
Abstract
Gender may be related with the outcome of patients with acute traumatic brain injury (TBI). We explored the effect of gender on the outcome of 7145 patients with acute TBI. There was no statistical difference between male and female sex in the causes of trauma, age, Glasgow Coma Scale score, computed tomgraphy findings, and surgical management. The mortality of 7145 patients with acute TBI in males and females was 7.48% and 7.22%, respectively, with the corresponding unfavorable outcomes of 16.05% and 17.23%, respectively (p > 0.05 in both cases). The mortality of 1626 patients with severe TBI in males and females was 19.68% and 20.72%, respectively, with the corresponding unfavorable outcomes of 46.96% and 48.85%, respectively (p > 0.05 in both cases). Our data suggest that sex does not play a role in the outcome of patients with acute TBI.
Introduction
Anumber of factors may influence the outcome of patients with acute severe traumatic brain injury (TBI), including age, gender, Glasgow Coma Scale (GCS), intracranial pressure, pupillary size and response, hypoxia, and computed tomography (CT) findings. 1 –9 It has been reported that female sex may be an independent risk factor for poor or better outcome post-TBI.. 10 –14 However, other reports show that there is no difference of outcome between males and females post-TBI. 15 –18 In this study, we assessed sex differences in the outcome of 1626 patients with severe TBI.
Methods
Clinical characteristics of the patients
From December 1, 2008 through August 20, 2009, 7145 patients with acute TBI (GCS 3–15) were consecutively admitted to 47 hospitals and enrolled in the Chinese Head Trauma Data Bank (CHTDB). A total of 5427 cases (75.96%) were male and the other 1718 (24.04%) were female. The three most common causes of TBI were motor vehicle crash (3836 of 7145; 53.69%), fall (2081 of 7145; 29.13%), and violence (804 of 7145; 11.25%). The age of 7145 cases with acute TBI ranged from 1 to 92 years, and the most common age category was adults (5381 of 7145; 75.31%). The GCS was assessed in all patients within 48 hours postinjury: 1626 cases were GCS 3–8, 1222 were GCS 9–12, and 4297 were GCS 13–15, respectively. CT scanning was routinely performed in all 7145 patients. Intracranial hematomas were found in 2738 cases (38.32%), including epidural in 1076, subdural in 873, intracerebral in 425, and multiple hematomas in 364. Cerebral contusion was found in 3691 cases (51.63%), and traumatic subarachnoid hemorrhage (tSAH) was found in 3566 (49.89%). A craniotomy for removal of intracranial hematomas and/or decompression was performed in 2589 cases (36.24%); the other 4556 (63.76%) received conservative treatments. Patients were treated according to the principles described in Guidelines for the Management of Severe Head Injury. 19
Assessment of neurological outcome
Patients' neurological outcome was determined at discharge from the hospital (31 ± 5.1 days). Patients' neurological outcome was scored according to the Glasgow Outcome Scale (GOS) 20 as follows: 1, death; 2, vegetative state—unable to interact with the environment; 3, severe disability—unable to live independently but able to follow commands; 4, moderate disability—capable of living independently but unable to return to work or school; and 5, mild or no disability—able to return to work or school. Good recovery and moderate disability were designated as favorable outcomes; severe disability, a vegetative state, and death were designated as unfavorable outcomes. 4,21,22
Statistical analysis
Data were analyzed by SPSS software (version 11.0; SPSS, Inc., Chicago, IL). Patients' outcome in male and female groups was compared with the use of chi-square tests and Fisher's exact tests, as appropriate. A p value of less than 0.05 was considered significant.
Results
Clinical characteristics of patients with acute traumatic brain injury
There was no statistical difference between males and females in the causes of trauma, age, GCS score, CT findings, and surgical management (Table 1).
Clinical Characteristics of 7145 Cases With Severe Traumatic Brain Injury in the CHTDB
CHTDB, the Chinese Head Trauma Data Bank; GCS, Glasgow Coma Scale; CT, computed tomography; tSAH, traumatic subarachnoid hemorrhage.
Effects of gender on the outcome of 7145 patients with acute traumatic brain injury
Mortality of 7145 patients with acute TBI in males and females was 7.48% and 7.22%, respectively, with corresponding unfavorable outcomes of 16.05% and 17.23%, respectively (p > 0.05 in both cases; Fig. 1).
