
Abstract
Penetrating brain injury (PBI) encountered in both the military and civilian sectors results in high morbidity and mortality due to the absence of effective treatment options for survivors of the initial trauma. Developing therapies for such injuries requires a better understanding of the complex pathology involved when projectiles enter the skull and disrupt the brain parenchyma. This study presents a histological characterization of bilateral PBI using a relatively new injury model in the rat, and also investigates the implantation of a collagen scaffold into the PBI lesion as a potential treatment option. At 1 week post-PBI, the lesion was characterized by dense macrophage infiltration, evolving astrogliosis, hypervascularity, and an absence of viable neurons, oligodendrocytes, and myelinated axons. Histomorphometric analysis revealed that the PBI lesion volume expanded by 29% between 1 week and 5 weeks post-injury, resulting in formation of a large acellular cavity. Immunohistochemistry showed a decrease in the presence of CD68-positive macrophages from 1 to 5 weeks post-PBI as the necrotic tissue in the lesion was cleared, while persistent glial scarring remained in the form of upregulated GFAP expression surrounding the PBI cavity. Implanted type I collagen scaffolds remained intact with open pores after time periods of 1 week and 4 weeks in vivo, and were found to be sparsely infiltrated with macrophages, astrocytes, and endothelial cells. Collagen scaffolds appear to be an appropriate delivery vehicle for cellular and pharmacological therapeutic agents in future studies of PBI.
Introduction
P
Previous researchers of PBI have fired projectiles into the brains of animals, including cats (Carey et al., 1989; Soblosky et al., 1992), rabbits (Novozhilova et al., 1997), and monkeys (Allen et al., 1982,1983). Studies of this kind have generally been discontinued, prompting the development of different animal injury models. Relatively recently, researchers at the Walter Reed Army Institute of Research (WRAIR) developed a rat model that reproduces several aspects of a ballistic PBI (Williams et al., 2005). The key feature of clinical PBI simulated by the model is the temporary cavity resulting from dissipation of kinetic energy as a projectile passes through the brain. Various studies have demonstrated (Sapsford, 2003) that the temporary cavity in PBI is likely to be several times larger than the volume of tissue damaged solely from the path of the projectile (Izci et al., 2003; Zhang et al., 2005b,2007b). The injury model involves insertion of a metal probe into the brain to mimic the projectile path, followed by inflation of a balloon attached near the probe tip to simulate the temporary cavity. Studies with the model have investigated various aspects of the injury, including histopathology (Williams et al., 2005,2006a), neuroinflammation (Lu et al., 2009; Wei et al., 2009; Williams et al., 2007), intracranial pressure changes (Wei et al., 2010), electrophysiology (Lu et al., 2011), cognitive impairment, and motor deficits (Shear et al., 2010). The model has been shown to produce results consistent with what is known about PBI from larger animal models and from human pathology (Lu et al., 2011; Williams et al., 2005,2006a,2007). It is, however, noted that certain PBI features such as retained bone and metal fragments, along with subsequent infectious processes, are not reproduced (Jankovic et al., 2000). The model nonetheless provides a useful method for studying several aspects of PBI pathophysiology through the creation of a standardized cavitary defect.
Published work using the PBI model has focused mostly on characterization and treatment of a frontal, unilateral injury. While this is likely to be the type of clinical PBI with the best outcome, bilateral injuries in which the projectile track crosses the midsagittal plane are common and also potentially survivable. Bilateral injuries have been reported to have an incidence between 33% and 66% among patients in several clinical PBI studies (Pruitt, 2001). Although a bilateral injury model in the rat was introduced in one study from WRAIR (Williams et al., 2006b), the results reported were restricted mainly to survival rates and levels of motor dysfunction. One of the aims of this work is to expand upon the initial WRAIR bilateral PBI study by adding a characterization of the histopathology at time points of 1 week and 5 weeks post-injury. These time points allow for a study of the temporal progression of the lesion, and a comparison with some aspects of the frontal injury research (Shear et al., 2010; Williams et al., 2006a).
While clinical PBI producing large bilateral lesions with ventricular involvement is extremely likely to be fatal (Martins et al., 2003; Pruitt, 2001), less severe bilateral injuries may have much higher levels of survival (Murano et al., 2005; Pruitt, 2001; Rosenfeld, 2002). For example, in a study of 190 patients with gunshot wounds to the head, the mortality rate for bifrontal injuries was 12% (Kaufman et al., 1995; Pruitt, 2001). The bilateral injury model introduced by researchers at WRAIR was described as resembling a clinically survivable PBI based on the primarily frontal anatomical location of the injury (Williams et al., 2006b). Further, the severity of the bilateral injury was limited by inducing an asymmetric lesion with most of the damage inflicted within one hemisphere. Based on the reasonable similarity to a clinically relevant bilateral PBI, along with the high survival rates reported, we elected to create a very similar bilateral injury for this study.
It is observed that the permanent cavity that eventually forms in the brain as a result of PBI lends itself to the possibility of treatment through implantation of a biomaterial. The biomaterial might act as a suitable delivery vehicle for pharmacological and cellular therapeutic agents to mitigate injury progression or promote regeneration. As a preliminary step towards developing such a treatment, this work evaluates the effects of implanting a preformed collagen scaffold either immediately after injury or 1 week later. Immediate implantation may be of benefit for delivery of therapeutic agents to treat the injury in the acute phase, while the 1-week time point may target delayed physiological effects of the injury. Additionally, the expanded lesion cavity at 1 week post-injury (Williams et al., 2006a) may offer more space to accommodate a biomaterial. The motivation for employing a collagen scaffold in this work was based in part on its favorable performance as an implant to bridge gaps in peripheral nerve (Chamberlain et al., 2000) and spinal cord (Spilker et al., 1997). In addition, the fabrication process for the collagen scaffolds used in this study offers control over potentially significant parameters such as pore size (O'Brien et al., 2004), pore alignment (Madaghiele et al., 2008), density (Harley et al., 2007), degree of cross-linking (Vickers et al., 2006), degradation rate (Harley et al., 2004; Pek et al., 2004), mechanical behavior (Harley et al., 2007; Wang and Spector, 2009), and material composition (Tang et al., 2007; Wang and Spector, 2009). Collagen scaffolds can also be modified to incorporate proteins (Pataquiva-Mateus et al., 2012), genes (Bolliet et al., 2008), cells (Cholas et al., 2012; Sun et al., 2009), and other therapeutic agents. In this preliminary work, a primary goal was to evaluate the safety of implanting a collagen biomaterial in a PBI lesion and allowing it to remain in vivo for a period of weeks. Further, we aimed to investigate whether the scaffold retained structural integrity and could support or promote the infiltration of viable endogenous cells.
Methods
Experimental design
Four groups of animals were used in this study (Table 1), with all undergoing surgical administration of a bilateral PBI. The injury involved rapid inflation of the PBI balloon to a volume equal to approximately 10% of the rat brain volume (Williams et al., 2006b). Group 1 was administered the injury and sacrificed 1 week later. Group 2 underwent the same injury, but was sacrificed 5 weeks later. It is noted that at 1 week post-injury, the group 2 animals underwent sham surgery to serve as controls for group 4. Group 3 was administered the injury, but was then immediately implanted with a collagen scaffold. Group 3 animals were sacrificed 1 week post-injury. Group 4 underwent the injury and 1 week later had a second surgery to implant a collagen scaffold. Group 4 animals were sacrificed 4 weeks after implantation of the scaffold (5 weeks post-injury).
PBI, penetrating brain injury; N/A, not applicable.
Penetrating brain injury apparatus
Technical details of the PBI apparatus (Dragonfly Inc., Ridgeley, WV) have been described in several publications (Williams et al., 2005,2007). Briefly, the apparatus consists of components including a balloon-tipped probe, a stereotaxic frame (David Kopf, Tujunga, CA), a piston-cylinder pneumatic device, and a pendulum. The pendulum is dropped under gravity to drive the piston, forcing the air in the cylinder through tubing of smaller diameter, and generating a pressure impulse to rapidly inflate the balloon. The balloon, which takes the shape of an ellipsoid, has been reported to remain inflated on average for less than 6.6 msec (Williams et al., 2005).
