
Abstract
Diffusion tensor imaging (DTI) has recently emerged as a useful tool for assessing traumatic brain injury (TBI). In this study, the prognostic value of the relationship between DTI measures and the clinical status of severe TBI patients, both at the time of magnetic resonance imaging (MRI), and their discharge to acute TBI rehabilitation, was assessed. Patients (n=59) admitted to the trauma center with severe closed head injuries were retrospectively evaluated after approval from the institution's institutional review board, to determine the prognostic value of DTI measures. The relationship of DTI measures, including apparent diffusion coefficient (ADC), fractional anisotropy (FA), axial (λ‖) and radial diffusivity (λ⊥) from the whole brain white matter, internal capsule, genu, splenium, and body of the corpus callosum, were compared with neurological status at MRI and at discharge to acute TBI rehabilitation. Whole brain white matter averages of ADC, λ‖, and λ⊥, and their coefficient of variation (CV) were significantly correlated with the Glasgow Coma Scale (GCS) score on the day of MRI. The average λ‖ was significantly correlated with GCS scores on the day of MRI in all measured brain regions. Outcomes were associated with whole brain white matter averages of ADC and λ‖, and the CVs of FA, ADC, λ‖, and λ⊥; and the averages and CVs of FA and λ‖ in all corpus callosum regions. The inclusion of regional and global DTI measures improved the accuracy of prognostic models, when adjusted for admission GCS score and age (p<0.05). Whole brain white matter and regional DTI measures are sensitive markers of TBI, and correlate with neurological status both at MRI and discharge to rehabilitation. The addition of DTI measures adjusted for age, gender, and admission GCS score significantly improved prognostic models.
Introduction
T
It is common for patients with TBI to have moderate-to-severe disabilities following head injury (Thornhill et al., 2000). In cases in whom cerebral lesions are present, these disabilities are appreciable even 15 years post-injury, with profound effects on quality of life (Teasdale and Engberg, 2005). However, even TBI patients with normal-appearing conventional magnetic resonance imaging (MRI) scans may demonstrate decrements in performance on tests of cognition (Kurca et al., 2006). TBI can have lasting effects on attention, cognitive speed, learning and memory, executive function, verbal ability, intellect, motivation, affect, and neurological function, with the degree of impairment and disability dependent on the nature and severity of the insult (Meythaler et al., 2001; National Institutes of Health Consensus Development Panel on Rehabilitation of Persons with Traumatic Brain Injury, 1999; Vaishnavi et al., 2009). The effects of physical insults can be immediate, or can manifest over several days following the initial injury (Meythaler et al., 2001; National Institutes of Health Consensus Development Panel on Rehabilitation of Persons with Traumatic Brain Injury, 1999). Secondary injury to the brain shortly follows the initial insult, and may include ischemia, cerebral hypotension, edema, elevated intracranial pressure, and altered metabolism.
Early in the course of TBI, prognosis can be complicated by the limitations of traditional clinical measures, such as the Glasgow Coma Scale (GCS) and computed tomography (CT) features. The GCS score is a less reliable indicator of TBI severity in mild or moderate TBI. Further, the validity of the GCS in severe TBI can be undermined by intoxication or medical intervention (intubation, sedation, or administration of paralytics) prior to admission or transfer to rehabilitation (Gabbe et al., 2003; Marshall et al., 1991; Moppett, 2007; Murray et al., 1999; Saatman et al., 2008; Stochetti et al., 2004). Due to these factors, the European Brain Injury Consortium (EBIC) found that a full GCS assessment was only testable in 56% of patients on admission to neurosurgical units (Murray et el., 1999). The GCS score can decline due to evolving pathology over the first 72 h post-injury, and up to one-third of patients who die of TBI will talk or obey commands before ultimately dying (Moppett, 2007). Injury classification systems based on CT findings, such as the Marshall classification, are able to predict important clinical end-points such as the risk of mortality or rising intracranial pressure (ICP), but qualitative scoring systems can suffer from significant inter-observer variability (Moppett, 2007; Saatman et al., 2008). In addition, patients can have normal-appearing CT and MRI results and still be profoundly comatose and have poor functional outcomes, or a normal CT and neurological status depressed by intoxication (Saatman et al., 2008). Only 10% of diffuse axonal injury (DAI) cases will present with the typical hemorrhagic pattern observed on CT, and more than 80% of DAI is non-hemorrhagic, leading to an under-appreciation of axonal injury (Meythaler et al., 2001). The diffuse nature of these injuries may not be apparent in the acute phase of injury on conventional diagnostic imaging, which may limit its prognostic value (Meythaler et al., 2001). Additionally, measures that are associated with survival may not necessarily be associated with good functional outcome as measured on the Glasgow Outcome Scale Extended (GOSE; van der Naalt et al., 1999).
There has been significant interest recently in the use of diffusion tensor imaging (DTI) in the evaluation of TBI patients. Diffusion MRI has shown sufficient sensitivity to visualize lesions that may be inconspicuous or absent on conventional MRI sequences (Arfanakis et al., 2002), and thus may better depict diffuse injury in TBI. Since DTI is a quantitative, physiologically-derived parameter, it may provide a more objective measure of axonal injury for use in TBI classification and prognosis. Decreased fractional isotropy (FA) in the lobar white matter, corpus callosum, internal capsule, and other white matter structures has been reported in acute TBI patients (Arfanakis et al., 2002; Huisman et al., 2004), which appears to persist or evolve in the sub-acute and chronic phases of TBI (Bendlin et al., 2008; Greenberg et al., 2008; Inglese et al., 2005). These decreases in FA have been linked to poor clinical outcomes or performance on cognitive testing in the chronic phases of injury (Kennedy et al., 2009; Kumar et al., 2009; Nakayama et al., 2006; Sidaros et al., 2008). Although there are some reports on the use of DTI among severely injured TBI patients in the acute stage (Meythaler et al., 2001), the use of DTI as a quantitative prognostic marker has not been assessed among severely injured patients.
The goal of this study was to determine whether DTI markers at admission, including axial diffusivity (λ‖), radial diffusivity (λ⊥), apparent diffusion coefficient (ADC), and FA at the whole-brain level and at the regional level provide prognostic information about the outcomes of severe TBI patients.
Methods
The University of Maryland's institutional review board approved this study for retrospective evaluation, and the study was compliant with the requirements of the Health Insurance Portability and Accountability Act.
