
Abstract
Clinical reports and case studies suggest that traumatic brain injury (TBI) can have significant social consequences, with social dysfunction reported to be the most debilitating problem for child and adolescent survivors. From a social neuroscience perspective, evidence suggests that social skills are not localized to a specific brain region, but are mediated by an integrated neural network. Many components of this network are susceptible to disruption in the context of TBI. In early development, a brain injury can disrupt this neural network while it is in the process of being established, resulting in social dysfunction. In order to clarify the prevalence and nature of social dysfunction after child TBI, studies of social outcomes in children and adolescents after TBI over the last 23 years have been reviewed. Despite casting a wide net initially, only 28 articles met review criteria. These studies were characterized by methodological weaknesses, including variations in definitions of TBI, limited assessment tools, reliance on parent reports, small sample sizes, and absent control groups. Despite these limitations, the weight of evidence confirmed an elevated risk of social impairment in the context of moderate and severe injury. While rarely examined, younger age at insult, pathology to frontal regions and the corpus callosum, and social disadvantage and family dysfunction may also increase the likelihood of social difficulties. More research is needed to obtain an accurate picture of social outcomes post-brain injury.
Introduction
S
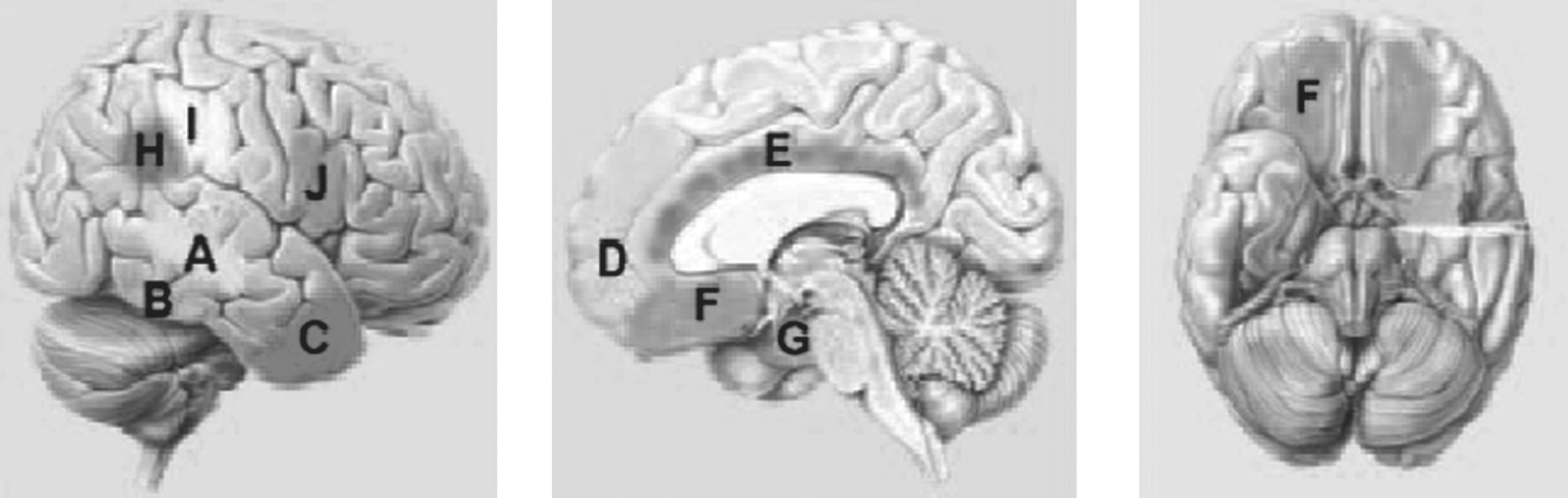
Brain regions contributing to the social brain network: (
In response to a largely atheoretical approach to the treatment of the social consequences of child TBI in the literature to date, more recent empirical work has drawn on theoretical models from normal development, developmental psychopathology, adult TBI studies, and the social neurosciences. A number of conceptual frameworks have now been described that each incorporate compatible components and assumptions (Beauchamp and Anderson, 2010; Crick and Dodge, 1994; Guralnick, 1999; Masten et al., 1999; Yeates et al., 2007). Importantly, these approaches highlight developmental principles and the unique characteristics of early disruption, and its capacity to derail both social functions and their underlying neural substrates. They also attempt to clearly define the key components of social function, including social information processing, social interaction, and social adjustment (Figs. 2 and 3). Current models also acknowledge the important contribution of cognitive abilities (e.g., attention, communication, and social cognition) to social outcomes.
