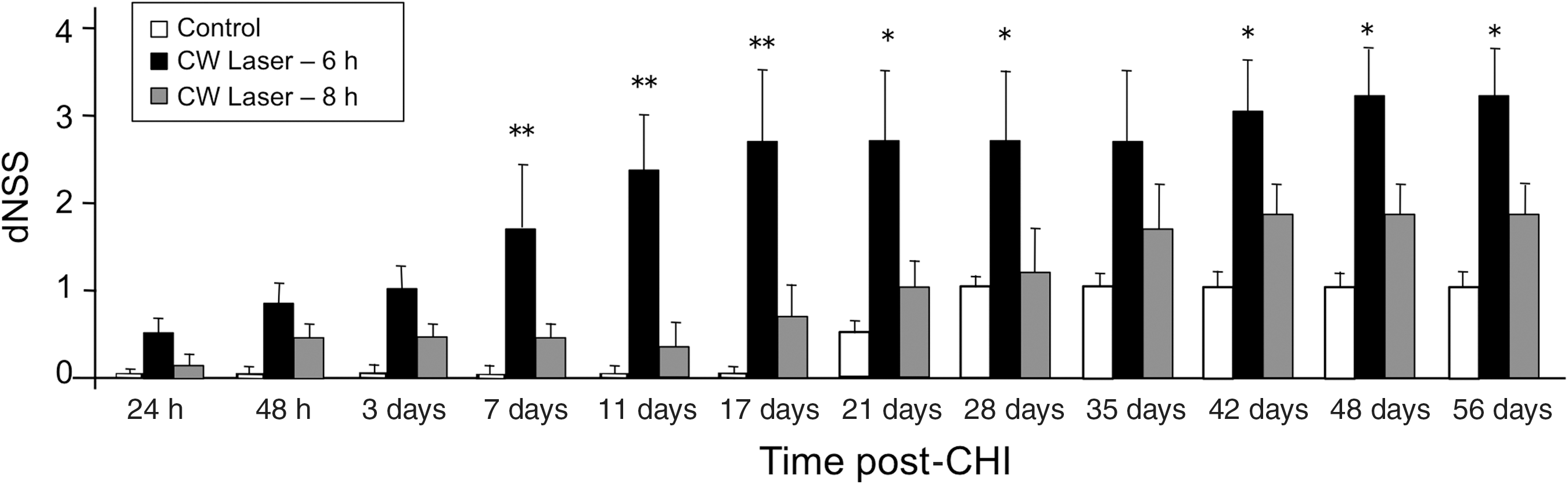
Changes (difference) in Neurological Severity Scores [dNSS=NSS1 – NSS (time)] of control non-laser-treated (open bars) and laser-irradiated mice with CW mode at 6 h (black bars), and 8 h (grey bars) post-closed-head injury (CHI). Results are expressed as mean±standard deviation (*p<0.05, **p<0.01 for laser-treated mice at 6 h post-CHI compared to controls). Statistically significant differences (p<0.05) also existed between mice treated 6 h post-CHI compared to 8 h post-CHI from 7 days until 56 days post-CHI (not shown).
Based on these results, a shorter therapeutic window was chosen, and in the second experiment laser treatment was begun at 4 h, and mice treated with the CW and the two PW modes (100 Hz and 600 Hz) were compared to control non-laser-treated CHI mice. Overall, at all time points post-CHI (24 h to 56 days), the laser-treated mice with all modes demonstrated better neurological behavior compared to the non-laser-treated mice (Fig. 2). While the laser applications with both the CW and PW modes gradually improved the dNSS of CHI mice with time up to 1 month, the non-laser-treated mice showed no improvement during this time interval. TLT at the PW 600 Hz mode demonstrated a lower dNSS during the first 20 days post-CHI compared to application at the CW and PW 100 Hz modes. However, beyond day 34 there were no statistically significant differences in the dNSS between the three modes of TLT. Nonetheless, all three modes had statistically significantly higher dNSS (p<0.05) than the control non-treated mice. These statistically significant differences in dNSS between laser-treated mice and control mice was sustained until 56 days post-CHI, when the dNSS scores of the laser-treated (all modes) mice were approximately 3.5-fold that of the control mice.