Collagen scaffold fabrication
Collagen scaffolds (1.0% weight:volume) were fabricated from medical grade porcine microfibrillar type I/III collagen (Geistlich Biomaterials, Wolhusen, Switzerland). A collagen suspension was first made in 0.001 N HCl, brought to pH 3, and mixed for 20 min. The slurry was blended at 15,000 rpm with an Ultra Turrax T18 blender (IKA, Staufen, Germany) for 30 min at 4°C, brought again to pH 3, and blended for an additional 2 h. The slurry was then centrifuged for 10 min at 5500 rpm to remove air bubbles, and mixed with a pipette for homogeneity. The slurry was poured in a metal mold and placed into an AdVantage Benchtop Freeze Dryer (VirTis, Gardiner, NY). The temperature was steadily decreased to −40°C over 180 min and held at that temperature for 60 min. Sublimation was conducted at a temperature of 0°C and pressure of 200 mTorr for 1020 min. Scaffold sheets were removed from the freeze dryer and dehydrothermally cross-linked overnight at 105°C under vacuum. Individual scaffolds were cut to 3 mm diameter and approximately 3 mm thick for implantation. Other studies using similar scaffolds have determined the pore size to be approximately 100–150 μm (Bolliet et al., 2008; Harley et al., 2007; Wang and Spector, 2009).
Surgical procedure and animal care
In all, 24 male Sprague-Dawley rats were used in this study. All procedures were approved by the VA Boston Healthcare System Institutional Animal Care and Use Committee.
The animals were shaved, anesthetized with isoflurane, and positioned in a stereotaxic frame where anesthetic delivery was maintained through a nose cone. A circulating water heating pad was used to maintain body temperature throughout the surgery, and also for several hours during the post-operative recovery period. Heart rate and blood oxygen saturation were monitored during the procedure.
After sterilizing the skin with 13% povidone iodine solution, a midline incision was made along the top of the head to expose the skull, followed by a lateral incision extending from the posterior aspect of the midline incision and passing just anterior to the left ear. With the top of the skull and the left side of the head exposed, a portion of the left temporalis muscle was excised with care taken to avoid damaging the temporal branch of the facial nerve. With the lateral aspect of the skull exposed, a 3-mm-diameter window was drilled in the skull at a position 1 mm anterior and 3 mm ventral to the bregma. The PBI probe was then positioned with the tip at the surface of the brain before pausing to briefly ensure stability of the animal's vital signs.
The PBI probe was then inserted into the brain, with the tip advancing 10 mm from the surface of the left hemisphere into the right hemisphere. The PBI balloon was inflated to a diameter of 6.3 mm to create an injury encompassing approximately 10% of the rat brain volume. The balloon was located several millimeters proximal to the probe tip, such that the balloon inflation was mostly in the left hemisphere, despite a substantial portion of the probe resting in the right hemisphere. This scenario mimics a projectile entering through the left side of the skull and dissipating its kinetic energy before coming to rest in the right hemisphere. The resulting injury was therefore predominantly in the left hemisphere, although the probe and the expanded balloon also caused a lesser amount of damage to the right hemisphere. The surgical procedure was nearly the same as that introduced previously (Williams et al., 2006b), with only a minor variation in the anatomical location. Specifically, the probe was inserted at a slightly more dorsal location to avoid damaging the exposed facial nerve. Additionally, the probe was advanced to a slightly lesser final depth to avoid the possibility of the tip passing entirely through the contralateral hemisphere. Following the balloon inflation, the probe was retracted from the brain and the biomaterials for the implantation groups were prepared. Animals in group 3 underwent implantation of a cylindrical collagen scaffold 3 mm in diameter and 3 mm thick into the defect at this time. Groups 1, 2, and 4 had no intervention. The cranial window was covered with a thin collagen membrane (Bio-Gide; Geistlich Biomaterials), and the surgical incision was closed with 4-0 sutures.
At 1 week after the injury, animals in groups 2 and 4 underwent a second surgery. A second incision was made parallel to the lateral incision from the first surgery, enabling access to the defect site. After removing the membrane covering the cranial window, the lesion site was exposed. Group 4 animals had a collagen scaffold implanted at this time, while group 2 animals had the same surgery to expose and briefly penetrate the lesion site, but without scaffold implantation (sham surgery). The cranial window in each case was covered again with a collagen membrane and the incision closed with 5-0 sutures.
Following all surgeries, the animals were allowed to recover in warmed cages with additional oxygen administered through a nosecone. Food and water were provided at bedding level. Buprenorphine (0.05 mg/kg) was given for pain relief, while cefazolin (20 mg/kg) was given to prevent infection.
Animal sacrifice and specimen processing
Before sacrifice, the animals were deeply anesthetized with an intraperitoneal injection of sodium pentobarbital (150 mg/kg). The animals were then transcardially perfused with 150 mL cold heparinized PBS (20 units/mL), followed by 250 mL cold 4% paraformaldehyde solution. The brains were extracted and immersed in 4% paraformaldehyde for 2–3 days at 4°C. The brains were processed through reagent alcohol dilutions (70% for 10 min, 80% for 90 min, 95% for 2×90 min, 100% for 2×90 min, and 100% for 90 min under vacuum), xylenes (3×90 min), and paraffin (2×180 min under vacuum at 58°C). Samples were then embedded in paraffin and sectioned on a microtome at 5 μm. The slides were dried on a warmer at 60°C for several hours.
Histology and immunohistochemistry
Routine hematoxylin and eosin (H&E) staining was conducted for histomorphometric analysis and general histologic observation of the injury.
Antibodies, dilution factors, and antigen retrieval methods used for immunohistochemistry are summarized in Table 2. For heat-induced epitope retrieval, a BioCare Decloaking Chamber was used (BioCare Medical, Concord, CA). The staining procedure was conducted at room temperature using an autostainer (Dako, Carpinteria, CA). Following deparrafinization, rehydration, and antigen retrieval, the slides were rinsed with wash buffer (Dako no. S3006) containing TBS and 0.05% Tween 20. The slides were blocked for 2 h with Dako protein block (Dako no. X0909) prior to addition of the primary antibody for 2 h. Following 3 rinses with wash buffer, the secondary antibody was added for 1 h. After 3 more rinses, a 100-ng/mL solution of the fluorescent DNA stain 4′,6-diamidino-2-phenylindole (DAPI) was added for 30 min. Three final rinses with wash buffer were performed, and the slides were then placed in TBS for 3 min. The slides were transferred to a 0.1% solution (in 70% reagent alcohol) of Sudan black (no. 199664; Sigma-Aldrich, St. Louis, MO) dye for 20 min to reduce tissue autofluorescence. Following three rinses in TBS, the slides were cover-slipped with Immu-mount aqueous mounting medium (no. 9990402; Thermo Scientific, Waltham, MA).
Secondary antibodies (Jackson ImmunoResearch, West Grove, PA) directed against rabbit, mouse, and goat primary antibodies were Dylight 488 donkey anti-rabbit IgG (711-485-152), Dylight 549 donkey anti-mouse IgG (715-505-150), and Dylight 488 donkey anti-goat IgG (705-485-003).
The fluorescent dye Fluoro-Jade C (no. AG325; Millipore, Billerica, MA) was used for visualization of degenerating neurons in the thalamus. Sections from approximately 2.5 mm posterior to the bregma were deparaffinized and rehydrated prior to incubation in 0.06% KMnO4 for 20 min. After 3 rinses in deionized water, the slides were then stained with 0.00015% Fluoro-Jade C solution for 20 min and rinsed 3 more times in water. The slides were dried on a warmer at 60°C for 10 min, placed in xylene for several minutes, and cover-slipped with mounting medium.
All coronal brain slices were processed and imaged as if viewing the brain from the front. As a result, the left side of the brain appears on the right side in all images.
Microscopy
Light microscope images were taken with an Olympus camera interfaced with an Olympus BX51 microscope, while fluorescence images were captured on an Olympus DP71 camera interfaced with an Olympus BX60 microscope. Adobe Photoshop CS3 was used for minor image processing procedures such as cropping and adjustment of levels to reduce background (Cromey, 2010).
