
Abstract
Polyuria contributes to bladder overdistention, which confounds both lower and upper urinary tract management in individuals having a spinal cord injury (SCI). Bladder overdistention post-SCI is one of the most common triggers for autonomic dysreflexia, a potentially life-threatening condition. Post-SCI polyuria is thought to result from loss of vascular tone in the lower extremities, leading to edema and subsequent excess fluid, resulting in polyuria. Mild SCIs that have near complete recovery would therefore be expected to have little to no polyuria, while severe injuries resulting in flaccid limbs and lower extremity edema would be expected to exhibit severe polyuria. Since interventions that may decrease lower extremity edema are recommended to lessen the severity of polyuria, step training (which promotes vascular circulation) was evaluated as a therapy to reduce post-SCI polyuria. In the present study, polyuria was evaluated in mild, moderate, and severe contusive SCI in adult male rats. The animals were housed in metabolic cages for 24-hour periods pre- and post-SCI (to 6 weeks). Urine, feces, food, water, and body weights were collected. Other assessments included residual expressed urine volumes, locomotor scoring, in-cage activity, and lesion histology. SCI produced an immediate increase in 24-hour urine collection, as early as 3 days post-SCI. Approximately 2.6-fold increases in urine collection occurred from weeks 1–6 post-SCI for all injury severities. Even with substantial gains in locomotor and bladder function following a mild SCI, polyuria remained severe. Step training (30 min/day, 6 days/week) did not alleviate polyuria in the moderate SCI contusion group. These results indicate that (1) mild injuries retaining weight-bearing locomotion that should have mild, if any, edema/loss of vascular tone still exhibit severe polyuria, and (2) step training was unable to reduce post-SCI polyuria. Taken together, these results indicate that the current mechanistic hypothesis of post-SCI polyuria may be incomplete.
Introduction
SCI impairments of urologic function manifest as various symptoms, beginning in the acute stage of SCI as bladder areflexia, followed by a slow return of spinally-mediated voiding reflexes. 7 These reflexes are not usually capable of efficiently emptying the bladder, and patients are often treated with anticholinergic drugs to reduce incontinence from bladder hyperreflexia and spasticity. The motor impairment of the sphincter results in detrusor-sphincter dyssynergia, meaning the bladder contracts against a closed sphincter, raising intravesical pressure to dangerous levels. 8 Maintaining low intravesical pressure and avoiding bladder overdistention are keys to maintaining upper and lower urinary tract health, as sustained high intravesical pressure leads to deterioration of the ureters and kidneys. 9
Nocturia, a urologic complication of SCI that has received considerably less attention, is gaining clinical recognition for its substantial impact on quality of life in able-bodied subjects. 10 The primary effect of nocturia is chronic sleep disruption, which leads to poor daytime functioning and is associated with higher rates of morbidity. Nocturia, waking one or more times during the night to void, is usually caused by nocturnal polyuria, an overproduction of urine during the night. 11 For SCI individuals, in addition to chronic sleep disruption, overproduction of urine contributes to bladder overdistention, confounding both lower and upper urinary tract management.
The need for extra (nightly) catheterizations to avoid enuresis (bed-wetting) and bladder overdistention leads to prolonged interrupted sleep for the patient and/or caregivers. Overdistention due to SCI-induced polyuria combined with poor bladder maintenance may further damage the bladder and cause ureteral reflux and nephritis (inflammation of the kidney). 12,13 In addition, polyuria-induced bladder overdistention may lead to episodes of autonomic dysreflexia, a potentially life-threatening condition. 14 Bladder distention is the most common trigger of autonomic dysreflexia. 15,16 Autonomic dysreflexia can be mild or severe, and is characterized by a rapid rise in blood pressure, bradycardia, throbbing headaches, profuse sweating, and flushing; in severe episodes, unconsciousness and death may occur.
The mechanism of polyuria post-SCI is unclear. It is known to be associated with low morning blood pressure and postural hypotension. 17 Traditionally, post-SCI nocturnal polyuria has been attributed to a loss of descending sympathetic tone and subsequent deregulation of antidiuretic hormone (ADH). 18 Briefly, sitting in a wheelchair or standing at an exercise/parallel bar for long periods of time leads to the pooling of venous blood in the lower extremities and third-space extracellular fluid due to a loss of skeletal muscle pumping on venous return. 19 Subsequently, central circulating blood volume is decreased. Upon lying down for rest, the pooled fluids redistribute, increasing blood volume and pressure, which subsequently decreases ADH levels and increases urine production.
Persons with SCI having nocturnal polyuria are sometimes treated with intranasal desmopressin (a synthetic analog of ADH). However, some individuals on desmopressin must still wake to catheterize. 20 Given that SCI individuals are prone to low serum sodium levels, desmopressin therapy increases their risk for developing hyponatremia. 21 Also of concern, individuals may feel comfortable using nasal desmopressin to reduce urine output during the day to reduce catheterizations at work. 20 Combined use during the day and night further increases the risk of hyponatremia. 22
Physical therapy exercises that promote vascular circulation could be beneficial non-pharmacological treatment options for SCI-induced polyuria. Ambulation training with functional electrical stimulation of paralyzed limbs, 23 static arm exercises, 24 and locomotor training 25 promote vascular circulation, blood redistribution, and improvements in cardiovascular responses to orthostatic stress. Task-specific step training after SCI continues to emerge as a safe and effective therapy that can provide increases in ambulation and perhaps other non-locomotor benefits. Therefore, we chose a step-training paradigm to investigate step training's potential beneficial effects on SCI-induced polyuria.
Polyuria has been noted in a rat model of contusive SCI, 26 but has yet to be studied in detail. Therefore, this study evaluated the effects of injury severity on polyuria in a rat model of contusive SCI. SCI's induction of a substantial loss of water due to polyuria prompted an estimation of the water budget to explore potential compensatory mechanisms of fluid conservation (oral water intake, gastrointestinal loss, metabolic water, and activity levels). Furthermore, we investigated step training as a likely intervention that might reduce the severity of polyuria. Additionally, we employed a forelimb-only training group to mimic human arm cycling exercises.
