
Abstract
The primary objective of this study was to evaluate the safety of early warfarin resumption following burr hole drainage for warfarin-associated subdural hemorrhage (SDH). This prospective, single-arm, single-center trial was conducted from February 2008 to April 2010. Inclusion criteria were premorbid warfarin therapy, subacute or chronic SDH requiring burr hole drainage, and an International Normalized Ratio (INR) of >1.5 at presentation. Three days after surgery, warfarin was re-administered to reach the target INR range of 1.7–2.5. Patients were followed by regular INR monitoring and serial brain CT scans, which were performed at 1 week, and at 1, 3, and 6 months after surgery. The primary outcome was recurrent SDH incidence. Twenty patients were enrolled and CT scans performed at 1 week revealed no new intracranial hemorrhage in any patient. Subsequent scans were performed at 1 month on 19 patients, and recurrent SDH was observed in three. However, this recurrence rate (15.8%; 95% CI 0,34) did not exceed that of ordinary SDHs, and all recurrent SDHs were successfully managed by repeated burr hole drainage. The other 16 patients completed their 6-month follow-ups uneventfully. SDH recurrence was found to be associated with older age (≥75 years), and a thicker SDH (≥25 mm), but not with post-operative anticoagulation status. None of the study subjects experienced a thromboembolic event during the study period. Restarting warfarin therapy does not need to be withheld for more than 3 days after burr hole drainage, particularly in patients with a high thromboembolic risk.
Introduction
O
Subdural hemorrhages (SDHs), which are more prone to rebleeding than other types of OAT-associated hemorrhages (De Vleeschouwer et al., 2005; Hawryluk et al., 2010; Majeed et al., 2010), account for 43–57% of all OAT-associated intracranial hemorrhages (Butler and Tait, 1998; Kawamata et al., 1995; Majeed et al., 2010; Wijdicks et al., 1998). Acute SDHs following severe head trauma usually accompany other traumatic hemorrhages, and thus require a large craniotomy or craniectomy, whereas many OAT-associated subacute or chronic SDHs can be simply evacuated by burr hole trephination (Diamond et al., 1988; Gonugunta and Buxton, 2001; Kawamata et al., 1995). However, restarting OAT tends to be delayed for weeks or months after surgery because of the considerable risk of recurrent SDH (Gonugunta and Buxton, 2001; Majeed et al., 2010), although recurrent SDH may develop without OAT (Gonugunta and Buxton, 2001; Santarius et al., 2009; Stanisic et al., 2005; Torihashi et al., 2008). Furthermore, because patients with a high thromboembolic risk are likely to benefit from restarting OAT as soon as possible, the impact of restarting OAT on the risk of SDH recurrence needs to be determined. The objective of the present study was to evaluate the safety of early warfarin (OAT) resumption following burr hole drainage for warfarin-associated subacute or chronic SDH.
Methods
Study design
This was a prospective, single-arm, single-center trial conducted from February 2008 to April 2010. The protocol for this study was reviewed and approved by our Institutional Review Board (IRB 2008-08-053-001).
Inclusion and exclusion criteria
Inclusion criteria
Subjects meeting all of the following criteria were considered for enrolment: (1) premorbid warfarin therapy with or without antiplatelet therapy; (2) a subacute, chronic, or mixed (containing some acute hemorrhage) SDH requiring burr hole drainage; 3) an INR of >1.5 at presentation; and (4) the provision of informed consent by the patient or the patient's legal representative.
Exclusion criteria
Subjects that met one or more of the following were excluded from participation: (1) the presence of an intracerebral, epidural, subarachnoid, or intraventricular hemorrhage; (2) SDH associated with a severe trauma mechanism and cerebral contusion; (3) vascular abnormalities that might be responsible for the SDH; (4) persistent INR prolongation despite correction; (5) a prothrombotic disorder; (6) thrombocytopenia; (7) liver cirrhosis; (8) renal failure; and (9) a dependent life prior to hemorrhage.
Study protocol
To correct INR prolongation to <1.5, fresh frozen plasma (FFP) was administered intravenously with 10 mg vitamin K. This was followed by burr hole SDH drainage under local anesthesia. Residual SDH was drained using a standard silicone catheter connected to a collection bag placed in a dependent position. A post-operative computed tomography (CT) scan was performed on the day after surgery to check for residual SDH or any recurrent hemorrhage. The drainage catheter was removed on 1 or 2 days after surgery depending on the amount of residual SDH. Patients were encouraged to ambulate early.
