
Abstract
Early prediction of hand function is crucial for efficient rehabilitation of cervical spinal cord injury (cSCI). This study investigated correlations between ulnar somatosensory evoked potentials (ulnar SSEPs) and functional outcome of hand function following acute traumatic cervical cord injury. Neurological assessment of sensory scores and hand function were compared with five ulnar SSEP categories of similar persistence and quality in 365 patients throughout the first year after cSCI. Of the 365 patients, 218 (68%) exhibited ulnar SSEP potentials at any one stage during the year, and in 147 patients (40.3%) ulnar SSEPs were obtainable at every assessment stage. While ulnar SSEP latency and amplitude assessments remained largely unchanged over time in the majority of patients, hand function improved remarkably during the first year following cSCI. One year outcome of hand function was predetermined by ulnar SSEP category due to distinct differences in the ulnar SSEP parameters. Additionally, an early prognostic group allocation by ulnar SSEP criteria at the first assessment stage within 4 weeks after spinal trauma allowed reliable prediction of hand function outcome after 1 year. We conclude that early assessment of ulnar SSEP as a non-invasive and objective neurophysiological test is a valuable marker of prospective hand function and independence 1 year after cSCI. This could be most relevant for planning neurorehabilitation, and in prospective clinical SCI trials.
Introduction
S
Methods
The “European Multicenter Study on Human Spinal Cord Injury” (
Patient selection
For this study, we selected 365 patients with traumatic tetraplegia and two or more completed ulnar SSEP measurements from the database. All patients included had been assessed neurologically according to the International Standards for Neurologic Classification in Spinal Cord Injury (ISNCSCI) (American Spinal Injury Association, 2000; Marino et al., 2003) in one of the first two stages, and they had their last assessment completed before December 2008. Patients were included in this study if their neurological level of lesion (according to the International Standards) (Marino et al., 2003), determined at the first available evaluation was between the second cervical (C2) and first thoracic (T1) segment. The term cSCI refers to cervical spinal cord injury, as thoracic lesions below T1 were excluded in this study about ulnar SSEP and hand function.
Parameters of interest
Ulnar somatosensory evoked potentials (ulnar SSEPs)
The ulnar SSEP measurements were conducted according to the guidelines of the “German Society for Clinical Electrophysiology and Medical Imaging” (Buchner et al., 2003). The ulnar nerve was stimulated at the wrist, and cortical potentials (N20/P25 complex) were recorded contralaterally at CP3 and CP4 (active) against Fpz (reference), according to the International 10/20 system for EEG electrode placement (Niedermeyer and Lopes da Silva, 2004). Impedance was maintained below 5 kΩ. Stimulus intensity was adjusted to produce a clear muscular response (1.5 times motor threshold, max. 40 mA) in order to assess all sensory fibers. N20 latencies and amplitudes of the N20/P25 complex were manually detected and used for statistical analyses.
American Spinal Injury Association (ASIA) measures
For comparisons of ulnar SSEPs with neurological deficits we focused our analyses on ASIA light touch scores (ASIA LT), as they correspond to SSEP measures and dorsal column function (American Spinal Injury Association, 2002; Beric et al., 1987). The mean of segmental LT scores caudal to the lesion level was used for all analyses. As a measure of neurological severity of injury, we used the ASIA Impairment Scale (AIS). The AIS classifies patients according to the degree of completeness of their injury.
Spinal Cord Independence Measure (SCIM)
The functional recovery of activities of daily living was monitored by the Spinal Cord Independence Measure (SCIM) (Catz et al., 2001,2007). The SCIM includes several sub-scores pertaining to self-care, respiration, and sphincter management and mobility. To examine motor function of hands and arms we chose the item “feeding” (sub-score 0–4) from the total self-care score (grooming, dressing, bathing, and feeding). This item correlates significantly with the total self-care score (p<0.001), producing a coefficient of 0.95. A score of zero needs parenteral, gastrostomy, or fully-assisted oral feeding; 1 needs partial assistance for eating, drinking, or for using adaptive devices; 2 eats independently but needs assistance for cutting food, pouring, or opening containers; 3 eats independently and needs adaptive devices; and 4 eats and drinks independently without adaptive devices. SCIM versions II and III used within the EMSCI database were combined in the present evaluation, as these don't differ in this item. Even though dorsal column function represents a part of the sensory system, a motor function test was of interest because SSEPs are known to correlate with motor function and recovery (e.g., ambulatory capacity) (Curt and Dietz 1997,1999).
Ulnar SSEPs and ASIA LT were assessed and analyzed for both body sides separately. However, as differences between the right and the left limb were not significant, we only report analyses and statistics from the right side.