Methods
Animals
All animal procedures were carried out according to National Institutes of Health (NIH) guidelines, and the protocols reviewed and approved by the Institutional Animal Use and Care Committee at the University of Louisville School of Medicine. For study 1, 14 adult (∼300 g) male Wistar rats received either a 150-kilodyne (kD, n=4), 210-kD (n=5), or 150-kD (n=5) contusion injury (1-sec dwell) at spinal level T9 using the Infinite Horizons impactor, 27 and were evaluated for polyuria, metabolic parameters, locomotor deficits, and in-cage activity. For study 2, 33 animals received a 210-kD injury (n=14 step trained, n=9 non-trained, n=10 forelimb trained). Three additional animals received laminectomy only and received no step training.
Surgeries
The animals were anesthetized with an intraperitoneal dose of mixed ketamine (80 mg/kg, Ketoset®; Fort Dodge Laboratories, Fort Dodge, IA), and xylazine (10 mg/kg, AnaSed; Lloyd Laboratories, Shenandoah, IA). Briefly, the surgical area was shaved and cleaned with chlorhexidine scrub. The eyes were lubricated to prevent drying and the following were administered subcutaneously: 0.5 mL of dual penicillin (PenJect®; The Butler Company, Columbus, OH) in a single dose perioperatively as a general prophylactic; 5 mg/kg gentamicin (GentaFuse®; Butler Schein, Dublin, OH) once per day for 5 days to prevent bladder infections; 2.5 mg/kg ketoprofen (Ketofen®; Fort Dodge Laboratories) twice per day for 2 days to alleviate post-surgical pain; and 10 mL saline. The surgeries were performed under aseptic conditions.
Normal body temperature was maintained during surgery and throughout the recovery period via heating pads. The T8 lamina was removed to expose the T9 spinal cord. Spinal clamps were applied to the T7 and T9 spinous processes to stabilize the spinal column. The Infinite Horizon impactor was used to deliver one of three injury forces/dwell times. Laminectomy-only animals had the T9 cord exposed. The muscle was closed with suture, the skin was closed with Michel clips, and topical antibiotic was applied. The animals were single housed with a 12-h:12-h light:dark cycle.
Training paradigm
At 2 weeks post-SCI the animals began a step-training regimen on a three-lane Exer 3/6 treadmill (Columbus Instruments, Columbus, Ohio). The treadmill was modified to accommodate a custom body weight support system with spring scales and side platforms. All animals were harnessed in a Lycra vest (Robomedica, Inc., Mission Veijo, CA), and the spring scales clipped onto the vest rostrally and caudally. The animals were randomized into groups at 1 week post-SCI. Untrained animals were placed on a platform with the spring scales adjusted to provide zero body weight support (this group generally slept or groomed their face and were not standing). Forelimb-trained animals' hindlimbs were supported on a platform just above the treadmill belt, allowing them to ambulate with their forelimbs only at a speed of 22 cm/sec (the spring scales were similarly adjusted to zero body weight support). Step-trained animals ambulated quadrupedally at a speed of 22 cm/sec with manual assistance at the ankle and hip flexor region from a trainer. Body weight support and assistance was adjusted as needed by the trainer. Trained animals were encouraged to step independently as they gained locomotor ability. Attention was given to proper paw placement (plantar, full toe extension, and no ankle rotation), and coordination. The animals were not forced to complete a training session if signs of stress were observed (e.g., porphyrin staining, erratic breathing, or excessive diarrhea). Potentially noxious stimuli were avoided; no tail/perineum pinching was used to facilitate stepping; training sessions were discontinued until skin or paw abrasions healed. All animals engaged in their assigned task 6 days/week, 30 min/day for 47–52 sessions.
Functional assessments
Following SCI, the animals' bladders were expressed via conscious manual crede maneuver twice daily for 7 days and then once weekly to measure residual volumes. The crede maneuver is gentle pressure applied to the abdomen with the thumb and forefingers. The expressed urine was collected in a 5-mL tube. Both the volume (to the nearest 0.1 mL) and weight (to the nearest thousandth of a gram) were recorded.
The animals were housed in metabolic cages for 24 hours to monitor SCI-induced polyuria, water/food consumption, and gastrointestinal (GI) water excretion. Body weight was recorded on the days of metabolic housing. Metabolic cages (Lab Products, Inc., Seaford, DE) utilized separate food and water bins with calibrated water bottles. The animals had ad libitum access to water and food (Laboratory Rodent Diet). Feces were separated with two grid mesh floors and urine was funneled into a collection tube. Urine output and water intake were recorded twice daily to yield two measurements: day/predominantly quiescent phase (8:30
Calculation of metabolic water and vapor loss is complex, requiring specialized airtight equipment to accurately record oxygen consumption, carbon dioxide production, nitrogen excretion, and water vapor. For the current study, metabolic water production and vapor loss values from 60-day-old Wistar rats published by Rafecas and associates 28 was used to estimate the total water balance. The water balance of laminectomy controls of the present study were nearly identical to those reported for naïve rats in the Rafecas study, confirming their accuracy. The only noticeable difference occurred in water loss through feces. Our method of collection at the end of the 24-h period likely allowed some evaporation before our measurements could be taken, resulting in a lower estimate.
In-cage activity was recorded with the Opto-M3 activity meter (Columbus Instruments). A cradle equipped with infrared beams was placed around their home cage. Activity was counted as total movements (number of beam breaks), and ambulatory movements (number of two consecutive beam breaks; e.g., the animal was moving across the cage, as the beams are 1 inch apart). These data were further divided into active (dark 6
The Basso-Beattie-Bresnahan (BBB) open field locomotor test 29 was performed during the quiescent phase to evaluate locomotor recovery. For BBB scoring, the left and right hindlimb scores were averaged together to yield one score per test session. Metabolic cage evaluation and BBB scoring were done pre-injury and on post-injury days 3, 7, and weekly thereafter for 6–8 weeks. The experimenters were blind to injury status.