Three days after surgery, the usual daily dosage of warfarin was re-administered to reach a target INR of 2.1 (target range 1.7–2.5) gradually under daily INR monitoring. The INR target was slightly lower than the usual therapeutic target of 2.5 (target range 2.0–3.0). When a patient was on concurrent antiplatelet therapy, the referring physician was consulted concerning the adjunctive use of antiplatelet therapy. A second CT scan was performed on post-operative day 7. Patients were discharged from hospital after confirming the absence of recurrent hemorrhage, and then followed regularly with INR monitoring. Additional brain CT scans were obtained at 1, 3, and 6 months after surgery.
Assessments of outcomes
The primary safety outcome was the incidence of recurrent SDH, documented by CT scans, within a month of surgery. The secondary safety outcomes were the incidences of recurrent SDH, any other intracranial hemorrhage, and any serious extracranial hemorrhage within 6 months of surgery. The primary efficacy outcome was the incidence of thromboembolic events within a month of surgery, and the secondary efficacy outcome was the incidence of thromboembolic events within 6 months, and an INR ≥1.7 on post-operative days 7, 14, and 30. Thromboembolic events were defined as ischemic strokes, transient ischemic attacks (TIAs), and peripheral arterial or venous thromboembolisms. Cardiopulmonary events including myocardial infarction were recorded but not considered outcome events.
Sample size and statistical analysis
The recurrence rate of ordinary SDHs has been reported to range from 9.2–28.8% after burr hole drainage (Santarius et al., 2009; Torihashi et al., 2008; Weigel et al., 2003). Assuming a minimum recurrence rate of 10%, we estimated that a sample size of 20 would be required to reject a 20% increment in the recurrence rate with a power of 80% and a one-sided significance level of 5%. Categorical data were compared using the Fisher's exact test, and continuous data were compared using the Mann-Whitney rank test. All statistical calculations were performed using commercially available software (PASW 17.0; SPSS Inc.), and p values of less than 0.05 were considered significant.
Results
Patient population
A total of 20 patients with a warfarin-associated SDH were enrolled within the study period. The study group was composed of 10 men and 10 women of mean age 65.1 years at presentation (range 33–83 years). Glasgow Coma Scale score at presentation was 9–13 in 10 patients, and 14–15 in 10 patients. Indications for warfarin therapy included a mechanical heart valve in 12 patients (10 of the 12 also had atrial fibrillation), atrial fibrillation in 5, mitral stenosis in 1, a femoral vascular graft in 1, and a cerebellar infarction related to multifocal vertebrobasilar stenosis in 1. The duration of warfarin therapy ranged from 1 month to 16 years. Eight of the 20 patients had experienced an embolic infarction or TIA prior to hemorrhage.
The CHADS2 scores, which were calculated based on the presence of congestive heart failure, hypertension, an age ≥75 years, diabetes mellitus, and stroke or TIA, were 0 in 5, 1 in 3, 2 in 5, 3 in 2, 4 in 2, and 5 in 3 patients (Gage et al., 2001). Two patients were on concurrent aspirin therapy due to infarction and recurrent TIAs related to middle cerebral artery stenosis. Another two patients with a vascular graft or vertebrobasilar stenosis were prescribed cilostazole in addition to warfarin. Six patients (30%) had a history of minor head trauma 2–10 weeks prior to hemorrhage, whereas the other 14 did not. INRs at time of admission ranged from 1.6–7.8 (mean 2.64).
Findings on initial CT scans and post-operative course
Initial CT findings included brain side affected, SDH density and maximal thickness, and degree of midline shift. In bilateral cases, the side with the larger hemorrhage was designated the primary side. Ten patients presented with a right-sided SDH, eight with a left-sided SDH, and the remaining two with bilateral SDH. CT densities were classified as high (n=7, containing some acute hemorrhage) or iso to low (n=13) compared with the cerebral cortex (Fig. 1). Maximal SDH thickness ranged from 11–34 mm (mean 20.2 mm), and the degree of midline shift ranged from 4–19 mm (mean 11.3 mm).