Statistical analysis
Descriptive statistics
The sample data were allocated according to the presence and persistence of ulnar SSEPs, resulting in a subdivision of five groups as was previously described (Spiess et al., 2008). Abolished ulnar SSEPs (aSSEPs) remained abolished in all assessment stages; recurring ulnar SSEPs (rSSEPs) were initially abolished but recurred consistently in follow-up recordings; inconsistent ulnar SSEPs (iSSEPs) were inconsistently recordable or lost throughout follow-up; and mild and significantly deteriorated ulnar SSEPs (mdSSEPs and sdSSEPs) were recordable in all stages. Ulnar SSEPs were considered significantly deteriorated if latency was prolonged (sdSSEP) by more than one standard deviation (SD=0.82 msec) above the normal latency range (according to body height-dependent normative values of the University Hospital Balgrist, L=0.1093 h + 3.85, where L indicates latency in milliseconds, and h is body height in centimeters). An ulnar SSEP with either normal or just slightly delayed latency often presented a distorted configuration or low amplitude. Therefore, this group was termed mildly deteriorated (mdSSEP).
Linear mixed models (LMM)
To estimate changes over time in our parameters, we used a linear mixed model (LMM) approach for our analysis to adequately treat the problem of missing values (mean amount of missing values 26.0%, SD 13.0%) (Piepho et al., 2003). The models included the intercept and subject as random factors, and assessment stage as a fixed effect. A value of p<0.05 was regarded as significant, while p<0.1 was regarded as a trend. Our analyses were performed with SPSS 14.0 and PASW Statistics 17.
Results
Patient demographics
The average age of the patients included was 46.2±19.3 (SD) years, with an average body height of 175.2±9.3 (SD) cm, and 76.4% of the subjects were male. According to the international standards, 35.6% were classified as AIS A, 14.5% as AIS B, 20% as AIS C, and 29.6% as AIS D, in the first available of the first two stages (2 or 4 weeks post-cSCI). One patient was not testable in a few segments and a differentiation between AIS C and D was not possible in those stages. Therefore he was excluded from further analysis.
Group allocation
Ulnar SSEPs were first categorized in five groups considering all stages to learn about their time course during the first year following cSCI. The group allocation is illustrated in Figure 1. In the rSSEP group, 39 of 57 (68.4%) recordings were delayed. Of all 57 rSSEPs, 12 (21.1%) recurred at stage 2 (after 4 weeks), 23 (40.4%) at stage 3 (after 3 months), 12 (21.1%) at stage 4 (after 6 months), and 10 (17.5%) at stage 5 (after 12 months). The mean-time to recur after cSCI was 4.8 months. Of the 44 patients with iSSEPs, 22 (50%) showed normal or slightly delayed latencies when a potential was recordable, and in 26 (59.1%) a first SSEP was recordable for the initial assessments. Within the group of iSSEPs, 9 out of 24 (37.5%) were absent at stage 1, 14 out of 38 (36.8%) at stage 2, 19 out of 36 (52.8%) at stage 3, 15 out of 30 (50.0%) at stage 4, and 15 out of 30 (50.0%) at stage 5.