Patients
Patients were selected and screened from a consecutive list of 126 individuals from the radiology database who received DTI as part of a standard clinical evaluation for blunt TBI on a 1.5-Tesla scanner between September 2007 and May 2009. Patients who were 18 years or older were considered for inclusion. Each patient's GCS score was obtained at admission (admission GCS), on the day of MRI (scan GCS), and at discharge (discharge GCS). Since the patient's GCS can be altered by intoxication, medical intervention prior to admission, or evolving TBI pathology, we used both the admission GCS and scan GCS to determine the severity of injury. This allowed inclusion of patients whose GCS scores declined from the time of admission to the MRI scan. Patients were considered to be in the severe TBI category if they had a low admission GCS or scan GCS score (GCS≤8). For comparison purposes, a higher-GCS TBI reference group was also included, whose GCS scores remained high (GCS≥13) throughout hospitalization, with negative CT and MRI findings.
Of the 126 patients screened, 30 patients who had severe motion artifacts or image distortion on diffusion-weighted images were not included in this study. Three additional patients were excluded due to the presence of stroke, as it was unclear whether the stroke preceded the trauma or was a result of the trauma. An additional 34 patients were not included because they did not meet the minimum age criteria, or because their GCS score was in the moderate range of 9–12, or because they met the mild-TBI reference group criteria, but had positive CT or MRI scans. The total number of patients who ultimately were included in this study was 59, with 41 patients belonging to the severe TBI group and 18 patients belonging to the mild TBI reference group.
The total patient population (n=59; age 37.2±16.8 years, range 18–83 years; 43 male, 16 female) that was included in the study consisted of a heterogeneous mixture of closed head injuries, from mechanisms including motor vehicle collisions (n=26), falls (n=15), struck pedestrians (n=7), other vehicular accidents (bicycles, motorcycles, and all-terrain vehicles: n=5), assaults (n=3), or other mechanisms (n=3: found down, sports injury, or struck in the head by thrown objects). Patients were imaged 3.7±6.1 days post-admission (max 28 days), with half of the sample imaged within 1 day of admission, and 81% imaged within 5 days of admission.
The outcome for the severe TBI group (n=41, age 38.0±17.0 years; 33 males) was determined by discharge status from the hospital. The four outcome categories for the severe TBI group included death (n=10, age 50.9±17.1 years, 7 male, admission GCS score 4.3±2.6), or neurological status at the time of discharge to the rehabilitation center: severe discharge GCS score (n=8, age 30.8±16 years, 7 male, admission GCS score 5.1±3.0), moderate discharge GCS score (n=17, age 36.5±15.3 years, 14 male, admission GCS score 5.0±3.0), or mild discharge GCS score (n=6, age 30.2±13.0 years, 5 male, admission GCS score 8.0±4.6). All surviving severe TBI patients were discharged to rehabilitation between 4 and 50 days post-admission, with a median length of hospitalization of 20 days.
Imaging findings varied among study patients, and included contusions (n=25), subarachnoid hemorrhages (n=13), subdural hematomas (n=23), diffuse axonal injury (n=18), diffuse cerebral edema (n=14), herniation (n=8), and midline shifts (n=7). Some patients underwent ventriculostomy (n=17) and craniectomy (n=12) prior to MRI.
The mild TBI reference group consisted of 18 individuals (age 35.3±16.6 years, 10 males) who were discharged from the hospital to home within 1.7±2.8 days. Example images of the patients belonging to each of the five outcome groups are shown in Figure 1.
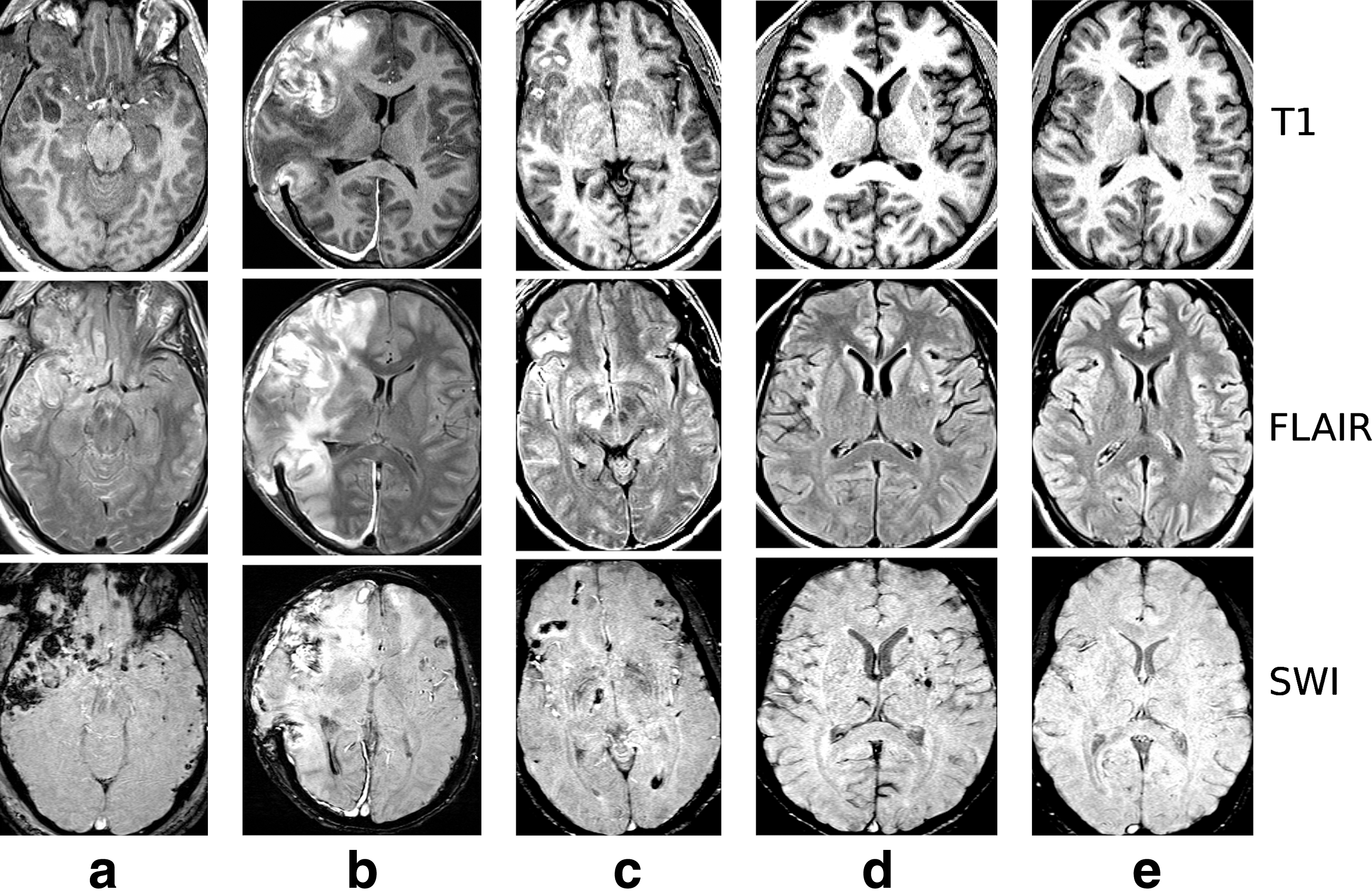
Example conventional images (T1-MPRAGE/FLAIR/SWI) for each outcome group. (
Magnetic resonance imaging
All imaging was performed on a 1.5-T Avanto scanner (Siemens Medical Solutions, Erlangen, Germany) with parallel imaging capability. Conventional MR imaging included axial T2 using turbo spin echo (TEeff/TR/ETL=113/5900 msec/15, 5-mm slices with 1-mm inter-slice gap, 0.6×0.4-mm in-plane resolution), fluid attenuated inversion recovery (FLAIR; TEeff/TI/TR/ETL=102/2500/8000/13 msec, 5-mm slices with 1-mm inter-slice gap, 1.2×0.9-mm in-plane resolution), volumetric T1 (TE/TR=4.76/11 msec with 20° flip angle, 1×1×2-mm voxels), and susceptibility weighted imaging (SWI; TE/TR=40/50 msec with 25° flip angle, 0.5×0.5×2-mm voxels).