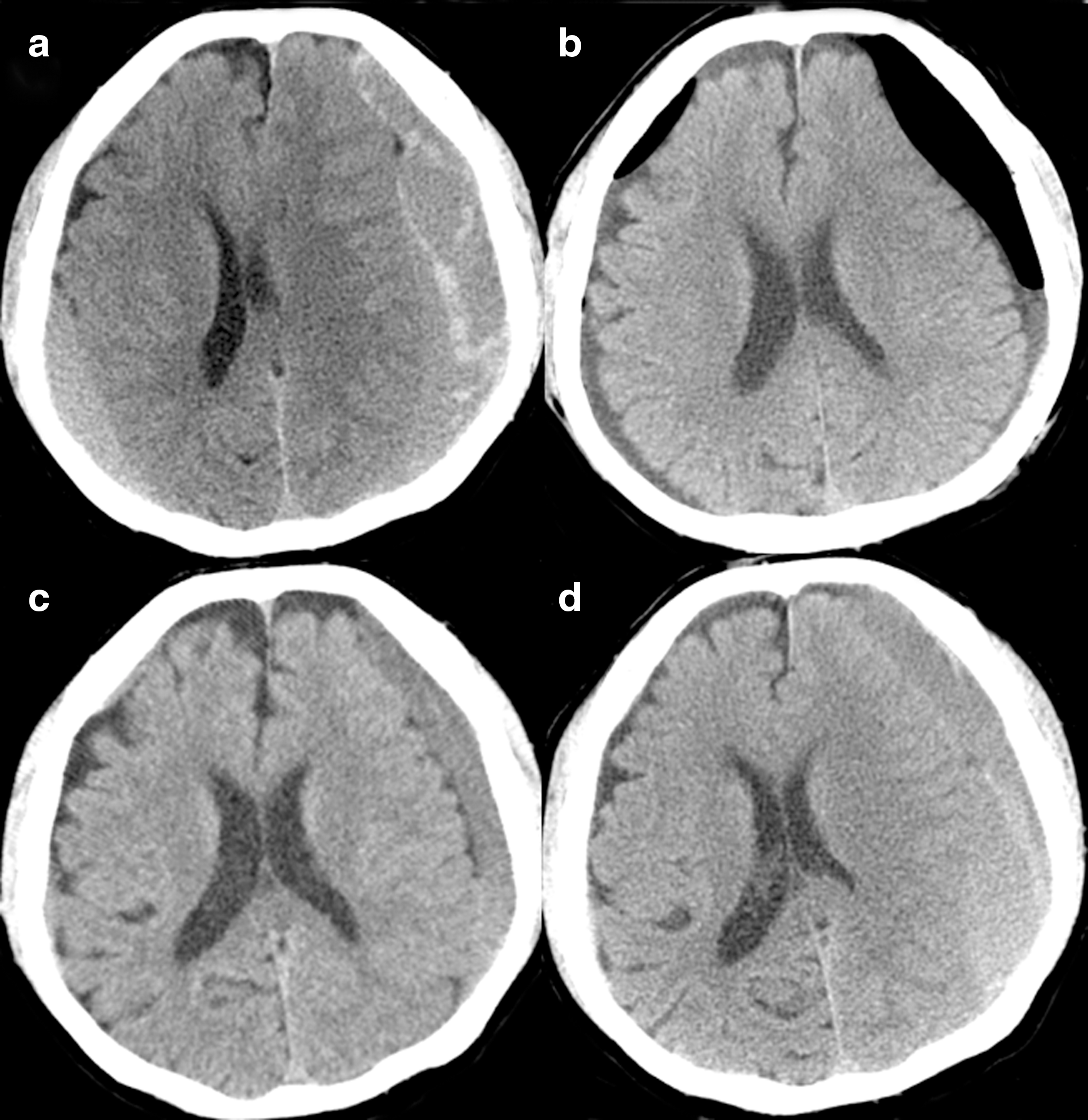
Recurrent subdural hemorrhage (SDH) in a 78-year-old male patient. The initial CT scan (
In total, 22 burr hole drainages were performed on the 20 patients. Two patients with bilateral SDH underwent simultaneous bilateral procedures. Immediately after surgery, clinical symptoms and signs improved in all patients. Post-operative CT scans performed the day after surgery revealed that SDHs had disappeared in 3 patients, mild residual SDH was seen in 10 patients, and moderate residual SDH was seen in 7 patients. No patients had a newly-developed hemorrhage on the first follow-up CT taken on the day after surgery. On the third day, warfarin was restarted at the usual daily dosage in all patients. Of the four patients on concurrent aspirin or cilostazole therapy, only one, with a CHADS2 score of 5, continued to take aspirin in accord with the referring physician's recommendation.