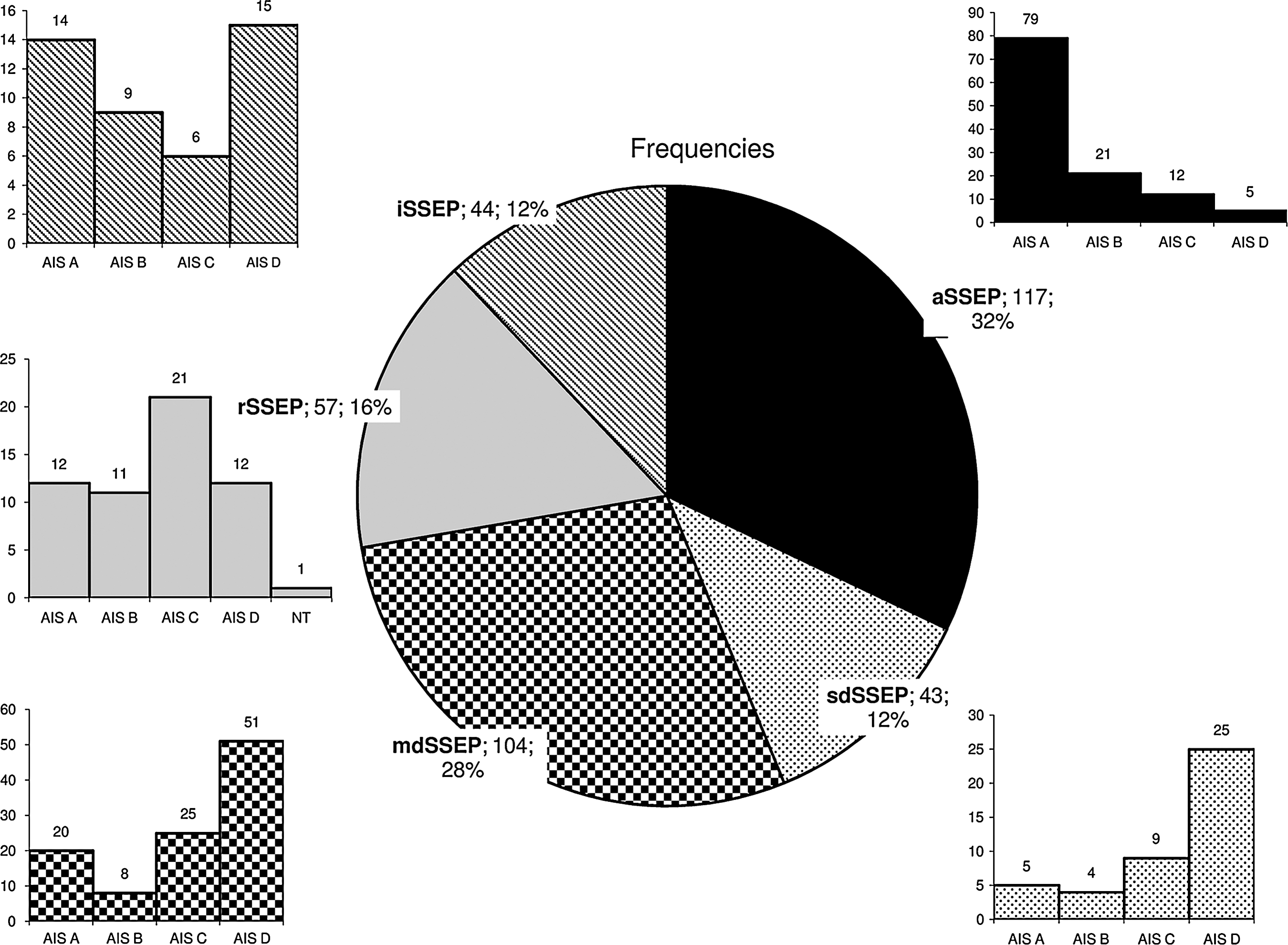
ASIA Impairment Scale (AIS) distribution within the different somatosensory evoked potential (SSEP) groups (NT, not testable; aSSEP, abolished SSEP; sdSSEP, significantly deteriorated SSEP; mdSSEP, mildly deteriorated SSEP; rSSEP, recurring SSEP; iSSEP, inconsistent SSEP; ASIA, American Spinal Injury Association).
A simplified stratification was then used to calculate three SSEP categories (iaSSEPs, initially abolished SSEPs; imdSSEPs, initially mildly deteriorated SSEPs; isdSSEPs, initially severely deteriorated SSEPs) within 4 weeks after trauma to establish a predictive account of initial electrophysiological ulnar SSEP testing for hand function outcome.
AIS distribution according to ulnar SSEP grouping
In the mdSSEP and sdSSEP groups, 76 (51.7%) of the subjects were AIS D at the first assessed stage. In the aSSEP group, 5 (4.3%) of subjects were AIS D, while 12 (10.3%) were AIS C, 21 (17.9%) AIS B, and 79 (67.5%) were AIS A. In the rSSEP group, 12 (21.1%) were AIS D, while 21 (36.8%) were AIS C, 11 (19.3%) were AIS B, and 12 (21.1%) were AIS A. One patient could not be assessed in either of the first two stages. In the iSSEP group, 15 (34.1%) of subjects were AIS D, while 6 (13.6%) were AIS C, 9 (20.5%) were AIS B, and 14 (31.8%) were AIS A.
Latencies and amplitudes of ulnar SSEP
Due to the limited availability of data, time effects were only evaluated for two of the five groups (mdSSEP and sdSSEP; Table 1 and Fig. 2) (main effects not shown in the tables; error bars in the figures represent 95% confidence intervals). Latencies of ulnar SSEPs were significantly reduced over time (main effect of stage F=5.3, df: 387.2, p<0.001). Patients of the mdSSEP group showed significantly shorter latencies compared to the sdSSEP group (main effect of group F=116.3, df: 150.3, p<0.001). A significant group×stage interaction (F=6.6, df: 387.2, p<0.001) indicated that a change of latencies over time depended on group allocation. Post-hoc analysis for each group revealed a significant reduction in latencies over time for sdSSEPs (F=4.2, df: 118.2, p<0.01), and a trend toward a slight increase in latency over time for mdSSEPs (F=2.1, df: 268.4, p<0.1).

Evolution of ulnar SSEP latencies of 43 patients with significantly deteriorated SSEPs (sdSSEP), and 104 patients with mildly deteriorated SSEPs (mdSSEP). Error bars represent 95% confidence intervals (SSEP, somatosensory evoked potential).
aSSEP, abolished SSEP (117 patients); sdSSEP, significantly deteriorated SSEP (43 patients); mdSSEP, mildly deteriorated SSEP (104 patients); rSSEP, recurring SSEP (57 patients); iSSEP, inconsistent SSEP (44 patients); SSEP, somatosensory evoked potential; ASIA LT score, American Spinal Injury Association light touch score; SE, standard error.
For SSEP amplitudes, there was a trend toward an amplitude increase at late stages (F=2.2, df: 379.6, p<0.1), but no main effect of group or group×stage interaction (Table 1 and Fig. 3).