Histomorphometric analysis and cell counting
The lesion area was demarcated in hematoxylin and eosin-stained sections taken at approximately 1-mm intervals spanning the lesion. The lesion was defined by areas of obvious necrosis with lack of cellularity, along with regions of dense macrophage infiltration, hemorrhage, gliosis, and vacuolization. A linear interpolation was used to reconstruct an approximate volume, with the volume between sections being equal to the average of the areas multiplied by the distance between them.
The density of Fluoro-Jade C-positive neurons in the thalamus was calculated by counting the total number of positive cells in the left thalamus and dividing by the total area of the thalamus in the section. Similarly, cell densities for the various immunohistochemistry markers in the collagen scaffolds were calculated by counting the number of positive cells within a scaffold section and dividing by the scaffold area.
Statistical analysis
Numerical values are reported as mean±standard error. Statistical analysis was performed using Statview (version 5.0.01; SAS Institute Inc., Cary, NC) software. Unpaired t-tests were used to compare differences between experimental groups, with a p value of 0.05 used for determining statistical significance.
Results
Animal survival, recovery, and qualitative behavioral observations
Twenty-one out of 24 animals survived for the intended duration of their experimental groups. Two of the 3 deaths occurred during the surgery to administer the injury, while the third occurred the day after the injury. All animals undergoing a second surgery (groups 2 and 4) survived with no apparent adverse effects of the additional surgery or the implanted biomaterial.
Animals undergoing a single surgery (group 1 and group 3) typically lost weight in the first 2–3 days after the injury, but thereafter recovered and continued to maintain or gain weight for the rest of the week. In each group, the average weight started to increase by the third day after surgery. Animals that had a second surgery (group 2 and group 4) showed similar weight loss to groups 1 and 3 following injury, but generally lost little or no weight after the second procedure.
Following the injury, the animals consistently showed a decreased ability to use their right forelimb for grasping food while eating. Additionally, a slight tremor of the head was observed in some animals. Both the forelimb deficit and the tremor appeared to mostly resolve within 3–4 days, based on observation of the animals eating, grooming, and ambulating normally. It is likely, however, that sensitive functional and behavioral tests would detect persistent deficits, even at later time points.
Lesion characteristics and volume
Histologically, the bilateral PBI was observed after 1 week to cause a large amount of damage to the left striatum, as well as lesser injury to elements of the sensory and motor cortex, corpus callosum, external capsule, and the lateral ventricles (Fig. 1). Limited areas of injury were also seen in the right cortex and striatum (Figs. 1c and 3a). The lesion site at 1 week consisted of a large amount of necrotic debris (Fig. 3a and b), with dense infiltration of macrophages, areas of hemorrhage, and some areas of vacuolization within the striatum. The size of the cavity was smaller than the entire lesion, as much of the dead tissue had not yet been cleared.
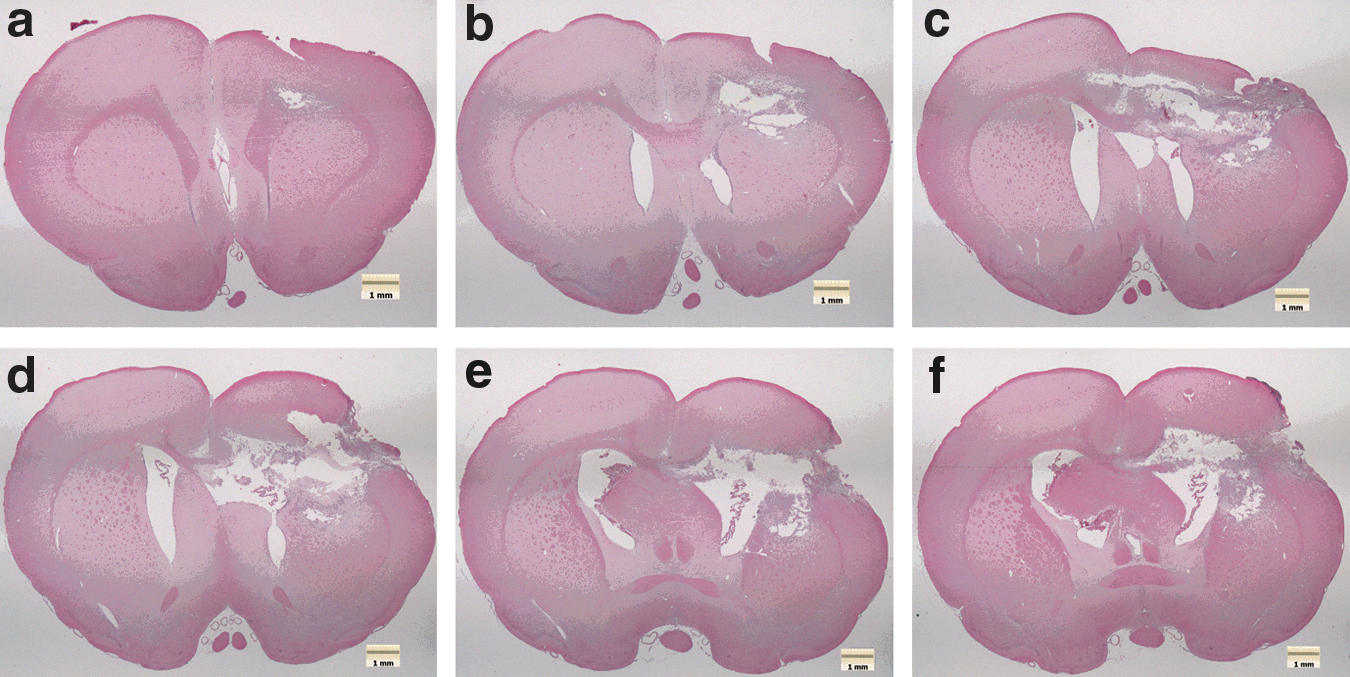
PBI lesion 1 week post-injury (group 1), showing damage to structures including the cortex, striatum, lateral ventricle, external capsule, and corpus callosum. Panels
At 5 weeks, however, the cavity had become much larger, as most of the necrotic debris had been removed (Fig. 2). Injured structures were largely the same as seen at 1 week post-PBI, though the injury appeared to have expanded to include much of the left striatum. Although a few areas of necrosis persisted within the cavity, notably at the edge of the corpus callosum (Fig. 3d), the remaining surrounding tissue appeared viable.
