
Abstract
This article presents a new method of cranioplasty in which polypropylene polyester knitwear was used as the filling material. The basis for prosthesis shaping was a three-dimensional model of the defect made according to the patient's CT scans. Previously, such material has never been a subject of computer-aided design and computer-aided manufacturing (CAD/CAM) individual forming. The process of the prosthesis design included CT bone scans and mold preparation for each patient. Such prostheses were implanted in 48 patients with cranial defects. The total number of prostheses applied was 51. The follow-up time was at least 6 months up to 36 months. The group of treated patients is described here, and sample pictures are shown to illustrate the results. The smallest defect had a size of 15 cm2; the biggest, 178 cm2. The coverage and the aesthetic results were very good in all cases. Two patients had postoperative complications. The cranioplastic solution described here is a valuable addition to the existing reconstructive methods, because of the low cost of the implant, the ease of its adjustment to the shape of the defect, and the short time of preparation.
Introduction
T
Such an approach was used in clinical practice with different materials. The oldest trials were conducted with titanium and acrylic resin (Cabraja et al., 2009; Lee et al., 2009), and more recent ones were conducted with porous polyethylene (Suwanprateeb et al., 2011). Previously, however, three-dimensional (3D) modeling and computer-aided forming were not applied to polypropylene polyester knitwear. Despite several trials having been undertaken throughout the last decade, there was no cheap or quick way to customize the prosthesis for an individual patient. On the other hand, the knitwear material seemed to be a good alternative to other cranioplastic materials because of its inherent properties. Knitwear consists of biologically inert polypropylene polyester threads. Its mechanical and thermal conduction properties (after thermal stabilization) are similar to bone.
Its minimal bending strength is 6–10 daN with surface weight 1900±290 g/m2 (Gawlik and Balcerzak, 1980).
It has a porous structure allowing for free migration of tissue fluids, which decreases the risk of any collection causing inflammation (Czepko and Kwinta, 2005). The polypropylene compound with low specific weight prevents water absorption. Polyester compound has high mechanical resistance. Several weeks after the implantation is performed with that substance, the whole surface of the prosthesis is joined to the surroundings with newly formed connective tissues anchored inside the implant structure, and the material is completely radiolucent, facilitating control imaging (see Fig. 1) (Andrzejak et al., 2005; Andrzejczak et al., 1992; Bani et al., 1991; Kotwica et al., 1991).
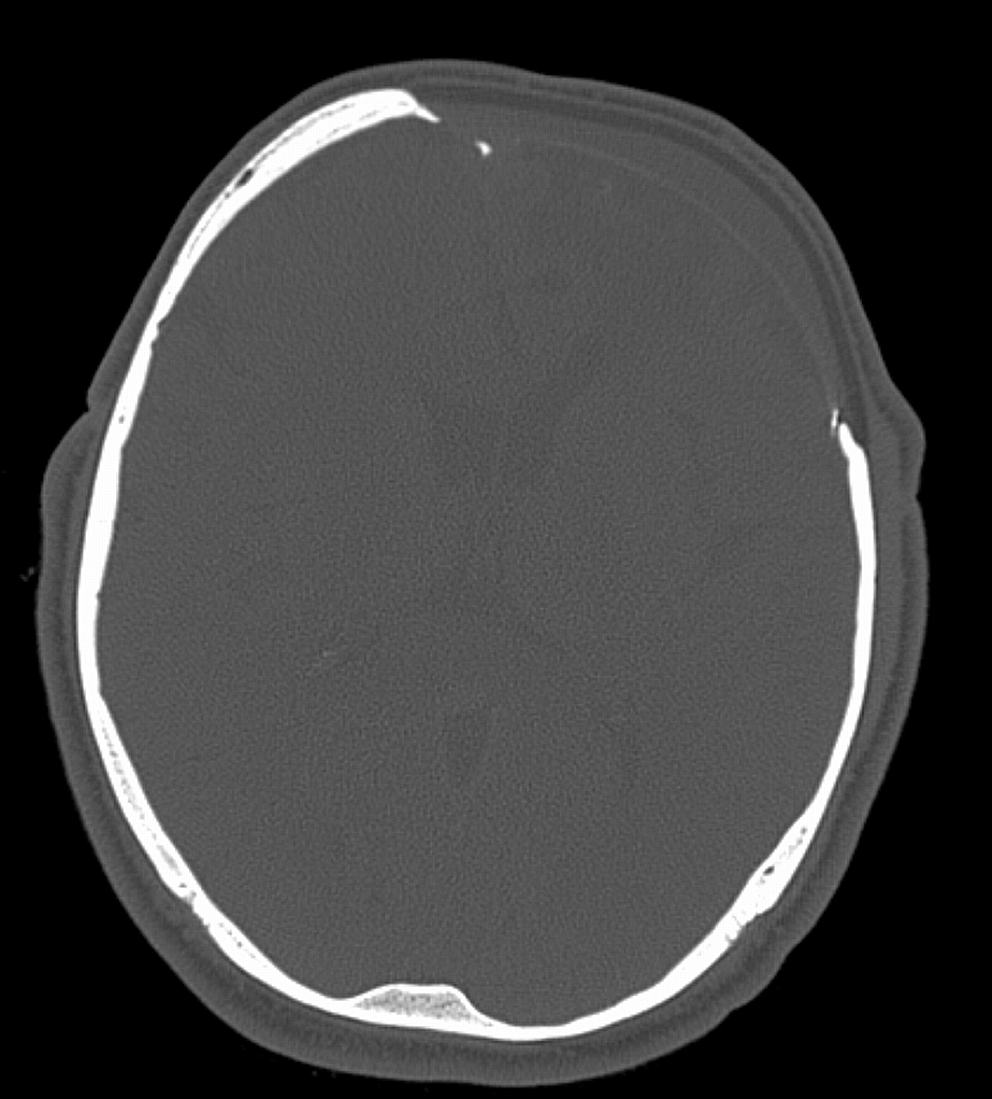