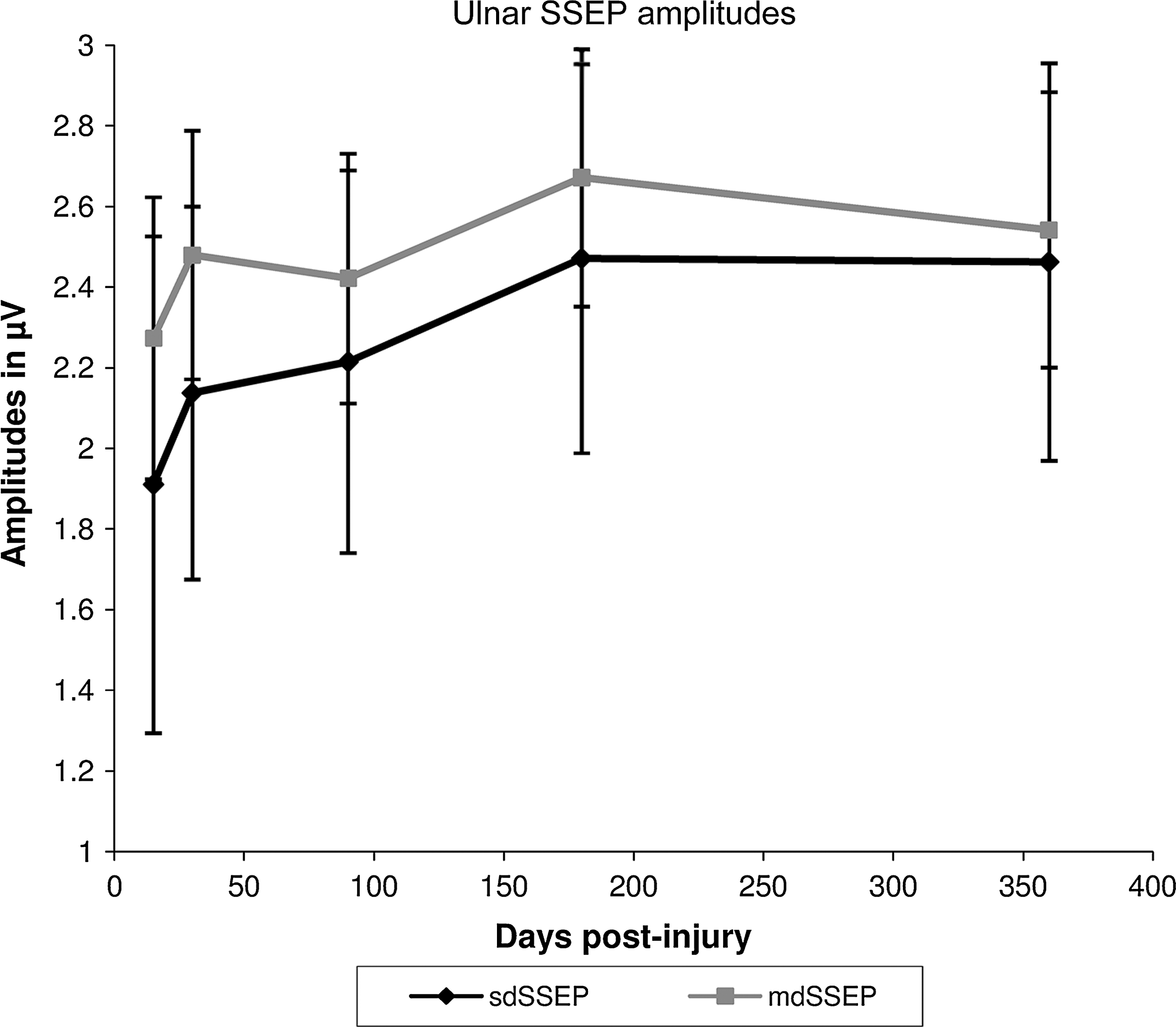
Evolution of ulnar SSEP amplitudes of 43 patients with significantly deteriorated SSEPs (sdSSEP), and 104 patients with mildly deteriorated SSEPs (mdSSEP). Error bars represent 95% confidence intervals (SSEP, somatosensory evoked potential).
ASIA LT score
ASIA LT sensory scores increased slightly during the first year after cSCI (main effect of stage F=35.5, df: 1053.2, p<0.001; Table 1, Fig. 4). Furthermore, there was a significant main effect of group (F=42.8, df: 359.5, p<0.001), for which the highest LT values were seen in the mdSSEP group, followed by the sdSSEP, rSSEP, iSSEP, and aSSEP groups. No significant differences were found for LT scores between the mdSSEP and sdSSEP, as well as the rSSEP and iSSEP groups. Therefore in a new model, these groups were merged into mdSSEP/sdSSEP and rSSEP/iSSEP groups. This model showed a significant main effect of group (F=38.9, df: 234.6, p<0.001). LT scores were higher in mdSSEP/sdSSEP patients than in rSSEP/iSSEP patients. Both combined groups differed significantly from the aSSEP group, in which the lowest score of all groups was found. There was no significant group×stage interaction for ASIA LT scores in this model.