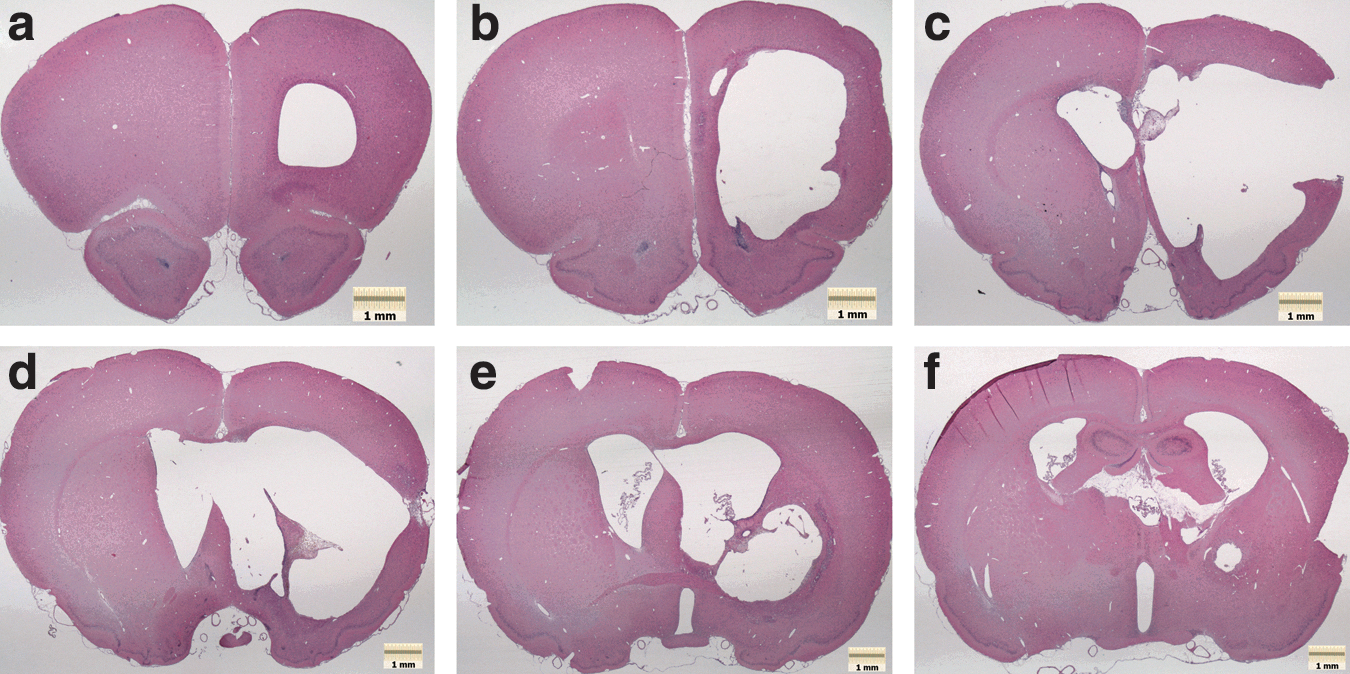
PBI lesion 5 weeks post-injury (group 2), showing that a very large cavity has formed with nearly all necrotic debris cleared from the lesion site. Panels
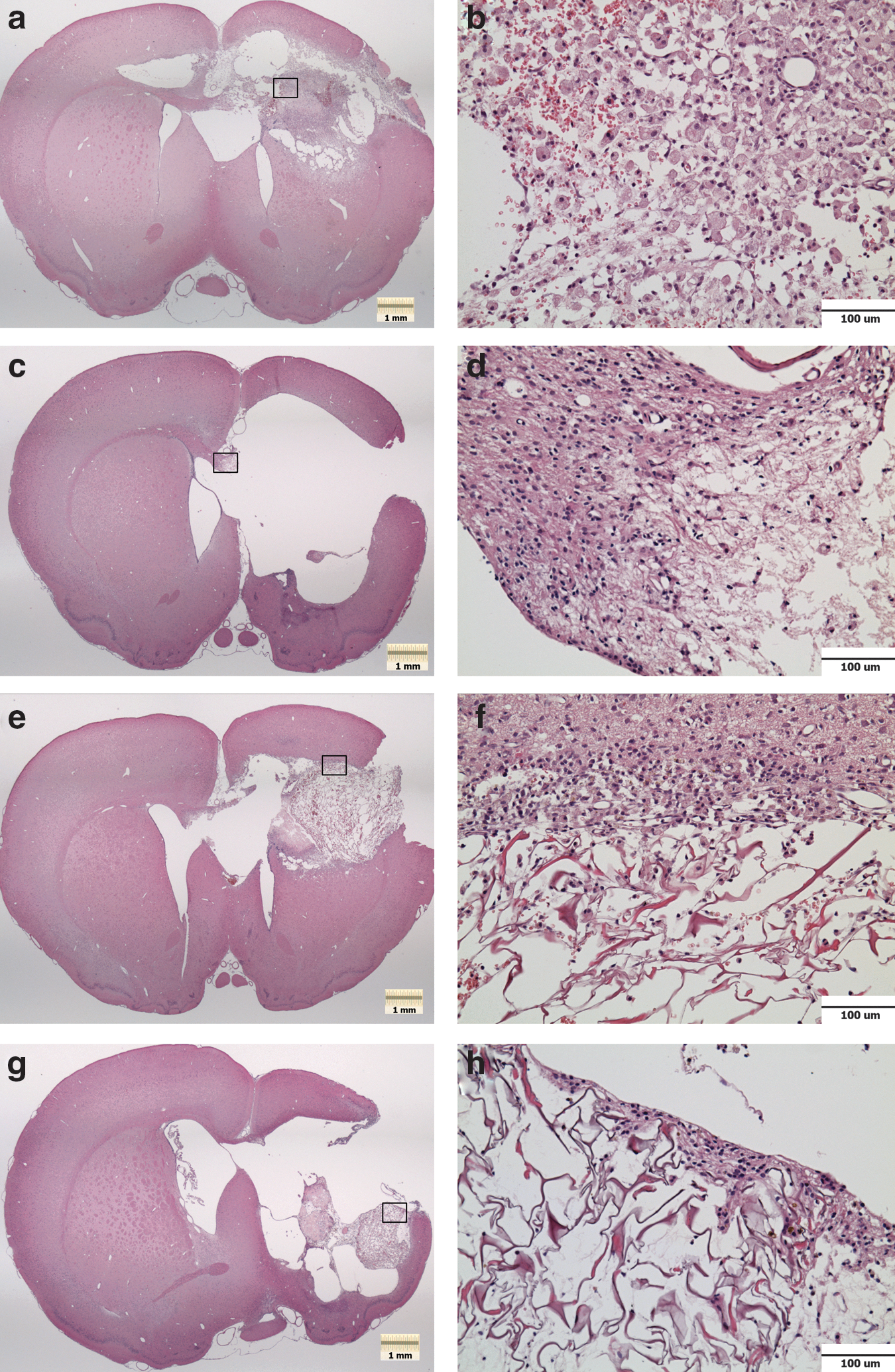
Hematoxylin and eosin (H&E) histology. (
The volume of the bilateral PBI lesion was calculated to be 51.2±3.7 mm3 at 1 week post-injury (group 1), while the volume expanded significantly to 65.9±2.7 mm3 (p=0.010) by 5 weeks (group 2). Group 3 animals undergoing immediate scaffold implantation with sacrifice at 1 week had an average lesion volume of 51.9±4.4 mm3. This volume was not significantly different than the untreated injury in group 1. Group 4 animals undergoing delayed implantation with 5-week sacrifice had an average lesion volume of 85.1±12.9 mm3, which was not significantly different than the untreated injury in group 2.
Scaffold localization and cellular infiltration
Scaffolds in group 3 remained intact within the lesion 1 week after implantation (Fig. 3e). The volume of the scaffold filled a substantial portion of the injury site, but was clearly smaller than the entire lesion. The scaffolds were generally localized to the injured regions in the left striatum and cortex, and were in contact with some tissue that appeared to be potentially viable. The scaffolds were observed to have open pores without apparent degradation of the scaffold struts. Cells from the surrounding tissue appeared to have infiltrated the scaffolds in relatively small numbers (Fig. 3f). Many of the cells had morphology similar to that of the inflammatory cells in the surrounding tissue. Erythrocytes were also observed within the scaffolds.
Group 4 scaffolds were observed to be much smaller than the size of the lesion at 5 weeks post-injury, and did not come close to filling the volume of the cavity (Fig. 3g). The scaffolds were also poorly integrated into the surrounding tissue, with only a fraction of their surface areas contacting viable tissue. The scaffolds were found localized to the lateral aspect of the lesion, and in 2 cases were partially adhered to the inside of the skull. One of the adhered scaffolds was not recognized as such, and was lost during extraction, most likely due to inadvertently removing it with a portion of the skull. In the remaining 4 samples, the scaffold pores were open and there was some cellular infiltration (Fig. 3h), which appeared qualitatively similar to group 3. The integrity of the scaffolds appeared to be maintained with no obvious signs of degradation present.
Glial scarring and inflammation: GFAP (astrocytes) and CD68 (macrophages)
Glial fibrillary acidic protein (GFAP) staining showed reactive astrocytes surrounding the lesion to varying degrees at the two time points. At 1 week post-injury (group 1), staining was irregularly distributed around the lesion site (Fig. 4a). While astrocytes were absent within some areas of necrosis, they could be seen organizing around the periphery of the lesion cavity (Fig. 4b). A glial scar appeared to be forming in conjunction with the remodeling of the lesion site. By 5 weeks post-injury (group 2), both the lesion site and the surrounding pattern of GFAP staining were much more organized (Fig. 4c). A well-defined band of gliosis with thickness up to approximately 100 μm was present bordering the lesion cavity (Fig. 4d). Additionally, an upregulation of GFAP was evident throughout a significant portion of the left hemisphere. Approaching the lesion site, a transition could be observed where astrocytes lost their typical star-like morphology and became indistinguishable from one another among the glial scar.