Findings during follow-up
In accord with the study protocol, subsequent CT scans were obtained on day 7 and at 1, 3, and 6 months after surgery. CT scans performed on the day 7 showed no significant change (n=14), or further decrements of residual SDHs (n=6). Recurrent hemorrhage was not observed in any of the 20 patients. Nineteen patients were successfully discharged from hospital a week after surgery. However, one patient, who had undergone a mechanical valve operation in the mitral (revision), aortic, and tricuspid positions a week before burr hole drainage, developed a fever 5 days after drainage. The source of infection was presumed to be an indwelling central catheter. Despite antibiotic management, this patient continued to deteriorate and expired from septic shock 1 month after burr hole drainage. Thus, this patient was excluded from the analysis.
A CT scan was performed at 1 month after surgery in the remaining 19 patients. SDH was found to have resolved completely in 7 and to have decreased further in 9, but recurrent SDH was observed in 3 (15.8%) of the 19 (Table 1). The INR was ≥1.7 in 10 patients (52.6%) on post-operative day 7, in 18 patients (94.7%) on post-operative day 14, and in 17 patients (89.5%) on post-operative day 30. The 16 patients that did not develop recurrent SDH were followed-up by CT at 3 and 6 months. Complete disappearance of SDH was noted in all 16. Other intracranial hemorrhages, serious extracranial hemorrhages, or thromboembolic events were not observed in any of the 19 patients within the 6-month study period. As for cardiopulmonary events, pulmonary edema occurred in a patient who had atrial fibrillation and mitral stenosis. This patient underwent open mitral commissurotomy 1 month after burr hole SDH drainage, and warfarin was temporarily replaced with heparin during the perioperative period.
CHADS2 score calculated based on the presence of congestive heart failure, hypertension, age≥75 years, diabetes mellitus, and stroke or transient ischemic attacks.
INR, International Normalized Ratio; SDH, subdural hemorrhage; POD, post-operative day; CT, computed tomography.
SDH recurrence
In two patients, SDH recurred in the ipsilateral hemisphere (Fig. 1), and in the other patient SDH recurred in the contralateral hemisphere. One of two with ipsilateral recurrence had taken aspirin with warfarin, and one with contralateral recurrence experienced repeated head trauma after surgery (Table 1). All three patients complained of a mild gait disturbance after recurrence and underwent repeated burr hole drainage after INR correction. Three days after surgery, warfarin was restarted (without aspirin) in two patients with cardiac disease, and replaced by cilostazole in one with a femoral vascular graft. No further hemorrhage occurred in these three patients as determined by CT scan at 1 or 3 months after repeated drainage.
Clinical data, CT findings, and anticoagulation status were analyzed to determine the potential influence of these factors on SDH recurrence within a month of surgery (Table 2). Of the variables analyzed, patient age and SDH thickness were found to be significantly associated with SDH recurrence (p=0.024 and p=0.006, respectively). All three patients that developed recurrent SDH were aged more than 75 years, and initially had a maximal SDH thickness exceeding 25 mm. Other factors included in the analysis did not reach statistical significance, although a trend toward rebleeding was observed in patients on concurrent antiplatelet medication (p=0.097). More specifically, these rebleedings were not associated with post-operative anticoagulation status measured on post-operative days 7, 14, or 30 (Fig. 2).