DTI images were obtained using a double spin-echo echo-planar imaging technique over a 23-cm field of view (FOV), at an in-plane resolution of 1.79×1.79 mm, and a slice thickness of 2 mm (3 averages; TE/TR of 95/11,200 msec, parallel imaging acceleration factor of 2). A total of 68 axial images were acquired to cover the brain from the apex to the skull base. Diffusion gradients were sensitized in 12 collinear directions at an effective b-value of 1000 sec/mm2.
Image processing and analysis
The DTI images were exported offline and processed using FDT (FMRIB Diffusion Toolbox; FMRIB, Oxford, U.K.). Images were first corrected for eddy current-induced image distortion, following which the brain parenchyma was extracted using the Brain Extraction Tool (BET) available within the FSL (FMRIB Software Library, Oxford, U.K.), and the diffusion tensor was estimated for each voxel (Smith, 2002; Smith et al., 2004).
The FA maps of all patients were aligned to the ICBM template derived using data from 152 subjects, and segmented into gray matter, white matter, and cerebrospinal fluid (CSF) maps using SPM5 (Wellcome Department of Imaging Sciences; University College London, London, U.K.). Segmented images were visually inspected to confirm the accuracy of white matter segmentation results. The segmented white-matter images were used to obtain information on whole-brain white matter ADC, FA, λ‖, and λ⊥ values. Regions of interest with varying geometry to best fit the regions as shown in Figure 2 were drawn on the genu, splenium, and body of the corpus callosum, and the internal capsule. Summary statistics such as the mean, standard deviation (SD), and coefficient of variation (CV) for each of the above parameters were calculated using MATLAB (Mathworks, Natick, MA). These summary measures were used in statistical models for predicting a patient's outcome category as described below.
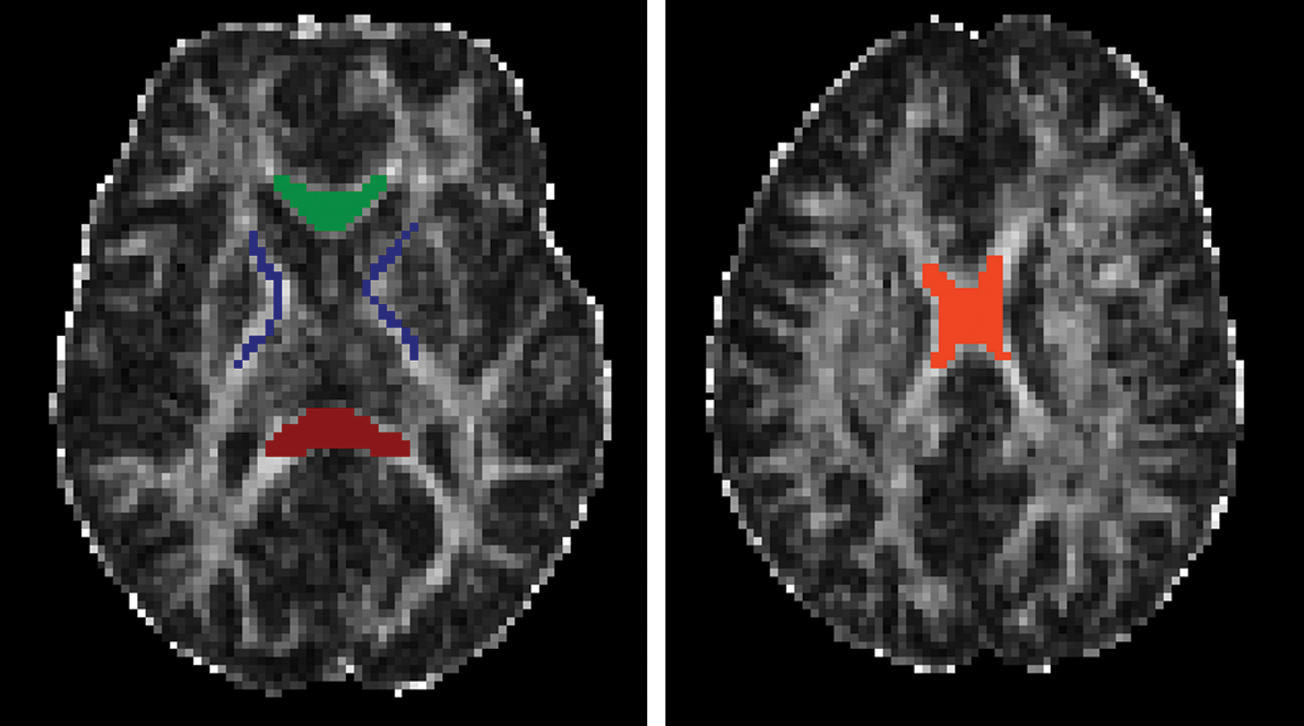
Example of typical regions of interest (ROIs) in the internal capsule (blue), genu (green), splenium (red), and body of the corpus callosum (orange), the areas where the diffusion tensor imaging parameters were obtained. Color image is available online at
Statistical analysis
Nonparametric correlation coefficients (Spearman's partial rho) adjusted for age and gender were used to examine the relationship in all patients between DTI parameters and the scan GCS and the discharge GCS. Further, the relationship between each outcome category and DTI parameters on a global and regional level in the white matter in all patients was also examined.
