
Abstract
In general, cranioplasty is viewed as a straightforward surgical procedure, and for many years the complications associated with the procedure have been underestimated. We reviewed our 5-year experience consisting of 218 cranioplasties. Study outcomes focused specifically on the occurrence of complications after cranioplasty. Autologous bone-assisted and prosthetic cranioplasties were considered. Variables described by other authors to be associated with complications were studied, including history of previous cranioplasty, wider craniectomy size, bifrontal craniectomy, and delayed cranioplasty. We also analyzed the influence of material used for craniectomy on the occurrence of complications. The overall complication rate was 19.7%. Nineteen cases of infection (8.7%), 5 cases of postoperative wound dehiscence (2.3%), 6 cases of epidural hemorrhage (2.8%), and 13 cases of cranioplasty dislocation (5.9%) were observed. Bifrontal cranioplasties were more frequently associated with complications (p=0.01; Fisher's exact test) and infection (p<0.0001; Fisher's exact test). Postoperative wound dehiscence was more frequently observed with hand-made or custom-made cranioplasties compared with autologous cranioplasties (p=0.02). Early cranioplasty (<3 months from craniectomy) was significantly associated with cranioplasty dislocation (p=0.03). Logistical regression analysis showed that the only factor independently associated with complication was the site of cranioplasty (p=0.01). In particular, patients with a bifrontal cranioplasty had a 2-fold increased risk of complication (CI 95 1.1–3.6, p=0.017) and a 2.5-fold increased risk of developing infection (CI 95 1.3–4.9, p=0.009) compared with hemispheric/bihemispheric cranioplasty. Our analysis confirms that cranioplasty is burdened by a significant complication rate. In this context, bifrontal cranioplasty is related to a higher risk of complication and, in particular, infection.
Introduction
C
Much of the modern literature regarding cranioplasty analyzes the technical aspects of the procedure (bone flap storing procedures, timing of surgical intervention), the use of different materials, or other specific modifications to either the craniectomy or cranial repair, which may influence the cranioplasty (Aziz et al., 1990; Carvi and Hollerhage, 2006; Ducic, 2002; Flannery and McConnell, 2001; Grossman et al., 2007; Horaczek et al., 2008; Lee et al., 2007; Li et al., 2008). Patient outcome after cranioplasty has been long neglected, and several recent literature reports have shown that the complication rate after this procedure has been underestimated (Chang, et al., 2010; Gooch et al., 2009; Lee et al., 2009). A review of the risk factors associated with complications would suggest measures to improve the care of these patients.
At present, the appropriate timing of cranioplasty, the ideal material for cranial repair and possible risk factors associated with complications constitute a matter of debate (Beauchamp et al., 2010; Chang et al., 2010; Neovius and Engstrand, 2010).
The aim of our retrospective study was to provide a complete review of any risk factor that may be associated with complication, in order to identify patients at high risk.
Methods
All adult patients who had undergone cranioplasty during a 5-year period (from January 2005 to January 2010) at our Institution were identified through a search in our electronic database of cranial procedures.
Clinical data (including sex and age at the time of cranioplasty), cause of cranioplasty, size and side of the bone defect, history of previous cranioplasty, time between craniectomy and cranioplasty, material used for cranioplasty, and complications of the procedure were recorded. This series included patients who had undergone decompressive craniectomy or removal of some portions of the cranial vault after brain injury (mainly open head fracture), patients who had undergone decompressive craniectomy after cerebrovascular accidents, patients who had undergone craniectomy for tumor resection (with brain swelling), and patients with a gap in the skull caused by a previous complication needing removal of skull plate.
Three different reconstructive techniques were used: repositioning of the autologous bone flap, shaping of hand-made polymethyl methacrylate (PMMA) implants (Cranioplastic™ Codman, Johnson & Johnson Medical, Pomezia –RM, Italy) or positioning of a custom-made prosthesis. The autologous bone flap, which was removed at the time of decompressive craniectomy, was stored and refrigerated at −27° C.
If the autologous bone flap was unavailable because of the etiology of the cranial defect (e.g., trauma with exposed bone or comminuted fracture), or if the repositioning of the autologous bone flap had been unsuccessful because of infection or bone flap resorption, a prosthetic material was used.
