
Abstract
The optimal treatment strategy for ossification of the posterior longitudinal ligament (OPLL) depends on symptoms and is uncertain. Whether the risk of spinal cord injury (SCI) is increased in patients with cervical spinal stenosis or myelopathy caused by OPLL remains unclear. This study aimed to evaluate the risk of SCI in patients with OPLL of the cervical spine when managed with conservative treatment (no surgery). Study subjects were identified from a nationwide cohort of 26,544,883 people from 1998 to 2005 and were divided into the OPLL group (n=265), who were hospitalized for OPLL but had conservative treatment (no surgery), and the comparison group (n=5339), composed of age- and sex-matched people. Until the end of 2008, a total of 5604 subjects were followed-up for 34,723.5 person-years. The propensity score method was used to adjust for covariates. Kaplan-Meier and Cox regression analyses were performed. The incidence rate of cervical SCI in the OPLL group was found to be significantly higher than in the comparison group (4.81 versus 0.18 per 1000 person-years; p<0.001). Cervical SCI was more likely to happen in the OPLL group than in the comparison group (crude hazard ratio [HR] 25.64; p<0.001). After adjustments, the OPLL group had a 32.16-fold (p<0.001) higher risk for cervical SCI. Disability caused by SCI had an even higher risk (HR=110.72, adjusted HR=104.78; p<0.001) for the OPLL group. Therefore, cervical SCI and related disabilities are more likely to happen in OPLL patients, who should be cautioned for subsequent SCI if treated conservatively.
Introduction
O
The incidence of OPLL is higher in Taiwan, an East Asian country like Japan, than in Western societies (Inamasu et al., 2006; Tsuyama, 1984). Thus this nationwide cohort study of Taiwan analyzed the risks of SCI when OPLL is managed conservatively. The National Health Insurance Research Database (NHIRD) of Taiwan, a national database containing 26 million insurants accumulated from January 1996 to December 2008, covers 99% of the country's population. As such, the follow-up rate is inherently high and accurate for subsequent SCI events.
Methods
Data source
The NHIRD had already undergone a de-identification and encryption process. The National Health Research Institute (NHRI) recompiled the medical claims and made the data publicly available for medical researchers in Taiwan. In order to protect privacy, individual and hospital identifiers were unique to the research database as well as the researcher, and could not be used to trace individual patients or health service providers. Therefore, this study was exempted from full review by the institutional review board. Moreover, the Bureau of National Health Insurance of Taiwan performed a cross-check and validation of the medical charts and claims, which ensured the accuracy of diagnosis coding.