Bone scan of the prosthesis after implantation. Constant thickness and radiolucency is visible.
Methods
In 2008, a new technique of polypropylene-polyester knitwear forming was finally developed (Kasprzak et al., 2011). The method involves a CT scan conducted before the planned operation with a protocol similar to that used for neuronavigation purposes. This scan can be performed in any scanner, including older devices. The CT scans are the basis for a 3D cranial model, which is then used to prepare a proper mold to form the knitwear. This technique makes it possible to produce a customized prosthesis for an individual patient (see Fig. 2). The resulting implants have constant thickness (4 mm), with hardness similar to bone. The external curvature recreates the required shape of the reconstructed part of the skull. Standard time of preparation is 2 to 3 weeks between the CT scan, after which the prosthesis ready to use. The total number of applications of such prostheses reached 73 in three neurosurgical departments: in Lodz, Gryfice, and Krakow, and in a traumatology center in Wroclaw. We analyzed the patient group for which the follow-up time was at least 6 months. This group consisted of 48 patients, 15 women and 33 men, 18–62 years of age. All patients were independent, although one female patient was using a wheelchair after meningioma removal. All patients were fully aware of the need for reconstructive operation. The number of cranioplasties performed in these patients was 50. Two patients had bilateral craniectomies. One patient had two prostheses for one defect – before the operation it was known that the defect would be substantially enlarged during the surgery, so two prostheses were prepared – one for the existing defect and the second implant for the planned bone resection. The cranioplasties were performed in 14 patients after operations for intracranial aneurysm, in 6 patients for benign neoplasms, and in 28 patients for post-traumatic defects. Departments in Gryfice, Krakow, and Wroclaw limited the use of prostheses only to post-traumatic cases and large defects. In Lodz other cases were also treated, especially after decompressions in vascular procedure cases (seven patients with craniectomy during aneurysm surgery and seven patients with delayed bone flap removal after aneurysm operation), five patients with meningioma, and one with low grade glioma. In all post-traumatic and vascular decompression cases, duraplasty was performed with autologous material. Wherever it was possible, the material was temporal muscle, however in three cases it was necessary to get a distant autotransplant. The authors tried to avoid the use of any foreign material in the neighborhood of the prosthesis. In all meningioma cases, dura removal was necessary, and closing of it was performed only with autologous material. Low-grade glioma cases required craniectomy after postoperative brain swelling, so they were treated as post-traumatic cases, with duraplasty.