Prognostic models of severe TBI patient outcomes were created using ordinal logistic regression models. These models were adjusted for age, gender, time to scan, and admission GCS score to determine if DTI parameters significantly improved prediction of patient outcome status among severe TBI patients. Improvement in model fit was judged by comparing the differences in model deviance to the critical values of the chi-square distribution. Regression models were chosen by best subset selection based on the score criterion, selecting from all whole-brain DTI measures. Statistical analysis was conducted with SAS 9.2 for Windows XP (SAS Corporation, Cary, NC), and plots were produced using R (R Foundation for Statistical Computing, Vienna, Austria). Correlations were corrected for multiple comparisons using the FDR method of Benjamini and Hochberg (1995). Statistical significance for all hypothesis testing procedures was set at p<0.05.
Results
There was no difference in the median age between severe TBI patients and the mild TBI reference group. However, there were significant differences between the median ages of the different outcome groups (p=0.016). Bonferroni-adjusted post-hoc tests indicate that the median ages significantly differed between severe TBI patients with mild discharge GCS scores (age 29.4±12.2 years), and severe TBI patients who died (age 50.9±17.1 years). No other groups differed significantly in median age.
Regional and global DTI correlation with GCS scores
Table 1 lists the partial correlations, corrected for age and gender, between the DTI and scan GCS scores among all the patients included in this study. The average ADC (r=0.46; p<0.0003), λ‖ (r=0.61; p<0.0001), and λ⊥ (r=0.33; p=0.013), for the whole-brain white matter demonstrated a strong positive relationship with GCS, indicating that global white matter decrements in DTI parameters are associated with poor clinical presentations. The CV of the above parameters, including those of FA, also demonstrated a significant negative correlation with GCS, suggesting that variability in the DTI values increased with the severity of injury. Similar patterns of decrements in average DTI parameters and increases in CV were observed in regional measures. The body of the corpus callosum showed strong positive correlations of average ADC (r=0.36; p=0.007), and λ‖ (r=0.63; p<0.0001), and negative correlations of the CV of λ‖ (r=−0.31; p=0.04) with GCS. The genu (r=0.56; p<0.0001), splenium of the corpus callosum (r=0.35; p=0.0075), and the internal capsule (r=0.40; p=0.0022), all demonstrated a strong correlation between λ‖ and the clinical status of the patient. The CV of λ‖ in the splenium (r=−0.26; p=0.049), and the CV of ADC in the internal capsule (r=−0.51; p<0.0001) also exhibited significant negative relationships with clinical status. The average FA (r=0.40; p=0.0019), and the CV of FA (r=−0.40; p=0.0072), demonstrated a strong correlation with the GCS only in the body of the corpus callosum, but not in other regions, or the whole-brain level.
The internal capsule could not be measured in one patient due to the severity of her injuries, which prevented placement of regions of interest. The p values are shown in parenthesis for each of the correlations. Significant correlations are shown in bold, and those that remained significant after corrections for multiple comparisons are marked with an asterisk.
FA, fractional anisotropy; CV, coefficient of variation; ADC, apparent diffusion coefficient; Avg, average; DTI, diffusion tensor imaging; GCS, Glasgow Coma Scale.
DTI parameters and patient outcomes
Table 2 lists the average values of the various DTI parameters for each of the four patient outcome groups and the mild TBI reference group for the whole-brain white matter, internal capsule, genu, splenium, and the body of the corpus callosum. At the whole-brain white matter level, reduced average ADC and λ‖ were associated with poor patient outcomes at discharge, while FA and λ⊥ were not significantly associated with patient outcomes. Regional measurements at the splenium, the body of the corpus callosum, the genu, and the internal capsule exhibited similar relationships with patient outcomes, with the exception that the association of FA with patient outcomes was much stronger on a regional basis. The variability of the DTI values within the regions of interest (ROI) were also associated with patient status, with greater heterogeneity in the white matter being associated with poor patient outcomes.
Values shown are mean±standard deviation.
FA, fractional anisotropy; ADC, apparent diffusion coefficient; Avg, average; DTI, diffusion tensor imaging.
The partial correlation coefficients, corrected for age and gender, between patient outcomes and DTI measures at the whole-brain white matter and at the regional level for all patients are listed in Table 3. Favorable patient outcomes were associated with higher mean ADC (r=0.33, p=0.011) in the whole-brain white matter, as shown in Figure 3. An even stronger relationship was observed between favorable patient outcomes and higher values of λ‖ (r=0.58, p<0.0001), suggesting that the association between water diffusion changes and patient outcomes is primarily driven by changes in axial diffusivity. Greater heterogeneity in the DTI values, as measured by the CV of ADC (r=−0.62, p<0.0001), and λ‖ (r=−0.56, p<0.0001), were strongly associated with poor patient outcomes. This association between the heterogeneity of the DTI values was also observed in the CV of FA (r=−0.31, p=0.01), and λ⊥ (r=−0.53, p<0.0001), although their average values (r=0.16, p=0.23 and r=0.17, p=0.22, respectively) did not exhibit a strong relationship with patient outcome.