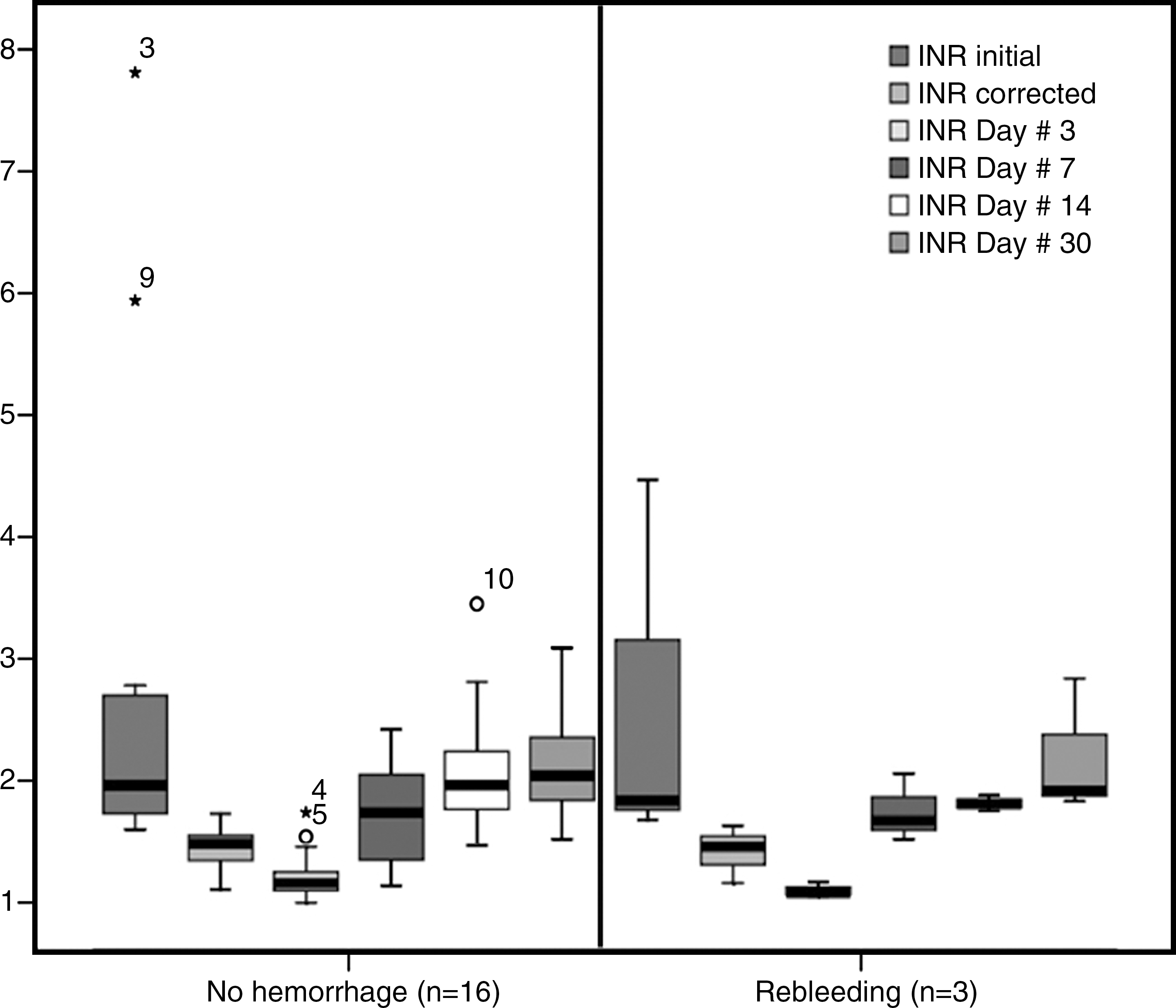
Comparison of International Normalized Ratio (INR) values.
p Value derived from the Fisher's exact test or the Mann-Whitney rank test.
Side of the brain, density, maximal depth, and midline shift determined on the side with the larger hemorrhage in bilateral cases.
CHADS2 score calculated based on the presence of congestive heart failure, hypertension, age ≥75 years, diabetes mellitus, and stroke or transient ischemic attack.
GCS, Glasgow Coma Scale; INR, International Normalized Ratio.