Study cohort
This study used a retrospective cohort composed of Taiwan's cumulative population of 26.5 million during the period from January 1, 1998 to December 31, 2005. During the 8-year interval, patients who were hospitalized for OPLL but not surgically treated were enrolled. For every participant, continuous observation began from the date of enrollment until December 31, 2008, rendering a minimum follow-up of 3 years. The flow of data processing is summarized in Figure 1.
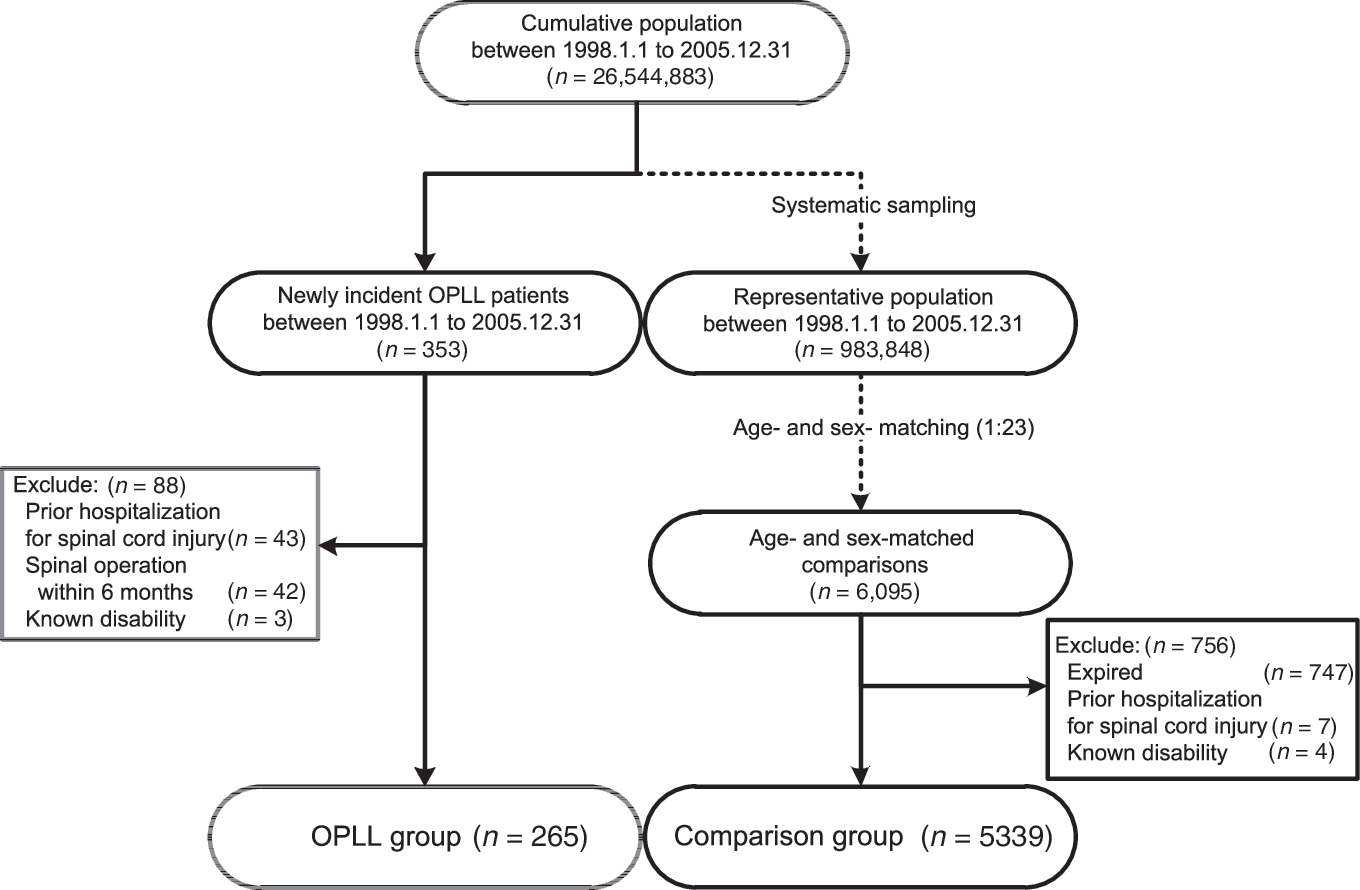
Flow of processing of the data. Study subjects were identified from a nationwide cohort of 26,544,883 people from 1998 to 2005 and were divided into the OPLL group (n=265), who were hospitalized for OPLL but had conservative treatment (no surgery), and the comparison group (n=5339), composed of age- and sex-matched people (OPLL, ossification of the posterior longitudinal ligament).
Identification of the conservatively-treated OPLL group
From the study cohort, subjects hospitalized with a first-time discharge summary containing the International Classification of Disease, 9th Version (ICD-9) code of OPLL (723.7x) during the study period were identified as patients with incident OPLL. Details of ascertaining the incidence of OPLL have been described previously (Wu et al., 2011). Those who had been hospitalized for OPLL but had not undergone any spinal intervention (i.e., spinal fusion or spinal decompression surgery) within the previous 6 months were regarded as OPLL patients managed conservatively, and were enrolled as the experimental group.
The date of the incidence of OPLL (index date) was designated as the first date of each patient's specific hospitalization. Subsequent spinal surgery was determined by any occurrence of hospitalization with procedure codes of spinal fusion (ICD-9 procedure codes 81.02-3 or 84.61-2), or spinal decompression (codes 03.02, 03.4x, 80.99, or 80.51) within the 6 months after the index date. Prior admission for cervical SCI was determined by hospitalization records with corresponding discharge diagnostic codes (ICD-9 codes 952.0x or 806.0-1) before the index date. Patients with a recorded disability before the index date in the registry of catastrophic illness were regarded as having a prior disability.
Initially, 353 OPLL patients were identified during the 8-year enrollment period. Eighty-eight patients were excluded, including 43 who were hospitalized because of cervical SCI, 42 who received spinal operations, and 3 with prior disability. A final 265 OPLL patients without prior disability or history of admission for SCI were thus enrolled as the conservatively-treated OPLL group (OPLL group) (Fig. 1).