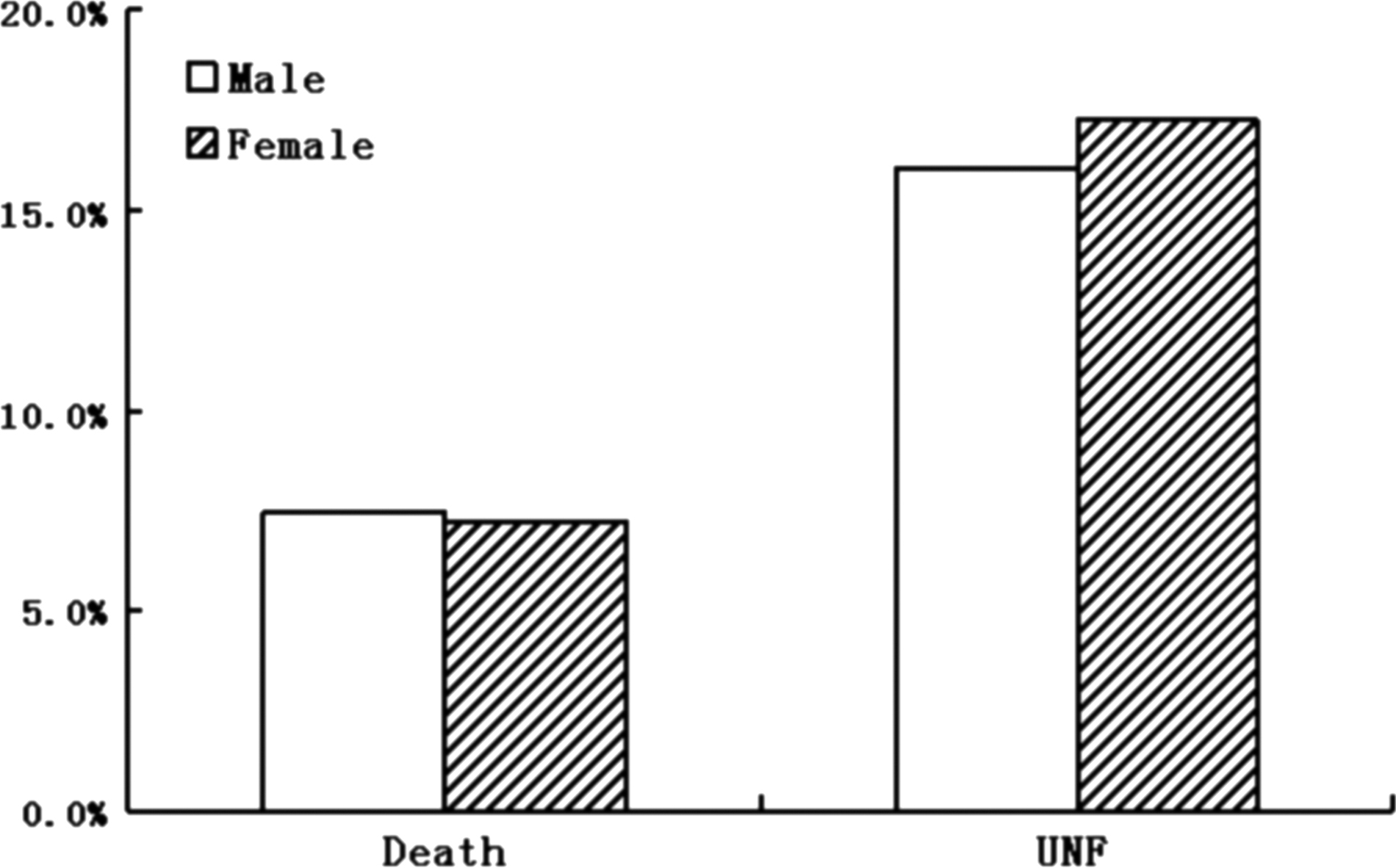
Effect of gender on mortality and morbidity of 7145 patients with severe traumatic brain injury. There is no statistical difference on the outcome of severe traumatic brain injury.
Effects of gender on the outcome of 1626 patients with severe traumatic brain injury
Mortality of 1626 patients with severe TBI in males and females was 19.68% and 20.72%, respectively, with corresponding unfavorable outcomes of 46.96% and 48.85%, respectively (p > 0.05 in both cases; Fig. 2).

Effect of gender on the mortality and morbidity of 1626 patients with severe traumatic brain injury. There is no statistical difference on the outcome of severe traumatic brain injury.
Discussion
We have found that there is no significant difference of the outcome of patients with acute TBI injury between males and females, which indicates that sex may not play a role in the outcome of patients with severe TBI.