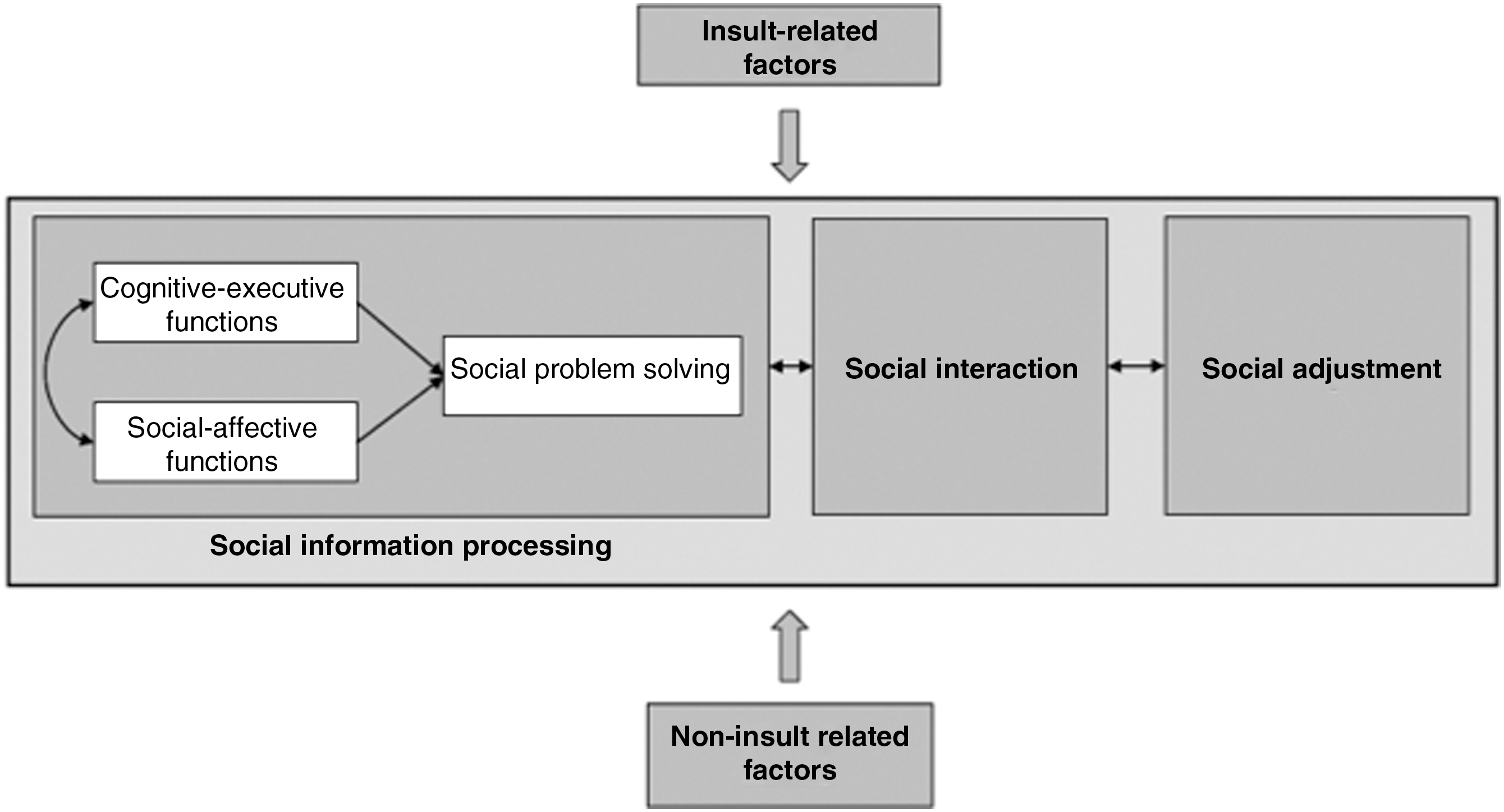
Shown here is the integrative multilevel model of social competence in children with brain disorders by Yeates and associates (Modified from Bigler et al., 2007.)