In such cases, hand-made implants were used whenever we needed to repair a bone defect as soon as possible. If the cranioplasty timing could be delayed or whenever hand-made prosthesis could not ensure satisfactory results because of the shape and size of the bone defect, a custom-made implant was preferred.
The custom-made prostheses were made either of synthetic materials, namely PMMA (CRANOS™ SIAD Healthcare, Assago –MI, Italy) or polyether ether ketone-PEEK (Synthes, Opera –MI, Italy), or of biological macroporous hydroxyapatite (Custom bone™ Finceramica, Faenza –RA, Italy). These options required performing a preoperative transverse 1-mm spiral CT-scan with three-dimensional reconstruction of the skull, in order to define the cranial defect and consequently to shape the implant.
Surgery and follow-up
At induction of anaesthesia, patients were given 2 g cephazolin intravenously. Postoperative doses of 2 g/day were administered every 12 h for 3 days after surgery. Culture-guided antibiotics were used for patients with a recent history of infection. During surgery, great care was taken during initial dissection of tissue planes. In cases of frank frontal sinus breach during surgery, which was evident in one patient, the defect was repaired with galeal flap and Tissucol Baxter®. Autologous bone, as well as synthetic prostheses, were fixed to the skull using titanium plates and screws. In cases of hydroxyapatite implants, silk sutures were used. Central and peripheral dural hitch sutures (3.0 silk) were used in all patients, in order to prevent the occurrence of epidural hematoma. In all cases a subgaleal drainage was left in place for the first 72 h after the surgical procedure. An early postoperative (1–72 h from surgery) CT scan was performed for all patients.
All patients were followed up as outpatients for minimum 18 months. During this period, patients with trauma underwent a radiological follow-up with brain CT scan (month 1, 3, 6, 12). Patients with tumor or vascular accidents underwent a radiological follow-up with brain MRI, whose frequency varied according with the histology of the tumor or the etiology of the vascular accident; all these patients underwent a brain MRI at months 1 and 3, postoperatively. No patients were lost to follow-up. Complications related to the cranioplasty were identified. Hydrocephalus was considered a complication dependent upon the natural history of the underlying disease (e.g., tumor, brain injury, subarachnoid hemorrhage); therefore, it has not been discussed among the complications of cranial repair.
Statistical analysis
Statistical software used for analyses was SPSS (Statistical Package for the Social Sciences) 11.0 for Windows. We tried to detect potential predictors of complications. Among available clinical data, we analyzed the impact of previous cranioplasty, craniectomy side (left vs. right), type of craniectomy (bifrontal, unilateral, bi-hemispheric), timing of cranioplasty (<3 months, 3–6 months, or >6 months from craniectomy) on the occurrence of complications. Dichotomous data were compared with the Fisher's exact test. Logistical regression model was used to assess the independent contribution of predictive factors to the occurrence of complications and to the occurrence of infection alone. Significance was set at p<0.05.
Results
In the study period, 218 cranioplasty procedures were performed on 185 patients. Thirty-two patients underwent a repeat surgery and one patient needed a third intervention. There were 111 males and 74 females (age ranging from 18 to 81 years). Sixty-two patients were <29 years of age, 110 were 30–59 years of age, and 46 were >60 years of age.
The main cause of primary cranioplasty was cranial defect after brain injury and subsequent decompressive craniectomy (98 cases, 45%), followed by vascular disease (bone flap not repositioned because of brain swelling after aneurysm clipping/ intracerebral hematoma evacuation, or decompressive craniectomy for malignant middle cerebral artery infarction) in 66 cases (30.3%), neoplasia (bone flap not repositioned after tumor removal because of brain swelling) in 51 cases (23.4%), and other etiologies in the remaining 3 cases (1.3%).
The site of the defect was unilateral hemispheric in 183 cases (83.9%), 109 being right-sided and 74 being left-sided. Cranial defect was bilateral in the remaining 35 cases (16.1%), the majority being bifrontal (25 patients), with only a minority being bi-hemispheric (10 patients).