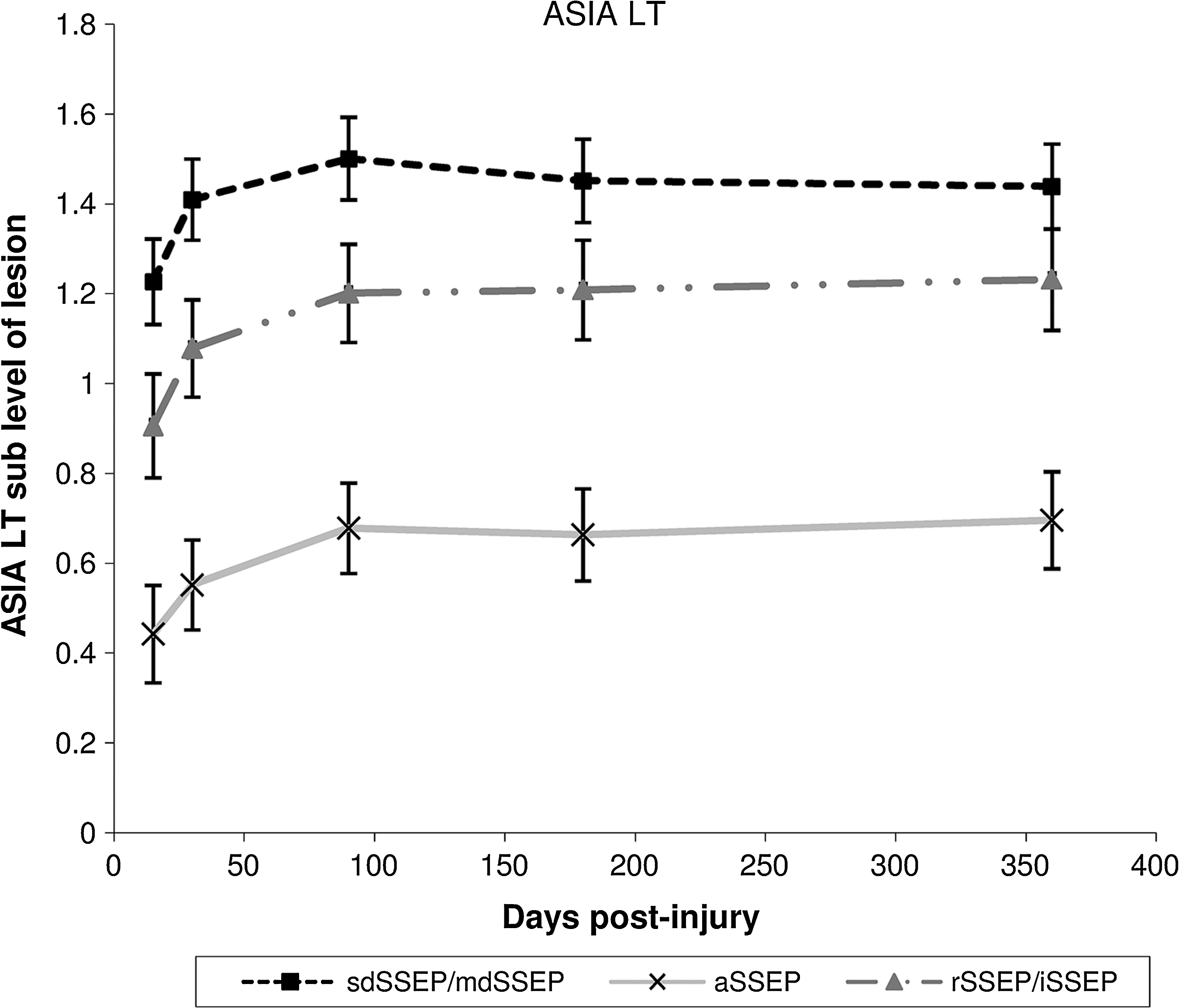
Evolution of American Spinal Injury Association light touch (ASIA LT) scores by sub-level of lesion. Groups that did not differ significantly were merged (sdSSEP, significantly deteriorated SSEP [43 patients]; mdSSEP, mildly deteriorated SSEP [104 patients]; rSSEP, recurring SSEP [57 patients]; iSSEP, inconsistent SSEP [44 patients]; aSSEP abolished SSEP [117 patients]; SSEP, somatosensory evoked potential). Error bars represent 95% confidence intervals.
Hand function detected by SCIM
LMM for SCIM sub-scores revealed significant main effects of stage (F=292.7, df: 1062.1, p<0.001), and group (F=55.6, df: 347.7, p<0.001), as well as a significant group×stage interaction (F=5.6, df: 1060.7, p<0.001; Table 1 and Fig. 5). Because no significant differences between rSSEPs and iSSEPs could be detected, they were combined for the model. The mdSSEP group compared to the sdSSEP group showed a trend toward higher SCIM scores (p<0.1). Group comparison between sdSSEP and rSSEP/iSSEP revealed significantly lower SCIM scores in rSSEP/iSSEP patients (F=9.3, df: 138.6, p<0.01), and rSSEP/iSSEP showed higher scores compared with aSSEP patients (F=48.7, df: 210.2 p<0.001). A group×stage interaction between the rSSEP/iSSEP and aSSEP groups was also shown (F=12.0, df: 650.6 p<0.001).