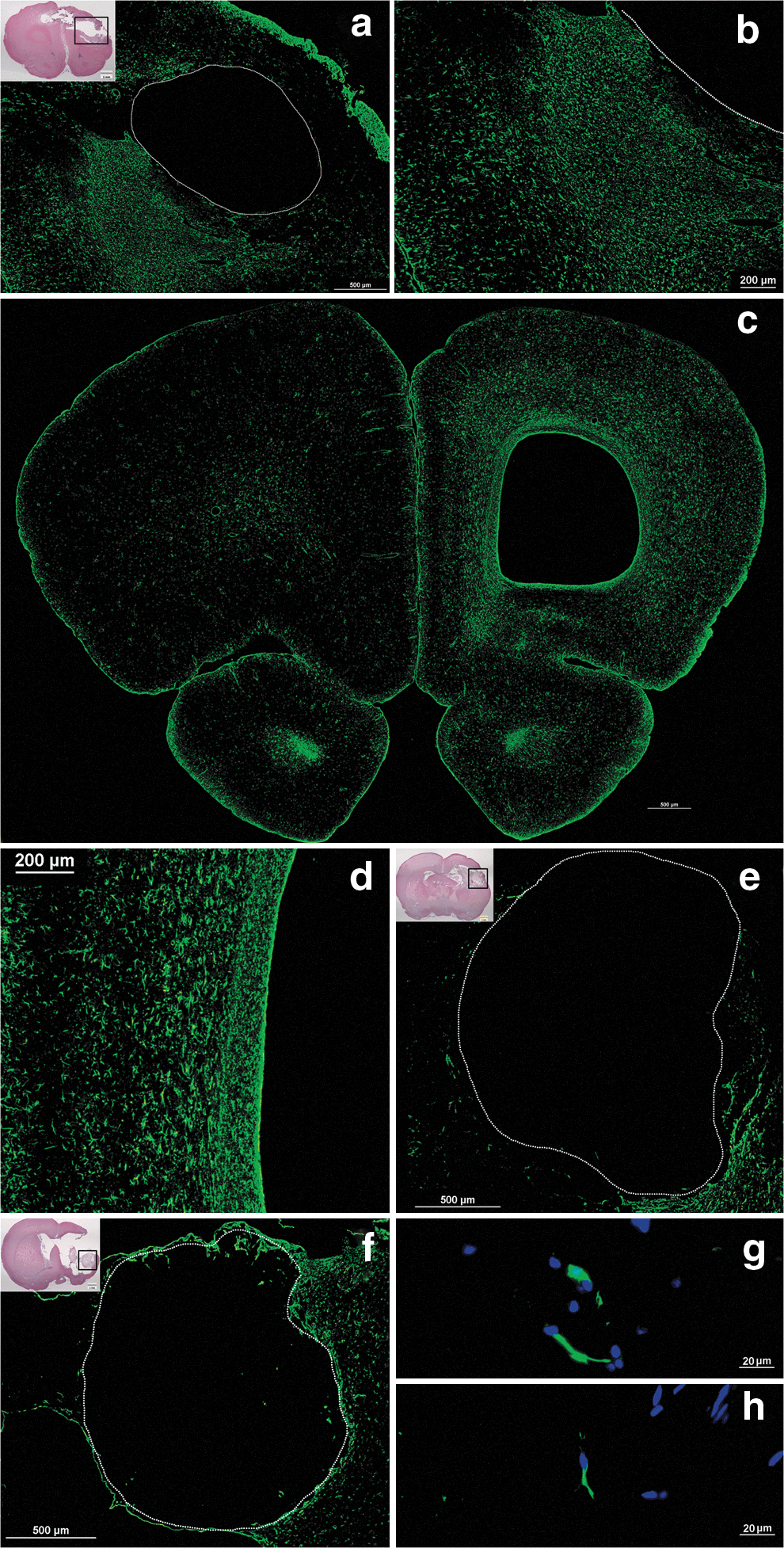
Glial fibrillary acidic protein (GFAP) staining for astrocytes. (
The collagen scaffolds in groups 3 and 4 did not appear to alter the general pattern of gliosis seen in the injury. At 1 week post-injury, the scaffolds of group 3 had irregular GFAP staining surrounding them with an absence of astrocytes in areas of necrosis (Fig. 4e). There were a relatively small number of astrocytes detected within the collagen scaffolds (Fig. 4g) at high magnification. The density of astrocytes in group 3 scaffolds was calculated to be 12.1±2.0 cells per mm2. Group 4 scaffolds were more uniformly surrounded by gliosis and were infiltrated by astrocytes to a slightly greater degree. Astrocyte density in the scaffolds was 19.0±2.1 cells per mm2, which was a marginally significant increase relative to group 3 (p=0.053).
CD68 staining confirmed the phenotype of many of the inflammatory cells in the lesion site as macrophages. Widespread CD68 reactivity could be observed throughout several regions, including the cortex, striatum, external capsule, and corpus callosum (ipsilateral and contralateral). The macrophage infiltrate was very dense at 1 week (Fig. 5a and b), while far fewer macrophages were observed at 5 weeks (Fig. 5c). However, at 5 weeks a degree of CD68 reactivity did persist within the small amount of necrotic debris in the lesion cavity. Additionally, macrophages were observed along the border of the lesion cavity (Fig. 5d), and in white matter tracts.

CD68 staining for macrophages. (
CD68 staining in the scaffolds of group 3 and group 4 revealed that many of the infiltrated cells were macrophages (Fig. 5e and f). The density of CD68-positive macrophages in group 3 scaffolds was 50.5±7.2 cells per mm2, while the density in group 4 scaffolds was 39.0±6.0 cells per mm2. The difference was not statistically significant.
Blood vessels and endothelial cells: Von Willebrand factor
Von Willebrand factor (VWF) staining displayed many blood vessels within and surrounding the lesion site. At 1 week post-injury, numerous vessels were present throughout the areas of necrosis and macrophage infiltration (Fig. 6a). At 5 weeks, after most of the debris had been cleared, vessels bordered the large lesion cavity (Fig. 6b), and persisted in the few remaining areas of necrosis within the lesion site.

Von Willebrand factor (VWF) staining for blood vessels and endothelial cells. (
An occasional VWF-positive cell or vessel was found within the group 3 scaffolds 1 week after injury (Fig. 6c), with the density being 0.9±0.4 per mm2. A small number of VWF-positive cells/vessels were also found in the group 4 scaffolds 4 weeks after implantation (Fig. 6d), with a density of 4.7±2.1 per mm2. The difference between groups 3 and 4, however, did not reach statistical significance.
Neuronal degeneration: Fluoro-Jade C
Many degenerating neurons were present in the thalamus 1 week after the injury. While individual neurons stained brightly for Fluoro-Jade C (FJC; Fig. 7c and d), there was also diffuse reactivity throughout areas of neuropil and extracellular matrix (Fig. 7a and b). Regions of the thalamus showing evidence of degeneration included the laterodorsal, ventrolateral, ventromedial, ventral anterior, ventral posteromedial, and ventral posterolateral nuclei. The positive staining of neuronal cell bodies was generally restricted to the left hemisphere, though a few degenerating cells could also be found in the right thalamus. The density of FJC-positive neurons in the left thalamus was 75.8±5.5 cells per mm2 (n=3) in group 1. Group 3 samples with implanted scaffolds had an average FJC density of 75.2±4.7 cells per mm2 (n=4), showing no significant difference relative to group 1. At 5 weeks post-injury, far fewer FJC-positive cells were observed relative to 1 week. Only a few scattered cells could be detected in the thalamus at high magnification.
Fluoro-Jade C (FJC) staining of degenerating neurons 1 week after PBI (group 1). (
Oligodendrocytes and myelinated axons: CNPase
At 1 week post-injury, there was a distinct absence of CNPase staining in and immediately around the lesion site. A clear discontinuity was observed in the corpus callosum (Fig. 8a), a white matter structure that would normally pass through the lesion area. Superior regions of the striatum that would normally have white matter bundles also showed an absence of staining (Fig. 8b). More inferior areas of the striatum showed preserved, but abnormal staining of white matter bundles. Relative to the contralateral hemisphere (Fig. 8c), the damaged white matter appeared to be filled with vacuoles that did not stain (Fig. 8d). Farther from the lesion, the CNPase staining regained an appearance similar to the contralateral hemisphere. At 5 weeks, with most of the necrotic tissue of the lesion cleared, CNPase staining was observed around the borders of the lesion area. In some cases, CNPase-positive axons traversed a path immediately along the edge of the cavity (Fig. 8e).