In 183 cases (83.9%), the cranioplasty was the first attempt at cranial repair, whereas the remaining 35 procedures (16.1%) followed an already failed cranioplasty. The timing of cranial repair was <3 months from craniectomy in the large majority of cases (143 cases-65.6%), from 3 to 6 months in 16 cases (7.3%), and >6 months in the remaining 59 cases (27.1%). In 135 cases (61.9%) the surgical procedure consisted of the repositioning of the autologous bone flap, custom-made cranioplasties were performed in 52 cases (23.9%) —PMMA in 15 cases, PEEK in 17 cases, porous hydroxyapatite in 20 cases—and hand-made PMMA cranioplasties were performed in 31 cases (14.2%).
The size of the bone flap removed depended upon the type of procedure being performed. In cases of decompressive craniectomy for traumatic brain injury or for malignant middle cerebral artery infarction, wide craniectomies were performed (hemicraniectomy, bilateral hemicraniectomy, bifrontal craniectomy), as described previously (De Bonis et al., 2011; Pompucci et al., 2007). In cases of unilateral hemicraniectomy, a large fronto-parieto-temporal bone flap was removed; other patients underwent bifrontal decompressive craniectomy, as described by Polin and associates (1997). In this case, frontal sinus opening (which virtually occurred in most cases during decompressive craniectomy), was repaired during the initial surgery, with meticulous extirpation of frontal sinus mucosa, followed by filling with autologous fat/muscle and Tissucol-Baxter, or with galeal flaps. For ruptured intracranial aneurysms, a standard pterional craniotomy was typically performed. The bone flap created for tumor surgeries was dependent upon the size of the lesion to be excised. The size of the cranial defect ranged from 51 cm2 to 280 cm2 (mean size 155 cm2) and was calculated with the formula of the segment of a sphere above the craniectomy area (De Bonis et al., 2010). Maximum size was obviously observed for bi-hemispheric craniectomies.
Complications
Overall, complications occurred in 43 out of 218 procedures (19.7%). Observed complications were: infection (19 cases, 8.7%), postoperative wound dehiscence (5 cases, 2.3%)—including three cases with postoperative cerebrospinal fluid (CSF) leak, epidural hemorrhage (6 cases, 2.8%), and cranioplasty dislocation (13 cases, 5.9%), including 10 cases with autologous bone flap resorption and 3 cases with hand-made/custom-made bone flap. Cranioplasty dislocation was clinically assessed and was confirmed with brain CT scans.
Bifrontal cranioplasties were more frequently associated with complications (10 out of 25 bifrontal cranioplasties, 40%), compared with unilateral hemispheric cranioplasties (30/183, 16.4%) and bi-hemispheric cranioplasties (3/10, 30%). This difference was statistically significant at univariate analysis (p=0.01).
There was no difference in the rate of complications between left and right cranioplasties. Previous cranioplasty did not constitute a risk factor for complication (20% in both patients with previous cranioplasty and in patients at first cranioplasty), nor was size of cranioplasty (<155 cm2 or ≥155 cm2, with 155 cm2 being the mean area of cranioplasty).
Timing of cranioplasty was not associated with complications, nor was the type of material used for cranioplasty (autologous bone, hand-made cranioplasty, custom-made prosthesis). Bifrontal cranioplasties were significantly associated with infection (8 out of 25 bifrontal cranioplasties, 32%) compared with hemispheric cranioplasties (10 out of 183 patients, 5,5%) or bilateral cranioplasties (1/10 patients, 10%, p<0.0001). Among cases with bifrontal cranioplasty, infection constituted the most commonly observed complication (Fig. 1). Previous cranioplasty, timing of cranioplasty and type of cranioplasty were not associated with infection. Postoperative wound dehiscence was more frequently observed with hand-made (2/31 patients) or custom-made cranioplasties (3/52 patients) than with autologous cranioplasties (0/135 patients, p=0.015).
