
Abstract
Traumatic brain injury is a heterogeneous entity that encompasses both surgical and non-surgical conditions. Surgery may be indicated with traumatic lesions such as hemorrhage, fractures, or malignant cerebral edema. However, the neurological exam may be clouded by the effects of medications administered in the field, systemic injuries, and inaccuracies in hyperacute prognostication. Typically, neurological injury is considered irreversible if diffuse loss of grey/white matter differentiation or if brainstem hemorrhage (Duret hemorrhage) exists. We aim to characterize a cohort of patients undergoing bilateral hemicraniectomy for severe traumatic brain injury. A retrospective consecutive cohort of adult patients undergoing craniectomy for trauma was established between the dates of January 2008 and November 2011. The primary outcome of the study was in-hospital mortality. Secondary outcomes were ICU length of stay, surgical complications, and Glasgow Outcome Score at most recent follow-up. During the study period, 210 patients undergoing craniectomy for traumatic mass-occupying lesion (epidural hematoma, subdural hematoma, or parenchymal contusion) were analyzed. Of those, 9 met study criteria. In-hospital mortality was 67% (6 of 9 patients). The average ICU length of stay was 12 days. The GOS score was 3 in surviving patients. Bilateral hemicraniectomy is a heroic intervention for patients with severe TBI, but can be a life-saving procedure.
Introduction
S
In general, acute subdural hematoma (SDH) represents the TBI subtype with the highest mortality, which is estimated at 40–60%. (Bullock, 2006; Fell et al., 1975; Gabl et al., 1989; Haselsberger et al., 1988; Hatashita et al., 1993; Koc et al., 1997; Servadei et al., 1998; Zumkeller et al., 1996), Among those patients presenting to the hospital in a coma (i.e. Glasgow Coma Scale [GCS] score <8), and then undergoing surgical intervention, mortality rates are as high as 68%. (Domenicucci et al., 1998; Gennarelli et al., 1982; Kotwica and Brzezinski, 1993; Lobato et al., 1983; Seelig et al., 1981; Wilberger et al., 1990,1991). However, little is known about the most efficacious treatment for patients with bilateral SDH, or a combination of other types of acute intra-axial or extra-axial mass-occupying lesions. A case series of bilateral craniectomies for penetrating head injury from combatants in the conflicts in Iraq and Afghanistan has been reported; however, pathophysiology from penetrating injury differs from that of closed-head injury (Ecker et al., 2011). Another study suggested that upfront bilateral craniectomy was preferable to delaying the procedure until intracranial pressure became refractory (Akyuz et al., 2010). The optimal management strategy and related outcomes for patients who present with acute, bilateral intra-axial or extra-axial mass-occupying lesions (such as large SDH, epidural hematoma [EDH], or parenchymal contusion) after closed-head injury is largely unknown. We review data from our high-volume neurotrauma center to isolate a case series of this infrequent entity.
Methods
Following approval by the Massachusetts General Hospital (MGH) Institutional Review Board (protocol #2010P002080), consecutive adult patients (age >17 years) undergoing craniectomy for mass-occupying lesions by all providers were retrospectively collected and observed from January 2008 to November 2011. Inclusion criteria included a bilateral cranial operation characterized by the removal of a large fronto-temporal-parietal bone window, with the bones being stored either in a freezer or subcutaneously in the patient's abdomen. Exclusion criteria were defined as any bifrontal operation or any operation in which the bone flap was replaced on the cranium in situ (craniotomy). Additionally, patients were excluded if their contralateral craniectomy was separated in time by more than 8 h.
Details of the patient's presentation were recorded, and included demographics, admission GCS score, presence of a third-nerve palsy, and admission serum alcohol level. Radiographic findings from their initial non-contrast head CT scan were recorded. Details of the operative procedure were previously recorded electronically in the anesthesia and surgical records, including the type of procedure performed, estimated blood loss, and length of surgery. The intensive care unit (ICU) courses of patients meeting entry criteria were retrospectively studied; each patient's electronic inpatient medical record (including daily progress notes, event notes, medication records, radiology records, and physician orders) was extracted for data.