Prosthesis before implantation. Knitted structure is visible.
The shortest time between craniectomy and cranioplasty was 3 months, and the longest was 2 years.
The surgical procedures were performed in a classic way, involving dissecting of the layers above the defect and fixing the prosthesis with bone stitches or titanium clamps. The skin was closed in two ways: with continuous monofilament suture (in 10 cases, smaller defects), or with self-adopting single sutures. In all cases, the authors used the drainage of subgaleal space; fluid permeability of the prosthesis excluded the necessity of the epidural one. Drains were removed within 24 h after cranioplasty.
Antibiotic protocol was not uniform. In Lodz and Wroclaw, patients had prophylactic antibiotics given for 1 week after surgery. In Gryfice, no antibiotic was used. In Krakow, antibiotics were administered only for 2 days after implantation.
In six craniectomy cases, frontal sinuses were involved, but only in two cases it was necessary to reopen them during cranioplasty. The third case in which sinuses were opened, was a patient mentioned earlier, for whom, during cranioplasty, it was necessary to remove the tumor and to perform additional craniectomy involving the frontal region. In all cases in which nasal mucosa was present, it was removed, and closing was performed only with autologous material (muscle).
All patients were followed up prospectively on a uniform schedule. This schedule consisted of observation during the stay in the hospital for the first week after implantation, later control visits at open clinic at 1 month after surgery, and every 6 months subsequently. Fifteen patients were followed for>24 months, 11 patients for>12 months, and 22 patients for>6 months. The smallest prosthesis had an area of 15 cm2 for craniectomy after aneurysm surgery, and the largest single prosthesis had an area of 158 cm2 and was implanted in a post-traumatic defect. The largest single defect treated was 171 cm2 and was treated with 2 prostheses in a meningioma operation. Two prostheses were used because the operation itself was performed as a two-stage procedure. The first stage involved meningioma removal with adjacent bone. The bone cut was planned according to the first prosthesis outline (in the frontal area). In the second stage, the prosthesis was implanted in the defect area that had existed preoperatively. Both prostheses were joined with monofilament nonresorbable stitches.
The aesthetic results were ranked through patient self assessment in all cases, and through the assessment of the curvature of the skull in CT scans in those patients in whom control examinations were performed. Postoperative CT was performed in 16 cases.
Results
In all 48 patients, the coverage and aesthetic aspect was ranked as very good. In all cases the healthy shape of the skull was restored. There is no known objective criterion for performing such an evaluation, but patients' self assessment was the most important. In those cases (16) in which CT scan was performed, the improvement of the skull exterior was visible. Curvature of the missing bone part was correct in all fillings. The prosthesis outline was good, although in 18 cases some minor border cuts were necessary during the procedure. All implants were well adjusted to the particular defect and well aligned with the surrounding tissues. The largest defect was treated with two prostheses and two patients had two defects (and two adequate prostheses). Complications were observed in two cases: one patient revealed a purulent process for an unknown reason 2 months after cranioplasty, which required the immediate removal of the prosthesis. There were no signs of general or local infection until a week before the beginning of the purulent process. Also, there were no indications of any injury in the implant area. Wound culture revealed non-methicillin-resistant Staphylococcus aureus (MRSA) S. aureus. The patient had acne. In the second complicated case, the titanium clamp used to fix the prosthesis was mobilized by a secondary trauma in the operated area. The patient was operated on again, the prosthesis was fixed again with bone sutures, and the patient was followed for 6 months with no additional complications.
Discussion
Computer-aided prosthesis forming gives good shape adjustment of the filling of the operated defect. The production process originating in CT scans can be done preoperatively and off site. Previously used methods in which some dental technicians were employed required the patient's presence during the production process (Kasprzak et al., 1992). The prostheses described in this article give good results even in those cases that are commonly recognized as more difficult to treat, such as where the bone openings reach the eyebrows and forehead, or in very large defects (see Figs. 3 –6). To date, computer-aided machining has been used for tooling of rigid materials such as ceramics, metals, and various plastics (Hoffmann and Sepehrnia, 2005). All such substances have some important limitations. For example, metals have high heat conduction rate, ceramics or acrylics are fragile, and computer-aided design and computer-aided manufacturing (CAD/CAM) forming of all of the abovementioned materials and of porous polyethylene is quite expensive (Gladstone et al., 1995; Kahraman et al., 2003).