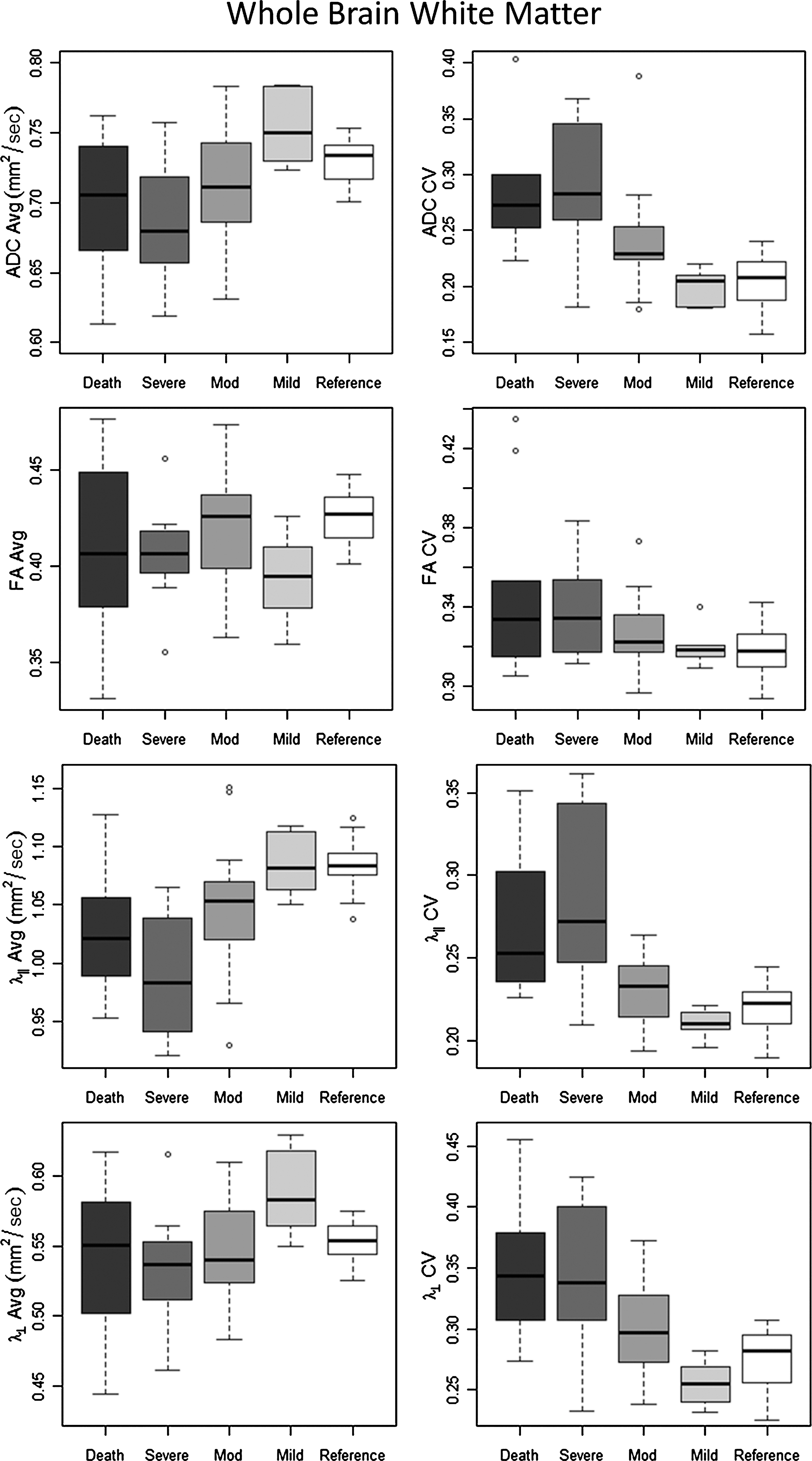
Diffusion tensor imaging (DTI) parameters, including average mean diffusity (MD), fractional anisotropy (FA), axial diffusivity (λ‖), and radial diffusivity (λ⊥), and their coefficient of variation (CV) for the whole-brain white matter for the different outcome groups (ADC, apparent diffusion coefficient).
The internal capsule could not be measured in one patient due to the severity of her injuries, which prevented placement of regions of interest. The p values are provided in parentheses for each of the correlations. Significant correlations are shown in bold, and correlations that remained significant after corrections for multiple comparisons are marked with an asterisk.
FA, fractional anisotropy; CV, coefficient of variation; ADC, apparent diffusion coefficient; Avg, average; DTI, diffusion tensor imaging.
In the genu of the corpus callosum, lower averages of ADC (r=0.35, p=0.0068), and λ‖ (r=0.59, p<0.0001), were significantly related to poor patient outcomes (Fig. 4). In the splenium of the corpus callosum, lower averages of FA (r=0.34, p=0.01), and λ‖ (r=0.38, p=0.0036), were significantly related to poor patient outcomes (Fig. 5). Additionally, higher CVs of FA (r=−0.32, p=0.014) were significantly related to poor patient outcomes. In the body of the corpus callosum, lower averages of FA (r=0.47, p=0.0002), ADC (r=0.32, p=0.016), and λ‖ (r=0.62, p<0.0001) were significantly related to poor patient outcomes (Fig. 6). The corpus callosum also exhibited higher CV of ADC (r=−0.30, p=0.024), FA (r=−0.52, p<0.0001), and λ‖ (r=−0.38, p=0.0037), that were significantly related to poor patient outcomes.
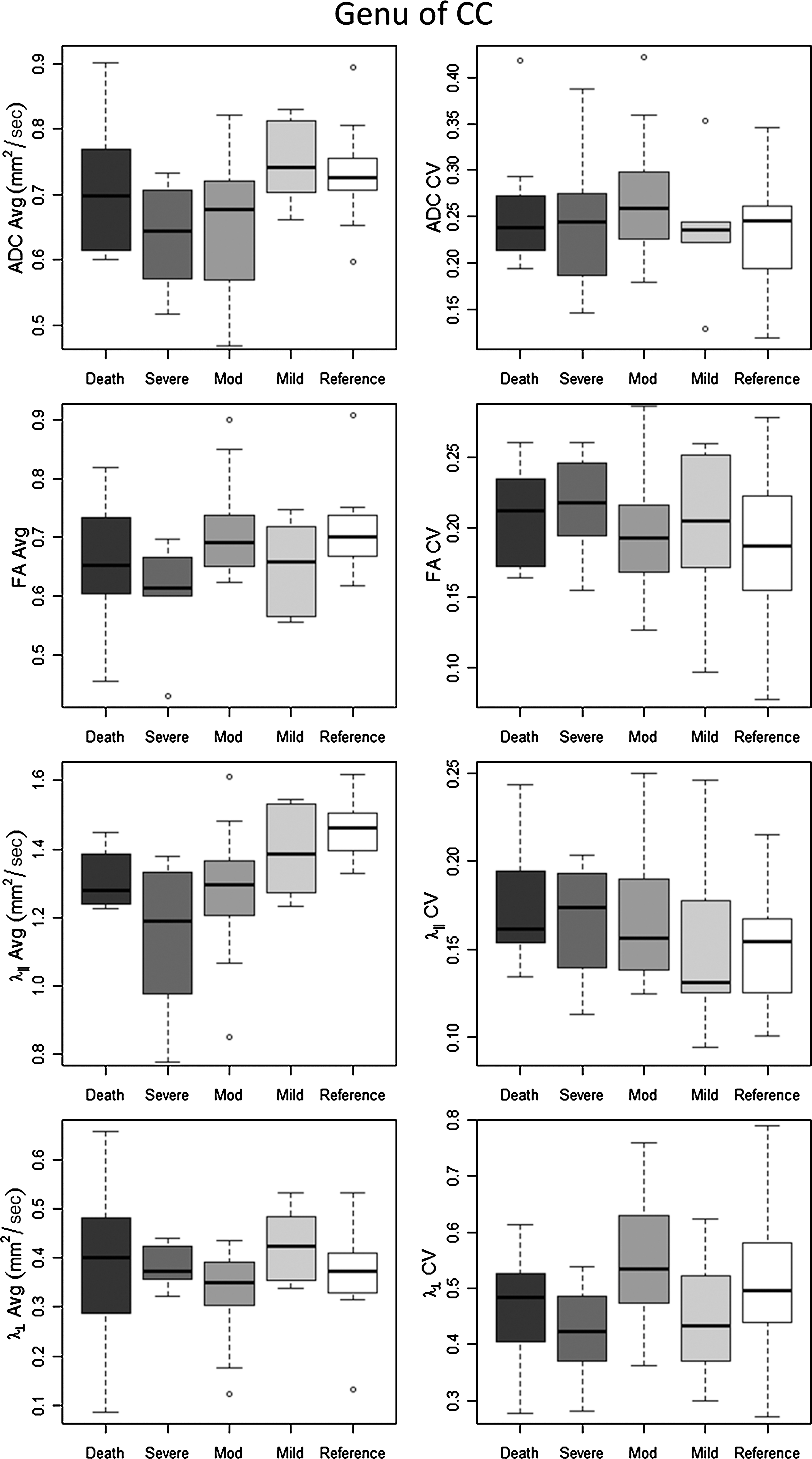
Diffusion tensor imaging (DTI) parameters, including average mean diffusity (MD), fractional anisotropy (FA), axial diffusivity (λ‖), and radial diffusivity (λ⊥), and their coefficient of variation (CV) for the genu of the corpus callosum (CC) for the different outcome groups (ADC, apparent diffusion coefficient).

