
Abstract
Traumatic brain injury (TBI) is a major cause of death and disability and impairs health-related quality of life (HRQOL). Psychiatric disorders have been recognized as major components of TBI morbidity, yet few studies have addressed the relationship between these outcomes. Sample size, selection bias, and retrospective design, are methodological limitations for TBI-related psychiatric studies. For this study, 33 patients with severe TBI were evaluated prospectively regarding demographic, clinical, radiological, neurosurgical, laboratory, and psychosocial characteristics, as well as psychiatric manifestations and HRQOL, 18 months after hospitalization. Psychiatric manifestations were assessed using the Structured Clinical Interview for DSM-IV Axis I Disorders (SCID-I), the Hospital Anxiety and Depression Scale (HADS), the Brief Psychiatric Rating Scale (BPRS), and the Apathy Evaluation Scale (AES). HRQOL was determined using the Medical Outcomes Study's 36-item Short-Form Health Survey (SF-36). Following TBI, a significant increase in the prevalence of major depressive disorder (MDD) and generalized anxiety disorder (p=0.02), and a significant decrease in the prevalence of alcohol and cannabinoid abuse (p=0.001) were observed. The most frequent psychiatric disorders following severe TBI were found to be MDD (30.3%), and personality changes (33.3%). In comparison to patients without personality changes, patients with personality changes experienced a decline in general health and impairments in physical and social functioning. Patients with MDD showed impairment in all SF-36 domains compared to non-depressed patients. This prospective TBI-related psychiatric study is the first to demonstrate a significant association between MDD, personality changes, and HRQOL, following severe TBI in a well-defined sample of patients.
Introduction
T
Conventional ways of assessing medical outcome usually take into account only disease-specific symptoms, ignoring patient subjective difficulties in daily life activities (Strawbridge, 1998). Instruments measuring health-related quality of life (HRQOL) have been employed increasingly to fill this gap, measuring the impact of disease through a patient's perspective, and identifying the role of specific factors in the disease's burden. In the case of TBI patients, studies have shown a decrease in HRQOL compared to samples of the general population, even many years after the trauma (Jacobsson et al., 2010; Teasdale and Engberg, 2005). Although some studies have shown an association between poor HRQOL and negative emotional states or symptoms of depression or anxiety (Hawthorne et al., 2009; Steadman-Pare et al., 2001; Von Steinbuchel et al., 2010), few studies have addressed HRQOL and a full psychiatric diagnosis based on a structured psychiatric interview in TBI patients (Bombardier et al., 2010; Bryant et al., 2010).
For this study, the occurrence of psychiatric disorders following severe TBI and their association with the patients' HRQOL were investigated prospectively. The demographic, clinical, radiological, and laboratory findings, and neurosurgical data collected during hospitalization were compared between evaluated and non-evaluated patients. Finally, a comparison of demographic and psychosocial characteristics, symptomatic status, and HRQOL was performed for the most frequent psychiatric disorders diagnosed in the patient population under study.
Methods
Study sample
All participants were recruited from the Governador Celso Ramos Hospital, a Level 1 trauma center assisting a population of approximately 800,000 inhabitants of the metropolitan area of Florianópolis, Brazil, from May 2006 until September 2009. During the study period, 76 consecutive patients living in the Florianópolis (southern Brazil) metropolitan region were admitted to the intensive care unit (ICU) with severe TBI. Twenty-four (32%) died during hospitalization, three (4%) died after hospital discharge and one (1.3%) remained in a persistent vegetative state after hospitalization. Among the 48 eligible patients, 33 (68.8%) completed psychiatric and HRQOL assessment (Fig. 1). The protocol study was approved by the Human Research Ethics Committee of the Universidade Federal de Santa Catarina (UFSC). Written informed consent was obtained from relatives and patients. Psychiatric interviews were performed an average of 18.4±6 standard deviation (SD) months after TBI, between June 2008 and September 2010. The inclusion criteria were as follows: (1) severe TBI as defined by Glasgow Coma Scale (GCS) score 8 or lower within the first 48 h of admission; (2) 18 years of age or older at the time of injury; and (3) resident of the Florianópolis metropolitan area. Victims of gunshot injuries were excluded from the study.