CNPase staining for oligodendrocytes and myelinated axons. (
While no CNPase staining was observed within the borders of the scaffolds in groups 3 and 4, myelinated axons did pass along the scaffold edges in some cases (Fig. 8f and g).
Post-mitotic neurons: NeuN
NeuN staining 1 week after injury revealed a boundary of the lesion within which no viable neurons were detected (Fig. 9a). The neuronal loss was found mainly in the striatum, though it extended to cortical layers in certain areas. At 5 weeks after injury, NeuN-positive neurons remained absent from the lesion site, but could be detected near the border of the PBI cavity (Fig. 9c). Neuronal nuclei could be observed in some cases as close as approximately 20 μm from the edge of the cavity (Fig. 9d).
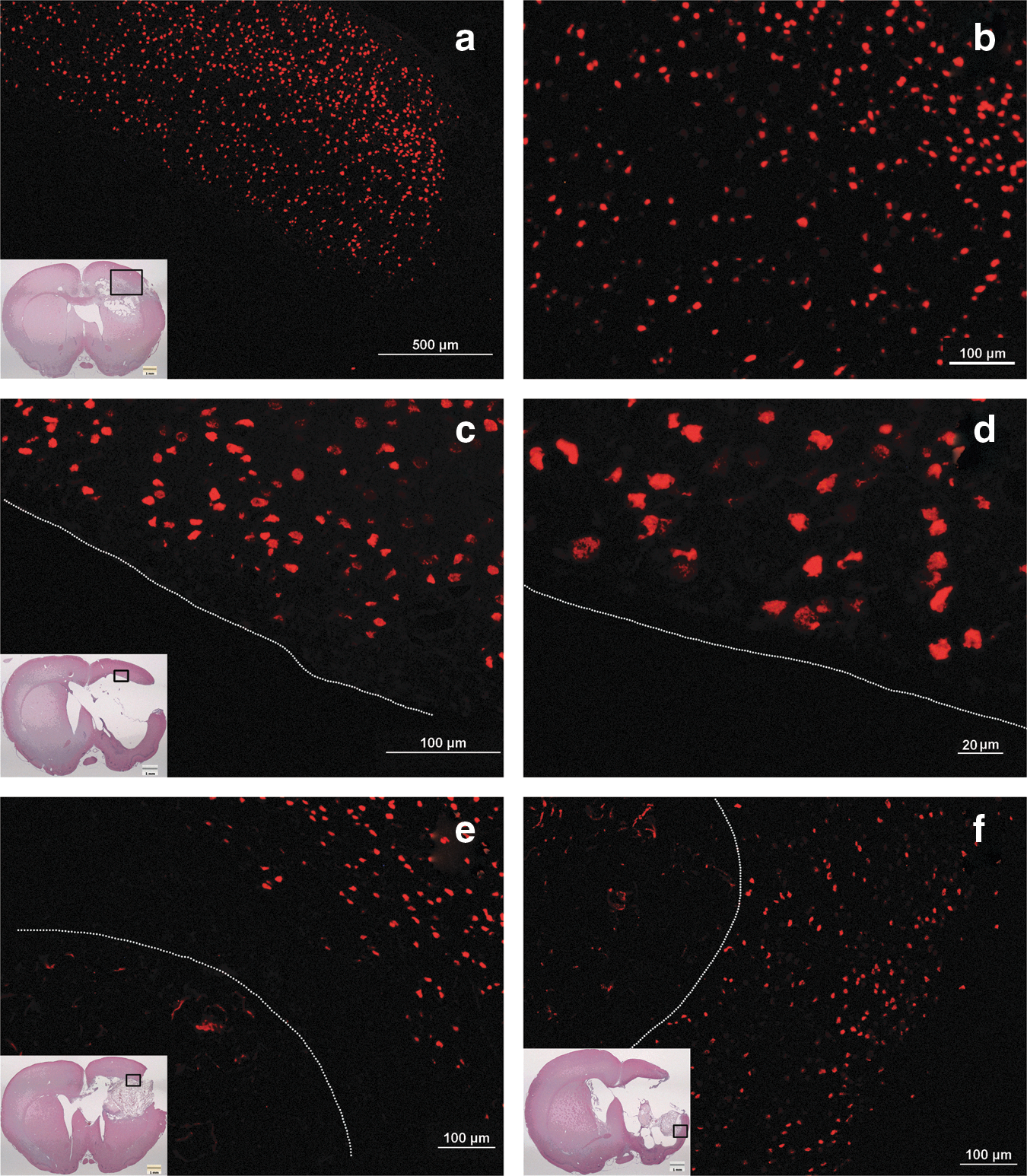
NeuN staining for post-mitotic neurons. (
No neurons could be detected in the scaffolds of groups 3 and 4. In group 3, there was a region of necrosis separating the areas of NeuN staining from the scaffold in some places (Fig. 9e). In group 4, the clearance of necrotic debris resulted in more areas where neurons were located in proximity to the scaffold border (Fig. 9f).
Neural progenitors: Doublecortin
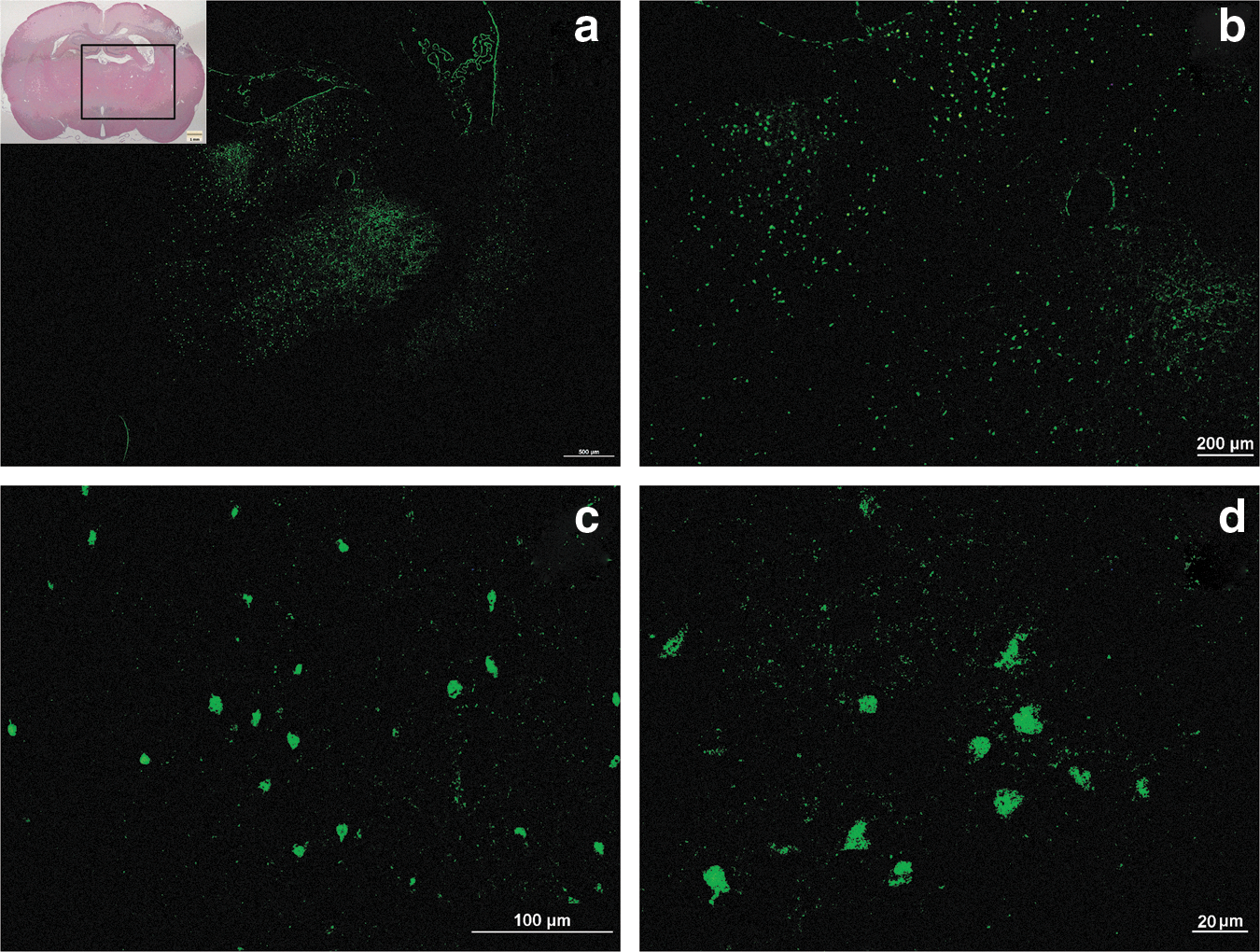
Cells staining positive for doublecortin (DCX) were observed in medial aspects of the lesion located near the lateral ventricles. At both 1 week (Fig. 10a) and 5 weeks (Fig. 10b) post-injury, DCX-positive cells could be seen spreading through the subventricular zone to the nearby border of the lesion cavity. The cells did not, however, appear to migrate to other regions of the injury. No DCX-positive cells were detected in or around the collagen scaffolds of groups 3 and 4.