Diffusion tensor imaging (DTI) parameters, including average mean diffusity (MD), fractional anisotropy (FA), axial diffusivity (λ‖), and radial diffusivity (λ⊥), and their coefficient of variation (CV) for the splenium of the corpus callosum (CC) for the different outcome groups (ADC, apparent diffusion coefficient).
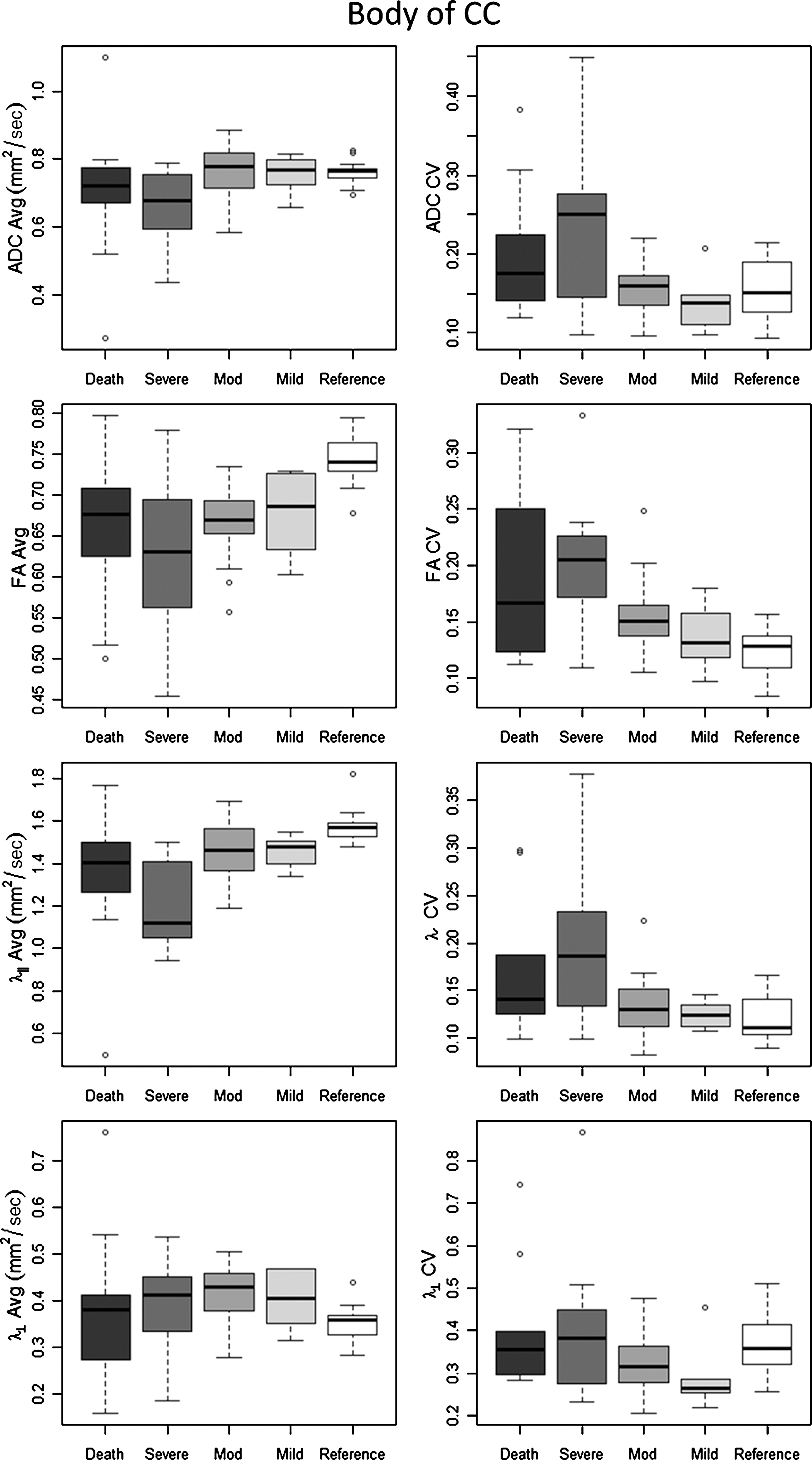
Diffusion tensor imaging (DTI) parameters, including average mean diffusity (MD), fractional anisotropy (FA), axial diffusivity (λ‖), and radial diffusivity (λ⊥), and their coefficient of variation (CV) for the body of the corpus callosum (CC) for the different outcome groups (ADC, apparent diffusion coefficient).
In the internal capsule, lower average λ‖ (r=0.41, p=0.0017), and higher CV of ADC (r=−0.52, p<0.0001), and λ⊥ (r=−0.28, p=0.036), were significantly related to poor patient outcomes.
Logistic models for patient outcomes using DTI parameters
When predicting outcome utilizing logistic models using a single whole-brain DTI summary measure, the CV for whole-brain white matter ADC or λ‖ best predicted outcome. The use of any whole-brain ADC or axial diffusivity measure (average or CV) significantly improved model prediction (p<0.05), when adjusted for admission GCS, age, gender, and time from admission to scan. Among the combinations of various DTI metrics, the addition of λ⊥ had the least effect on model prediction, while λ‖ and ADC had the strongest influence on model prediction. Due to the correlation between the various DTI measures at both the whole-brain and regional level, little additional improvement in model fit was observed by adding more than three DTI measures.