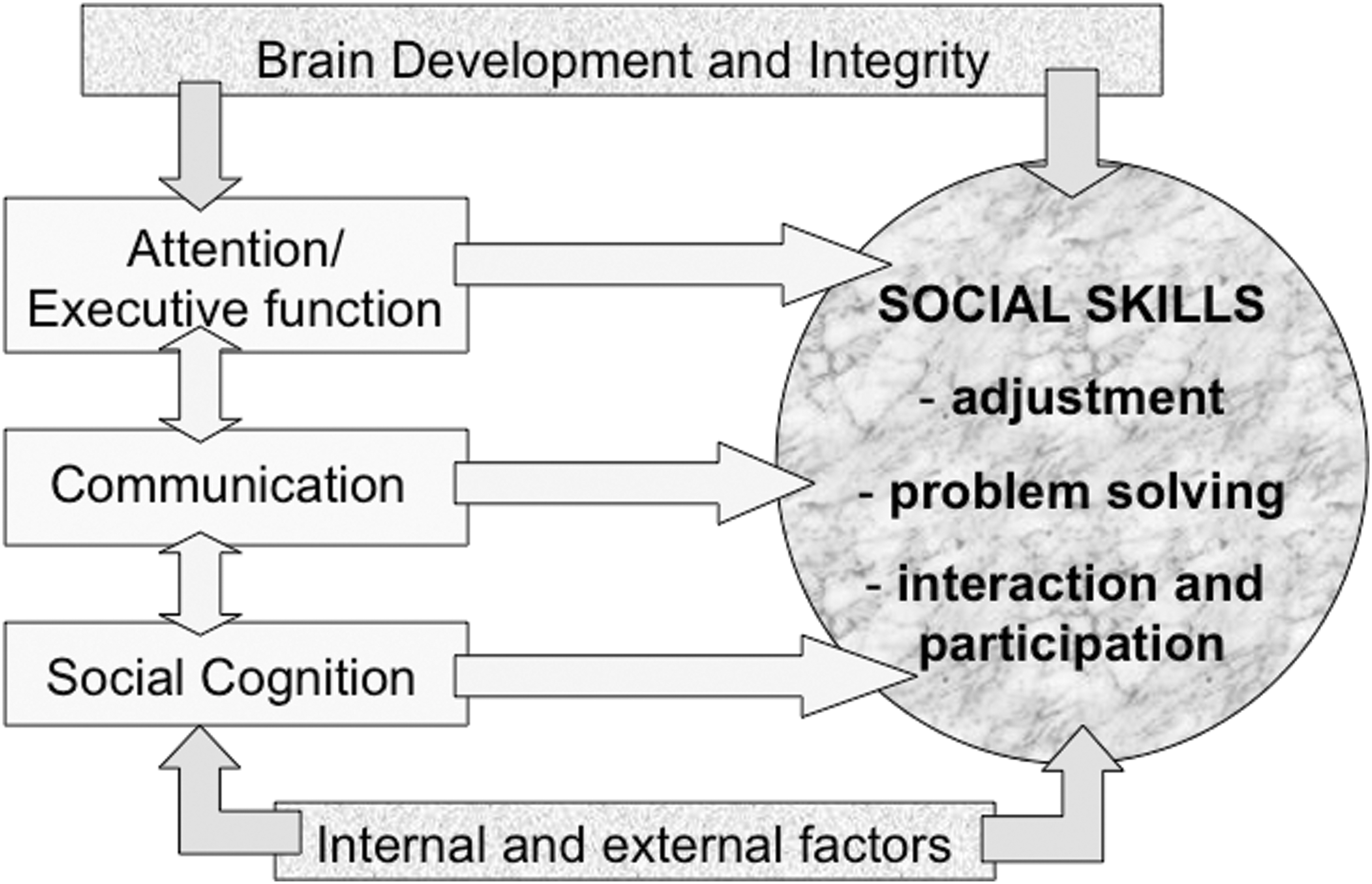
The Socio-Cognitive Integration of Abilities Model (SOCIAL) (Modified from Beauchamp and Anderson, 2010.)
Utilizing a developmental neuroscience framework it is reasonably well established that social outcomes are influenced by brain development and brain integrity (e.g., age and injury factors), as described above. In contrast, child TBI research is only just beginning to consider other important influences on social function, such as environmental factors (e.g., parenting style, family function, and socioeconomic status), and individual attributes (e.g., temperament and disability; Fig. 2). Of note, the importance of the child's environment is already established in the developmental psychology literature, with distal factors, such as socioeconomic status, and more proximal influences, such as family environment, implicated in the development of social function (Ackerman and Brown, 2006; Bowlby, 1962; Bulotsky-Shearer et al., 2008; Guralnick, 1999; Masten et al., 1999).
Prior to the 1990s the child TBI literature reveals some clinical commentary on social outcomes (e.g., Brown et al., 1981; Klonoff, 1971; Lehr, 1990; Rutter, 1983), but until that time the majority of research in this area was focused on physical and cognitive outcomes. In keeping with the emergence of social neuroscience, research has now begun to address social outcomes. The seminal early work of Stephen Anderson, Paul Eslinger, and their colleagues documented detailed case studies of patients with early brain damage and their long-term socio-moral impairments (Anderson et al., 2000; Grattan and Eslinger, 1992), providing rich clinical insights into the impact of early injury on social abilities, and the potential mediating role played by high-level cognitive skills (e.g., executive function and communication skills). Empirical research has begun to build on this early work (Anderson et al., 2005; Didus et al., 1999; Hanten et al., 2008; Janusz et al., 2002). Although not directly assessing links between these deficits and social function, these studies have provided a platform for conceptualizing the presence of social dysfunction. Only a very small number of studies have attempted to examine possible links between specific cognitive domains implicated in social function and social outcomes (Ganesalingham et al., 2007a,2007b; Muscara et al., 2008), with early results supporting the presence of such relationships.