Surgical complications were defined as the development of a clinically significant post-operative hematoma, ischemic stroke, systemic infection, surgical site infection, myocardial infarction, and death, when patient comfort was not the main treatment objective. The Glasgow Outcome Scale (GOS) score was used as a secondary outcome.
Results
During the study period, 210 sequential patients undergoing craniectomy for traumatic mass-occupying lesion (EDH, SDH, or cerebral contusion) were analyzed. Of those, 9 met study criteria (7 male, 2 female). The average age was 40 years (range 19–67 years). Indications for surgery included severe traumatic brain injury with a combination of bilateral SDH, EDH, or parenchymal contusion (Fig. 1). All patients underwent bilateral hemicraniectomy, consisting of a large fronto-temporal-parietal bone flap removal (Fig. 2). This was accomplished either through a single bicoronal incision (Fig. 3), or via separate, standard trauma “reverse question mark” incisions. In-hospital mortality was 67% (6 of 9 patients). ICU length of stay averaged 12 days (range 1–32 days). Complications most commonly included respiratory failure and pneumonia; in addition there were other medical complications, as well as a case of post-operative hemorrhage re-accumulation requiring emergent surgery (Table 1). GOS score for survivors was 3 in all cases.
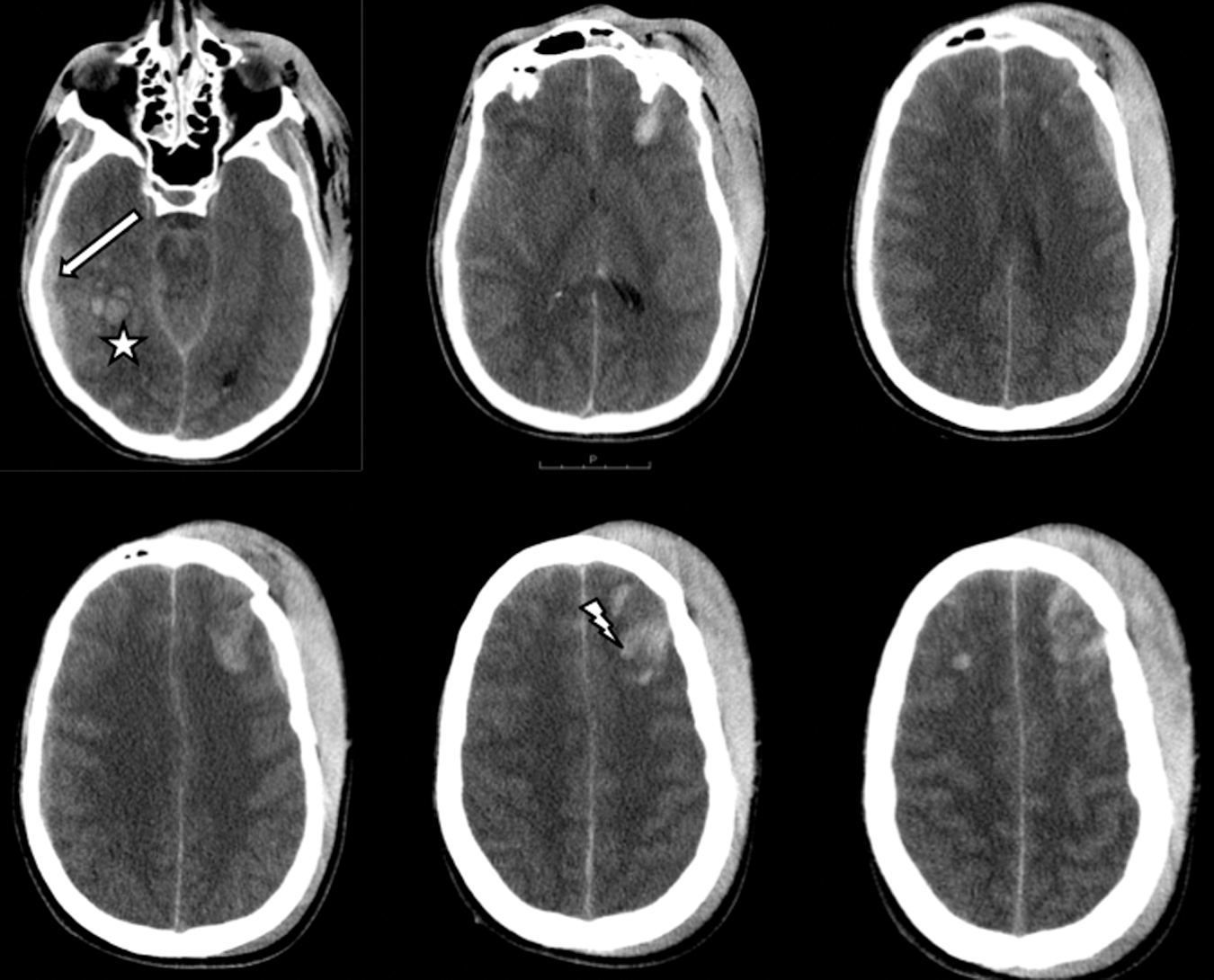
Preoperative head computed tomography (CT) scan. This axial non-contrast head CT obtained upon arrival demonstrates a bilateral severe traumatic brain injury. Surgical lesions are identified as a right-sided temporal contusion (star), right-sided subdural hematoma (arrow), and left-sided frontal contusion (lightning bolt), resulting in brainstem compression.
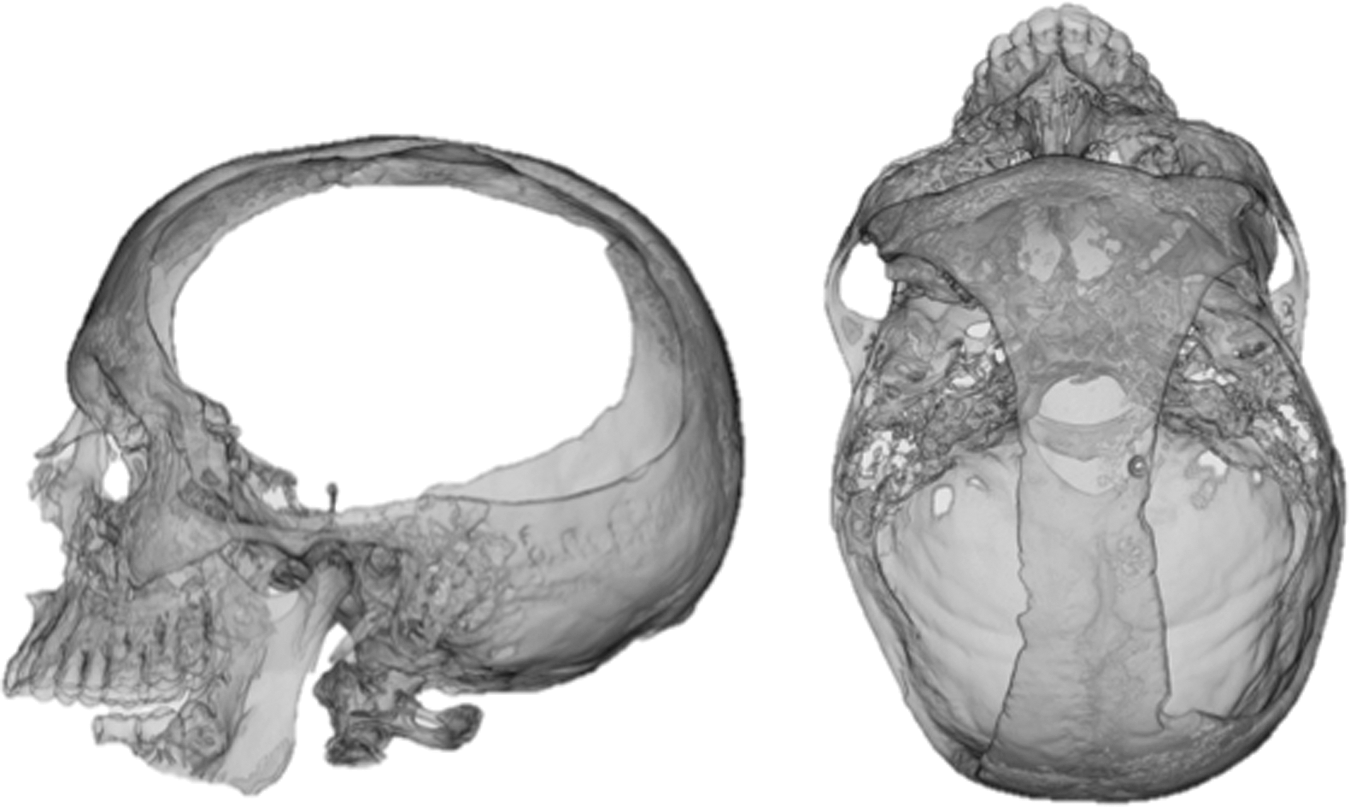
Post-operative head computed tomography (CT) scan reconstruction. Three-dimensional reconstruction of axial-acquired non-contrast head CT scan demonstrates large fronto-temporal-parietal craniectomies.