Histological analyses
At 6–10 weeks post-SCI the animals were deeply anesthetized with 50% urethane. Fixation was done by transcardial perfusion with heparinized saline, followed by 4% paraformaldehyde. Spinal cord epicenters were dissected and cryoprotected in 30% sucrose/phosphate buffer solution with 1% sodium azide for at least 24 h. The dura was then removed and the cord frozen in Tissue Tek OCT medium, and transversely serially sectioned at 30 μm on a Leica CM 1850 cryostat. The sections were stained using a modified Klüver-Barrera method utilizing Luxol fast blue for myelin and cresyl violet counterstain for Nissl substance to identify residual spared white and gray matter. Spot Advanced software (Diagnostic Instruments, Sterling Heights, MI) and a Nikon E400 microscope were used to define spared white matter, gray matter, and cavitation. The lesion epicenter was defined as the section displaying the greatest damage. Percent damage was determined by dividing the total lesion area at the epicenter by the respective total area minus the cavity (white and gray matter sparing at the epicenter as a percent). A few animals were excluded from the histological analysis due to premature death or other invasive anatomical investigations that compromised the collection of spinal tissue from the injury site.
Statistical analysis
For study 1, repeated-measures one-way analysis of variance (ANOVA) followed by Tukey HSD or Bonferroni mixed-model post-hoc tests was performed for comparison of each functional assessment. 30 Levene's test for inequality of variance was performed. A Mann-Whitney U nonparametric test was used for comparison of laminectomy controls to each injured group due to the small sample size. Twenty-four-hour polyuria was analyzed using ANOVA followed by Tukey HSD post-hoc t-test. For study 2, prior to analysis 4 animals were excluded (n=2 non-trained; n=1 trained, n=1 forelimb), as they had a mild injury based on the following criteria: impactor displacement below 1000 μm, greater than 25% white matter sparing at lesion epicenter, or a BBB score ≥14 pre-training (which corresponds to late-stage recovery). Repeated-measures one-way ANOVA followed by Bonferroni mixed-model post-hoc tests were performed for each functional assessment. Statistical significance was set at p<0.05.
Results
The degree of locomotor and urological deficits vary with injury severity
SCI has two phases of injury progression. The first is an initial severing of axons and cell death from the direct impact, hemorrhage, and vascular insult. The second is a secondary injury cascade resulting in demyelination, gliotic scar formation, and cystic cavitation. Histological analysis at 6 weeks post-SCI showed a loss of white and gray matter with increasing injury severity (Fig. 1). A moderate SCI in rats using the IH impactor resulted in central cavitation with only a small amount of spared white matter located in the ventrolateral portions of the cord, as seen with the 210-kD injury. Mild injury produced by the 150-kD force resulted in substantially greater sparing of white and gray matter and no cavitation. However, the addition of a 1-sec dwell time to the 150-kD impact resulted in virtually no white or gray matter spared and substantial gliosis. The mean percent of white matter sparing for each group (mild to severe) are as follows: 150 kD, 47.8%; 210 kD, 10.9%; and 150 kD (1 sec), 1.6%.
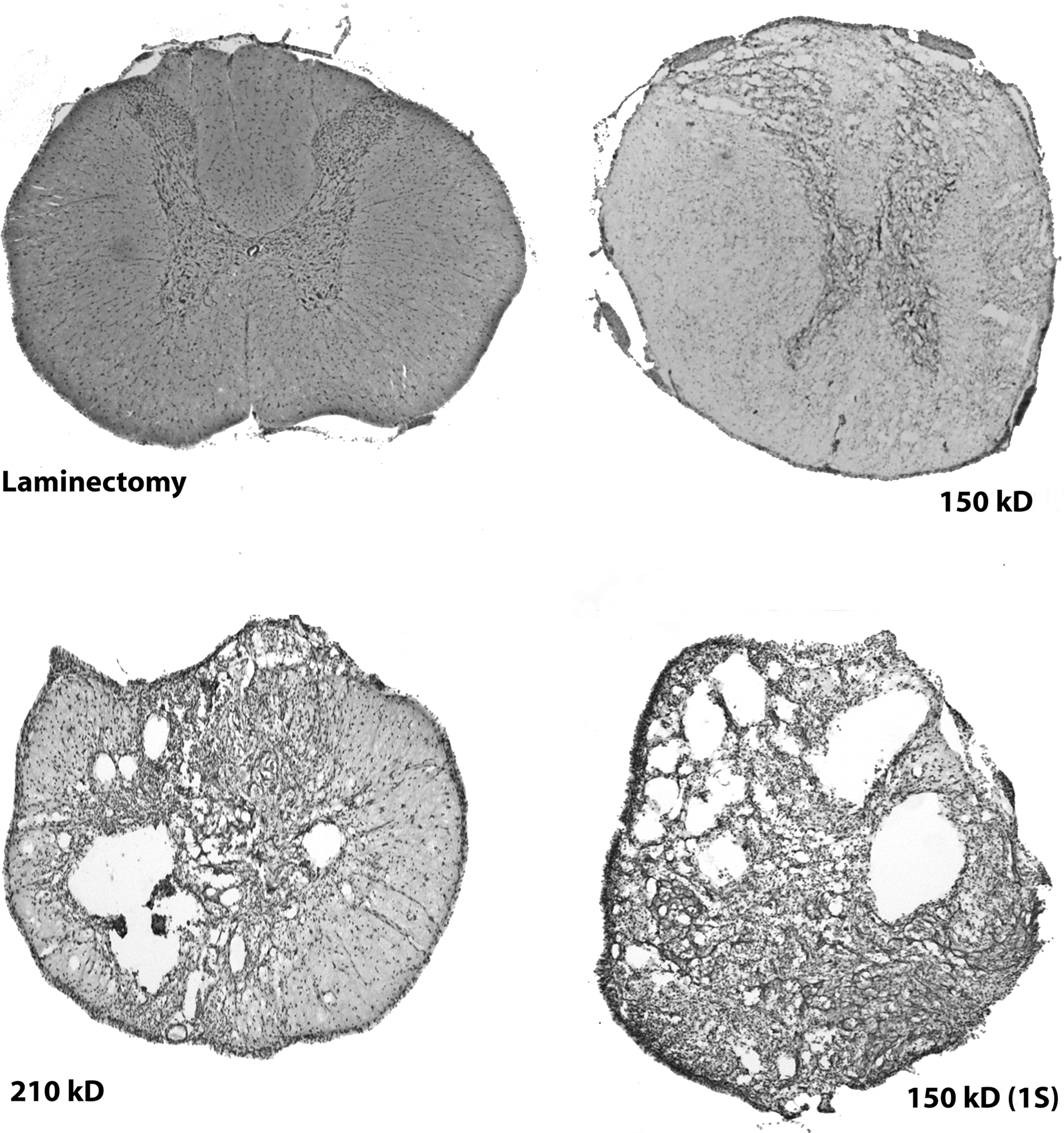
Lesion histology of the epicenter (area with the most damage), demonstrating a loss of white and gray matter with increasing severity. The 150-kD injury results in the loss of white matter without cavitation. More moderate injuries leave a small rim of white matter, such as in the ventral portions of the spinal cord, with the 210-kD injury. The addition of a 1-sec dwell time yields substantial tissue loss (epicenter area and total volume), with no visible white or gray matter at the epicenter and substantial gliosis.