Discussion
Risk of rebleeding after warfarin resumption
The risk of recurrent intracranial hemorrhage after anticoagulation resumption has not been previously evaluated on a prospective basis, with the exception of a preliminary study (Leker and Abramsky, 1998), in which four patients with an OAT-associated intracerebral hemorrhage were managed with intravenous heparin. In the present study, we prospectively evaluated the risk of rebleeding while on re-initiated warfarin therapy in a homogeneous group of patients with a warfarin-associated SDH. All patients were managed by burr hole drainage and warfarin was uniformly restarted 3 days after surgery. This delay of 3 days was chosen to exclude the possibility of early rebleeding, which might have been related to incomplete anticoagulation reversal or a drainage procedure (Bertram et al., 2000; De Vleeschouwer et al., 2005; Hawryluk et al., 2010). INR was increased gradually over several days to reach the lowest effective INR range of 1.7–2.5 (Aguilar et al., 2007).
Although none of our patients suffered from rebleeding during the first post-operative week or beyond the first month, rebleeding did occur in 3 of the 19 patients during the second to fourth weeks (15.8%; 95% CI 0,34%). However, this recurrence rate is similar to that seen after ordinary chronic SDHs, which has been reported to average 15% (range 9.2–28.8%) at 1 or 2 months after burr hole drainage (Gonugunta and Buxton, 2001; Santarius et al., 2009; Shimamura et al., 2009; Stanisic et al., 2005; Torihashi et al., 2008; Weigel et al., 2003). Furthermore, we found that these rebleedings were not associated with post-operative anticoagulation status measured on post-operative days 7, 14, or 30 (Fig. 2). No extracranial or other intracranial hemorrhage occurred during the study period. Thus despite the limitations of a single-arm study design, early warfarin resumption did not appear to increase the risk of rebleeding.
On the other hand, SDH recurrence was found to be greatly affected by other factors. In particular, whereas none (0%) of the 11 patients aged <75 years experienced rebleeding, 3 (37.5%) of the 8 patients aged ≥75 years did (relative risk=1.6; 95% CI 0.94,2.74; p=0.058). Furthermore, given that 3 of the 4 patients with an SDH thickness of ≥25 mm experienced rebleeding, the risk of rebleeding increased fourfold for a maximal SDH thickness of ≥25 mm (95% CI 0.73,21.84; p=0.004). This increased risk of recurrence in elderly patients with a thicker SDH is probably best explained by a slow post-operative expansion of a severely collapsed, atrophied brain in relation to presumed tearing of parasagittal bridging veins (Markwalder, 1981; Stanisic et al., 2005; Stroobandt et al., 1995), which is likely to be further exacerbated by minor (even unrecognized) head trauma. Furthermore, premorbid or post-operative use of concurrent antiplatelet therapy may increase the risk of rebleeding due to their persistent antiplatelet effects, regardless of anticoagulation status (Hawryluk et al., 2010; Shimamura et al., 2009). Other factors previously suggested to predict SDH recurrence include hematoma density (Stanisic et al., 2005), bilaterality (Torihashi et al., 2008), and surgical technique (Santarius et al., 2009).
Timing and intensity of warfarin resumption
To balance the perceived risks of rebleeding and thromboembolism, various strategies of anticoagulation resumption have been recommended based on the results of retrospective studies. These strategies include restarting oral warfarin, intravenous heparin, or subcutaneous low-molecular-weight heparin (LMWH) at the same or a reduced intensity within 1 week (Kawamata et al., 1995; Nagano et al., 1991), or after 1–2 weeks (Furie et al., 2011; Phan et al., 2000), 3 weeks (Gonugunta and Buxton, 2001), 4–6 weeks (Crawley et al., 2000), or more than 10 weeks (Majeed et al., 2010). However, as 67% of recurrent intracranial hemorrhages were recurrent SDHs (Majeed et al., 2010), the inclusion of patients with an SDH prone to recurrence, even without warfarin therapy, might have exaggerated the risk of rebleeding after warfarin resumption, and thus delayed the timing of warfarin resumption.
The risk of ischemic stroke after discontinuing warfarin was retrospectively analyzed in 141 high-risk patients with an intracranial hemorrhage and a mechanical heart valve, atrial fibrillation, or a recurrent stroke (Phan et al., 2000). The median time not on warfarin was 10 days. Although the authors concluded that the risk of a thromboembolic event due to the discontinuation of warfarin for 1– 2 weeks was low (Phan et al., 2000; Wijdicks et al., 1998), the estimated 7-day risk of ischemic stroke was found to range from 2.6–4.8% depending on the indications for warfarin. Accordingly, patients with high embolic risk factors would benefit from restarting warfarin as soon as possible if rebleeding can be adequately managed (Hawryluk et al., 2010; Romualdi et al., 2009).