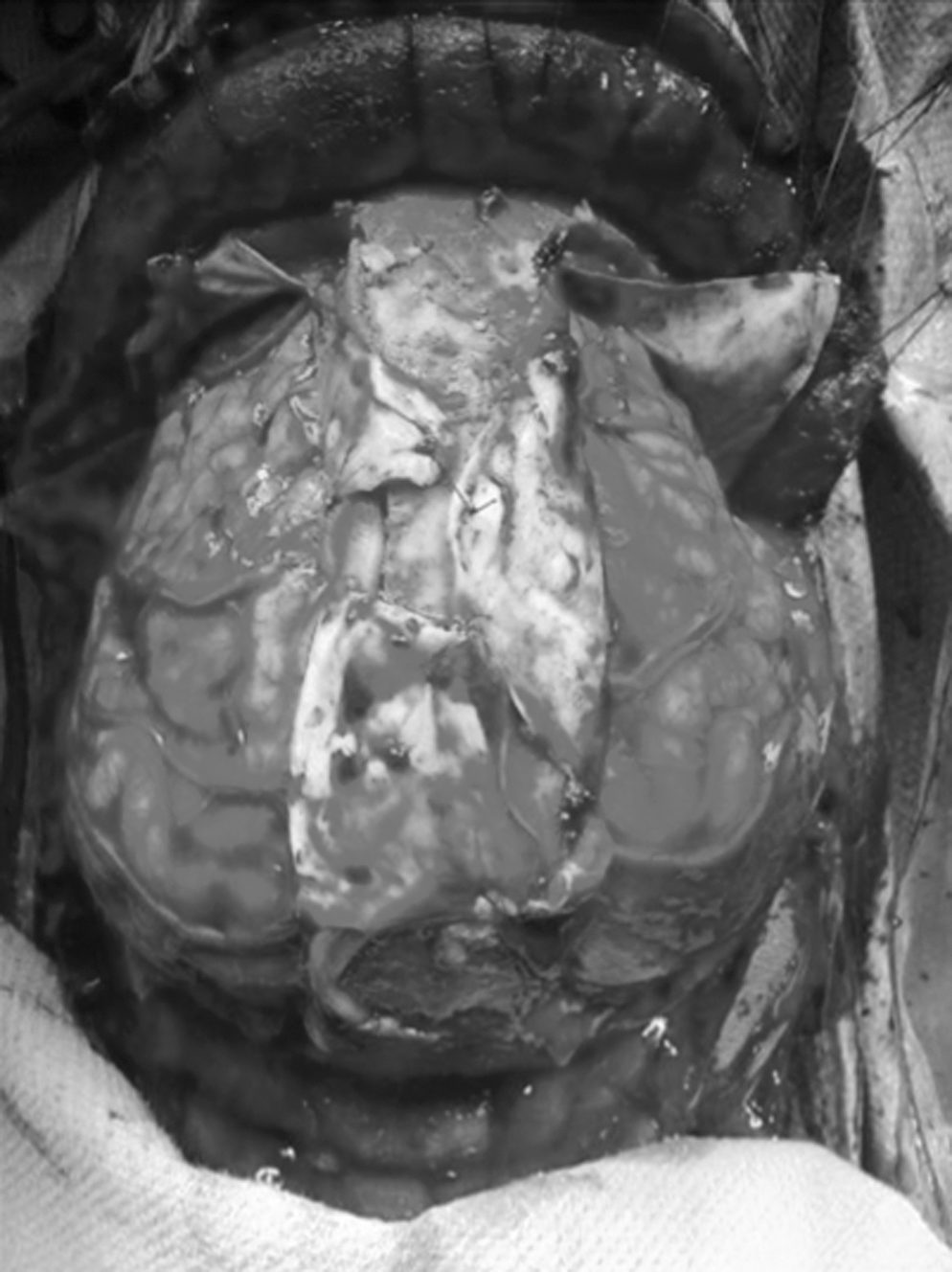
Intra-operative photograph. In this photograph, the patient is positioned supine with the anterior superior aspect of their cranium at the top of the image. Large bilateral craniectomies were performed with the peri-sagittal dural leaflets tacked to each other over a strip of bone that covers the superior sagittal sinus.