In order to clarify the impact of TBI on social function in children and adolescents, a thorough review of the current literature is needed. This article aims to systematically review all studies of social outcome after TBI in children and adolescents completed over the last 23 years, with the objective of identifying methodologically rigorous studies, and establishing common findings.
Methods
To review the literature addressing social outcomes from child TBI, the terms prosocial behavior, social adjustment, social cognition, social competence, social function, social interaction, social outcomes, and social skills, were combined with head injury/brain injury/TBI and employed in our search. The search was conducted in the PsycInfo, Medline, and CINAHL databases, and The Cochrane Controlled Trials Register (CCTR), to identify studies published in English between January 1989 and December 2011. The age range of participants was limited to childhood and adolescence, from birth until 18 years of age. The search yielded 343 publications. Reference lists from each of these publications were also searched. Studies were included when they directly reported social outcomes as primary research findings (n=22), or reported data on social function following TBI in a related study (n=6), using social measurement or questionnaires with a social subscale. Studies reporting on children with localized brain lesions were excluded, and studies of acquired brain injury were included only when there was a TBI subgroup included (n=2). Publications focusing on inflicted TBI were excluded, because these injuries differ from accidental TBI in presenting characteristics and injury types, and are likely to result in the child's removal from their parents, which may impact social skills significantly (Myhre et al., 2007). Publications describing and studying different treatments, interventions, or rehabilitation were also excluded.
The initial plan was to conduct a meta-analysis, but due to the differences in populations, severity groups, measurements, and lack of standardized scores meant that this was not possible, and thus the studies were reviewed descriptively.
Results
Twenty-eight studies met the outlined inclusion criteria. Table 1 summarizes the key methodological characteristics of each of these studies, including design, sample characteristics, TBI definitions, measurement tools, and findings. Specific aspects of each of these characteristics are described below.
ToM, theory of mind; SCI, spinal cord injury; DTI, diffusion tensor imaging; TBI, traumatic brain injury; OI, orthopedic injury (control group); MRI, fMRI, functional magnetic resonance imaging; CO, healthy control group; SD, standard deviation; BT, brain tumor; VABS, Vineland Adaptive Behavior Scale; DAABS, DeBlois Aggressive & Antisocial Behavior Scales; CSEI, Coopersmith Self Esteem Inventory; CLS, Children's Loneliness Scale; CBCL, Child Behavior Checklist; CBCL:TRF, Child Behavior Checklist: Teacher Report Form; PSND, Peer Social Support Network Diagram; FQQ, Friendship Quality Questionnaire; RCC, Ratings of Child's Competence; BRIEF, Behavior Rating Inventory of Executive Function; PKBS-2, Preschool & Kindergarten Behavior Scales-2; HCSBS, Home and Community Social and Behavior Scales; DEX, Dysexecutive Questionnaire; CIQ, Community Integration Questionnaire; SWLS; Satisfaction with Life Scale; ECBI, Eyberg Child Behavior Inventory; SESBI-R, Sutter-Eyberg Student Behavior Inventory-Revised; SSRS, Social Skill Rating System; ERC, Emotion Regulation Checklist; DGT, 10-Minute Delay of Gratification Task; ABAS, Adaptive Behavior Assessment System; VR-SPS, Virtual Reality-Social Problem-Solving Task; INS, Virtual Reality Interpersonal Negotiations Strategy; Flanker, Flanker-No-Go Task; FES, Facial Emotion Sorting; VABS, Vineland Adaptive Behavior Scale; SPSI-R, Social Problem-Solving Skills Inventory-Revised; FAVRES, Functional Assessment of Verbal Reasoning and Executive Strategies; LSDS, Loneliness and Social Dissatisfaction Scale; PIC-2, personality inventory for children 2; SDQ, Strengths and Difficulties; FAB, Florida Affect Battery; SSQ, Social Skills Questionnaire; TASIT, The Awareness of Social Inference Test; CALS, Comprehensive Assessment of Spoken Language; SPSM, Social Problem-Solving Measure; AVM, arteriovenous malformation.
Methodological factors
Design
Of the 28 studies identified, most employed cross-sectional designs (n=20, 77%), with the remaining 8 studies prospective and longitudinal. Eight studies (32%) did not differentiate the TBI samples into severity groups. Only 6 studies (20%) did not include a control group, with 4 of these making comparisons across injury severity groups. For those studies that utilized a control group, 7 studies recruited children with orthopedic injuries as a comparison group, and 13 recruited non-injured children as a comparison group.