Male patient with post-traumatic defect in the frontoparietal region. Prosthesis 3D model, pre- and postoperative picture.

Male patient with post-traumatic defect in parietal region. Prosthesis 3D model, pre- and postoperative picture.

Female patient with bifrontal defect after meningioma operation. Prosthesis 3D model, pre- and postoperative picture.

Male patient with eyebrow post-traumatic defect. Prosthesis 3D model, pre- and postoperative picture.
Some materials mentioned earlier are very hard, which precludes intraoperative shape correction. Newer plastic substances without extreme rigidity such as porous polyethylene, have continuous structure preventing free transmission of body fluids (Cabraja et al., 2009; Chuo et al., 2009), and at the same time they are expensive. The geometry of any cranial prosthesis is described by two features: the curvature and the outline. The curvatures obtained with 3D designing are usually correct, and they were also correct in all cases described here. The outline is a much less certain attribute because of the partial volume effect, a faulty feature of any CT scanning method. In such cases, some intraoperative correction may be necessary. Any adjustment is very difficult in hard or solid implants and much easier in the case of polypropylene-polyester knitwear (such correction was made in 18 of our prostheses). The required cuts were usually performed with surgical scissors without the use of a high speed drill.
Another important property of the knitwear material is its radiolucency, which facilitates the postoperative assessment. Similar prostheses made of ceramics or metals, and also some acrylic implants, are radio-opaque, which can produce artifacts and difficulties in radiological examination. A notable feature of the knitted prosthesis is its constant thickness. Such an implant is formed with 3D techniques but the result is a 2,5D prosthesis. Such prosthesis recreates the missing bone in X and Y axis but in Z dimension – only the external surface. The internal one is the offset of the external. This can be a disadvantage, in particular in cases in which a titanium clamping system is chosen as the method of fixing. When the bone stitches are the method of fixation, however, such constant thickness does not have any influence on prosthesis fitting. Constant thickness is also an advantage when intraoperative prosthesis outline correction is necessary. A 4 mm thick prosthesis is relatively easy to cut to the required contour.
That there was one case in the series in which a two-part prosthesis was used also shows that the knitwear material can be safely joined and healed. Further studies on that issue are necessary because such cases are extremely rare. This confirms the conclusions from animal studies on knitwear (Gawlik and Balcerzak, 1980) and oral reports on the use of such methods in clinical practice. Until now, however, it has never been described in any source known to the authors.
Knitwear has become the material accepted for neurosurgical use in the European Union. However, before the method presented in this article was developed, there had been no inexpensive and quick method of preparation of customized prostheses. The series of cases discussed here demonstrates that the preparation of the mold for implant forming with computer-aided tools gives a good curvature and outline. The prostheses formed in such a manner can be implanted even in more complicated cases. The total cost of the knitwear implant preparation is at least two times lower than for other computer-aided techniques; in cases discussed in this article, the cost did not exceed 1000 € (∼1200 US$) per prosthesis.
Conclusion
The true novelty of the method described in this article is the combination of 3D forming of the prosthetic implant and the knitwear material. There were other prostheses prepared with CT scanning previously, but these were never made of polypropylene polyester knitwear. There were standard implants made of such knitwear but they were prepared by the producer as a part of a sphere, and they could not be adjusted to the needs of a given cranial defect. This article shows the results the authors obtained when knitwear material and CT-dependent forming were combined together. Such a method of preoperative prosthesis preparation is useful in clinical practice. It can be assessed as a good alternative to other methods of customized prosthesis manufacturing in which hard or solid materials are used. It reduces the time of surgery and gives good coverage and aesthetic results. It is easier to use than any other prosthesis with intraoperative forming, because the surgeon does not need to spend time on prosthesis creation during the surgery. The implant can be fixed with bone stitches, which results in a minor additional cost; it is not necessary to use more expensive titanium clamps. The production process is fairly quick; not more>3 weeks. And last but not least, such a prosthesis is much cheaper than other prostheses prepared with CAD/CAM techniques.
Footnotes
Author Disclosure Statement
No competing financial interests exist.