
Abstract
Taurine, an abundant amino acid in the nervous system, is reported to reduce ischemic brain injury in a dose-dependent manner. This study was designed to investigate whether taurine protected the brain against closed head injury (CHI) in rats. Taurine was administered intravenously 30 min after CHI. It was found that taurine lessened body-weight loss and improved neurological functions at 7 days after CHI. Moreover, it lowered brain edema and blood–brain barrier permeability, enhanced activity of superoxide dismutase and the level of glutathione, and reduced levels of malondialdehyde and lactic acid in traumatic tissue 24 h after CHI. In addition, it attenuated neuronal cell death in hippocampal CA1 and CA3 subfields 7 days after CHI. All of these effects were dose dependent. These data demonstrated the dose-dependent protection of taurine against experimental CHI and suggest that taurine treatment might be beneficial in reducing trauma-induced oxidative damage to the brain, thus showing the potential for clinical implications.
Introduction
T
Taurine (2-aminoethanesulfonic acid) is the major intracellular free β-amino acid present in most mammalian tissues. It possesses a number of cytoprotective properties through its actions as a neurotransmitter, neuromodulator, osmoregulator, modulator of intracellular calcium homeostasis, antioxidant, membrane stabilizer, and anti-inflammation factor and is reported to protect against a variety of pathological conditions, including hypoxia, glutamate-induced neurotoxicity, and inflammation. 4 –7 Clinically, taurine has been used with varying degrees of success in the treatment of a wide variety of conditions, including cardiovascular diseases, epilepsy and other seizure disorders, Alzheimer's disease, and alcoholism. 8 In previous studies, we have demonstrated the neuroprotection of taurine against experimental stroke. 9 –11 These data suggest that taurine may act as an endogenous neuroprotectant to block multiple targets of detrimental cascade after TBI, because current knowledge regarding the pathophysiology of cerebral ischemia and brain trauma indicates that similar mechanisms contribute to loss of cellular integrity and tissue destruction. 1
For investigating the mechanisms of brain injury and corresponding therapy, various models of TBI have been established. Marmarou's weight-drop model is one of the most frequently used constrained rodent models of acceleration closed head injury (CHI) because it is inexpensive and easy to perform, although the biomechanics of the impact produced by this model is not fully and strictly controlled. This model is produced by dropping the weight onto the stainless steel disc cemented to the skull face. It has been shown to induce neurological deficits, brain edema, increased permeability of the blood–brain barrier (BBB), biochemical changes, and widespread damage of neurons, axons, dendrites, and microvasculatures, but there was no supratentorial focal brain lesion. 12,13 Taken together, this model successfully replicates major biochemical and neurological changes of diffuse clinical TBI. In addition, the neurons in hippocampal CA1 and CA3 subfields are more vulnerable to TBI, 14 and the hippocampal neuronal damage resulting from CHI has been reported on. 15,16 Therefore, for determining the protection of taurine against diffuse TBI, Marmarou and colleagues' weight-drop model was used to investigate the effects of taurine on neurological deficits, brain edema, BBB permeability, OS, and neuronal death in hippocampal CA1 and CA3 subfields in this study.