Identification of the comparison group
A comparison group was randomly extracted from a 1-million representative cohort database at a case-control ratio of 1:23. The comparison group consisted of 6095 age- and sex-matched controls. An index date was designated as its matched case's index date (first admission date for OPLL hospitalization). However, 758 subjects were excluded due to expiration prior to their index date (n=747), hospitalization for prior cervical SCI (n=7), and previously known disability status (n=4). The final comparison group was composed of 5339 age- and sex-matched controls (Fig. 1).
Ascertainment of covariates and outcomes
Co-morbidities included osteoarthrosis (ICD-9 code 715.x), osteoporosis (code 733.0x), rheumatoid arthritis (code 714.x), diabetes mellitus (code 250.x), and hypertension (code 401-5.x), and were designated as covariates. These were determined by the presence of either diagnostic codes of outpatient records or discharge codes of hospitalization records 6 months before the index dates to the date of outcome event or the end of follow-up. To further adjust baseline differences between the groups, propensity scores were calculated by logistic regression analysis and included all covariates (Rubin, 1997).
All subjects in the OPLL and comparison groups were followed-up until the end of 2008. There were two end-points. The first, hospitalization of cervical SCI, was determined by the date of hospitalization records with a discharge diagnostic code of cervical SCI (ICD-9 code 952.0x or 806.0-1) after the index dates. The second end-point, occurrence of disabling SCI, was determined by the date registered with the catastrophic illness record for disability because of SCI (ICD-9 code 952.x). The registry of catastrophic illness patients (HV1997-2007) of the NHIRD was used to identify patients with SCI causing moderate and severe disability. Patients with severe neurological deficits like paraplegia, tetraplegia, and incontinence caused by SCI were all included. The study censored follow-ups for the following: when the subjects expired, on the dates of outcome, or at the end of this cohort (December 31, 2008).
Statistical analysis
All of the data were linked using SQL server 2008 (Microsoft Corp.) and analyzed with SPSS software (SPSS, Inc., Chicago, IL). Chi-square and independent t-test were used to assess differences in age, gender, and co-morbidities between the OPLL and comparison groups. The Kaplan-Meier method and log-rank test were used to estimate and compare the incidence rates of hospitalizations for SCI and disabling SCI. A Cox proportional hazard model with propensity scores was used to compare the incidence rates of cervical SCI and disabling SCI between the two groups after adjustment for the aforementioned covariates. A two-tailed level of 0.05 was considered statistically significant.
Results
A total of 5604 subjects (265 conservatively-treated OPLL patients, and 5339 age- and sex-matched controls) were followed-up for 34,723.5 person-years. The mean age of the OPLL group was 60.35±13.97 years (at the index dates of first hospitalization for OPLL). The overall incidence rate of hospitalized SCI was 0.37 per 1000 person-years, which was twice as high as the overall incidence rate of disabled SCI, at 0.17 per 1000 person-years. On average, the time interval between the first admission for OPLL (index date) and first hospitalization for SCI was 2.59±2.51 years, whereas the average time interval between index dates and disabled SCI was 2.52±2.54 years.
Comparison of co-morbidities
The baseline characteristics of the OPLL and comparison groups are shown in Table 1. Age, sex, and proportions of rheumatoid arthritis, diabetes, and hypertension were similar between the two groups (p=0.099, 0.494, 0.27, 0.853, and 0.363, respectively). However, osteoarthrosis and osteoporosis were higher in the comparison group (p=0.034 and p<0.001, respectively) than in the OPLL group (Table 1).
p Values were calculated using the chi-square test except for mean age, for which p values were calculated using the t-test.
OPLL, ossification of the posterior longitudinal ligament.
Incidence of hospitalized SCI and hazard ratios
Patients in the OPLL group were more likely to be hospitalized for SCI than those in the comparison group. The incidence rate of hospitalized SCI in the OPLL group (4.81 per 1000 person-years, 95% CI 2.29,10.09) was 26.7 times higher than that in the comparison group (0.18 per 1000 person-years, 95% CI, 0.08,0.40; the incidence rate ratio for the OPLL group versus the comparison group, 26.66, 95% CI 7.67,96.01, p<0.001). The crude hazard ratio (HR) for hospitalized SCI was 25.64 (95% CI 8.61,76.36, p<0.001). After adjusting for co-morbidities, the adjusted hazard ratio was 32.16 (95% CI 10.44,99.02, p<0.001), which suggested a more than 30-fold higher incidence rate in the OPLL group than in the comparison group (Table 2).
p<0.001.