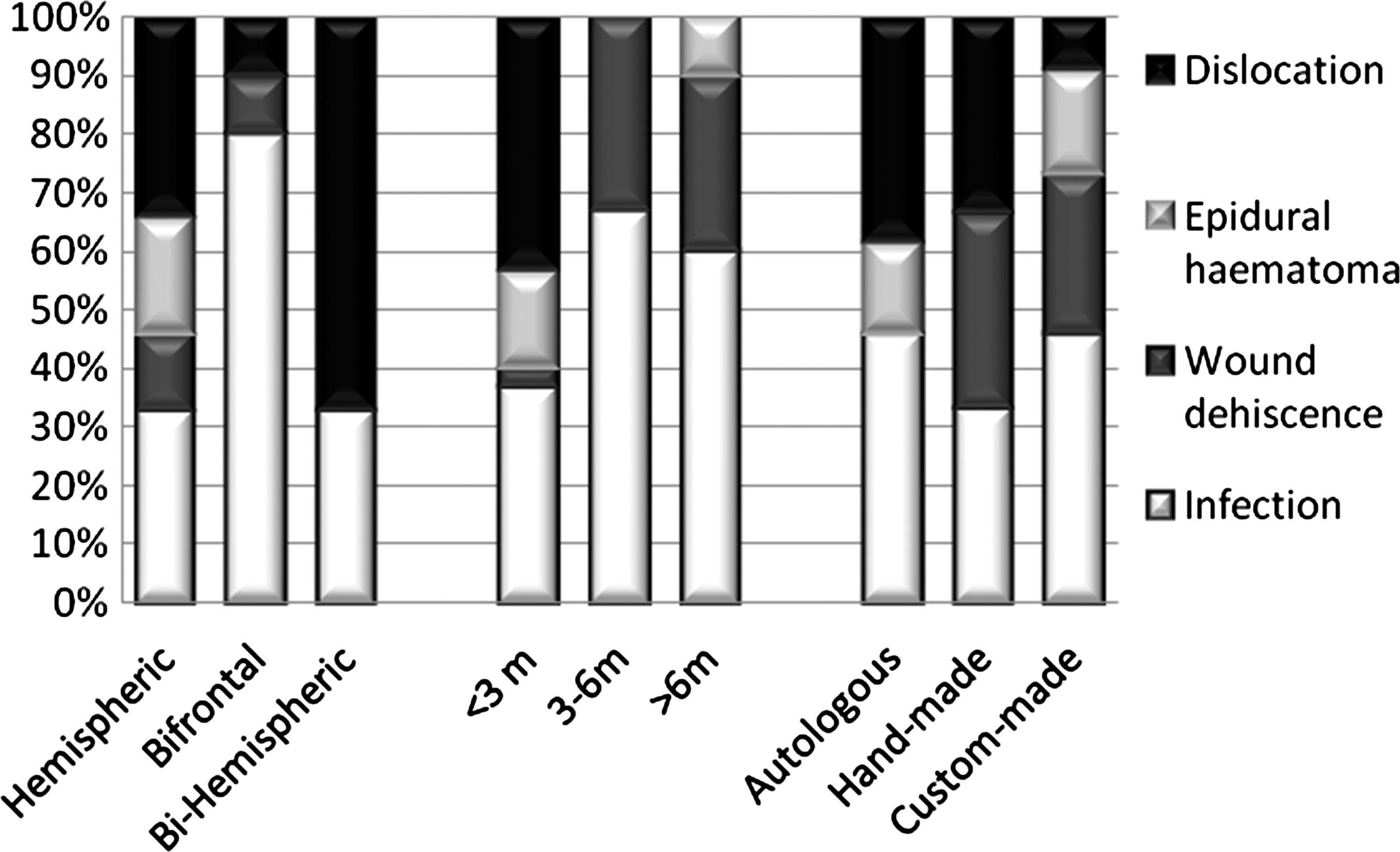
Cases with complication. Bar charts showing the relationship between type of complication and site of cranioplasty (left), timing of cranioplasty from craniectomy (center), type of cranioplasty (right). The most frequent complication of bifrontal cranioplasties was infection (80% of complications within this group), whereas the most frequent complication of bi-hemispheric cranioplasties was dislocation (67% of complications within this group). Wound dehiscence was more frequent in cranioplasties performed more than 3 months after craniectomy and in patients receiving a hand-made or custom-made implants.