Whether sex plays a role in the outcome of severe TBI is still controversial. Berry and colleagues have made a retrospective review of all patients with isolated moderate-to-severe TBI using data from the National Trauma Database (version 6.2; 2000–2005). Logistic regression analysis was used to determine the relationship among female sex, mortality, and development of complications after moderate-to-severe TBI. A total of 72,294 patients with moderate-to-severe TBI were evaluated. Females showed a significantly lower risk in both mortality and in developing any type of complications than the male population after adjusting for differences in patient characteristics. They concluded that female sex is independently associated with reduced mortality and decreased complications post-TBI. 10 Groswasser and colleagues have reported the effect of sex on the outcome of 334 consecutive TBI patients, including 72 females and 262 males (age range, 5–65 years). They have also found that female TBI patients had a better predicted outcome. 12 However, Ng and colleagues investigated whether there are possible sex differences in relation to outcome after closed severe TBI in a predominantly Asian population. A study has been conducted using our prospectively maintained TBI database of 672 patients with severe TBI admitted into our neurosurgical intensive care unit. Females have a significantly higher mortality and poorer outcome compared to males. 14 Kraus and colleagues have examined sex as an independent predictor of survival post-TBI. A prospective cohort of severe and moderate TBI individuals is identified from two trauma centers over a period of 3.5 years. Patients enrolled in the cohort are followed for as long as 18 months postdischarge. Overall, mortality is 1.28 times higher in females than males, with the greatest difference of 2.14 found in deaths postdischarge. Controlling for age, admission GCS, penetrating as compared with blunt injury, and the presence of multiple trauma, females are 1.75 times more likely than males to die of their TBI. Further, females are 1.57 times more likely to experience poor outcomes (i.e., severe disability or persistent vegetative state) than males. 13 Coimbra and colleagues have performed a retrospective, case-controlled study matching female patients to male counterparts for overall injury severity; hemodynamic status at admission, and head, chest, and abdomen Abbreviated Injury Scale score. An overall comparison between women (n = 914) and their male matched counterparts (n = 916) was performed. Patients were then stratified according to severity of TBI on the basis of admission GCS score into three groups: group 1, GCS score of 13–15 (788 female patients, 769 male patients); group 2, GCS score of 9–12 (40 female patients, 42 male patients); and group 3, GCS score <9 (63 female patients, 87 male patients). There was no statistically significant difference in outcome overall or in subset analysis of mild (group 1), moderate (group 2), or severe (group 3) TBI. They concluded that sex does not play a role in post-traumatic mortality or in the incidence of acute complications after any degree of TBI. 15 Leitqeb and colleagues have reported that 17 Austrian centers prospectively enrolled 863 patients with moderate and severe TBI, including 134 female and 305 male patients. Hospital mortality was 39.6% for females and 32.5% for males. Rates of unfavorable outcome were 58.7% for females and 53.4% for males. There were no significant mortality differences between females and males for factors such as age groups, trauma mechanisms, GCS scores, lesions on CT scan, or treatment factors. Logistic regression revealed that sex had no significant influence on mortality of unfavorable outcome. The differences in outcome were owing to the higher mean age of females (61.4 vs. 50.4; p < 0.001) and, possibly, because of small differences in GCS scores and in CT scores. They conclude that female sex is not an independent risk factor for in-hospital mortality post-TBI. 16
The mechanisms for different effect of sex on outcome of TBI is not clear. Arellano-Orden and colleagues assessed the role of sex as an independent factor in cerebral oxygenation variations after red blood cell transfusion (RBCT). They found differences in age, weight, mean arterial pressure, Injury Severity Score, and cerebral perfusion pressure between groups. After adjusting for these covariables, they observed that sex and age are related to increase in PbrO2. The data suggest that the effect of RBCT on cerebral oxygenation, as measured by PbrO2, is greater in women than in men. 6 Ost and colleagues have demonstrated a connection between apolipoprotein E (APOE) genotype and outcome post-TBI. A total of 96 patients with GCS < or =8 were prospectively and consecutively included. Twenty-six patients expressed APOE epsilon 4, whereas 70 patients did not. Outcome demonstrated that patients with APOE epsilon 4 had a worse outcome vs. those lacking this allele. When subdividing patients into sex, males with APOE epsilon 4 were worse, a difference not observed among female patients. The data show that APOE epsilon 4 correlates to worse outcome in TBI patients, and males with APOE epsilon 4 had a poor outcome whereas females did not. They concluded that genetic polymorphism may influence outcome post-TBI. 7 Wagner and colleagues have found that a significant sex effect is observed with F2-isoprostane/lactate/pyruvate. Females had a significant inverse relationship between day 1 F2-isoprostane/glutamate ratios and GOS scores as well as day 1 F2-isoprostane/lactate/pyruvate ratio and GOS scores. These results indicate that females had smaller oxidative damage loads than males for a given excitotoxic or ischemic insult, and female gonadal hormones may play a role in mediating this neuroprotective effect. 25 Bayir and colleagues have evaluated the effect of gender on lipid peroxidation (LPO), as assessed by cerebrospinal fluid (CSF) levels of F2-isoprostane, after severe TBI in humans. LPO was assessed in CSF from 68 adults after severe TBI. F2-isoprostane was approximately 2-fold higher in males than females. They suggest that LPO occurs early after severe TBI in adults and is more prominent in males versus females. 26
In summary, although some previous reports show different effects of sex on the outcome of acute moderate-to-severe TBI, our data strongly suggest that sex does not play a role in the outcome of patients with acute TBI.
Footnotes
Acknowledgments
This work was supported by grants from National Health Science Grant (no. 200802093), National Key Basic Research Project (no. 2012CB518100), Science and Technology Committee of Shanghai (nos. 10JC1409800 and 08411951900), and Program for Shanghai Outstanding Medical Academic Leader. The authors thank Dr. Jin-fen Zhu for assistance with statistical analysis.
Author Disclosure Statement
No competing financial interests exist.