Adjustments were made for patient age, gender, and propensity scores calculated by diabetes, hypertension, osteoporosis, rheumatoid arthritis. and osteoarthrosis.
OPLL, ossification of the posterior longitudinal ligament.
The cumulative incidence rate of hospitalized SCI in the OPLL group was 2.98% (95% CI 1.41,6.32%), which was significantly lower in the comparison group at 0.19% (95% CI 0.08,0.48; p<0.001 by log-rank test; Fig. 2). The cumulative incidence rate of hospitalized SCI in the OPLL group increased abruptly after the index date, and a majority of SCI in the OPLL group occurred within 2 years after the index date (the incidence rate for hospitalized SCI was 12.06 per 1000 person-years in the second year versus 3.72 per 1000 person-years in the sixth year). The median time interval between the index date and the date of SCI hospitalization was much shorter in the OPLL group than that in the comparison group (0.65 versus 3.40 years, p=0.063).
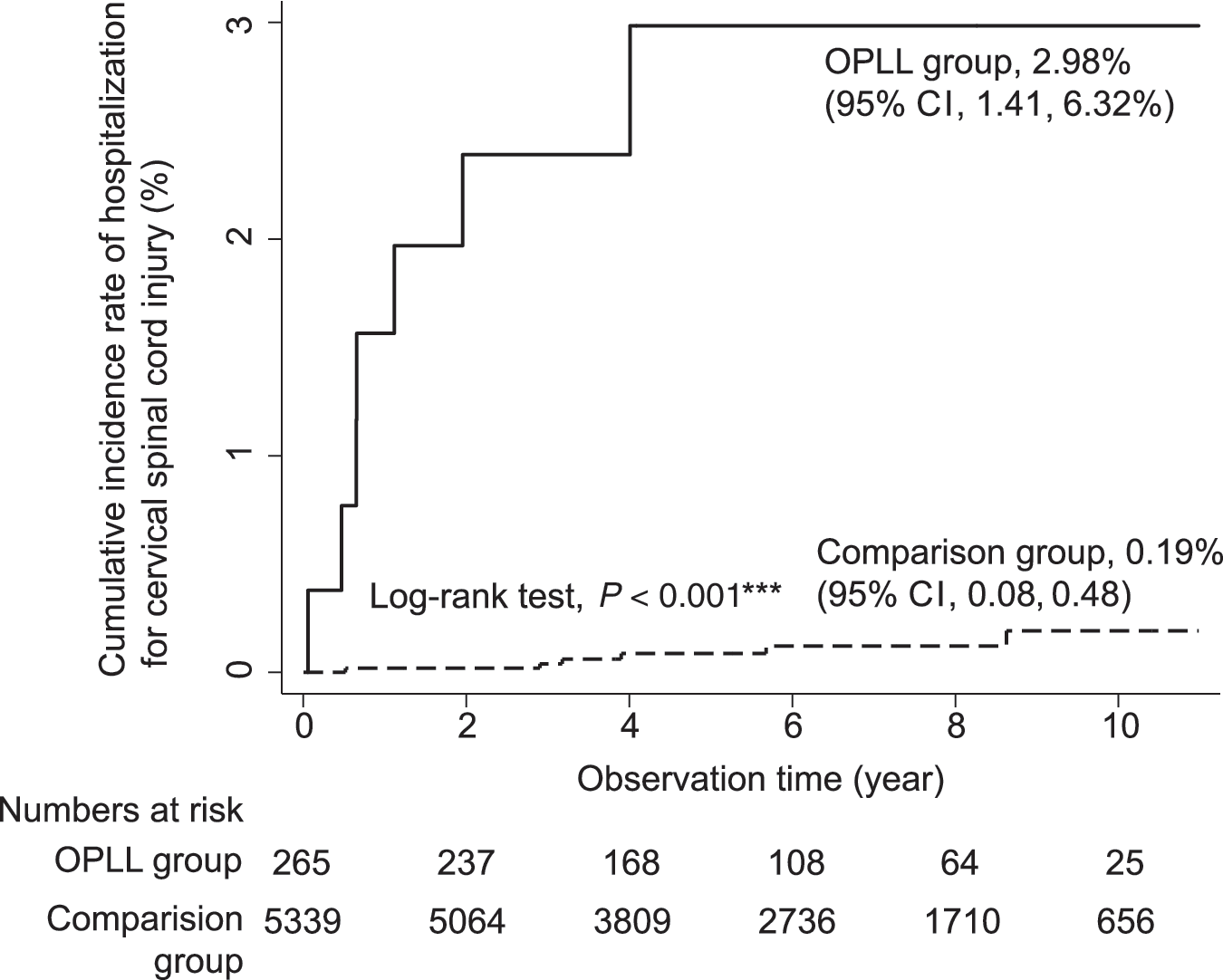
Cumulative incidence rates of hospitalized cervical spinal cord injury (SCI). The OPLL group had a significantly higher rate of hospitalized SCI than the comparison group (2.98% versus 0.19%, p<0.001 by log-rank test; OPLL, ossification of the posterior longitudinal ligament).