Methods
Closed head injury model
All animal procedures were in accord with the Guidelines for Care and Use of Laboratory Animals and were approved by the institutional animal care and use committee. Male adult Sprague-Dawley rats (weighing 290–330 g, Beijing Vital River experimental animals; Technology Ltd., Beijing, China) were kept under controlled light conditions with a 12/12-h light/dark cycle. Food and water were provided ad libitum. With rats under chloral hydrate anesthesia (400 mg/kg, intraperitoneally), experimental CHI was induced using a weight-drop device described previously 12,17 and modified in our laboratory. Briefly, the skull of the rat was exposed by a longitudinal incision of the skin. A metal disc 0.45 cm in diameter and 2 mm in thickness was firmly fixed by quick adhesive to the right skull vault of the rat 1 mm lateral to the mid-line, just in front of the coronal suture. The rat was placed on a foam bed in the prone position right under a 25-cm-tall Plexiglas tube. A 200-g weight inside the tube was allowed to precisely strike the disc cemented to the skull face. The foam bed, together with the rat, was then moved away from underneath the tube immediately after impact to ensure a single hit. The rat was placed on the operating table for close observation to determine whether the skull vault was fractured. The scalp was then sutured and the rat was allowed to recover from anesthesia. Rats that died on impact and those with skull fractures were excluded. In sham-operated rats, the surgical procedure was prepared for impact in the same way as described above, but animals were not subjected to the head trauma. Rectal temperature was continuously monitored and maintained at 37±0.5°C by a negative-feedback–controlled heating pad during the whole experiment. Body weights were measured before surgery and at 7 days after surgery in all animals, and change of body weight was expressed as the body weight at 7 days after surgery minus that before surgery (Δbody weight).
Experimental protocols
Rats were randomly assigned to six groups treated with taurine or vehicle: 1) taurine (Nanijng Pharmaceutical Factory Co., Ltd., Jiangsu, China), 2 mg/kg; 2) taurine, 5 mg/kg; 3) taurine, 15 mg/kg; 4) taurine, 50 mg/kg; 5) vehicle, a similar volume of normal saline (2 mL/kg); and 6) sham, a similar volume of normal saline (2 mL/kg). Taurine was dissolved in normal saline and administered intravenously (i.v.) twice, in a volume of 2 mL/kg, 30 min and again 4 h after induction of CHI. Control traumatic and sham animals were given vehicle (normal saline). Neurological severity score (NSS) was evaluated 24 h, 48 h, and 7 days after CHI (n=16/group), and histopathology was observed 7 days after CHI (n=14/group). Water content in injured tissue (n=16/group), BBB integrity (n=13/group), levels of malondialdehyde (MDA), glutathione (GSH), and lactic acid, and activity of superoxide dismutase (SOD; n=14/group) were assayed 24 h after CHI.
Neurobehavioral evaluation
In all animals, a battery of neurobehavioral tests was performed before CHI and at 1, 2, and 7 days after CHI by an investigator who was blinded to the experimental groups. Neurological function was measured in terms of NSS, an 18-point scale that assesses functional neurological status based on the presence of certain reflexes and the ability to perform motor and behavioral tasks, such as beam walking, beam balance, and spontaneous locomotion. 18
Measurement of water content in traumatic brain tissue
Water content in the ischemic hemisphere was measured by the wet-dry weight method, as described previously. 19 Briefly, rats were killed 24 h after CHI under 10% chloride hydrate anesthesia. The right hemisphere was dissected and the surface of the sample was gently blotted with tissue paper to remove small quantities of adsorbent cerebrospinal fluid. The sample was weighed as wet weight, then dried in a 120°C incubator for 24 h. Dried tissue was weighed as dry weight after cooling. Tissue water content (%) was calculated as follows: (wet weight – dry weight)/wet weight×100.
Evaluation of blood–brain barrier integrity
Integrity of the BBB was investigated by assessing extravasation of Evans blue dye (EBD), as previously described. 20,21 Briefly, EBD (2% in saline) was injected i.v. (4 mg/kg) 24 h after CHI and allowed to circulate for 2 h. To remove the intravascular dye, we perfused animals with saline through the left ventricle at 100 cm of water pressure until clear perfusion fluid was obtained from the right atrium. After animals were decapitated, brains were removed. The right hemisphere was dissected and incubated in 5 mL of formamide in room temperature for 3 days. The resultant solution was centrifuged at 14,000g for 10 min. The supernatant solution was collected and tissue levels of EBD were assessed using a multi-functional microplate reader (Tecan Trading AG, Salzburg, Austria) at an excitation wavelength of 620 nm and an emission wavelength of 680 nm. Sample values were compared with those of EBD standards mixed with the solvent (0.625–20 μg/mL). The hemisphere was dried in a 120°C incubator for 24 h, then weighted as dry weight after being cooled. Levels of EBD in the hemisphere were expressed as μg/mg dry weight.