Discussion
Conventional CT and MR imaging provide valuable information for surgical planning in TBI patients, but are not adequate for the characterization, quantification, and determination of the extent of axonal injury (Haacke et al., 2010; Meythaler et al., 2001). The GCS is a rough neurological measure with known limitations in classifying the true extent of TBI, including reduced sensitivity in the lobar white matter, ceiling effects, and questions of reliability in the presence of intoxication or medical interventions prior to admission (Gabbe et al., 2003; Marshall et al., 1991; Moppett, 2007; Saatman et al., 2008; Stochetti et al., 2004). In this study, DTI values obtained in the acute phase of injury were associated with gradations in neurological status as measured by the GCS. Severe TBI patients with good outcomes had DTI values similar to those of mild TBI patients. In models of severe TBI patient outcomes, DTI values provide prognostic information about a patient's discharge status, independent of factors that may make the GCS unreliable (Brain Trauma Foundation et al., 2000; Gill et al., 2004; Kornbluth and Bhardwaj, 2010). The relationship between DTI and severe TBI outcomes persists even after adjusting for age and admission GCS, two of the strongest prognostic indicators of mortality and functional outcome (Lingsma et al., 2010, van der Naalt et al., 1999).
Poor clinical outcomes were associated with acute global reductions in the averages of both λ‖ and ADC. While the association between global white matter FA averages and clinical outcomes did not reach statistical significance, the CV did exhibit a strong association with clinical outcomes. The CV appears to be a powerful and sensitive summary measure of DTI alterations in TBI. Investigation of ADC as a trauma biomarker have been mixed, with trauma being associated with increased ADC (Bendlin et al., 2008; Kumar et al., 2009; Lipton et al., 2008; Salmond et al., 2006; Shanmugnathan et al., 2004), decreased ADC (Huisman et al., 2004), or no change in ADC relative to controls (Arfanakis et al., 2002). This heterogeneity may be due to differences in the anatomical regions sampled, quantitative methodological differences, or temporal trends in ADC following TBI, as seen in various animal studies (MacDonald et al., 2007a,2007b).
Similar investigations into whole-brain DTI have also found relationships between DTI parameters and trauma. Benson and colleagues (2007) have reported associations between the DTI metrics and neurological status and post-traumatic amnesia. In particular, they found higher-order moments of the FA distribution to be better indicators of injury than the whole-brain FA mean.
Several investigators have reported regional ADC in different white matter regions following trauma, with mixed results. Some investigators have found increased ADC in TBI patients relative to controls (Bendlin et al., 2008; Kumar et al., 2009; Lipton et al., 2008; Salmond et al., 2006; Shanmugnathan et al., 2004), while others have found either decreased ADC in patients (Huisman et al., 2004), or no relationship to injury status (Arfanakis et al., 2002). Animal studies may shed some light on these mixed results, for which the relationship between ADC and trauma has been shown to be highly time-dependent, with decreased diffusivity in the acute phase, and increased diffusivity in the chronic phase (MacDonald et al., 2007a). Significant differences in data analysis methodologies across the literature may also account for some of the mixed results, with some investigators using voxel-based morphometry (Lipton et al., 2008; Salmond et al., 2006), others sampling normal-appearing white matter (Arfanakis et al., 2002), and still others measuring pre-specified regions regardless of appearance on conventional MRI (Bendlin et al., 2008; Kumar et al., 2009).
In our study, the association between the average FA of the whole-brain white matter and discharge neurological status did not reach statistical significance. However, regional FA measures in the corpus callosum demonstrated greater sensitivity. In the corpus callosum, average axial diffusivity and average FA were significantly related to clinical outcomes, with worse outcomes associated with increasing decrements in these parameters. The relationship between decreased FA and trauma severity in several regions of the brain including the corpus callosum has been reiterated by several other investigations of TBI, regardless of injury severity and the time since injury (Bendlin et al., 2008; Greenberg et al., 2008; Huisman et al., 2004; Kumar et al., 2009; Rutgers et al., 2008a; Sidaros et al., 2008; Sugiyama et al., 2009; Tollard et al., 2009), suggesting that changes in the fractional anisotropy within the corpus callosum are both a sensitive and stable marker of injury in TBI. Some investigators found relationships between changes in FA and outcome status in severe TBI patients (Bendlin et al., 2008; Sidaros et al., 2008; Tollard et al., 2009), while at least one study found no association between FA changes and either the post-resuscitation GCS or the GOS (Newcombe et al., 2007). Controlled cortical impact (CCI) animal models of TBI help elucidate the pathological mechanisms underlying DTI changes. Mac Donald and colleagues (2007a) observed acute and subacute (4 h to 4 days post-injury) reductions in ADC, FA, and axial diffusivity, in the cortex ipsilateral and contralateral to the lesion, which were associated with primary axonal injury. Subacute (1 week to 1 month post-injury) increases in ADC and axial diffusivity were associated with edema, demyelination, and gliosis. Reduced ADC and axial diffusivity at the acute stage following CCI were also reported by Xu and associates (2011), as well as by Zhuo and colleagues (2012). However, they also observed significant changes in axial diffusivity at the very acute stage, and a normalization of DTI changes toward subacute stages. In yet another CCI study, by Mac Donald and co-workers (2007b), reduced relative anisotropy and axial diffusivity were seen within 4–6 h of injury, while T2 relaxation time, ADC, and radial diffusivity were not significantly altered. Taken together, these studies support the notion that changes in FA and ADC, which are primarily driven by changes in axial diffusivity, may be most indicative of the extent of axonal injury during the initial hours following injury. Since the majority of our study group was imaged within 5 days of injury (acute to subacute stage), it is likely that our findings of reduced axial diffusivity are reflective of a combination of primary axonal injury and the early effects of secondary injury (Mac Donald et al., 2007a), and that the extent of this axonal injury could be predictive of patient outcome.
Few other studies have focused on the utility of DTI measures in evaluating severe TBI. In concordance with our study, Newcombe and associates (2007) found decreased FA in the white matter among 33 severely injured TBI patients who required mechanical ventilation. In contrast to our study, however, they found increased ADC relative to control subjects, and the changes in FA and ADC were driven by changes in radial diffusivity, not axial diffusivity as in the present study. They also found no association with either the post-resuscitation GCS or GOS and the DTI parameters. Bendlin and colleagues (2008) observed a progressive decrease in FA, an increase in mean diffusivity, and a reduction in brain volume, over 1 year, although significant improvements were observed on neuropsychological testing. However, this study only addressed the longitudinal DTI changes seen in gray and white matter, and did not address patient outcomes. Perlbarg and colleagues (2009) investigated 30 TBI patients with varying injury severity and observed lower average FA in the posterior limb of the internal capsule and posterior corpus callosum among the patients with poor GOS scores 1 year after injury, and found that DTI parameters offered prognostic value above and beyond clinical measures. Sidaros and co-workers (2008) observed a reduced axial diffusivity and increased radial diffusivity among 30 severe TBI patients in many regions, including the corpus callosum and the internal capsule, which appeared to normalize by 12 months among patients with good GOS scores at 1 year after injury. Tollard and associates (2009) observed significantly reduced FA in several regions among 43 severe TBI patients with poor outcomes, compared to those who had favorable outcomes at 1 year based on the GOSE scale, although the FA was still reduced among the favorable outcome group compared to normal control subjects.