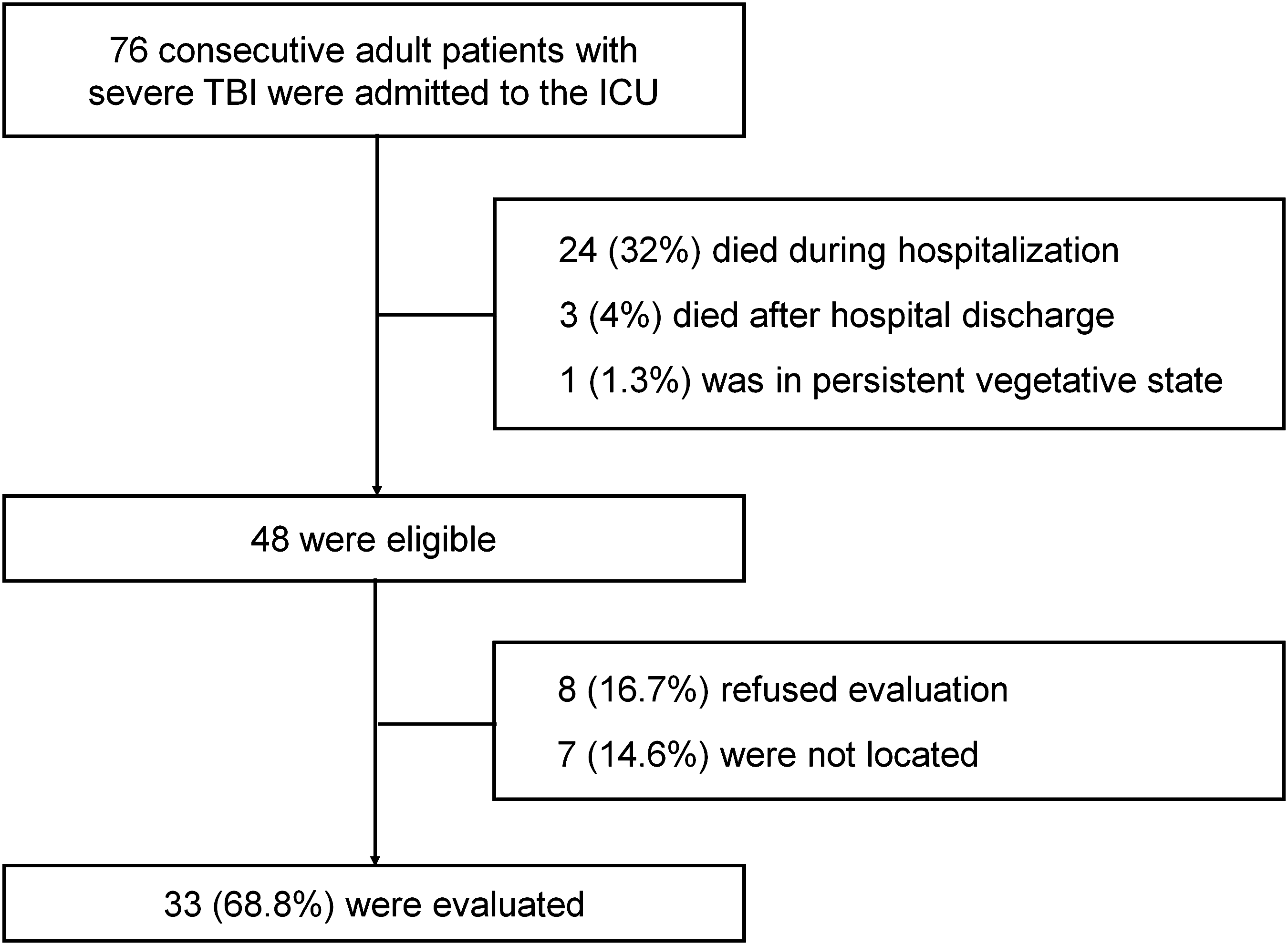
Sampling course for psychiatric and health-related quality of life evaluation of adults consecutively admitted to an intensive care unit (ICU) due to severe non-missile traumatic brain injury (TBI) an average of 18 months following trauma.