GCS, Glasgow Coma Scale (“T” indicates intubated); ICU, intensive care unit; ED, emergency department; ICP, intracranial pressure.
No ICP monitor in place.
Discussion
The decision to operate emergently on traumatic brain injury patients is determined by limited objective data points such as radiographic evidence of mass-occupying lesions and neurological exam results. It is difficult to determine those patients who will ultimately benefit from surgical intervention. Therefore our protocol is to err on the side of surgical intervention when any opportunity for survival and recovery is present. It should be noted that all survivors in our series had an emergency department GCS score of at least 6T and no evidence of a midbrain compression (third-nerve palsy). Alternatively, bilateral closed intracranial injuries causing mass effect, combined with evidence of midbrain compression and poor neurological exam results (GCS score 3T) were associated with universal mortality in our series. In general, prognostication is aided by some factors such as advanced age (Hukkelhoven et al., 2003; Mosenthal et al., 2002) and Duret hemorrhages (Parizel et al., 2002), tend to predict poor outcomes from severe traumatic brain injury. However, survival has been reported after Duret hemorrhage (Stiver et al., 2009), and even patients older than 80 years may be able to return to pre-injury functional baselines (Lau et al., 2012). Other prognostic indicators we use include the early evidence of large hypodensities on the initial non-contrast head CT scan. These patients are expected to have poor outcomes secondary to neuronal death and subsequent secondary brain injury from cerebral edema, as a result of either hemispheric (Duhaime and Durham, 2007; Lobato et al., 1988) or global ischemia (Yoshino et al., 1985). While not all patients with severe traumatic brain injury undergo CT angiography as the initial evaluation, cerebrovascular injury is a common entity and has been shown to affect outcomes (Miller et al., 2002). Occasionally, we have also used CT angiography to demonstrate impaired cerebral blood flow in cases of presumed extremely elevated intracranial pressure or occlusive causes of stroke.
In patients with bilateral operative severe traumatic brain injuries, diagnosis, prognostication, and treatment must be performed almost simultaneously. There is no role for placement of intracranial pressure monitors when the patient needs to be transported immediately to the operating room for a decompressive procedure. En route, several things can be done that may help the patient. For one, optimization of P
This cohort is limited to surgical patients, not taking into consideration patients who were deemed nonsurgical candidates upon initial assessment. Selection bias is also present by excluding patients whose bone flap was replaced, such as in several patients with contralateral epidural hematomas. In these cases, it is likely that less severe injuries existed for which the surgeon did not feel that cerebral edema would be clinically significant. For these reasons, it is likely that the mortality associated with significant bilateral acute lesions is unknown given the size and selection of our cohort.
Bilateral hemicraniectomy is a heroic but potentially life-saving procedure for patients with severe traumatic brain injury following closed-head injury. It is difficult to prognosticate outcome in the hyperacute preoperative evaluation. Therefore, we favor aggressive surgical intervention in the form of bilateral hemicraniectomy when bilateral lesions warrant treatment, particularly in younger patients. Awareness of the associated morbidity and mortality must be conveyed to the patient's representatives when they are available in the preoperative period.
Footnotes
Author Disclosure Statement
No competing financial interests exist