No factors correlated with development of epidural hematoma.
Cranioplasty dislocation occurred in 13 patients. Ten out of 135 (7.4%) patients had cranioplasties with autologous bone flap, 2/31 (6.5%) patients had hand-made bone flap, and 1/51 patient had custom-made bone flap (2%). This difference was not significant (p=0.36). Early cranioplasty (performed within 3 months of craniectomy) was significantly associated with cranioplasty dislocation (p=0.03). All 13 patients experiencing a cranioplasty dislocation had been operated on within 3 months of the initial surgical procedure.
The rate of complications did not differ among patients with PMMA, PEEK, or porous hydroxyapatite custom-made cranioplasty.
Logistical regression analysis showed that the only factor independently associated with complication was the site of cranioplasty (p=0.01). In particular, patients with a bifrontal cranioplasty had a 2-fold increased risk of complication (CI 95 1.1–3.6) compared with patients with hemispheric/bi-hemispheric cranioplasty (p=0.017) (Table 1). Moreover, patients with bifrontal cranioplasty also had a 2.5-fold increased risk of developing infection (CI 95 1.3–4.9) compared with patients with hemispheric/bi-hemispheric cranioplasty (p=0.009) (Table 2).
Discussion
The main limitation of our study is its retrospective, non-randomized nature (these studies may overestimate the effect of treatments because of attrition, detection, difference of follow-up, or performance bias) and the different number of patients in each group.
In our study, many of these biases were avoided because no patients were lost to follow-up, the outcome and prognostic variables were standardized, and the completeness and quality of the data were carefully checked.
Cranioplasty has long been considered a conceptually intuitive and simple procedure. Recently, some authors observed that poor literature data are available on complications after cranial repair (Chang et al., 2010; Gooch et al., 2009) These authors reported that complications after cranioplasty occurred in 16–34% of patients, that is, a much larger number than after other elective cranial procedures (Chang et al., 2010; Gooch et al., 2009).
When looking at predisposing factors that may influence the rate of complications after cranioplasty, bifrontal craniectomy seems to be the central issue (Gooch et al., 2009) Older age, diagnosis of tumour rather than of trauma, timing of cranioplasty delayed over 6 months from the decompressive procedure have also been reported as relative risk factors (Chang et al., 2010). Furthermore, shorter duration of the reconstructive procedure has been speculated to be crucial for lowering the infectious risk (Lee et al., 2009).
In the present study, we reported an overall complication rate of 19.7% for cranioplasty, confirming the data reported by Chang and associates (2010; 16.4% of 213 procedures), Moreira-Gonzales and associates (2003; 23.6% of 449 procedures) and Gooch and associates (2009; 34% of 62 patients).
In our experience, only bifrontal cranioplasty resulted in a higher risk of complications with statistical significance at multivariate analysis, as already observed by Gooch and associates (2009). Wound healing complication has been exclusively noticed after a hand-made or custom-made cranioplasty, and this risk association reached statistical significance at univariate analysis. The patients receiving such an implant had already undergone at least two surgical procedures, namely craniectomy and autologous bone repositioning (with few exceptions for patients who had undergone tumor removal and cranioplasty as the second surgical procedure). Therefore, the wound healing became more difficult. Furthermore, custom-bone implants have frequently been implanted after resorption of autologous bone flap. In such cases, some degree of skin retraction has been noticed parallel to the bone resorption.
Another finding of our study was a greater incidence of cranioplasty dislocation for cases operated within 3 months of initial decompressive craniectomy.
This is not exceedingly surprising, as early cranioplasties were usually performed by repositioning the autologous bone flap. Therefore, we can speculate that dislocation mainly depends upon autologous bone flap resorption, rather than the timing of cranioplasty.
Several factors have been related to the risk of bone flap resorption (for a review see Grossman et al., 2007). The observation that bone flap resorption occurs more frequently after post-traumatic cranial repair than after other elective cranial procedures suggests that also the storage of the bone flap, the timing of its replacement, and the brain injury itself could be involved. Also, the cryopreservation was thought to compromise the function of the bone flap to serve as an osteoconductive template for remodelling growth, although more recently such damage has not been confirmed (Iwama et al., 2003; Posnick et al., 1993; Prolo et al., 1979). We did not use the alternative storage option of subcutaneous pocketing (Movassaghi et al., 2006), because it requires two abdominal surgical procedures and it does not abolish the risk of bone flap resorption.