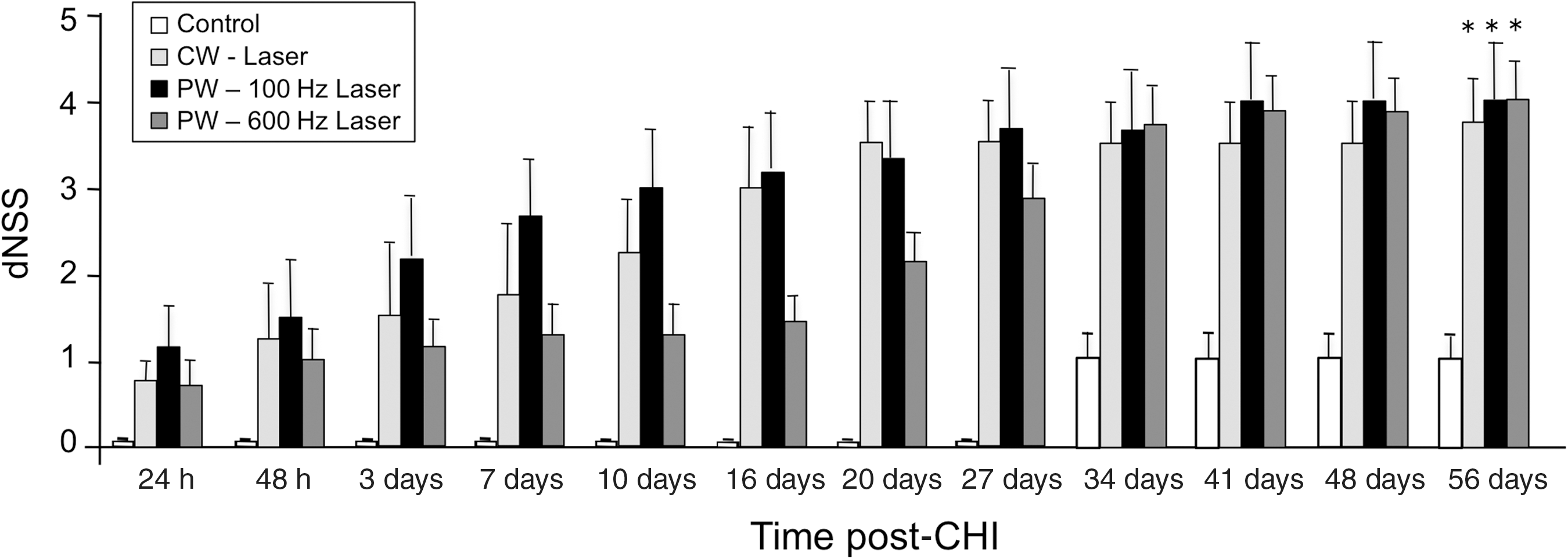
Changes (difference) in Neurological Severity Scores [dNSS=NSS1 – NSS (time)] of control non-laser-treated (open bars) and laser-irradiated mice at CW (grey bars) mode, and PW mode at 100 Hz (black bars), and 600 Hz (dark grey bars). Results are expressed as mean±standard deviation. Statistically significant differences (*p<0.05) existed at all time intervals post-closed-head injury (CHI) between the laser-treated and control mice (significance shown only for the 56-day time point).
This study also analyzed the effect of treatment on the recovery of mice by comparing the number of mice in each group in both experiments that reached full recovery by day 56 post-CHI, namely NSS=0. Figure 3 shows the percentage of mice in each of the groups that showed NSS=0 at 56 days post-CHI. It can be seen that while in the non-laser-treated control groups (combined) none of the mice completely recovered from the CHI, in the laser-treated mice 26% and 34% of the mice completely recovered from CHI when the laser was applied at the CW mode at 4 and 6 h post-CHI, respectively. In the group that received CW laser treatment at 8 h post-CHI none of the mice reached NSS=0 at 56 days post-CHI (Fig. 3). In the PW 100 Hz and 600 Hz groups, 67% and 28% of the mice, respectively, had completely recovered from CHI at 56 days post-trauma and laser application.