Doublecortin (DCX) staining for neural progenitors. (
Discussion
While some general characteristics of the bilateral PBI lesion were similar to those reported for the unilateral frontal injury, significant differences were also noted. In particular, previous work with the frontal injury has suggested that most necrotic tissue is cleared by 1 week post-injury to form the permanent cavity (Williams et al., 2006a). In contrast, we found in the bilateral injury that an abundant amount of necrotic tissue was still present and in the process of being removed by macrophages at 1 week. This was the case despite the fact that the overall bilateral lesion volume was similar to values reported for the unilateral frontal injury (Shear et al., 2010; Williams et al., 2006a) at the same time point. The reason for the discrepancy is not certain, but it appears that acute trauma extending into both hemispheres may strain the brain's response capacity more than a comparable unilateral injury, resulting in slower remodeling of the lesion site.
The significant expansion of the lesion that we observed over time also differs from the reported progression of the unilateral frontal injury. Rather than expanding, the volume of the unilateral injury was noted to decrease between 1 and 5 weeks post-injury (Shear et al., 2010). The authors suggested that the decreased lesion volume may have been the result of increased pressure in the lateral ventricles associated with post-traumatic hydrocephalus. The disagreement between the results of the two studies might be related in part to the slower histological response we have noted in the bilateral injury. It is possible that the relative persistence of necrotic debris and associated cytotoxic elements might result in more secondary injury and loss of otherwise viable surrounding brain tissue. As a result, the long-term volume of the bilateral lesion may exceed that of the comparable unilateral lesion. While it is also possible that the sham surgery we conducted in group 2 may have caused a larger lesion, any such additional injury was expected to be small relative to the PBI. This is supported by previous work comparing the PBI to various surgeries involving insertion of the probe without inflating the balloon (Williams et al., 2005). Minimal injury was found in those procedures, which were more severe than the sham surgery we conducted.
With regard to potential biomaterial therapies, the time course for clearance of necrotic debris and cavity formation is important in determining the appropriate implantation time and biomaterial size. These issues must also be balanced with the ideal time for delivery of therapeutic agents. For example, certain neuroprotective agents would likely need to be delivered very shortly after the injury to have maximum efficacy in sparing viable tissue (Jain, 2008). In contrast, cellular or pharmacological agents aimed at axonal regeneration might be better suited for later time points, when the levels of cytotoxic and inflammatory elements are reduced (Williams et al., 2007; Zhang et al., 2005a). The use of a biomaterial at an early post-injury time point may be limited by the lack of space in the lesion, as the permanent cavity has not yet formed. While we have demonstrated in this study that a relatively small collagen scaffold can be implanted shortly after PBI, we found that it did not fill the cavity after several weeks in vivo. Immediate implantation of the collagen scaffold could be useful for delivering a neuroprotective agent, but the scaffold would be less effective for a long-term regenerative therapy unless the growth of the lesion were significantly reduced. As an alternative, delayed implantation would allow for the cavity to more fully form so that a biomaterial designed for its final size could fill it. The injury environment at a later time point may also be more hospitable for cellular therapies or pharmacological agents intended for axonal regeneration. The major drawback of delayed intervention is that the injury will progress uninhibited during the period before the therapy. The potential for limiting the damage of the injury would thus be greatly reduced. The 1-week implantation time point used in group 4 may have potential benefit in future work since the cavity has started to form, but the extent of secondary injury might potentially still be limited. However, the difficulty of simultaneously addressing the various aspects of this complex injury supports the notion that a combinatorial therapeutic strategy will ultimately be necessary for development of satisfactory treatment options. One potential approach could be to administer neuroprotective drugs peripherally or via targeted injection shortly after injury, while a biomaterial with cellular or pharmacological agents could be implanted into the lesion cavity at a later time.
In the choice of the biomaterial's size, it should be noted that there is a significant risk of damaging viable tissue if too large a material is forced into the brain lesion before a suitable cavity is available. In addition, mechanical properties should be taken into account to avoid an overly stiff material that might cause further injury to the soft brain tissue. Using a compliant material with characteristics reasonably similar to brain tissue may help to reduce the risk of damage during implantation. With an appropriate material, one might implant a large, but soft, scaffold into a small cavity such that the material will expand to continue to fill the cavity as it grows larger. We have recently conducted a study of viscoelastic mechanical properties of collagen scaffolds in order to help select appropriate scaffolds for future in vivo implantation experiments (Elias and Spector, 2012).
Relative to the unilateral frontal injury, the bilateral injury also displayed differences in the levels of gliosis and macrophage activation. It has been reported that GFAP and OX-18 (activated microglia) immunoreactivity after frontal PBI peaks around 3 days and returns to a very low level of reactivity by 7 days (Williams et al., 2007). We found in the bilateral injury that gliosis persisted at high levels at 7 days, while a robust macrophage response also clearly remained in progress. These results are consistent with the histological observation that the bilateral injury results in a slower remodeling of the lesion site relative to the unilateral injury.
The organized glial scar observed at 5 weeks post-injury presents an obstacle to regeneration (Fitch and Silver, 2008; Galtrey and Fawcett, 2007), and may be a target for therapeutic molecules delivered by a biomaterial. The persistence of macrophages at 5 weeks post-injury, particularly in white matter tracts, likely reflects the clearance of debris from slowly degenerating axons (Vargas and Barres, 2007). Myelin proteins in the CNS injury environment have been shown to induce growth cone collapse in regenerating axons, and therefore might also be therapeutic targets (Lee et al., 2003).
The other immunohistochemical markers also provide insight into features of the injury that may be relevant to development of therapeutic strategies. The profiles of NeuN and CNPase staining help to reveal the extent of the lesion by showing where neurons and myelinated axons have been lost or spared. In particular, the presence of neurons in proximity to the cavity border after 5 weeks suggests that it may be possible to promote cellular and axonal ingrowth if the cavity is filled with a substrate. The VWF staining illustrates that survival of implanted or endogenous cells within the lesion site may also be possible due to the location of blood vessels immediately bordering the cavity. The large decrease in Fluoro-Jade C-positive cells in the thalamus between 1 and 5 weeks post-injury likely reflects a stabilization of the lesion. The time course for resolution of the injury progression may help to determine appropriate times for therapeutic intervention. The presence of DCX-positive neural progenitors near the lesion cavity may have benefit in potentially replacing certain populations of neurons. The fate of progenitors from the subventricular zone has been studied in stroke models, where it was shown that DCX-positive neuroblasts can migrate to the damaged striatum and express markers of medium spiny neurons (Arvidsson et al., 2002; Parent et al., 2002; Picard-Riera et al., 2004; Yamashita et al., 2006). Cells from the subventricular zone have also been noted to proliferate and migrate to injured regions following traumatic brain injury (Goings et al., 2004; Ramaswamy et al., 2005; Richardson et al., 2007; Salman et al., 2004). Delivery of chemoattractant molecules such as stromal derived factor 1 (SDF-1; Sun et al., 2004) and stem cell factor (SCF; Chang et al., 2007) may improve recruitment of the progenitors to the lesion site.