Demographic and hospitalization characteristics
Demographic, clinical, neurosurgical, radiological, and laboratory data were obtained prospectively in the emergency department and during admission to the ICU, following the research protocols developed by Martins and Gullo and their associates (Gullo et al., 2010; Martins et al., 2009), and included: gender, age, GCS score, pupillary status, computed tomography (CT) scan according to the Marshall classification (Marshall et al., 1992), the presence of subarachnoid hemorrhage (SAH) on the CT, and the presence of associated trauma (spine, thorax, abdomen, or limbs). The Marshall CT classification differentiates TBI by four types of diffuse injuries and two types of focal injuries, according to neuroradiological findings on CT. The classification is as follows: type I, diffuse injury with no visible pathology; type II, diffuse injury with present cisterns, midline centered; type III, diffuse injury and swelling; type IV, diffuse injury and shift; type V, evacuated mass lesion; and type VI, non-evacuated mass lesion. The hemodynamic and respiratory parameters, serum electrolytes, and blood gas parameters were obtained on average 12 h after injury, ranging from 6.5–19 h, early in the morning on the first day of ICU admission. The presence during hospitalization of respiratory or urinary infection, renal failure, and neurosurgical procedures were also evaluated.
Psychiatric and health-related quality of life assessment
Patients were interviewed simultaneously by two board-certified psychiatrists (A.P.D. and M.L.S.) in the outpatient clinic of the university hospital, with both interviewers blinded to all hospitalization variables. Interviews were carried out in two 1.5-h sessions with a 30-min break. Additionally, all interviews were conducted with a patient relative present, most often the parents or a close relative, who was capable of providing additional information necessary for more complete and reliable data collection. Due to the lengthy time of the evaluations, patients and their relatives were advised they could request a break at any point during the interview. The Structured Clinical Interview for DSM-IV Axis I Disorders (SCID-I; First et al., 1996) was applied to assess the Axis I psychiatric diagnosis. This tool also permits the assessment of past psychiatric disorders. In both situations (current or past diagnostic), the onset of the disorder was classified as “before” or “after” TBI, depending on the temporal relationship between the onset of symptoms and the date of the trauma. The SCID-I has been cross-culturally translated and validated in Brazil (Tavares, 1996). Personality changes that do not have a diagnosis covered by the SCID-I were determined using criteria of the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision (DSM-IV-TR). According to the DSM-IV-TR, personality changes due to a general medical condition is a diagnosis distinct from “personality disorders,” and “is characterized by a marked change in personality style and traits from a previous level of functioning. Patients must show evidence of a causative organic factor antedating the onset of the personality change” (Sadock and Pedro Ruiz, 2009). This diagnosis was assessed mainly using information gained from the relative during the interview. Thus, for this study, “personality changes” is considered to be personality changes in general, more specifically due to a severe head trauma. Depressive and anxiety symptoms were also quantified using the validated Brazilian version of the Hospital Anxiety and Depression Scale (HADS; Botega et al., 1998). The HADS is an instrument used to measure depression and anxiety in patients with general medical conditions (Zigmond and Snaith, 1983). General psychopathology was assessed by the validated Brazilian version of the Brief Psychiatric Rating Scale (BPRS; Crippa et al., 2001; Rhoades and Overall, 1988). Apathy was quantified using the Apathy Evaluation Scale (AES; Marin et al., 1991).
HRQOL was determined using the Brazilian version of the Medical Outcomes Study 36-item Short-Form Health Survey (SF-36; Ciconelli et al., 1999). The SF-36 is a widely employed instrument which consists of eight domains of health status: physical functioning, role limitations related to physical health, bodily pain, general health perception, vitality, social functioning, role limitations related to emotional problems, and mental health (Ware and Sherbourne, 1992). For each domain, a summation of item responses is linearly transformed into a score ranging from 0–100. The SF-36 has been used previously to evaluate HRQOL in TBI patients (Guilfoyle et al., 2010).
Statistical analysis
To compare dichotomous diagnostic groups, an unpaired t-test was used for continuous variables and chi-square analyses, and when appropriate, Fisher's exact tests were used for categorical data. For nonparametrically distributed continuous data, the Mann-Whitney U test was used to compare the groups among all studied variables. The significance level was set at p<0.05.