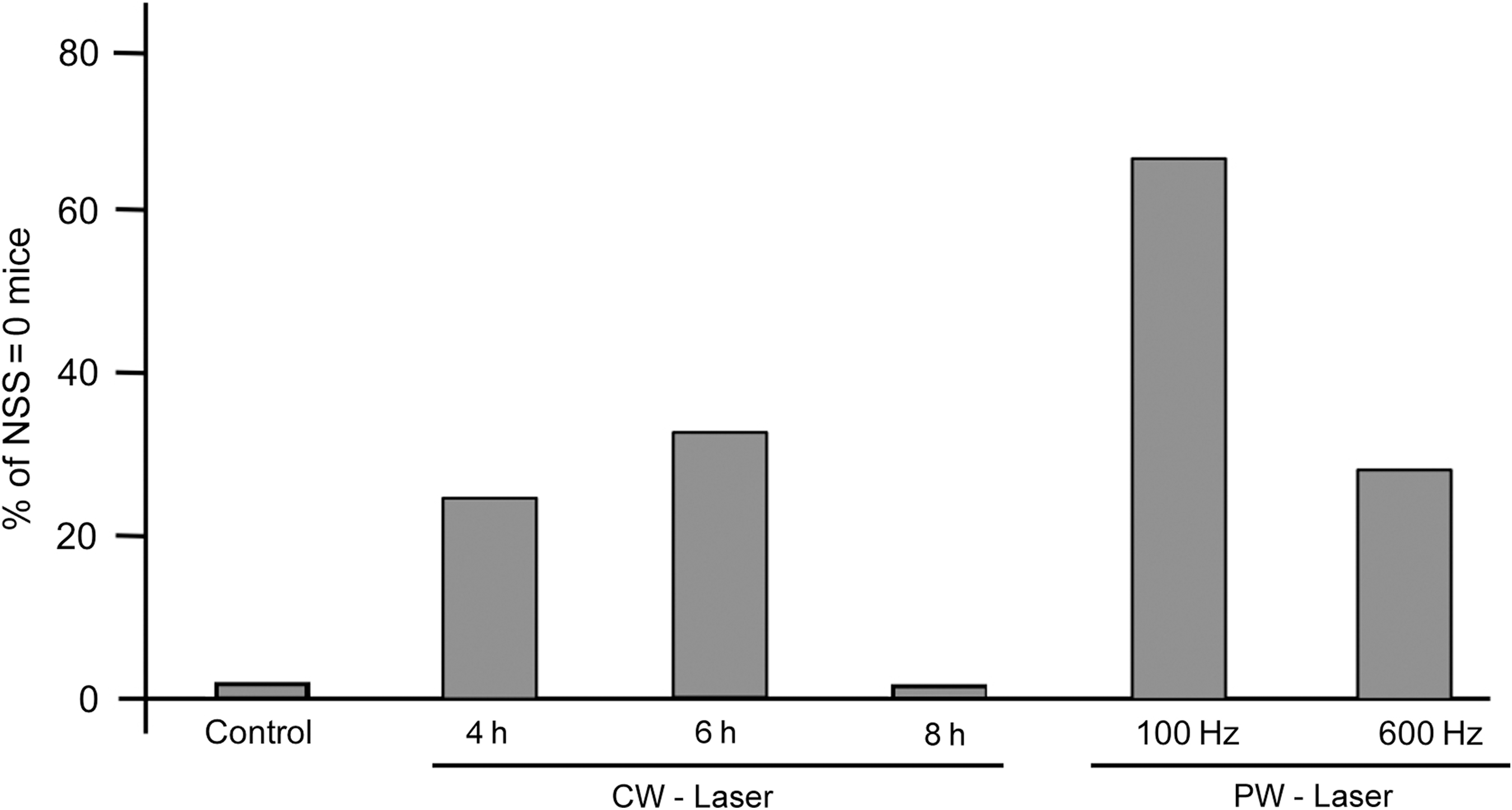
Percentage of mice out of the total number of mice in each group (combined control groups, CW or PW modes at 100 Hz and 600 Hz) demonstrating NSS=0, identical to intact mice (CW, continuous wave; PW, pulsed wave; NSS, Neurological Severity Score).
Lesion size on MRI
At 56 days post-CHI, at the end of the follow-up period, brain lesions were assessed using MRI. Figure 4 demonstrates representative MRIs of control and treated mice. Analysis of the total area of the pathological signal on MRI slices revealed that the lesion volumes (as percentages of the total brain volume) were (mean±SD) 4.8%±1.2% for control mice, and 1.4%±0.3% and 0.7%±0.5% for the CW and PW laser-treated mice, respectively. In both CW and PW laser-treated mice the lesion volume was significantly (p<0.01) lower than in the control rats. There were no significant differences between the lesion volumes of the CW and PW laser-treated mice.