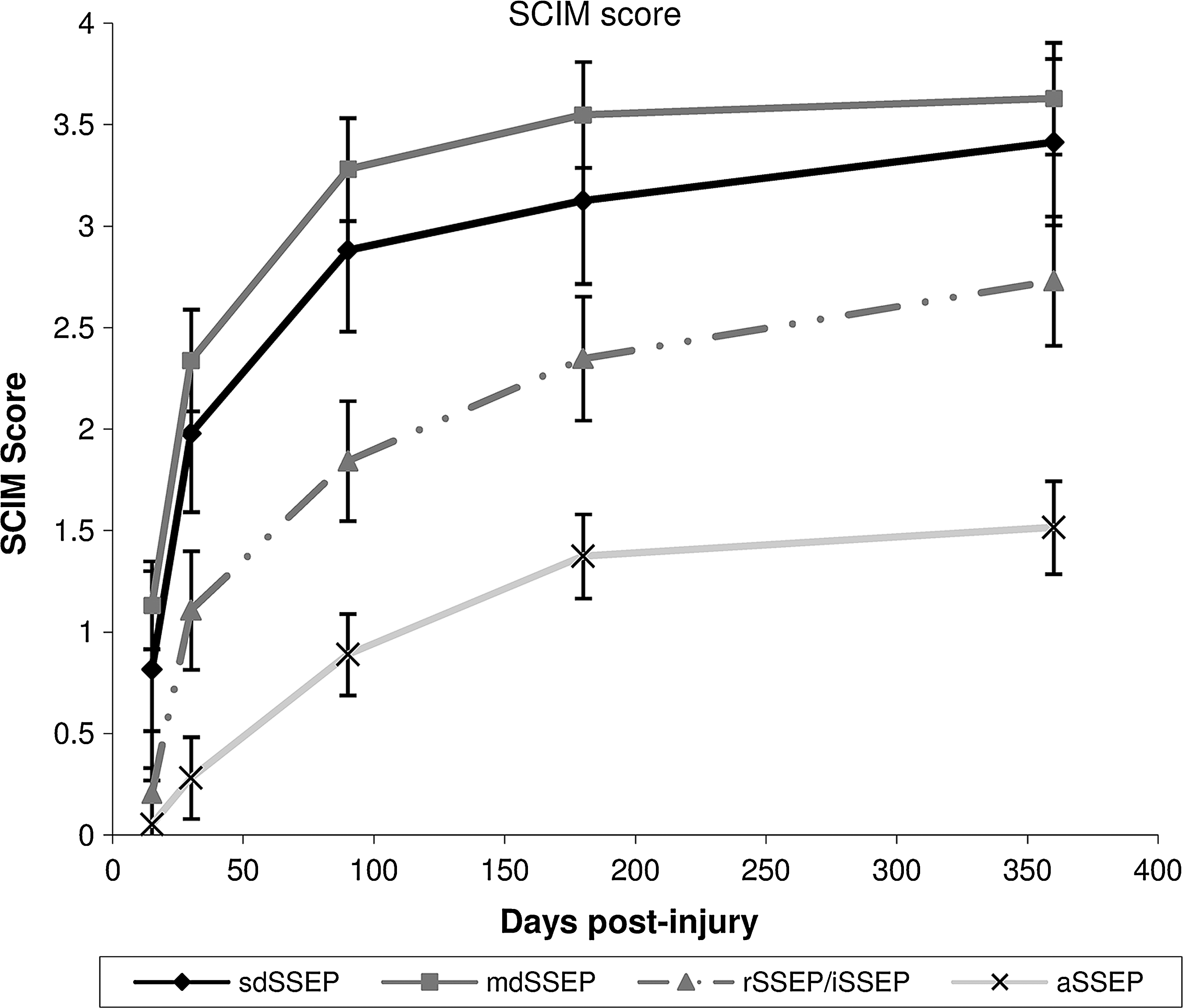
Evolution of Spinal Cord Independence Measure (SCIM) scores. Groups that didn't differ were merged (sdSSEP, significantly deteriorated SSEP [43 patients]; mdSSEP, mildly deteriorated SSEP [104 patients]; rSSEP, recurring SSEP [57 patients]; iSSEP, inconsistent SSEP [44 patients]; aSSEP, abolished SSEP [117 patients]; SSEP, somatosensory evoked potential). Error bars represent 95% confidence intervals.
Prognosis of hand function by ulnar SSEP assessments
In terms of prognosis, it was of interest to assess patient outcomes within the first 4 weeks (stage 1 and 2) by ulnar SSEP assessments with respect to SCIM results 6 and 12 months post-injury (stages 4 and 5). SCIM sub-score values for feeding of 3 and 4 were rated as manually independent. Of 284 cSCI subjects with an available SSEP measurement in stage 1 or 2 (first month), and an available SCIM sub-score in either stage 4 or 5, 175 (61.6%) became manually independent (sub-score SCIM 3 or 4). When assessed within 30 days, 115 of 175 (65.7%) cSCI subjects who eventually became manually independent presented in the isdSSEP or imdSSEP categories. Of 109 cSCI subjects who did not become manually independent (sub-score SCIM 0–2) 84 (77.1%) had no ulnar SSEPs (iaSSEP) initially, while 25 (22.9%) of them had an ulnar SSEP at an early assessment within 4 weeks. The positive predictive value (PPV) was 82.1%. The negative predictive value (NPV) was 58.3% (Pearson chi-square test: p<0.001).