Results
Demographic and clinical characteristics of the sample
Table 1 shows the distribution of demographic and hospitalization characteristics of the evaluated and non-evaluated eligible patients. The mean age was 32.3 (SD±11.7) years, and 87.5% of the patients (n=42) were male. Evaluated subjects (n=33) and non-evaluated subjects (n=15) for psychiatric and HRQOL parameters did not differ significantly regarding gender, age, admission GCS score, pupils, Marshall CT classification, presence of SAH, surgical intervention, associated trauma, respiratory or urinary tract infection, or renal failure during hospitalization, and early hemodynamic, respiratory, and laboratory parameters after ICU admission (p>0.33).
one missing; btwo missings; cthree missings.
The patients were evaluated 18±6 (mean±SD) months after injury.
GCS, Glasgow Coma Scale; CT, cranial computed tomography; SAH, subarachnoid hemorrhage; F
Frequency of psychiatric disorders
Table 2 shows the frequency of psychiatric diagnosis in the 33 patients evaluated after the severe TBI. A significant increase in the rate of major depressive disorder (MDD; p=0.02) and generalized anxiety disorder (p=0.02) after the severe TBI was observed. A significant decrease in the rates of alcohol and cannabinoid abuse were observed as well (p=0.001). The incidence of personality changes was found to be 33.3%. The rate of other psychiatric disorders did not change significantly after TBI (p>0.15).
One patient had a depressive episode before traumatic brain injury and a manic episode after traumatic brain injury. The other patient had a depressive and a manic episode after traumatic brain injury.
p Value determined by chi-square testing.
Presence of psychiatric disorder 18±6 (mean±standard deviation) months after severe traumatic brain injury.
Health-related quality of life and psychiatric disorders
Table 3 shows demographic, psychosocial, and psychiatric characteristics, as well as HRQOL domains of patients with or without current MDD or personality changes. Patients with or without current MDD did not differ significantly regarding gender, age, education level, working status, marital status and litigation situation, presence of personality changes after TBI, or psychoactive drug abuse after TBI (p≥0.13). Patients with current MDD demonstrated lower HADS and BPRS scores than patients without current MDD (p<0.01). Apathy scores, as measured by the AES, were similar in both groups (p=0.21). In comparison to non-depressed patients, patients with current MDD showed impairment in all SF-36 domains (p≤0.02).
1 patient has never worked; b1 missing case; cSignificance level analyzed by Student's t-test; dSignificance level analyzed by Mann-Whitney U test because the distributions violated assumptions for parametric testing.
AES, Apathy Evaluation Scale; BPRS, Brief Psychiatric Rating Scale; HADS, Hospital Depression and Anxiety Scale; MDD, major depressive disorder; NA, not applicable; SF-36, Medical Outcomes Study 36-item Short-Form Health Survey.
Patients with or without personality changes did not differ significantly regarding gender, education, litigation situation, lifetime MDD, or psychoactive drug abuse following TBI (p≥0.13). Patients with personality changes showed more apathy according to the AES, and more general psychopathology according to the BPRS scales (p<0.001), compared to patients without personality changes following TBI. The presence of personality changes was not associated with HADS score (p=0.84). Concerning the SF-36 domains, patients with personality changes showed lower scores in physical and social functioning and general health (p≤0.05). These patients also showed a non-significant trend toward lower scores in the physical role (p=0.09), and the emotional role (p=0.06), of the SF-36 domains. Personality changes were not associated with bodily pain (p=0.56) nor mental health (p=0.41).
Discussion
In the present study, a representative sample of surviving patients admitted to the ICU for severe TBI was evaluated prospectively regarding their acute hospitalization variables and their subsequent psychiatric and quality-of-life status. MDD with a current depressive episode and personality changes were the most common psychiatric disorders. Both conditions were associated with impairments in HRQOL. According to the current literature, few studies assessing the association between HRQOL and full psychiatric disorders currently exist (Bombardier et al., 2010; Bryant et al., 2010; Gould et al., 2011). Despite a high prevalence in low- and middle-income countries, statistics on TBI patients in these countries are scarce, and its psychiatric consequences remain virtually unknown (Martins et al., 2009; Perel et al., 2008).