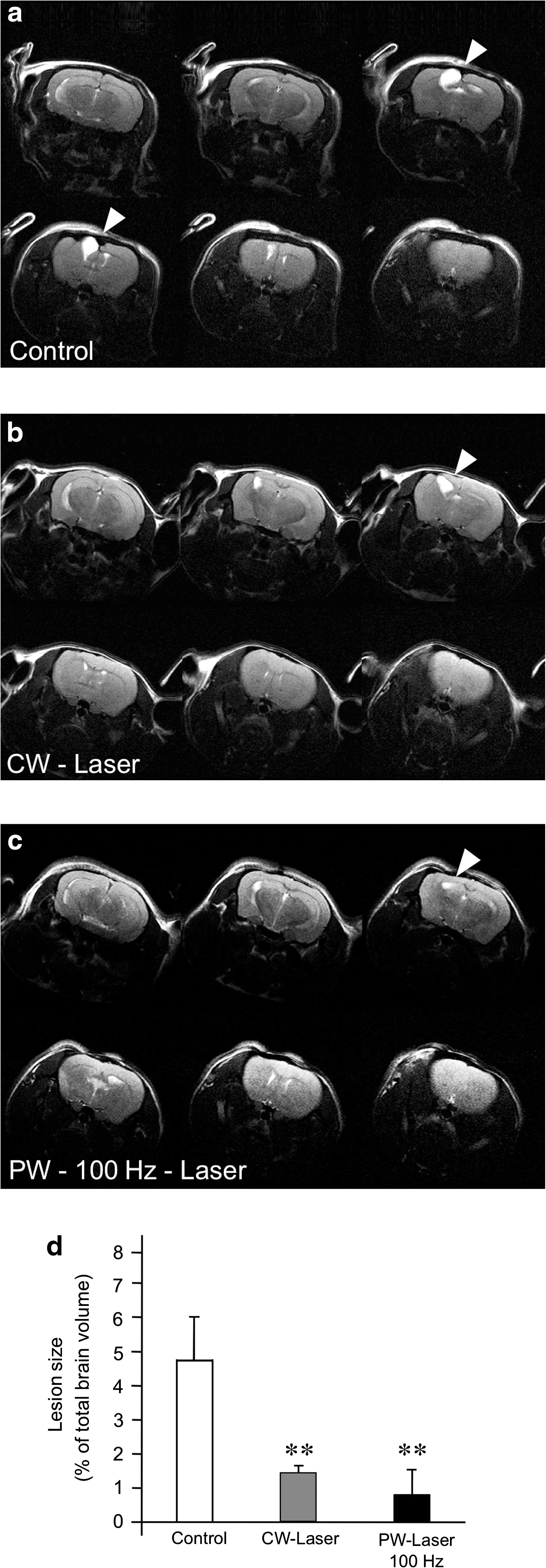
Representative micrographs of MRIs of (
Discussion
The results of the present study demonstrate for the first time that transcranial laser therapy in CW and PW modes, given at 4–8 h post-TBI to mice, improves short- and long-term (56 days) neurobehavioral function and results in smaller brain lesion volumes. These results corroborate our previous findings that TLT improved neurological behavior in mice post-TBI up to 28 days post-trauma (Oron et al., 2007). The results are also in accord with studies in rat and rabbit models demonstrating that LLLT applied transcranially improves functional outcome after stroke (Lapchak et al., 2004,2007,2008; Oron et al., 2006; Streeter et al., 2004). Indeed, it has been shown that the mechanisms of damage from cerebral ischemia and head trauma are quite similar, with a common involvement of both harmful and protective mechanisms (Leker and Shohami, 2002). In previous studies of the effect of LLLT on stroked rats, however, it was shown that the beneficial effect on neurological function was evident only at 2–3 weeks post-laser application (De Taboada et al., 2006; Oron et al., 2006), whereas in the present study the marked improvement in overall neurological function of the laser-treated mice over sham-treated control mice was already significant at 5 days post-trauma. It may be postulated that this difference in laser effects is due to the different experimental models and the effects of TLT on the physiological processes post-CHI versus post-stroke. The beneficial effect of TLT for CHI can be partially explained based on the rapid elevation of ATP content, as previously demonstrated post-laser-irradiation in the ischemic heart (Oron et al., 2001a,2001b). Furthermore, increases in total antioxidants, angiogenesis, heat-shock protein content, and anti-apoptotic activity following LLLT were found previously for ischemic heart and skeletal muscles (Avni et al., 2005; Oron et al., 2001; Shefer et al., 2002; Yaakobi et al., 2001), and can be suggested as possible processes that are also attenuated by LLLT in the ischemic/traumatic brain. It may be postulated that modulation of the above as found for the ischemic heart could also take place post-TBI in mice and cause the beneficial effects seen in this study. Recently, it was shown that TLT causes a significant elevation in ATP content in the rabbit brain (Lapchak and De Taboada, 2010). This could also partially explain the beneficial effect of TLT post-TBI, since using the same CHI model, it has been shown that ATP content was significantly decreased at the lesion site after 4 h, and in the remote cortex at 12 h post-injury (Mautes et al., 2001). Another mechanism that may contribute to the long-term improvement of neurological function seen in the laser-irradiated mice post-TBI is that of the neurogenesis that is induced by LLLT, as was found in laser-treated stroked rats (Oron et al., 2006). Neurogenesis may also partially account for the significant reduction in lesion size in the laser-treated mice compared to controls, as demonstrated qualitatively by MRI of the brains in the present study.