When comparing those patients with initially normal or mildly deteriorated ulnar SSEPs (imdSSEP), to patients showing initially severely deteriorated ulnar SSEPs (isdSSEPs), the SCIM sub-score for feeding at stage 4 (6 months) was significantly lower (p<0.01) for the latter group, while at stage 5 (12 months) it was not significantly different in both groups (p<0.1).
Discussion
This study examined the evolution of ulnar SSEP in order to stratify patients with tetraplegia, and by doing so to predict clinical and functional outcomes 1 year after traumatic cSCI. Ulnar SSEPs offer an objective, quantifiable evaluation of the functional integrity of the posterior spinal column. They require minimal patient participation and are therefore well suited for assessments immediately after injury when numerous factors prevent the patient from actively engaging in clinical testing. Therefore, the use of ulnar SSEPs to predict hand function after 1 year could be of great value to both patients and clinicians in terms of prognosis and planning of rehabilitation.
The demographics of our patient sample are in accordance with previous epidemiological studies regarding completeness and level of spinal injury, as well as the ratio between men and women in SCI subjects (Albert and Ravaud, 2005; Dahlberg et al., 2005; Martins et al., 1998; Van Asbeck et al., 2000). We therefore consider that the results of this study can be regarded as a representative sample for cSCI.
Persistence and evolution over time of ulnar SSEPs
Severe damage to the human central nervous system is known to be followed by minor or irrelevant regeneration and repair (Edgerton and Roy, 2002). Previous smaller studies probing the integrity of spinal tracts by neurophysiological techniques revealed no relevant changes of SSEP parameters over time after cSCI (Curt and Dietz, 1997; Curt et al., 2008). Comparably, the present study showed that the latencies in the ulnar sdSSEP group, although improved over time, never attained normal values. The small change in ulnar SSEP latency found here stands in contrast to earlier work (Curt and Dietz, 1997; Curt et al., 2008). However, it is important to understand that the improvement was limited to the sdSSEP sub-group, and probably could not be seen in previous studies due to different classification systems and/or smaller patient numbers. In summary, the observed latency and amplitude changes of ulnar SSEPs were of minor dimension and are probably not relevant in terms of hand function. However, the occurrence and persistency of ulnar SSEPs needs consideration when evaluating treatment. Compared to a tibial SSEP study in the lower extremities performed by Spiess and associates (Spiess et al., 2008), fewer patients were classified as aSSEP in the present study. Only 32% of ulnar SSEPs were classified as aSSEP here, whereas nearly 60% of the tibial SSEPs were always absent in the former study. This could be explained by the larger proportion of complete or very severe spinal lesions in paraplegics as compared to tetraplegics. Inclusion of paraplegic as well as tetraplegic patients in the tibial SSEP study by Spiess and coworkers, as opposed to the sole inclusion of tetraplegics in the present study, resulted in a different distribution of lesion severity. The small decrease in latencies and potentially a recovery of amplitude could be explained by a resolution of neurapraxia. However, this is rather unlikely for later stages when significant changes in latencies still occurred. It could be argued that the effects observed over time are caused by spontaneous tract remyelination or re-organization of existing pathways (Nathan et al., 1986). Small changes in spinal impulse conductivity, represented by latency and amplitude modifications, as were found in the sdSSEP and mdSSEP subgroups, may reflect underlying mechanisms of neural plasticity, such as synaptic transmission efficiency or increasing spinal excitability (Fernandez-Galinski et al., 1996; Tao et al., 1996).
ASIA light touch scores
The classification by occurrence and quality of ulnar SSEPs resulted in distinct groups with regard to their average LT scores below the level of lesion, which recovered in parallel for all groups over time. The ulnar SSEP groups could therefore be used as a proxy for ASIA LT scores. No significant differences could be found between the mdSSEP and sdSSEP, or between the rSSEP and iSSEP groups. However, the pooled data from the mdSSEP/sdSSEP groups showed the highest LT scores, whereas the lowest average scores were observed in aSSEP patients. This is consistent with the variation in lesion severity. While differences in LT were large between groups, the average LT scores within each group showed little change over time. Regardless of the initial score, less than a third of a point of improvement over time could be observed below the level of the lesion (Fig. 4). Improvements were found no later than 100 days after cSCI, and their rate of recovery did not differ between groups.
Spinal Cord Independence Measure
Functional evolution of hand and arm function was assessed by the feeding SCIM item, which correlates highly with the total self-care score. This sub-score, ranging from 0–4, reflects sensorimotor function of the hands and arms. All groups showed significant and parallel improvements during the year; however, this could be due to a variety of factors, including compensation strategies. Patients classified as aSSEP seemed to improve less than the other groups. The evaluation revealed a trend toward higher scores in mdSSEP compared with sdSSEP patients (Fig. 5). The difference in average SCIM sub-scores between the mdSSEP and sdSSEP groups indicates that latency and amplitude criteria may additionally help to distinguish early between groups with differing prognoses.