While most prior research in TBI compares TBI patients to healthy volunteers, the present study investigated the association between DTI values in the acute phase of injury and the natural history of severe TBI. A group of mild TBI patients with negative CT and MRI scans were included to provide context for the DTI values of severe TBI patients, and these patients were not used in any models of patient outcomes. This should be taken into consideration when comparing our results with prior research. Other differences between the present study and prior research include time of the MRI scan from the time of injury, and the method of outcome classification. Despite these differences, there appears to be a consensus among these studies and ours, that changes in the corpus callosum may be predictive of outcomes from severe TBI. (Newcombe et al., 2007; Perlbarg et al., 2009; Rutgers et al., 2008b).
The development of accurate diagnostic and prognostic markers in TBI is an important step in developing effective treatment and rehabilitation strategies (Haacke et al., 2010; Moppett, 2007; Saatman et al., 2008). Diffusion tensor MRI appears to provide several biomarkers that relate to the physiological conditions of the white matter, which are correlated with existing clinical measures, yet provide more information about a patient's discharge status. Furthermore, these markers are often obtained within a week of injury, and their measurement is not affected by intoxication, swelling around the eyes, medical interventions prior to admission, or other factors that may limit the usefulness of the GCS score. DTI also has been shown to detect abnormalities that are not visualized or appreciated on conventional imaging. Neurological status was related to decreases in the mean DTI measures, in particular the axial diffusivity and the average ADC in the whole-brain white matter, and in the body of the corpus callosum in the subacute stage of the injury. These changes were accompanied by significant increases in their CV with injury severity, and were strongly associated with patient outcomes, even after adjusting for other prognostic factors, including age and admission GCS score. The quantitative protocol used in this study could easily be translated to the clinical setting, and the regional measures could help extend the usefulness of DTI to patients whose injuries prohibit the use of whole-brain segmentation algorithms to separate gray and white matter. The usefulness of these DTI parameters as prognostic markers needs to be further extended to longitudinal studies relating DTI findings to long-term biological, psychological, and social outcomes.
Since our patients were retrospectively evaluated in the acute setting at discharge to TBI rehabilitation, rehabilitation outcome measures such as the GOS were not available (Lipton et al., 2008). While the GCS score on admission to rehabilitation is associated with functional recovery (Avesani et al., 2011), further research is necessary to associate acute DTI with long-term functional outcomes. Without established scoring criteria for MRI, analogous to the Marshall classification for CT (Marshall et al., 1991), it is difficult to compare the prognostic value of DTI to conventional imaging. While our study involved only patients with head injuries, future studies should involve healthy volunteers to determine an absolute scale between normal human variability and the range of DTI values seen across the spectrum of TBI.
Our study investigated severe TBI patients in the acute setting, who are under-represented in the literature. Patients were evaluated with DTI early in the course of injury using a simple whole-brain and ROI methodology that could readily be translated for clinical use. Prognostic models showed that axial diffusivity and FA provided prognostic information about patient outcomes in severe TBI, which likely reflects the degree of underlying axonal injury. The CV of these DTI measures is a powerful summary measure, capturing both decreases in mean values and increases in variance within ROIs.
Our study included patients in the age range of 18–83 years. DTI parameters are known to be affected by age. The results of this study demonstrate that the DTI parameters provide significant prognostic value, even after adjusting for age. Further, a re-analysis of the data (not shown) from patients sampled from a more stringent subset of patients in the age range of 18–65 years, who were scanned within 5 days post-injury, essentially provided the same results. Once again these observations suggest that DTI parameters could play a significant role in the evaluation of the patient at the acute stage, while providing valuable prognostic information.
The results of this study have to be taken in the context of its limitations. Due to the retrospective nature of the study, we were limited to data that were collected with only 12 diffusion-encoding gradient directions per the existing clinical protocol. It is well known that variability in DTI parameters is reduced if larger numbers of diffusion directions are used (Papadakis et al., 2000). While we do not think this had a large effect on the outcome of our results, future studies should use more diffusion directions to minimize any variability in DTI parameter estimation.
DTI may prove to be a valuable complement to conventional imaging, and may help us better appreciate and quantify pathology. Unfortunately, no widely-validated MRI scoring system for TBI severity currently exists. Without a healthy control population, it is difficult to compare DTI findings near lesions visualized on conventional imaging, as occult pathology may be present in the homologous region contralateral to the lesion. This study only included patients during their acute hospitalization for TBI. The GOSE is typically used for measuring clinical outcomes in TBI. It measures a patient's independence in and outside the home, as well as participation in social and leisure activities, which only apply to outpatient or rehabilitation settings (Wilson et al., 1998). Since not all patients attended affiliated rehabilitation facilities, these data could not be collected for all individuals. In spite of this fact, neurological status on admission to acute TBI rehabilitation, as represented by the discharge GCS score, is a strong prognostic marker of functional recovery (Avesani et al., 2011). Future research is necessary to see if these results generalize to outcomes in the subacute and chronic phases of TBI, which are measured by the GOSE and other measures of cognitive, social, and occupational recovery.
However, the above limitations should also be viewed in the context of several key aspects of the study. First, while other studies have investigated the possibility of using DTI to quantify brain injury after trauma, many of these studies are limited by long and highly variable intervals between injury and imaging, sometimes spanning the acute, subacute, and chronic phases of injury. The vast majority of our sample was imaged within 5 days of injury, measuring the acute effects of severe TBI. Second, while mild TBI has been relatively well studied, we focused on severe TBI patients, which are underrepresented in the DTI literature. Third, most other studies examine FA or ADC, and do not consider radial or axial diffusivity, the latter of which appears to be a promising marker of injury. Fourth, while other studies have looked at averages of DTI parameters, we found that the variability and CV may be even stronger indicators of injury severity. Finally, our study looked at both regional and global changes, the combination of which may better depict the diffuse and heterogeneous nature of TBI.
Conclusion
Our study demonstrated that DTI parameters at the whole-brain level and regional level can provide prognostic information about the discharge status of a patient, while circumventing many problems associated with currently used clinical measures, including the GCS. The relationship between DTI and discharge neurological status remained significant, even after adjusting for two of the strongest prognostic factors in TBI. Axial diffusivity appears to provide the most prognostic information about outcome status, on both regional and global scales. The CV captures information about both the mean and the variability in the data, making it a parsimonious summary measure for DTI values. While these results are promising, prospective longitudinal studies are necessary to validate these findings.
Footnotes
Acknowledgment
The authors thank Brigitte Pocta for reviewing the manuscript. This work was partly supported by a grant from the U.S. Army (W81XWH-08-1-0725).
Author Disclosure Statement
No competing financial interests exist.