The results of this study also address the therapeutic window of CW TLT. It can be concluded that CW TLT may be applied up to 6 hrs post-TBI but not beyond this time interval. At 8 hrs the efficacy of CW TLT to TBI is not significant over non-treated mice, as indicated by the neurological behavioral results. It can be postulated that during the window time of 6–8 hrs post CHI processes associated with oxidative stress, release of pro-inflammatory cytokines and attenuation of inducible nitric oxide synthase activity could take place. These harmful processes once occurred prior to laser application could account for the differences in the beneficial effects of the TLT at 6 vs. 8 hours post CHI. Further studies are necessary to determine precisely which physiological processes happen between 6 and 8 hours that make TLT no longer effective. When CW TLT was applied 8 hrs post-CHI none of the mice completely recovered from the trauma, reflecting the outcome in control non-treated mice. This was not the case when CW TLT was applied 4 to 6 hrs post-CHI, where 26–34% of the mice recovered completely from the head trauma.
The present study also indicates a possible preferable mode of laser use for TLT application after injury. Although at 56 days post-CHI there were no statistically significant differences between TLT applied using the CW or the PW mode in neurological behavioral testing. The PW-100 Hz mode demonstrated a better outcome in the percentage of mice showing complete recovery over the CW- or PW-600 Hz modes. As for the superiority of pulsed laser energy at 100 Hz to 600 Hz, we have no good explanation at this time. One possible explanation of the superiority of the 100-Hz compared to the 600-Hz frequency may be associated with a resonance effect between pulsed light and brain waves (such as alpha waves and theta waves). Those waves have prominent 4- to 10-Hz rhythms (Winson, 1972), which is closer to the 100-Hz frequency than to the 600-Hz frequency. Lapchak and De Taboada (2010) also showed a higher elevation in ATP content in the rabbit brain when laser energy was applied at the PW-100 Hz mode, over CW or PW 600 Hz. It may thus be postulated that the PW-100 Hz mode is perhaps the preferable mode with which to obtain a beneficial effect after TBI.
The quantitative MRI analysis of lesion volume corroborates the above by demonstrating a lower, but not statistically significant, lesion volume in the PW mode versus the CW laser mode. We have previously shown by histological analysis using hematoxylin and eosin staining (Oron et al., 2007) that lesion volume of laser-treated mice was reduced post-CHI compared to the non-laser-treated traumatized mice. These findings are in full agreement with our present findings on lesion volume achieved by MRI, confirming that both laser modes (CW and PW) lead to a dramatic decrease in lesion volume.
The results of the present study may also have clinical relevance. The successful laser treatments were given 4–6 h post-trauma, which is a reasonable therapeutic time window for a patient to arrive at the hospital emergency room. In prior short- and long-term safety studies in rats, no alterations in functional neurological outcome or brain histopathology were found in rats that had undergone near-infrared TLT at various laser intensities and frequencies compared to control non-laser-treated rats (Ilic et al., 2006; McCarthy et al., 2010). Furthermore, the PW mode laser that was found to be optimal to obtain neurological improvement is preferable over the CW setting for transcranial application post-CHI in humans, since it may cause less overheating of skull, skin, or brain, than the CW mode at the same laser power densities (Hashmi et al., 2010; Ilic et al., 2006).
In conclusion, the present study indicates that TLT applied up to 6 h post-CHI to mice significantly promotes the long-term restoration of neurological function post-injury, and also reduces brain lesion size, as indicated by MRI of the mouse brain. The mechanism associated with this phenomenon as a potential therapy for TBI warrants further study.
Footnotes
Acknowledgment
E. Shohami is the incumbent of the Dr. Leon and Dr. Mina Deutch Chair in Psychopharmacology at the Hebrew University of Jerusalem.
Author Disclosure Statement
J. Streeter was senior officer at Photothera Inc. (1997–2009). L. Detaboada was a Photothera Inc. employee from 1997–2011. U. Oron was a Photothera Inc. employee from 2002–2003 and 2005–2007.