BBB locomotor scoring (Fig. 2) is consistent with anatomical reconstructions of the injuries. Immediately following SCI, a period of spinal shock prevents spared axons from communicating ascending or descending information. Therefore, even a mild injury results in acute flaccid paralysis below the lesion. The results demonstrate that mildly injured (150 kD) animals had no weight-bearing ability at 3 days post-SCI, but rapidly recovered near normal locomotion by the completion of the study, including coordination and paw position. Deficits persisted in tail and trunk instability. Moderately-injured (210 kD) animals demonstrated very little hindlimb movement and no weight bearing at 3 days post-SCI, but gradually achieved weight-bearing steps by 2 weeks post-SCI. However, these animals never regained coordinated ambulation. Severely-injured animals (150 kD+1 sec) were only capable of slight movements of one or two joints at 3 days post-SCI, and never regained the ability to take weight-supported steps.
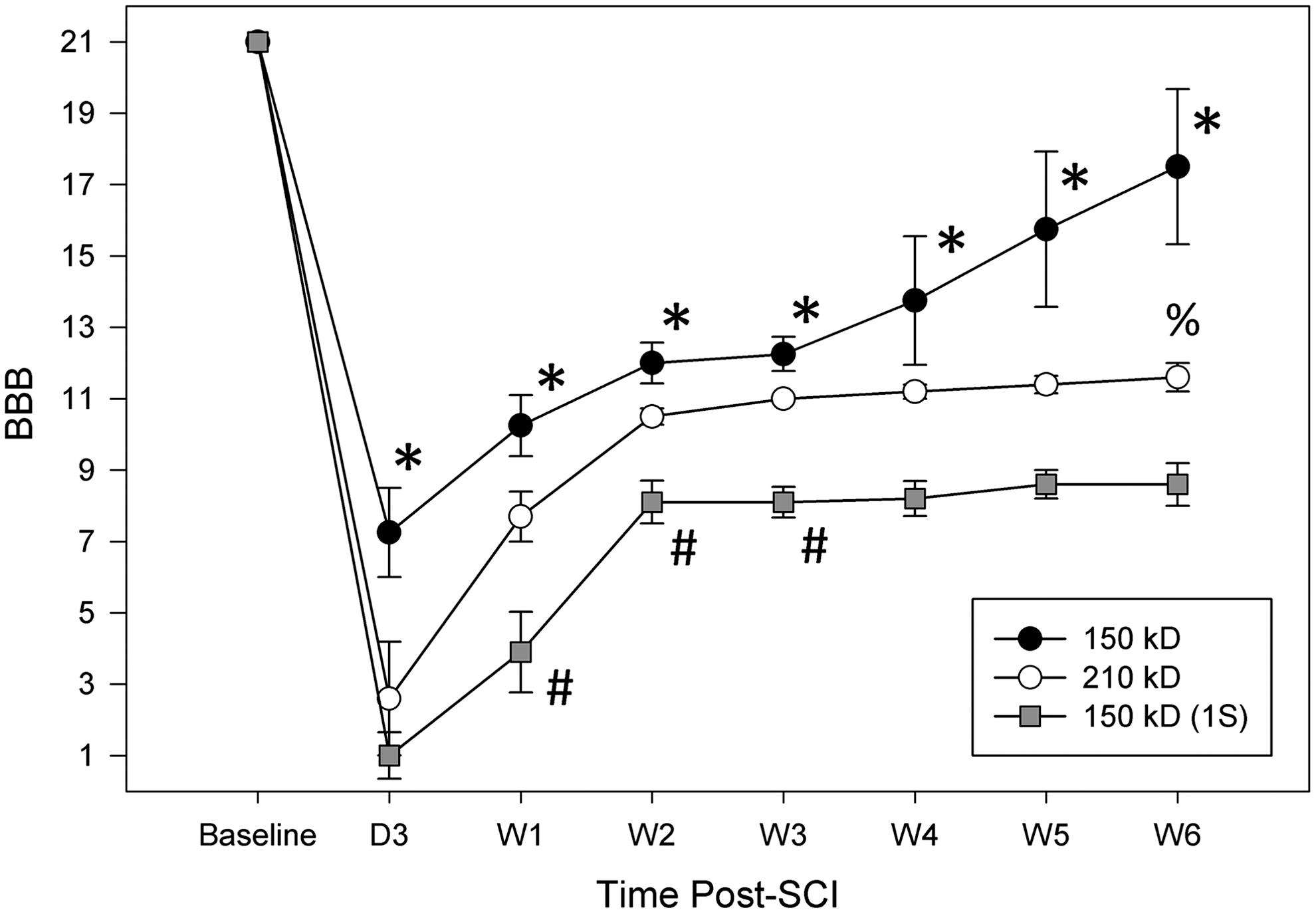
Basso-Beattie-Bresnahan (BBB) locomotor scores show that although the 150-kD group was able to recover coordinated stepping, the addition of a 1-sec (1S) dwell time prevented the animals from achieving weight-bearing steps (*p<0.05 for 150 kD versus 150 kD+1S; #p<0.05 for 150 kD+1S versus 210 kD; %p<0.05 for 210 kD versus 150 kD).