Sample characteristics
Details provided regarding sample characteristics varied across studies. Age at injury ranged from 2–22 years, and was not reported in 5 articles (23%). Age at assessment was similarly broad, between 3–22 years. With the exception of prospective studies, time since injury was generally reported imprecisely, with most studies recording only a lower limit for data collection, usually around 6–12 months post-injury. Only two articles considered the effect of age at injury on social outcomes (Donders and Warschausky, 2007; Hanten et al., 2008).
Across studies, TBI was typically defined as evidence of head trauma and altered consciousness. In terms of TBI severity, the majority of studies made comparisons across the severity groups and used similar definitions of injury severity. These definitions typically used a combination of the Glasgow Coma Scale (GCS; Teasdale and Jennett, 1974), duration of loss of consciousness, and post-traumatic amnesia and radiology results, as illustrated in Table 2. In keeping with adult TBI research, mild TBI was described as a score of 13–15 on the GCS, moderate TBI was described as a GCS score of 9–12 or a score of 13–15 with brain lesions, and severe was described as a GCS score 8 or less, and sometimes as a GCS score between 3 and 8. A few studies used a different division of the GCS scores. Turkstra and associates (2004,2001) and Hanten and colleagues (2011) had a general description of severe injury as a GCS score of 8 or less, but described moderate TBI as GCS scores of 9–13 or 14–15 with intracranial lesions. In some cases, however, different TBI severities were combined into a single TBI group and compared to a non-injured comparison group (Hanten et al., 2008; Poggi et al., 2005; Tonks et al., 2007; Turkstra et al., 2004,2001,2008). Other studies reported only a specific severity grouping, such as severe TBI (Warschausky et al., 1997), or mild TBI (Anderson et al., 2001).
GCS, Glasgow Coma Scale; CT, computed tomography; MRI, magnetic resonance imaging; PTA, post-traumatic amnesia; LOC, loss of consciousness; TBI, traumatic brain injury; RV, recreational vehicle.
Not all studies documented cause of injury, but those that did reported that most instances of TBI were due to motor vehicle accidents (passenger and pedestrian), or falls (Anderson et al., 2001; Fletcher et al., 1990; Ganesalingam et al., 2006,2007a,2007b; Hanten et al., 2011; Max et al., 1998; Papero et al., 1993; Stronach and Turkstra, 2008). With the exception of Hanten and associates (2008), and Newsome and colleagues (2010), the studies did not report on lesion/pathology location with regard to social competence in the TBI groups, and when brain imaging data were included the information was relatively non-specific (e.g., frontal or subcortical).
Assessment tools
Assessment tools used in each study are described in Table 3. The majority of publications utilized indirect assessment methods (e.g., parent- and teacher-rated questionnaires) to describe children's social skills. The Vineland Adaptive Behavior Scale (VABS; Sparrow et al., 1984) was the most frequently used measurement (n=11), followed by the Child Behavior Checklist (CBCL; Achenbach and Edelbrock, 1983; Achenbach, 1991; n=8). Further examination of the range of measures reported across the 28 studies demonstrates that a total of 39 measures were administered overall. Of these, 11 were generic measures of behavior, adaptive ability, or executive function, and included one or more subscales tapping social function. All of these were parent or teacher rated. Another 13 measures were specific to social function, and examined a range of social domains (e.g., the Social Skills Rating System; Gresham and Elliot, 1990; and the Children's Loneliness Scale; Asher et al., 1984), with most again completed by parents. Thirteen different measures evaluated a single aspect of social function: 4 measures of self-regulation or executive function (2 child measures, 1 parent report, 1 child/parent report); 3 measures of communication (all child measures); and 6 tasks tapped aspects of social cognition (all child measures). Of these latter 13 measures two were questionnaire-based, with others being skill-based using narrative presentation. The exception was a recent study by Hanten and associates (2011), which employed computer-based technologies and virtual world avatars to present social problem-solving scenarios.
Social outcomes
In keeping with the social literature, most studies focused on “social adjustment,” “social interaction,” and “social cognition,” corresponding to the model illustrated in Figure 2 (Yeates et al., 2007), which identifies these three social components as critical to social competence. After examination of the definitions of “social cognition” and “social information processing” employed in the reviewed papers, we concluded that these two labels were referring to equivalent skills, and were thus collapsed into a single “social information processing” domain. In the following section we discuss study outcomes using these three social domains.
Social adjustment
Social adjustment is described as “the capacity of individuals to adapt to the demands of their social environment” (Beauchamp and Anderson, 2010), or as “the degree to which children get along with their peers; the degree to which they engage in adaptive, competent social and communicative behavior; and the extent to which they inhibit aversive, incompetent behavior” (Crick and Dodge, 1994). In the studies reviewed, a wide range of questionnaires was used to measure social adjustment, with the most popular being the VABS and CBCL.