With regard to the timing of the cranioplasty, the belief that an early skull reconstruction is associated with a poorer outcome arises from old articles concerning the treatment of penetrating brain injuries and the risk of operating on a potentially contaminated wound (Rish et al., 1979). This supposed advantage of late reconstruction is counterbalanced by a higher risk of post-craniectomy sequelae (Dujovny et al., 1997, 1999).
On the contrary, a lower complication rate has been reported if cranioplasty is performed within 3 months of craniectomy (Chang et al., 2010). A recent systematic review, instead, showed a similar infection rate between early surgery and late surgery (cutoff 3 months) (Yadla et al., 2011) Although our analysis confirms this observation, we actually prefer to replace the bone flap as soon as possible; namely, as soon as there is resolution on CT scan of brain swelling outside of the cranial vault, and the patient is not in an infectious state. An early cranioplasty carries several advantages as it allows an easier dissection of tissue planes, may allow an improvement of neurological functions and prognosis, and lowers the overall cost of care by eliminating the need for additional hospital admissions (Beauchamp et al., 2010; Liang et al., 2007).
Among all complications, infection has the greatest impact on patient outcome, as bone graft infections require surgical removal of the implanted bone graft, prolonged antibiotic therapy, and a further surgical intervention for cranioplasty. Then research on the factors influencing the rate of bone graft infection is required. The infection rate after cranioplasty reported in the literature ranges from 6% to 12% (Cheng et al., 2008; Lee et al., 2009; Matsuno et al., 2006). In this series, we reported an infection rate of 8.7%, which is in line with other reports. In our series, infection represented the most frequent complication (44% of all complications). The infection rate was similar among custom-made (9.6%), hand-made (6.5%), and autologous-bone cranioplasties (8.9%). This observation is consistent with the results of a recent systematic review by Yadla and associates (2011), but different from what was reported by Lee and associates (2009) who observed a higher incidence of infections for hand-made PMMA prostheses, and related the higher risk of infection to the increased operating time needed for hand-made PMMA cranioplasty.
In a recent series of 96 patients, Sobani and associates (2011) found a correlation between site of cranioplasty and complications. In particular, they observed that parietal cranioplasties were burdened by a higher complication rate compared with frontal and standard trauma cranioplasties. Nonetheless, these authors did not specify the extent of frontal craniectomy. Therefore, the proximity with the frontal sinuses in their series cannot be determined. We also observed that the site of cranioplasty significantly correlated with the risk of infection, with 32% of bifrontal cranioplasties subject to infection. We can speculate that this was probably partly because of the proximity of the frontal sinus, which could represent a source contamination both during surgery and after surgery, even if a prompt sinus filling is performed. The only difference we found among patients according to the site of cranioplasty was that in patients with bifrontal cranioplasty, the frontal sinus had been opened (and obliterated) during the decompressive surgery in the great majority of cases (whereas it had very rarely been opened in patients who had undergone hemicraniectomy and in patients who had undergone bilateral hemicraniectomy). The usefulness of antibiotic-impregnated cranioplasties in preventing such complications in these high-risk patients could be evaluated.
Conclusion
Cranioplasty of a bifrontal post-surgical cranial defect is related to the higher incidence of complication, especially infection. Therefore, maximal attention must be paid to seal any communication with frontal sinuses, both at the moment of the craniectomy and at the moment of cranial reconstruction, in order to minimize infectious risk.
Moreover, second-line prosthetic cranioplasties are related to a higher risk of wound complication. Therefore, skin retraction must be carefully considered in the shaping of the implant. Finally, further studies are required to identify the best option to store autologous bone flap after craniectomy and allow a subsequent effective and safe autologous bone-assisted cranial repair.
Footnotes
Author Disclosure Statement
Pasquale De Bonis received grants from Codman and from Synthes in 2010.