Residual urine volumes (urine that remains in the bladder after voiding as a result of nervous system dysfunction) paralleled the pattern of locomotor dysfunction (Fig. 3). As seen with locomotor behavior, immediately following injury, flaccid bladder paralysis ensues, resulting in an areflexic bladder that must be manually relieved during post-operative SCI care. These residual volumes prominently increased as early as 6 h post-SCI in severely-injured animals (data not shown). Peak dysfunction occurred 3–4 days post-SCI, followed by a re-emergence of a spinally-mediated voiding reflex that is initially present in human infants and rat neonates. 31 All SCI animals required bladder expression for a minimum of 1 week post-SCI, when most animals' residual urine volumes had decreased to below 1-day post-SCI values. Chronic residual volumes (out to 6 weeks post-SCI) recovered in correlation with injury severity. The severe-injury group had significantly greater residual volumes than the mild-injury group (Fig. 3). However, even the mild-injury group retained on average (1 day post-SCI through 6 weeks post-SCI) more than six times the amount of urine as non-injured animals (as reported via ultrasound measurement by Keirstead et al. 32 ).
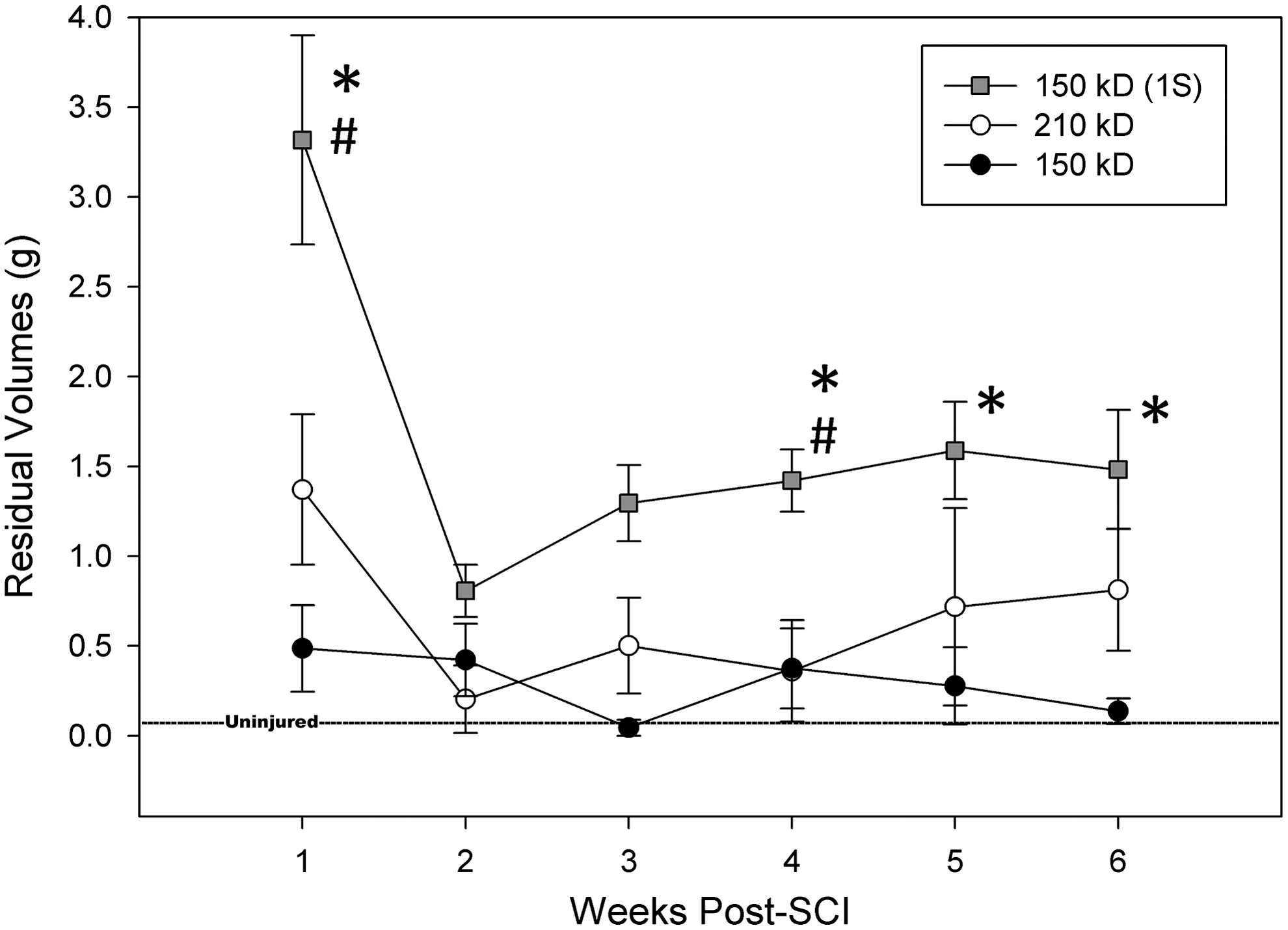
Chronic urological deficits manifest as low voiding efficiency, leaving urine within the bladder. Combined with polyuria, these high residual volumes increase the risk of bladder infection, pyelonephritis, renal damage, and autonomic dysreflexia. Uninjured control value from Keirstead et al. 32 (*p<0.05 for 150 kD+1-sec dwell time [1S] versus 150 kD; #p<0.05 for 210 kD versus 150 kD+1S).
SCI induces polyuria regardless of injury severity
Twenty-four-hour polyuria
Laminectomy control animals' urine output remained the same from baseline. SCI-induced polyuria was evident by 3 days post-SCI and remained elevated from baseline over the length of the study. Each injured group produced significantly more urine in the first 24 h post-SCI compared to baseline. No significant differences were detected between injury groups. SCI resulted in an average 2.6-fold increase in urine production compared to laminectomy controls at 6 weeks post-SCI (Fig. 4).

All injury groups had significantly increased urine production from the pre-injury baseline (#p<0.01), and the 150-kD and 150-kD+1-sec groups were significantly greater than the laminectomy group at week 6 post-SCI (^p<0.01). Laminectomy controls remained the same.