Limitations in the literature on psychiatric manifestations of TBI include the retrospective design of studies, evaluation of outpatients or referred patients, and the use of samples with heterogeneous severities of TBI. Moreover, psychiatric evaluation is frequently performed using instruments that do not correspond to the current psychiatric nosological systems, or include only measures of symptoms without a formal diagnosis of all psychiatric disorders. Finally, a lack of follow-up is common in studies of the long-term outcome of TBI, a situation that may be particularly problematic in the case of psychiatric manifestations (Corrigan et al., 2003). In the present study, we aimed to address these methodological issues by evaluating a sample of patients consecutively admitted to the ICU with severe TBI, and by using well-known, structured psychometric instruments. Structured interviews, such as SCID-I, are very useful instruments for psychiatric diagnosis in patients with neurospsychiatric disorders, including epilepsy, Parkinson's disease, and TBI (Bragatti et al., 2010; Jorge et al., 2004; Leentjens et al., 2000). Despite being considered the gold standard for psychiatric diagnosis, the current diagnostic tools used in this study may not include or may not account for confounding by some common TBI patient symptoms, such as apathy, sleep disturbance, and fatigue, and thus may have reduced validity for use in this type of study (Riggio, 2010; Seel et al., 2010). Patients who were and were not available for psychiatric and HRQOL evaluation were compared regarding their hospitalization variables to provide some insight into any significant differences that may exist between the two groups. For example, in the case of cognitive impairment, poor early clinical conditions have been related to a worse outcome (Ariza et al., 2004). However, some important psychosocial factors need to be addressed when studying variables associated with psychiatric disorders. Premorbid mental health disorders, family history of psychiatric disorders, premorbid employment status, and years of education, were some of these psychosocial factors that were not compared in this study between the evaluated and non-evaluated groups. If the evaluated patients were to be significantly different from non-evaluated patients for these characteristics, the representativeness of our sample may be overestimated. Moreover, these variables could have been a source of confounding in the analysis by influencing the prevalence of psychiatric disorders in our sample.
Several reasons exist as to why some patients refused evaluation or did not return for follow-up. For instance, some patients refused evaluation because they considered themselves to be “very well” and thus didn't need this kind of evaluation. Relatives of two patients lost to follow-up reported to the investigators that the patient “was living on the streets” or “was too aggressive to go to the hospital.”
Most patients (90%) with current MDD had onset of their disorder after TBI. This prevalence and temporal relationship are compatible with most studies on the subject, not only confirming that depression is common in head-injured patients, but also suggesting that TBI has a causal role in depression symptoms (Schwarzbold et al., 2008; Van Reekum et al., 2000). Nevertheless, despite the increased prevalence of some psychiatric disorders after neurotrauma in our sample, we cannot confirm that these disorders are a consequence of TBI. Further studies comparing severely-injured patients with and without TBI could assist in determining this association. However, Jorge and colleagues (Jorge et al., 2004) found a significantly higher prevalence of psychiatric disorders in patients with TBI than in patients without TBI who were severely injured, or with a similar degree of functional impairment, suggesting a causative relationship between TBI and depression. Some psychiatric disorders may have a delayed onset after TBI. Further prospective studies with larger sample sizes and longer patient assessment periods are necessary to better establish the relationship between severe TBI and diagnoses of psychotic disorders (Koponen et al., 2002).
As expected, depressed patients had higher scores on the HADS and BPRS compared to non-depressed patients. However, depressed patients did not differ regarding demographic and psychosocial characteristics. The mechanisms by which TBI would directly cause depression remain unclear. According to recent evidence from neuroimaging and experimental studies, although psychosocial factors are considered important (Gomez-Hernandez et al., 1997), biological factors seem to be contributing factors as well (Chen et al., 2008; Schwarzbold et al., 2010). In the TBI literature, studies on personality changes using current nosological definitions are rare. According to the DSM-IV, personality changes due to a general medical condition are defined as a persistent disturbance in the subject's previous pattern of personality with a general medical condition as a plausible causal factor. Symptoms predominantly include apathy, behavioral disinhibition, affective lability, aggression, or paranoid ideation. Using DSM-IV criteria, Pelegrín-Valero and colleagues (Pelegrín-Valero et al., 2001) found personality changes of some type in 60% of a consecutive sample of severe TBI survivors. In a preliminary study evaluating outpatients with TBI of different severities, Rao and colleagues (Rao et al., 2008) found personality changes in 32% of patients. Personality changes were associated with more severe TBI, cognitive impairment, and unemployment. In our study, personality changes also were associated positively with poor working status. Similarly to the results of the study by Pelegrín-Valero and associates (2001), apathy was the most common type of personality change, as evidenced by higher scores on the AES. As expected, these patients demonstrated more general psychopathology on the BPRS. However, they did not differ significantly regarding the presence of a major depressive episode and a poor HADS score, reinforcing the concept that apathy and depression are independent nosological conditions (Levy et al., 1998). In addition, patients with personality changes were older than those without the disorder. Similar findings have been described in the case of functional sequelae (Marquez de la Plata et al., 2008).