Incidence of disabled SCI and hazard ratios
The OPLL group was more likely to have disabled SCI than the comparison group. The incidence rate of disabled SCI in the OPLL group (3.42 per 1000 person-years, 95% CI 1.42,8.21) was 114 times higher than that in the comparison group (0.03 per 1000 person-years, 95% CI 0.004,0.21), for an incidence rate ratio of 113.62 (95% CI 12.71,5374.19, p<0.001). The crude HR for disabled SCI was 110.72 (95% CI 12.92,948.76, p<0.001), while the adjusted HR was 104.78 (95% CI 12.04,911.82, p<0.001). This suggested a more than hundred-fold higher incidence rate in the OPLL group than in the comparison group (Table 3). The cumulative incidence rate of disabled SCI in the OPLL group was 2.90% (95% CI 1.14,7.37%), which was significantly lower in the comparison group at 0.02% (95% CI 0.00,0.13; p<0.001 by log-rank test; Fig. 3). The median time interval between the index date and the date of disabled SCI was 3.38 years.

Cumulative incidence rates of disabled spinal cord injury (SCI). The OPLL group had a significantly higher rate of disabled SCI than the comparison group (2.90% versus 0.02%, p<0.001 by log-rank test; OPLL, ossification of the posterior longitudinal ligament).
p<0.001.
Adjustments made for patient age, gender, and propensity scores calculated by diabetes, hypertensions, osteoporosis, rheumatoid arthritis, and osteoarthrosis.
OPLL, ossification of the posterior longitudinal ligament.
Discussion
This study used a comprehensive national database to investigate the incidence of SCI in 265 patients with cervical OPLL managed conservatively, who were compared to 5339 age- and sex-matched controls after adjustment for co-morbidities that may predispose to SCI. The results demonstrated that these non-operatively treated OPLL patients were significantly more likely to suffer from subsequent SCI (the adjusted HRs were 32.16 for hospitalized SCI and 104.78 for SCI with disability) than patients without OPLL. This remarkable disparity in the risk of subsequent SCI warrants clinical correlation in the management of OPLL patients.
It is intuitive to infer that minor trauma or a relatively small external force can cause SCI in OPLL patients due to the underlying narrowed spinal canal (Endo et al., 1994; Wu et al., 2011). However, the assumption that these patients with spinal stenosis are prone to SCI has not been proven by clinical trials or observational cohort studies. Co-existing OPLL has been reported to be associated at a rate of 6.5–10.1% with cervical SCI in different series (Endo et al., 2009; Okada et al., 2009), but the rate of SCI in OPLL patients is not evident in the literature. This lack of information can be attributed to the rarity of both OPLL and SCI, and the difficulty of continuously following-up conservatively managed OPLL patients for a long period.
Similarly, the natural history of cervical spondylotic myelopathy, to which OPLL often contributes, is variable and treatment decisions need to be tailored (Cheng et al., 2010). The present study provides a unique longitudinal observation period across a time span longer than a decade, to demonstrate the extraordinary increase in the incidence of SCI in OPLL that is managed conservatively. The results may also shed light on the understanding of the natural history of cervical spondylotic myelopathy.