Active-phase (5 pm to 8:30 am ) versus quiescent-phase (8:30 am to 5 pm ) polyuria
All three injury severity groups had significantly greater active-phase urine output (6 weeks post-SCI versus the baseline and laminectomy groups; Fig. 5). The moderate and severe injury groups had significantly greater quiescent-phase urine output (6 weeks post-SCI versus baseline). No group was significantly increased versus the laminectomy group for quiescent-phase polyuria. Therefore proportionally, the active phase was the major contributor to polyuria, with larger increases post-SCI, especially for the most severe group (Fig. 6). This is particularly interesting when the physiological values are considered. In the 150-kD+1-sec group, there was approximately a 20-mL increase from non-injured status. First, this much extra urine leads to bladder overdistention and very frequent, small voids (hyperreflexia). Second, this amount of water loss is not sustainable unless compensatory mechanisms of fluid homeostasis are active.

Proportional representation of quiescent-phase and active-phase polyuria in a 24-h period. All injury groups significantly increased urine production at night compared to baseline. Daytime urine production was also significantly increased for the 210-kD and 150-kD+1-sec (1S) groups compared to baseline (W6, 6 weeks).
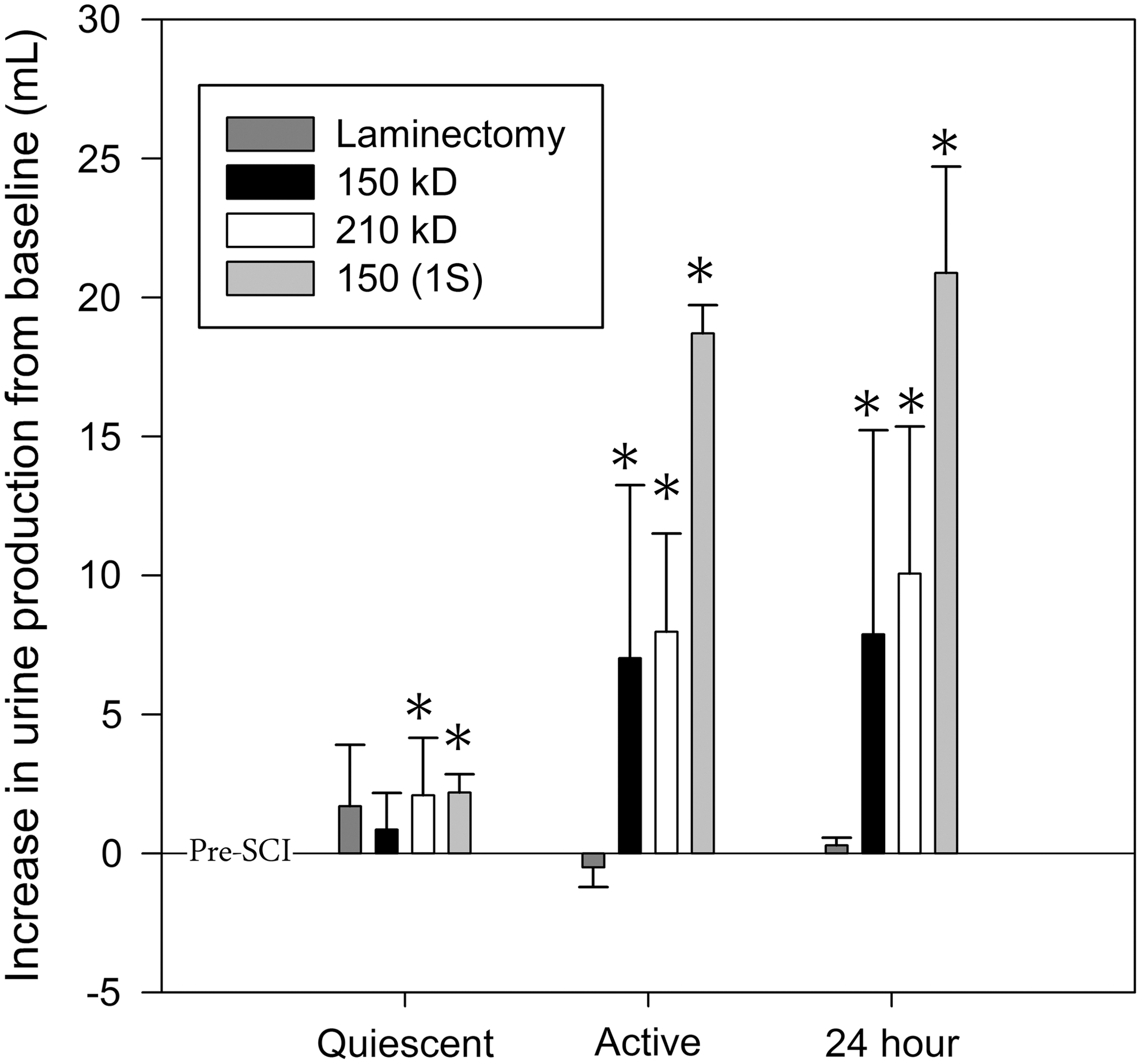
Polyuria at 6 weeks post-SCI quantified as physiological increases (in milliliters) from pre-SCI/baseline. Polyuria affected all SCI groups, and was especially notable in the active phase. Also of note is the approximately 20-mL increase in urine output for the most severely injured group (SCI, spinal cord injury).