The collagen scaffold and associated surgical procedures in this study appear to be tolerable for the animals, based in part on the absence of mortality during and after the scaffold implantations. In addition, scaffold implantation immediately after injury did not cause an increase in the lesion volume or the density of degenerating neurons in the thalamus 1 week later. The scaffold also did not appear to cause a major inflammatory response at the histological level. It does, however, appear that the delayed scaffold implantation procedure could have the potential to increase lesion volume in some cases. This possibility may be investigated further in a future study using multiple scaffolds varying in size and mechanical behavior.
The observation that the scaffold remained intact with open and interconnected pores may have benefit in treatment applications. By establishing that the scaffold can retain its structure in the brain for several weeks and potentially longer, we have shown that it can act as a long-term extracellular matrix analog. The regeneration of axons is a relatively slow phenomenon, so a biomaterial therapy with this goal would likely require a slow degradation rate. Additionally, a scaffold that resorbs slowly may allow for sustained delivery of incorporated pharmacological agents over weeks or months. The preserved pore structure also ensures that endogenous or exogenous cells can migrate into the lesion site.
Although a recently published study involving the frontal PBI model has also reported the use of a collagen scaffold (Chen et al., 2011), substantial differences exist in both the material used and the results obtained. While we employed a pre-formed collagen scaffold with a defined pore structure, the collagen material used by the Chen group was a liquid suspension injected by syringe into the lesion site. The collagen appeared to undergo rapid degradation when injected alone, as it could not be detected in the brain 2 weeks later. This is in contrast to the lack of degradation observed in the scaffolds in our study over several weeks. The liquid injection appears as though it may be of value for short-term therapies, while the pre-formed scaffold in our work might be more suitable for a longer time frame. Interesting future work could involve a study devoted specifically to identifying the degradation rates of various scaffolds implanted into PBI lesions.
Another potentially beneficial aspect of the scaffold used in this work was seen in the ability of various cell types to cross the tissue-implant interface. Although the numbers of astrocytes, macrophages, and endothelial cells were relatively low, the open and interconnected pores appeared to facilitate cell migration into the defect. While it is possible that some cells could have been brought into contact with the scaffold margins during the implantation procedure, it is likely that most cells infiltrated the scaffold after implantation. This is supported by the fact that CD68-positive macrophages are generally not present in the uninjured brain (based on our work with the antibody), implying that scaffolds implanted immediately after injury would not have encountered that cell type. Additionally, the absence of significant amounts of extracellular matrix makes it less likely that the astrocytes and endothelial cells originated from pieces of tissue embedded in the scaffold pores. The open pore structure and the observation of cells crossing the boundary with the brain suggest that many cells were the result of infiltration in both the immediate and delayed implantation groups. While it is not possible to definitively determine when cells entered the scaffold, future work might include multiple time points to study the time frame for cellular infiltration.
The relatively small number of astrocytes detected within the scaffolds is interesting in that some studies using scaffolds in the brain have reported astrocytes as a major component of cellular infiltration (Deguchi et al., 2006; Tian and Kyriakides, 2009; Tian et al., 2005; Woerly et al., 1992,1999; Wong et al., 2008). However, our study and others indicate a wide variability in the degree of astrocyte infiltration (Hou et al., 2005; Nakada et al., 2009; Plant et al., 1997; Wong et al., 2007; Zhang et al., 2007a). In addition to potential factors such as the injury model, the implantation time, and the duration of the study, astrocyte infiltration might also be significantly affected by the material composition of the scaffold. While we observed that type I collagen scaffolds did not appear to promote infiltration of large numbers of astrocytes, two studies using synthetic materials (Deguchi et al., 2006; Tian et al., 2005) described scaffolds containing more astrocytes than macrophages. Further study of astrocyte infiltration is of significance in part because it has been suggested that a scaffold may modify the formation or persistence of a glial scar (Hou et al., 2005; Tian et al., 2005; Woerly et al., 1992; Wong et al., 2007). While a collagen scaffold by itself does not appear to have a significant effect on the glial scar after PBI, it could potentially be used to deliver an appropriate therapeutic molecule.
Many of the cells present in the collagen scaffold were CD68-positive macrophages, but the absence of multinucleated giant cells suggests there was not a strong foreign body response. While there may have been a mild macrophage response to the scaffold itself, it is likely that some cells were responding to the presence of necrotic debris and hemorrhage in the vicinity of the scaffold. Erythrocytes, for example, could be observed within the scaffold where they were likely undergoing phagocytosis by macrophages. The presence of macrophages is consistent with other reports of implanted biomaterials in the brain (Deguchi et al., 2006; Hou et al., 2005; Nakada et al., 2009; Plant et al., 1997; Tian and Kyriakides, 2009; Tian et al., 2005; Woerly et al., 1992,1999; Wong et al., 2007,2008). While macrophages have complex functions in mediating physiological processes related to inflammation, angiogenesis, cell survival, and regeneration (Hunt et al., 1984; Kigerl et al., 2009; Knowlson, 1974), they can also play an important role in degrading biomaterials in tissue engineering applications. For example, in treating skin and peripheral nerve injuries, one may design a biomaterial to undergo degradation at a rate similar to the rate of synthesis of new tissue (Yannas, 2005). In the brain, a modest goal for newly synthesized tissue might be a vascularized extracellular matrix that could serve as a substrate for endogenous or exogenous cells to repopulate a lesion site. The scaffold used in this study showed resistance to degradation over the time course studied, but a more robust infiltration of macrophages and other cells might result in eventual resorption.
The positive staining for endothelial cells in the collagen scaffold has significant implications for treating PBI. A vascularized biomaterial can provide both a physical substrate for cells in the lesion cavity, as well as a supply of oxygen for long-term cell survival. Based on the time course for vascularization, one could potentially implant the scaffold and then deliver exogenous cells via targeted injection at a later time. While our results are comparable with other work (Nakada et al., 2009), the infiltration of endothelial cells was likely limited by the small size of the scaffold relative to the PBI lesion. Implantation of a larger scaffold would increase the surface area contacting the surrounding brain, which could potentially increase cellular infiltration and vascularization. Studies using other biomaterials have also reported vascularization of implanted scaffolds when they are in contact with the surrounding tissue (Hou et al., 2005; Plant et al., 1997; Tian et al., 2005; Woerly et al., 1992,1999; Zhang et al., 2007a). In addition to using a larger scaffold, a molecule such as vascular endothelial growth factor (VEGF) could be incorporated to increase vascularization (Zhang et al., 2007a).
Conclusions
This work has provided histological characterization of a bilateral PBI and examined differences in comparison to published work with a frontal unilateral injury. The progression of the lesion from 1 week to 5 weeks has also been described, with a notable increase in the size of the PBI lesion and resulting cavity in the brain. This information contributes to an understanding of the histopathology of PBI, but also provides guidance in the development of a therapeutic approach using biomaterials. Based on our initial work implanting a 3-mm-diameter collagen scaffold in the PBI lesion, we have seen that the scaffold must be significantly larger in order to fill the PBI cavity after several weeks. Further, it was noted that cellular infiltration of implanted collagen scaffolds was of low density after periods of 1 week and 4 weeks in vivo. Cells present in the scaffolds consisted mostly of macrophages, although astrocytes and endothelial cells were also present. Future studies may incorporate cellular or pharmacological agents into collagen scaffolds to promote neuroprotection and stimulate regeneration.
Footnotes
Acknowledgments
The research reported here was supported by the U.S. Department of Veterans Affairs, Veterans Health Administration, Rehabilitation Research and Development Service. M.S. is a VA Research Career Scientist.
We thank Drs. Kimberly Leite-Morris and Rahmatullah Cholas for valuable assistance with the initial animal surgeries and surgical photographs. We also thank Alix Weaver for assistance with the hematoxylin and eosin staining. We are indebted to Dr. Frank C. Tortella of the Walter Reed Army Institute of Research (Silver Spring, MD), and Dr. Anthony J. Williams (then of WRAIR), and to James Groer of Dragonfly Research & Development, Inc. (Ridgeley, WV), for their advice, helpful discussions, and encouragement.
Author Disclosure Statement
No conflicting financial interests exist.