A number of studies (n=4), conducted at different time points post-injury, reported that parents rated their children and adolescents with TBI as having impairments in socialization and communication skills, and demonstrated more social impairments than control groups (Fletcher et al., 1990; Ganesalingam et al., 2011; Max et al., 1998; Levin et al., 2009; Poggi et al., 2005; Yeates et al., 2010). A similar number found no significant group differences (Anderson et al., 2001; Chapman et al., 2010; Hanten et al., 2008; Papero et al., 1993; Poggi et al., 2005; Ross et al., 2011). It was unclear from the available studies whether increased injury severity resulted in more social adjustment deficits. Some studies suggested that children with severe TBI had more impaired communication and social competence than children with milder injuries (Asarnow et al., 1991; Chapman et al., 2010; Fletcher et al., 1990; Ganesalingam et al., 2011; Max et al., 1998; Yeates et al., 2004,2010). In contrast, Papero and associates (1993) found no differences in these domains across severity groups.
Using a combination of direct child measures and parent ratings, Andrews and associates (1998) found that children with TBI scored significantly lower on adaptive behavior and self-esteem, and higher on loneliness, maladaptive, aggressive, and antisocial behavior. Using a similar design, Ganesalingam and colleagues (2006,2007a,2007b) found that children with moderate and severe TBI were more socially impaired than uninjured children. Specifically, they reported that children with TBI had impaired social skills, poorer emotional and behavioral self-regulation, and that they responded more often with aggressive, avoidant, or irrelevant solutions to social problems than uninjured children. There were no differences between children with severe and moderate TBI. No mild group was included in this study, therefore the impact mild TBI has on these areas is unclear from this research.
Social interaction
Social interaction refers to the social actions and reactions between individuals or groups adapted to the situation (Beauchamp and Anderson, 2010). To study this aspect of social function, Bohnert and associates (1997), and Prigatano and Gupta (2006), investigated friendships of children who had sustained a TBI. Both Bohnert and co-workers (1997), and Ross and associates (2011), found no differences between children with and without TBI in friendship networks, or on the Friendship Quality Questionnaire (FQQ; Parker and Asher, 1993), as reported by children. Prigatano and Gupta, on the other hand, reported results that supported a dose-response relationship using the open questions with regard to friends from the CBCL parent report. They found that children with a TBI had fewer close friendships. In addition, severity of injury had an effect on friendships, with children with severe TBI having fewer close friendships than children with moderate or mild TBI, and children with moderate TBI having fewer close friendships than children with mild TBI.
Social cognition
Social cognition refers to the mental processes used to perceive and process social cues, stimuli, and the environment (Beauchamp and Anderson, 2010). For the purpose of this review, social cognition was divided into social problem-solving and social information processing, which includes theory of mind (ToM) and emotion perception.
Several recent studies have investigated social cognition in children and adolescents post-TBI, using child measures. Hanten and associates (2008,2011) and Janusz and colleagues (2002) used the Interpersonal Negotiation Strategies (INS) task, a child-based tool, to measure social problem-solving (Yeates et al., 1990). This tool consists of hypothetical interpersonal dilemmas, which involve four social problem steps: defining the problem, generating alternative strategies, selecting and implementing a specific strategy, and evaluating outcomes. Hanten and associates (2008) found that children with a TBI scored significantly lower on social problem-solving from baseline through 1-year post-TBI with no differential improvement between the time points for both the TBI and control groups. More recently, Hanten and colleagues (2011) later replicated these findings, using a virtual reality version of the INS task. Similarly, Janusz and associates (2002) found that children with TBI scored significantly lower on social problem-solving than normally-developed children; children with TBI were able to generate solutions to social problems, but had difficulty choosing the optimal solution. These authors also investigated differences between severity groups, but detected no severity effects in performance on social problem-solving between children with severe and moderate TBI. Warschausky and co-workers (1997) used a similar paradigm, the Social Problem-Solving Measure (Pettit et al., 1988), to assess solutions to social problems in children aged 7–13 years. Children with TBI provided significantly fewer peer entry solutions, trying to enter an ongoing peer activity, in social engagement situations than control children, but the groups did not differ with regard to the number of solutions to peer provocations. Muscara and colleagues (2008) investigated the relationship between executive function and social function 10 years post-childhood TBI, extending earlier work proposing that social problem-solving is a mediator between neurocognitive function and social skills (Yeates et al., 2004). Muscara and associates (2008) identified that executive dysfunction was associated with less sophisticated social problem-solving skills and poorer social outcomes. Further, the maturity of social problem-solving skills was found to mediate the relationship between executive function and social outcomes in TBI, providing the first empirical evidence for a link between executive and social skills in the context of childhood acquired brain injury, due to the mediator link of social problem-solving.