The optimal treatment strategy for OPLL patients depends on symptoms and remains uncertain. Matsunaga and associates in 2004 reported a cohort of 450 OPLL patients (Matsunaga et al., 2004). Among these 304 were managed conservatively and 146 underwent surgery. For those initially presenting without myelopathy, 71% remained myelopathy-free after 30 years. They also demonstrated no significant difference between surgical and non-surgical treatment if the patient presented with mild (Nurick grade 1 or 2) myelopathy. Surgery was advocated for myelopathy patients with Nurick grades 3 and 4, but not grade 5, which implied that severe myelopathy (Nurick grade 5) was irreversible despite surgical intervention. One caveat of their study was that 55 patients who initially had no myelopathy later deteriorated to myelopathy and crossed over to undergo surgery. Both operative and conservative management have been regarded as viable options for patients with mild cervical spondylotic myelopathy who were younger than 75 years (Matz et al., 2009). They also recommended decompression surgery for patients with cervical stenosis without myelopathy, but abnormal electromyographic findings or clinical radiculopathy because of the likelihood of developing cervical spondylotic myelopathy (Matz et al., 2009).
To date, whether the risk of SCI is increased in patients with cervical spinal stenosis or clinical spondylotic myelopathy remains unclear. The present study focuses on hospitalized OPLL patients who did not receive surgery, which implies that they were of milder clinical severity. The results also corroborate that the risk of severe neurologic deterioration caused by SCI is higher in OPLL patients, even though they are asymptomatic or mildly symptomatic.
The limitations of the current study include unidentified confounders of SCI, the small numbers of SCI patients, the lack of detailed neurological examination records, and the lack of analysis of radiographic data. Risk factors for SCI include male gender, younger age, involvement in risky physical activities, and underlying bone or joint disorders. Most known risk factors were controlled for or have been adjusted in the current study design. For unknown confounders such as the surgeon's preference of treatment a statistical adjustment model was applied. The propensity score method, indicating the likelihood of being in the OPLL group, has been incorporated into the Cox regression model to attenuate the selection bias (Rubin 1997). Moreover, the incidence of traumatic SCI is low, reportedly varying between 12.1 and 57.8 per million persons (van den Berg et al., 2010). Therefore, the current study design contains a 1:23 control group to address these issues. Under the premise of age- and gender-matched comparisons, possible influences from other major bone and joint disorders such as osteoarthrosis, osteoporosis, and rheumatoid arthritis, were adjusted. The comparison group was also deliberately large enough to allow meaningful observation for the low incidence of SCI.
The NHIRD does not incorporate records of neurological examination. It is also incapable of tracing back each individual's medical charts. The presence or severity of myelopathy upon hospitalization for OPLL or SCI is not available for analysis and may be subject to substantial variability. The mechanisms of these SCI events were also beyond the scope of this study. Nonetheless, the catastrophic illness record of the NHIRD has been used to identify SCI-associated disabilities. It also serves billing and social welfare benefits, so it is under prudent internal monitoring. Any fraudulent coding is subjected to heavy penalty, thus the accuracy of coding is assured. A recent validation study also suggests the reliability of diagnostic codes in the NHIRD (Cheng et al., 2010). Hence the number of disabled SCI patients in the current study as computed by the registry of catastrophic illness is valid and accurate. The proportion of SCI with disability serves as a proxy for the measurement of neurological function. Likewise, the lack of analysis of radiographic evaluations in these OPLL patients is an inherent limitation of this database. The length and thickness of OPLL, which might correlate with SCI, were not available in the current study. The relationship between the diameter of the spinal canal, the degree of cord compression, and the risk of myelopathy were not investigated in detail. However, the database provided a large number of patients with comprehensive follow-up. This longitudinal observation yielded some perspective of the natural course of OPLL. However, there may be patients with OPLL who have never been hospitalized and whose natural history may be different than the patients enrolled in this study. The present study is unable to ascertain how many patients who are never hospitalized for OPLL later have an SCI.
Although not perfect, the results here are valuable in the prediction of outcomes among patients with OPLL, especially for the prevention of SCI. Future larger-scale studies, longer follow-up, and a more detailed description of neurological status are required to evaluate the pathophysiology of OPLL-related SCI.
Conclusions
Cervical SCI and related disability are more likely to occur in OPLL patients. The incidence rate of SCI for conservatively managed OPLL is as high as 4.8 per 1000 person-years. Patients with OPLL treated conservatively should be observed for subsequent SCI.
Footnotes
Acknowledgments
This study was based partly on data from the NHRI database provided by the Bureau of National Health Insurance (BNHI), Department of Health, and managed by NHRI in Taiwan. The interpretation and conclusions contained herein do not represent those of the BNHI, the Department of Health, or NHRI.
Author Disclosure Statement
No competing financial interests exist