Estimation of water balance
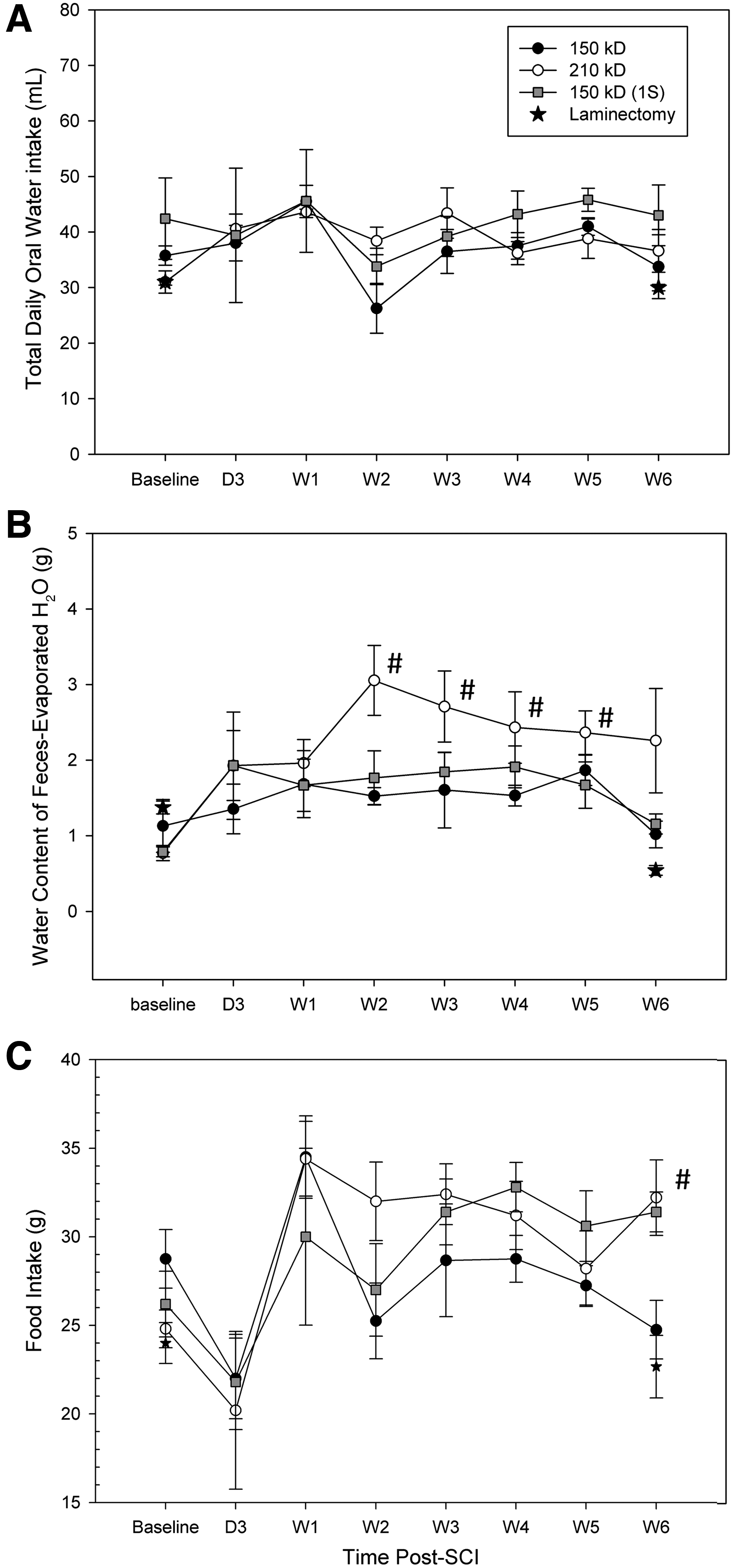
Oral water intake remained stable throughout the study for all groups (Fig. 7A, no significant differences over time or between groups). Water excreted in feces increased post-SCI, but returned close to baseline values by 6 weeks post-SCI for all groups. Interestingly, the 210-kD group displayed the greatest water losses through excrement (in contrast to other functional assessments such as BBB and residual volumes). The 210-kD group lost significantly more water through excrement at weeks 2 through 5 post-SCI compared to baseline (Fig. 7B). In agreement with our findings, Medeiros and colleagues 33 also reported increased water excretion through the gut following a spinal transection.
(
Food consumption was increased in moderately- and severely-injured rats, and therefore the amount of water derived from food also significantly increased compared to baseline, while laminectomy animals remained the same or decreased (Fig. 7C). Greater food intake also translates into greater ingested metabolizable energy (significantly increased in moderate and severe SCI compared to baseline; Table 1). However, the digestive efficiency (grams solid feces/grams solids ingested) remained the same (Table 1). The rate of body weight gain for SCI rats was not significantly different from laminectomy animals (Table 1).
p<0.01; #p<0.05.
Excrement is dry weight. Digestive efficiency is the grams of solid feces/grams solid ingested. Values are means (standard deviation).
Activity does not decrease due to SCI
Activity meter records showed decreased activity with time (Fig. 8). No significant effect of injury severity on activity was detected. Both the injured and laminectomy control groups significantly decreased ambulatory and total movements with time from injury. The injured and laminectomy control groups decreased activity at the same rate (there were no significant differences between groups). Therefore, even severely-injured animals (150 kD+1-sec), which had no hindlimb weight support, moved approximately the same distance as laminectomy animals by pulling their body with the forelimbs and trunk.

Activity meter data of in-cage activity following SCI, represented as both ambulatory (left) and total (right) movements. There were no statistically significant differences between injury groups, and therefore the three groups were combined as “SCI,” and compared to laminectomy only. Both quiescent-phase/lights on and active-phase/lights off are shown. No significant differences were found between the laminectomy and SCI groups. Rats naturally decrease activity with age (Jones et al. 50 ; SCI, spinal cord injury).
Step training 30 min/day 6 days/week does not relieve polyuria
For the training study, the moderate 210-kD injury severity was chosen for measurable deficits that could be reversible. Injury parameters and white matter spared at the epicenters demonstrated uniform injuries in each treatment group. The mean percentage of white matter sparing for each group (non-trained, forelimb, and step-trained) were as follows: 9.2%, 11.4%, and 12.8%, respectively.
Urine collection over 24 h showed no significant differences between step-trained, forelimb-trained, and non-trained SCI animals. The active-phase and quiescent-phase urine collection groups also showed no differences. In agreement with study 1, water consumption could not account for fluid homeostasis. Other metabolic parameters (water excretion in feces, feces, food consumption, and rate of weight gain) did not show any group differences between step-trained, forelimb-trained, and non-trained SCI controls.
Discussion
Functional outcomes following varying degrees of SCI
Graded injury severities resulted in graded histological outcomes, as was evident by the amount of tissue sparing seen at the epicenter. Functional outcomes with both BBB locomotor scoring and residual urine volumes in the bladder were also graded commensurate with severity. However, SCI-induced polyuria affected all injury severity groups, even those with significant locomotor recovery, 26 and reduced residual volumes. In addition, the urine collection during the active phase of the day accounted for most of this increase. Although rats are nocturnal animals, it appears they experience the greatest urine output during their active phase. This is different from the human experience, in which polyuria is evident mostly during the night while asleep. 17 This difference may be partially explained by the manner in which SCI-rats void compared to humans.