Studies investigating social information processing have focused primarily on ToM and emotion perception. Turkstra and colleagues (2004,2008) measured social information processing in adolescents with TBI using a second-order belief task and a pragmatic judgment test. They reported that compared to healthy controls, adolescents with TBI were deficient in judging whether a speaker was talking at the listener's level, and recognizing an individual monopolizing a conversation. In contrast, the TBI group performed similarly to controls on a first-order belief task, identifying a good listener, as well as on a faux pas test and the Strange Stories test. Children and adolescents with TBI have also been shown to have more difficulty recognizing emotions than controls (Tonks et al., 2007; Turkstra et al., 2001). Similarly, Tonks and associates (2007) reported that children with a TBI had significantly greater difficulty recognizing emotions from the eyes than control children, although they performed similarly when recognizing emotions from whole faces, suggesting that adding context assisted social information processing.
Predicting social outcomes after child TBI
Few of the 28 studies identified in our review considered potential predictors of social outcome, with the exception of injury severity. Most studies divided participant groups into children with and without TBI, or into specific severity groups. To date two studies (Donders and Warschausky, 2007; Hanten et al., 2011) have examined the long-term impact of age at injury on social outcomes. Donders and Warschausky (1997) reported on a group of adolescents and young adults who had sustained TBI in either childhood or adolescence. They found that children sustaining a TBI before the age of 12 demonstrated poorer social development than children injured after age 12 years. Further, participants with early-onset TBI were less satisfied with their social integration and less likely to be their own legal guardian or to possess a valid driver's license than participants with late-onset TBI. Hanten and colleagues (2008,2011) have added to this literature by exploring the effects of injury location on social skills. In their 2008 article, they examined neural correlates of social problem-solving in children with lesions in the frontal, temporal, parietal, and occipital regions, and in the corpus callosum and basal ganglia. Consistent with findings from the adult literature, and in keeping with our current understanding of the social brain network, they found poorer performance in social problem-solving only in children younger than 12 years old with a frontal lesion, and in all children with a lesion in the corpus callosum. More recently Hanten and colleagues (2011) investigated the relation between social problem-solving and cortical thickness using a virtual reality social problem-solving task and functional magnetic resonance imaging (fMRI). The results showed that the adolescents with TBI had more difficulties defining the problem (DP) and evaluating the outcome (EO). Further, Newsome and associates (2010) investigated the brain activation while thinking about self from another person's perspective using the Trait Attribution Task (modified from D'Argembeau et al., 2007). They found that adolescents with TBI have greater activation in posterior brain regions, including the left lingual gyrus, posterior cingulate, cuneus, and parahippocampal gyrus, while performing more poorly on the social problem-solving tasks.
In terms of investigating the influence of environmental factors on social development, Chapman and associates (2010) reported links between social incompetence and low socio-economic status, family dysfunction, and permissive parenting, while Yeates and colleagues (2004,2010) also found a link between family resources and social outcomes.
Discussion
This systematic review identified 28 studies that examined social function in children and adolescents after TBI. These studies were located via a detailed and systematic literature search, and included articles that described an aspect of social function. The results provide valuable information on social outcomes after TBI in childhood and adolescents. To the authors' knowledge, this is the first time that empirical evidence for social outcomes of TBI in childhood and adolescence has been comprehensively reviewed. This review is timely, given the rapid recent development of the social neurosciences, the need to extend this knowledge to both developmental and clinical contexts, and the increasing recognition of the importance of intact social function for quality of life. While initially a meta-analysis was planned, the significant differences in the focus and design of the available studies and the assessment tools used meant this was not possible, and despite broad criteria only 28 were appropriate for inclusion for review. Interestingly, of these, half were published in the last 5 years, highlighting growing interest in the social domain. This suggests that social outcome after TBI is an area that has been given relatively little attention to date, and needs further research.