In the present study, warfarin was restarted 3 days after surgery, and no thromboembolic complications were observed during the following 6 months. However, in view of the time required for warfarin to take effect, patients may be at risk of thromboembolic complications for several days until INR has reached the therapeutic range. It has been reported that the risk of thromboembolism associated with a brief (≤5 days) periprocedural interruption in warfarin therapy is approximately 0.7% (Garcia et al., 2008). For this reason, the concomitant use of heparin or LMWH could be considered. However, the use of bridging anticoagulation therapy has not been formally studied in neurosurgical patients, and could jeopardize patients undergoing elective surgery, even those on subtherapeutic increasing doses of LMWH (Niemi and Armstrong, 2010; Niemi et al., 2009). Furthermore, in another study, the SDH recurrence rate was found to increase to 18–57% when heparin was administered during the perioperative period (Diamond et al., 1988; Zingale et al., 1999). Accordingly, it appears that the merits of bridging anticoagulation therapy require further validation.
The earlier restarting of warfarin within 24 or 48 h of surgery offers another strategy. Given that the complete reversal of the effects of preoperative warfarin takes 1 or 2 days with FFP and vitamin K administration, this strategy may be facilitated by more rapid anticoagulation reversal using prothrombin complex concentrate (Ansell et al., 2008; Morgenstern et al., 2010; Pabinger et al., 2010). Rapid INR correction can be also achieved with recombinant factor VIIa (Skolnick et al., 2010). However, recombinant factor VIIa does not replace the other factor deficiencies (Aguilar et al., 2007), and thus clotting may not be restored in vivo (Morgenstern et al., 2010; Skolnick et al., 2010).
We set the intensity of warfarin resumption in the lowest effective INR range of 1.7–2.5. However, as we found no relationship between post-operative anticoagulation status and SDH recurrence, it would appear that only a modest reduction in the incidence of rebleeding could be achieved, even with rigorous anticoagulant control. In this regard, warfarin may be safely restarted using the usual therapeutic INR range of 2.0–3.0 or more. Alternatively, the use of direct thrombin inhibitors such as dabigatran etexilate can be considered. Dabigatran has been reported to have a rapid onset of action and few drug or food interactions that do not require coagulation monitoring (Stangier, 2008). Furthermore, the rate of intracranial bleeding with this drug was less than half the rate with warfarin in a large randomized trial, with no reduction in efficacy against ischemic stroke (Connolly et al., 2009).
Study limitations
In the present study, we included only patients that underwent burr hole drainage for warfarin-associated SDH, and thus our observations cannot be extrapolated to patients with other types of hemorrhage or patients that have undergone a larger craniotomy or craniectomy. Furthermore, the lack of significance found for some comparisons could have been due to the small number of cases enrolled. In addition, outcomes could not be compared with those of non-warfarinized patients due to the single-arm study design. The fact that temporary discontinuation of warfarin is associated with a low risk of thromboembolism (Garcia et al., 2008; Wijdicks et al., 1998) indicates that a large randomized trial is required to determine the efficacy of early warfarin resumption.
Conclusions
The results of the present study highlight the lack of a definitive relationship between SDH recurrence and post-operative anticoagulation status. Furthermore, the study shows that although attention should be paid while managing elderly patients aged ≥75 years with an SDH thickness of ≥25 mm on concurrent antiplatelet therapy, even recurrent SDH can be simply and effectively managed by repeated burr hole drainage without sequelae. Accordingly, we conclude that restarting warfarin therapy does not need to be withheld for more than 3 days following burr hole drainage for warfarin-associated subacute or chronic SDH, particularly in patients with a high thromboembolic risk.
Footnotes
Acknowledgments
We would like to thank Drs. Pyo Won Park and Kiick Sung, Department of Thoracic and Cardiovascular Surgery, for patient referrals and consultations.
This work was supported by Samsung Medical Center Clinical Research Development Program Grant (#CRDP CRS-109-23-1).
Author Disclosure Statement
No competing financial interests exist.