Can stratification by ulnar SSEP criteria serve to determine outcome of hand function in cSCI early on?
SSEP evaluation was suggested as a powerful predictive factor for functional outcome (Curt and Dietz, 1999). Ulnar SSEPs are not only objective and independent metrics, but they also are readily obtainable much earlier than functional assessments. It may not be possible to have a meaningful early assessment of SCIM, as many cervical SCI patients at the early points of recovery cannot be reliably rated due to severe constraints and health impairments such as pain, cardiorespiratory insufficiency, orthostatic hypotension, and other complications impeding patient participation in testing. Accordingly, in our dataset 122 of 365 (33.4%) SCIM assessments were not available 2 weeks after cSCI (stage 1). This makes it difficult to make a valid prediction based on early SCIM assessments. We have found that SCIM scores may be predicted by a single ulnar SSEP assessment performed shortly after cSCI. A time window of 4 weeks was chosen in order to allow for prediction of manual independence, and thus for reasonable rehabilitation planning. An initially present ulnar SSEP (imdSSEP or isdSSEP) is associated with a favorable hand function outcome (PPV 82.1%), whereas an initially absent ulnar SSEP (iaSSEP) is less expressive (NPV 58.3%). Initially mildly or normal SSEP (imdSSEP) subjects show stable SCIM sub-scores after 6 months, whereas isdSSEP patients still improve hand function during the second half of the year following cSCI. Therefore isdSSEP patients showed a prolonged improvement, but reached equal independence levels in this SCIM sub-score 1 year after cSCI. This may indicate a group of patients who could benefit from occupational therapy more than 6 months after cSCI. Early prediction is important for planning the length of stay, and for adjusting occupational therapy to the expected level of independence with regard to training strategies, need for nursing, and technical support. Furthermore it is most relevant to both the patient and caregivers to avoid inaccuracies in prediction.
Significance and limitations of SSEP recording
In spite of significant correlations between ulnar SSEPs and clinical and functional scores in cSCI, a general assessment for neurological outcome and anatomical changes can hardly be drawn from ulnar SSEP recordings. Even aSSEP cSCI subjects with no improvement of impulse conductivity in the dorsal tract may exhibit some neurological improvement. A direct relationship between neurological and neurophysiological parameters cannot be assumed. Moreover, the temporal coincidence of improvements in ASIA LT scores, SCIM sub-scores, and ulnar SSEPs, cannot be taken as evidence of a causal relationship between neurophysiological and functional recovery.
It must be noted that there were epidemiological differences between the ulnar SSEP groups. sdSSEP patients were significantly older than mdSSEP patients, and latencies are known to increase while amplitudes decrease with older age (Zumsteg and Wieser, 2002). This may explain some of the group differences. Bias could have also been introduced because we did not control for other relevant factors such as mechanism of injury, initial surgical treatment or side effects of polytrauma, in this analysis.
Nevertheless, this study is in accord with an analogous previous investigation of tibial SSEPs (Spiess et al., 2008). It supports the notion that there is little or no repair in sensory tracts, and SSEPs remain largely stable during the year post-injury. An ulnar SSEP assessment within the first month after cSCI can therefore be helpful for prediction of hand function outcome. This data collection precisely describes the small amount of change in terms of ulnar SSEP amplitude and latency, as well as minimal sensory change, whereas much larger improvements in function can be expected for particular subgroups well-defined by ulnar SEP categories. Latencies of evoked potentials mainly reflect fast-conducting spinal tract fibers, and thus cannot necessarily be assumed to be representative of the majority of dorsal tract fibers. For the same reason any sensory recovery would not necessarily be reflected by the sensory evoked potentials. Nevertheless, these results make a strong argument that functional gain is not due to sensory recovery, and therefore it can objectively be predicted by an early assessment of ulnar SSEPs. It is suggested to apply SSEPs as a routine test within 4 weeks after acute cSCI.
Footnotes
Acknowledgments
This study was supported by the International Institute for Research in Paraplegia (IFP) Zürich. We thank John Kramer for review and valuable discussion of the manuscript.
We would like to thank all SCI centers who participate in the European Multicenter Spinal Cord Injury (EM-SCI) project, especially the following clinics: Werner Wicker Klinik, Bad Wildungen; Krankenhaus Hohe Warte Bayreuth; Raymond Poincare University Hospital, Garches/Paris; Berufsgenossenschaftliche Kliniken Bergmannstrost, Halle; Stiftung Orthopädische Universitätsklinik Heidelberg; SRH Klinikum Karlsbad-Langensteinbach; Berufsgenossenschaftliche Unfallklinik Murnau; Sint Maartenskliniek, Nijmegen; Spinal Cord Injury Center, University Hospital Balgrist, Zurich.
Author Disclosure Statement
No conflicting financial interests exist.