Patients with personality changes had lower scores on the SF-36 domains of physical functioning, general health, and social functioning, in comparison to those without personality changes. On the other hand, patients with current MDD, when compared to those without current MDD, had lower scores on all SF-36 domains. Thus these findings suggest that depression affects HRQOL in TBI patients in a more global manner, perhaps due to its wide range of symptoms, including changes in vegetative function and loss of energy. Curiously, patients with and without personality changes did not differ significantly regarding their mental health domains. Lack of awareness of the limitations caused by TBI, or even anosognosia, may underlie these findings. Giacino and Cicerone (1998) argued that impaired cognition, psychological reactions, and denial, as well as brain damage itself, may contribute to a lack of awareness of deficits following brain injury. However, the theory of impairment of quality of life as a consequence of the psychiatric disorder rather than as a result of other factors related to the trauma is questionable, especially since these other trauma-related factors (and the resulting impairment of quality of life), may be aggravating factors that contribute to the manifestation of the psychiatric disorder. Additionally, instruments designed to measure general HRQOL may not be the most appropriate for the assessment of TBI patients (Guilfoyle et al., 2010; Hawthorne et al., 2010). Apathetic patients, for example, may not report themselves as being distressed by their symptoms.
Certain limitations of this study are due in part to the current state of knowledge in the field, and thus are important to discuss. First, the size of the sample was relatively small, and despite our efforts, we were not able to locate and interview all eligible patients. Thus, in order to evaluate the representativeness of our sample, we compared patients who were and were not evaluated regarding early-phase demographic and clinical characteristics. In this comparison, the groups were not found to differ significantly by these variables. Second, we were not able to compare the levels of HRQOL in our sample to those of the general population, since there are no Brazilian norm-referenced scores for the SF-36. Finally, definitions of personality changes are poorly specified in the current psychiatric nosological systems, and the lack of compatible structured instruments is apparent. As previously mentioned, specific characteristics of TBI patients may also interfere with the interpretation of the SF-36 (Guilfoyle et al., 2010; Hawthorne et al., 2010).
Extensive efforts have been made during the last decade to develop neuroprotective strategies in TBI, yet so far results from experimental studies have not been successfully translated into clinical practice (Marklund and Hillered, 2010). The study of early mortality as a major outcome in TBI therapy is evidently fundamental. However, as new therapies emerge, refined outcome measures, such as HRQOL and psychiatric and cognitive symptomatology, will become more important. Additionally, instruments that take into account specific characteristics of TBI patients will be needed (Hawthorne et al., 2010). An immediate impact of psychiatric outcome evaluation in TBI patients will be improvements in the identification and treatment of mental disorders, which are sometimes simply accepted as normal reactions to a devastating event. The lack of more specific definitions for personality changes is remarkable, in light of their relevance and impact on the patient's life. Perhaps this reflects under-recognition of personality changes in the psychiatric setting. Little is known about the causes and mechanisms of psychiatric disorders following TBI and their relationship with the phenomenology of trauma.
Diagnostic and therapeutic decisions are based on patient prognosis, and several studies using mortality as the main outcome have identified demographic, clinical, laboratory, radiological, and neurosurgical factors as predictive markers (Gullo et al., 2010; Perel et al., 2008). In the future, well-controlled studies should investigate variables associated with the prognosis of psychiatric and cognitive disorders following TBI, to provide further insight into the mechanisms and treatment of these conditions.
Footnotes
Acknowledgments
This research was supported by Fundação de Amparo à Pesquisa e Inovação do Estado de Santa Catarina (FAPESC) and CNPq (Dr. Walz). Dr. Schwarzbold is a post-graduate fellow from CNPq (Brazil).
Author Disclosure Statement
No competing financial interests exist.