Voiding in neonates is dependent on a somato-visceral reflex in many species (e.g., cats, rats, guinea pigs, and deer), whereby the mother stimulates voiding by licking the genitals/perineal region to induce voiding until the post-natal maturation of the adult spinobulbospinal micturition pathways. 34 –36 Without maternal utilization of this reflex, urinary retention develops and leads to death. 37,38 A similar involuntary reflex micturition is present in human infants. 39 Injury to the spinal cord reverts micturition function back to a spinal reflex, leaving humans and animals incontinent. 40 Thus SCI voiding is an involuntary spinal reflex that has re-emerged after the loss of descending supraspinal control. SCI rats empty the bladder through this reflex voiding, in which contact of the genitals with the cage floor evokes the involuntary somato-visceral spinal reflex to trigger voiding. Humans, on the other hand, utilize scheduled catheterizations for bladder emptying to control incontinence.
Thus for SCI rats, the frequency of voiding increases during the active phase due to more somato-visceral stimulation as the animals move/drag, which leads to an increase in urine collection (which may differ from actual renal production rate). During the quiescent phase, not as much stimulation occurs, so the bladder becomes full and overdistended. In contrast, SCI individuals catheterize to empty their bladder and prevent gross overdistention, but actual nightly urine production is approximately double that of a non-injured individual, 17 requiring multiple catheterizations during the night. If the bladder is not emptied, bladder overdistention and bed-wetting occur. It is crucial to maintain dry skin to avoid pressure sores, 41,42 and bladder overdistention presents the very real danger of an autonomic dysreflexic event that can be fatal. 43 While most of us are aware of what one bad night's sleep can do to the next day's functioning, 44 continued poor sleep leads to negative impacts on mood, 45 perceived quality of life, 46 and daily performance. 47
Water balance and metabolic considerations
The rat model of SCI-induced polyuria has identified important questions. As shown in Table 1, SCI rats experience a 10- to 20-mL post-SCI increase in 24-h urine output, which would be unsustainable unless alterations in overall water budget occur. Water is gained through three sources: free drinking water, moisture in food, and metabolic water (water derived from oxidative metabolism). Water is lost in three ways: urine, vapor (loss from the lungs and mucosa during respiration), and via the gastrointestinal tract (feces).
SCI rats significantly increased their food consumption compared to baseline. Therefore, SCI rats also derived more water through food, since the food is 10% moisture (Laboratory Rodent Diet 5001,
Values for a naïve 60-day-old Wistar rat (Rafecas et al., 1993).
In consideration of activity levels (Fig. 8), it would appear that SCI rats eat more not for the water content (it would seem more logical to drink it), but to maintain the same level of activity as a non-injured rat. Moving the same amount of body weight the same distance but without the power from hindlimbs likely requires a great effort and energy expenditure. In comparison to the human condition, movement without the lower limbs is made easier with the use of assistive devices, namely wheelchairs. 48,49
Mechanistic considerations
Although the working hypothesis for polyuria post-SCI is based on lower extremity fluid edema, SCI rats do not experience such extreme diurnal postural differences that would lead to tissue edema. However, for a rat, fluids may accumulate in the lower body due to inactivity and reduced vascular tone below the injury. Increased activity during the active phase or during forelimb and step training should cause muscle pumping to promote circulation and reduce edema (and subsequently polyuria). However, even the mild-injury group that recovered near-normal locomotion exhibited profound polyuria. Additionally, forelimb and step training for a 30-min period per day failed to reduce polyuria. These results suggest that alternate hypotheses for the basis of polyuria should be considered.
Examination of SCI individuals reveals that during the day, ADH levels are increased compared to healthy controls. However, despite 1.5- to twofold ADH upregulation compared to controls, SCI individuals' daytime urine production remained relatively the same as their night-time production. 17 Therefore, the kidneys of an SCI individual may be less responsive to changing levels of ADH. That catheterization is still necessary while taking desmopressin (which has been modified to render it more potent), supports the hypothesis that the kidney is less responsive to ADH. Postural changes that affect blood pressure and circulatory volume have acute effects on ADH activity. Upregulated daytime ADH may be an adaptive response to low blood pressure, and the kidneys may have adapted to ignore this signal for the sake of maintaining blood pressure. Further study is needed to elucidate the true cause of nocturnal polyuria for successful management of urological health and quality of life. Potential targets include aquaporin-2, atrial natriuretic factor, aldosterone, and the renin-angiotensin pathway. In addition, it would also be of interest to investigate polyuria in individuals undergoing longer sessions (1 h or more) of locomotor step training, functional electrical stimulation of the lower limbs, and other physical therapies that may reduce lower extremity edema and promote circulation.
Conclusions
Polyuria is present in all injury severities of the rat model of contusive SCI. Despite near-normal locomotor and residual volume recovery in the mild-injury group, polyuria did not recover and was comparable to that seen in the most severely-injured group. Step training (30 min/day) was not able to reduce the severity of polyuria compared to forelimb and non-trained SCI controls. Even when patients are grouped based on injury location affecting sympathetic pathways (e.g., lesions above or below T6), polyuria manifests itself similarly. 17 Clinicians should be aware that even individuals that have substantial recovery may still experience significant polyuria, regardless of injury location, and should be offered pharmacological and/or non-pharmacological treatment options (e.g., desmopressin, compression stockings, elevating the legs before bedtime, and scheduling fluid intake).
Footnotes
Acknowledgments
The authors would like to acknowledge Christine Nunn for surgical assistance; James Armstrong, Jason Fell, and April Herrity for technical assistance; and Darlene Burke for statistical assistance. This work was supported by grants from the NIH, National Center for Research Resources grant RR015576, National Institute for Neurological Disorders and Stroke grant NS-40919, and National Research Service Award grant F31NS070329 (to P.J.W.), as well as funding from the Department of Defense.
Author Disclosure Statement
No competing financial interests exist.