TBI and social outcomes
The results of this systematic literature review confirm that children and adolescent survivors of TBI have an elevated risk of social dysfunction, with consistent difficulties identified for social adjustment and social cognition. Studies of social adjustment reported poor self-esteem, loneliness, maladjustment, and social isolation, in the context of reduced emotional control and aggressive antisocial behavior (Andrews et al., 1998; Fletcher et al., 1990; Ganesalingam et al., 2011; Levin et al., 2009; Max et al., 1998; Yeates et al., 2010). These social difficulties are known to be associated with persisting psychological problems, reduced social participation, and reduced quality of life (Anderson et al., 2010; Cattelani et al., 1998; Van Tol et al., 2011). Studies of social cognition described impaired emotional recognition and social problem-solving as their most consistent findings (Hanten et al., 2008; Janusz et al., 2002; Tonks et al., 2001; 2007; Warshausky et al., 1997)
Predictors
Surprisingly few studies considered the impact of injury factors. For studies examining injury severity effects, the weight of the evidence suggests that mild TBI has few social consequences, and that such insults are below the threshold for social consequences. Children with moderate and severe TBI, in contrast, demonstrated an elevated risk of social problems, particularly in the domains of social interaction (few close friendships), and social cognition (communication, social problem-solving, and emotion recognition). Of interest, the available data are unable to assist in determining whether a dose-response relationship exists within moderate-to-severe injury groups (Asarnow et al., 1991; Chapman et al., 2010; Fletcher et al., 1990; Ganesalingam et al., 2011; Max et al., 1998; Yeates et al., 2004,2010). Even less is known about the influence of site of injury. Only a couple of studies systematically addressed the relationship between lesion location and social impairments (Hanten et al., 2008,2011; Newsome et al., 2010), identifying links between frontal regions and the corpus callosum and poor social function, consistent with adult research (Adolphs, 2001). Recent advances in the social neurosciences provide exciting new opportunities to extend these findings in the future.
The impact of age at injury is also largely unexplored. Studies by Donders and Warschausky (2007) and Hanten and associate (2008) provide preliminary evidence for an age-at-injury effect for social impairment, in particular social cognition, after child TBI; however, the age groups studied were older than those previously identified as uniquely vulnerable to TBI due to rapid brain development. Thus further research is needed to determine whether social consequences follow a similar pattern to cognitive consequences with respect to age at injury.
Social context and family environment are well-established influences for social development (Ackerman and Brown, 2006; Bowlby, 1962; Bulotsky-Shearer et al., 2008; Guralnick, 1999; Masten et al., 1999). Thus it is surprising that this domain has not attracted more interest in the context of child TBI. Of the studies reviewed, only two considered the contribution of environment (Chapman et al., 2010; Yeates et al., 2004), with both identifying low socioeconomic status, family dysfunction, permissive parenting, and family resources as predictors for social competence.
Limitations of this study and future directions
While we believe that this systematic review has successfully identified the key methodologically-sound research in the field, it may be that the search terms employed did not exhaustively cover all relevant publications. In considering this possibility, it is important to note that 341 potential articles were initially identified, but less than 10% met the review criteria, suggesting that, consistent with the emerging nature of this research domain, much of the research conducted in the field is characterized by weak methodologies. Even in the 28 studies meeting inclusion criteria, a range of methodological flaws and inconsistencies limited the interpretations and conclusions that could be drawn. Despite common strengths with respect to adequate sample size, inclusion of appropriate comparison groups, and adherence to accepted diagnostic approaches, many studies had significant design flaws. The most common of these were: (1) unacceptably broad ranges for injury age and age at assessment, which precluded the examination of important developmental processes; (2) inconsistencies in definitions of injury severity; (3) limited details regarding time since injury, resulting in difficulties in determining recovery trajectories for social skills; (4) the use of tests that are insensitive or unreliable measures of social function or that possess inadequate normative data; (5) an over-reliance on parent reports; and (6) lack of neuroimaging data. On an optimistic note, there is a trend toward more recent studies to address these inadequacies, with evidence of more attention to developmental issues like age of injury and time since injury, better use of more sensitive measures of social function, and the growing use of multiple informants of social function.
It is vital that future research utilizes the advances of the social neurosciences, and begins to explore brain correlates of social function that are specifically relevant to the developing brain. Further, research designs that simultaneously examine the role of brain and environment for social outcome are warranted. Finally, within the context of child neuropsychology, it is critical to broaden our theoretical framework to incorporate knowledge from other relevant fields, including developmental and social psychology and the social neurosciences, in our conceptualization of social function following child TBI.
Conclusions
Developmental social neurosciences is a rapidly-emerging field that has highlighted the possibility of gaining a better understanding of the etiology and nature of social impairment that occurs in the context of injury to the developing brain. In this evolving research environment, this review provides valuable information describing current empirical findings with respect to social outcomes in children and adolescents following TBI. Despite methodological inadequacies and somewhat inconsistent approaches, the findings of this review provide initial evidence that children with TBI are at risk of experiencing impaired social function. Further, the limited studies available identify deficits across the range of key social domains, and provide early support for relationships between social function and other factors, including injury severity, age at injury, location of brain pathology, and social and family factors. The small pool of literature dedicated to this topic, and the varied results from published studies, indicate that the social outcome after TBI in children and adolescents is an area that needs further investigation, preferably employing research designs with sound methodologies that facilitate the evaluation of the contributions of both biological and environmental factors to social outcomes following child TBI.
Footnotes
Acknowledgments
This work was funded through research grants awarded by the Victorian Neurotrauma Institute and the Foundation for Children Fund.
Author Disclosure Statement
No competing financial interests exist.