Measurement of the levels of malondialdehyde, glutathione, and lactic acid, and the activities of superoxide dismutase
The rat was deeply anesthetized by 10% chloride hydrate at 24 h after CHI, and the brain was removed. The right hemisphere was collected, frozen with liquid nitrogen, and kept under −70°C until analysis. Samples frozen at −70°C were irrigated well with a solution of NaCl (0.9%), and homogenization at a ratio of 1:10 was achieved. The homogenate was centrifuged (3500g, 20 min, 4°C), and the supernatant was used to measure levels of MDA, GSH and lactic acid, as well as the activity of SOD, by kits (Nanjing Jiancheng Bioengineering Institute, Nanjing, China). The protein concentration of the supernatant was determined by Bradford's method. 22
Histopathological examination of hippocampus
Animals were anesthetized with chloral hydrate and transcardially perfused with heparinized normal saline, followed by 4% paraformaldehyde 7 days after CHI. Brains were removed, fixed, and embedded in paraffin, and the 8-μm-thick coronal sections through the hippocampus were collected. Hematoxylin and eosin (H&E) staining was performed following the procedures described in our previous article. 23 Sections were examined with light microscopy and pictures were taken with a digital camera. Quantification of neurons in hippocampal CA1 and CA3 subfields was performed in two adjacent H&E-stained coronal sections of the dorsal hippocampus for each animal. All attempts were made to use the same region of the dorsal hippocampus as was used for evaluation. Clearly defined pyramidal neurons (cell body and nucleus) in hippocampal CA1 and CA3 subfields were counted in two high-power fields (HPFs), and hippocampal normal neurons in CA1 and CA3 subfields were expressed as neurons per HPF.
Statistical analysis
Data are presented as mean±standard error. Comparisons between groups were statistically evaluated by one-way analysis of variance with Bonferroni's post-hoc test (body-weight loss, brain edema, BBB permeability, levels of MDA, GSH, and lactic acid, and activities of SOD, as well as the neuronal numbers in CA1 and CA3 subfields). Neurological deficits were analyzed with Mann-Whitney's nonparametric U test. A probability of <0.05 was considered statistically significant.
Results
Effects of taurine on body weight loss after closed head injury
Before surgery, there was no significant difference among body weights in all groups (Table 1). CHI rats treated with vehicle solution had higher amounts of weight loss, compared to those of sham-operated rats (p<0.01). Treatment with 2 or 5 mg/kg of taurine had no significant effects on body-weight loss; however, 15 or 50 mg/kg of taurine markedly reduced the weight loss after CHI (both p<0.05 vs. vehicle-treated rats). There was no significant difference in weight loss among animals receiving different doses of taurine.
Data are presented as mean±standard error of the mean (n=16/group. Changes of body weight (Δbody weight) are expressed as body weight at 7 days after surgery minus that before surgery.
Mean±standard error.
p<0.01 versus sham-operated rats.
p<0.05 versus vehicle-treated rats.
CHI, closed head injury.
Effects of taurine on neurological severity score after closed head injury
All rats before induction of CHI and sham-operated rats after surgery showed no neurological deficits and performed normally (NSS=0). Vehicle-treated rats showed significant neurological deficits at 24 h, 48 h, and 7 days. Treatment with 2 or 5 mg/kg of taurine reduced NSS at 24 h, 48 h, and 7 days after CHI, but it did not show statistical significance (Fig. 1). Rats treated with 15 or 50 mg/kg of taurine showed marked reduction of NSS at 24 h, 48 h, and 7 days after CHI versus vehicle-treated rats (15 mg/kg: p<0.01, 0.05, and 0.01, respectively; 50 mg/kg, all p<0. 01). In addition, the improvement of neurological function in rats treated with 50 mg/kg of taurine at 24 h after CHI was better than that in rats treated with 2 mg/kg of taurine (p<0.05), and there were no statistical differences among the other groups treated with different doses of taurine.
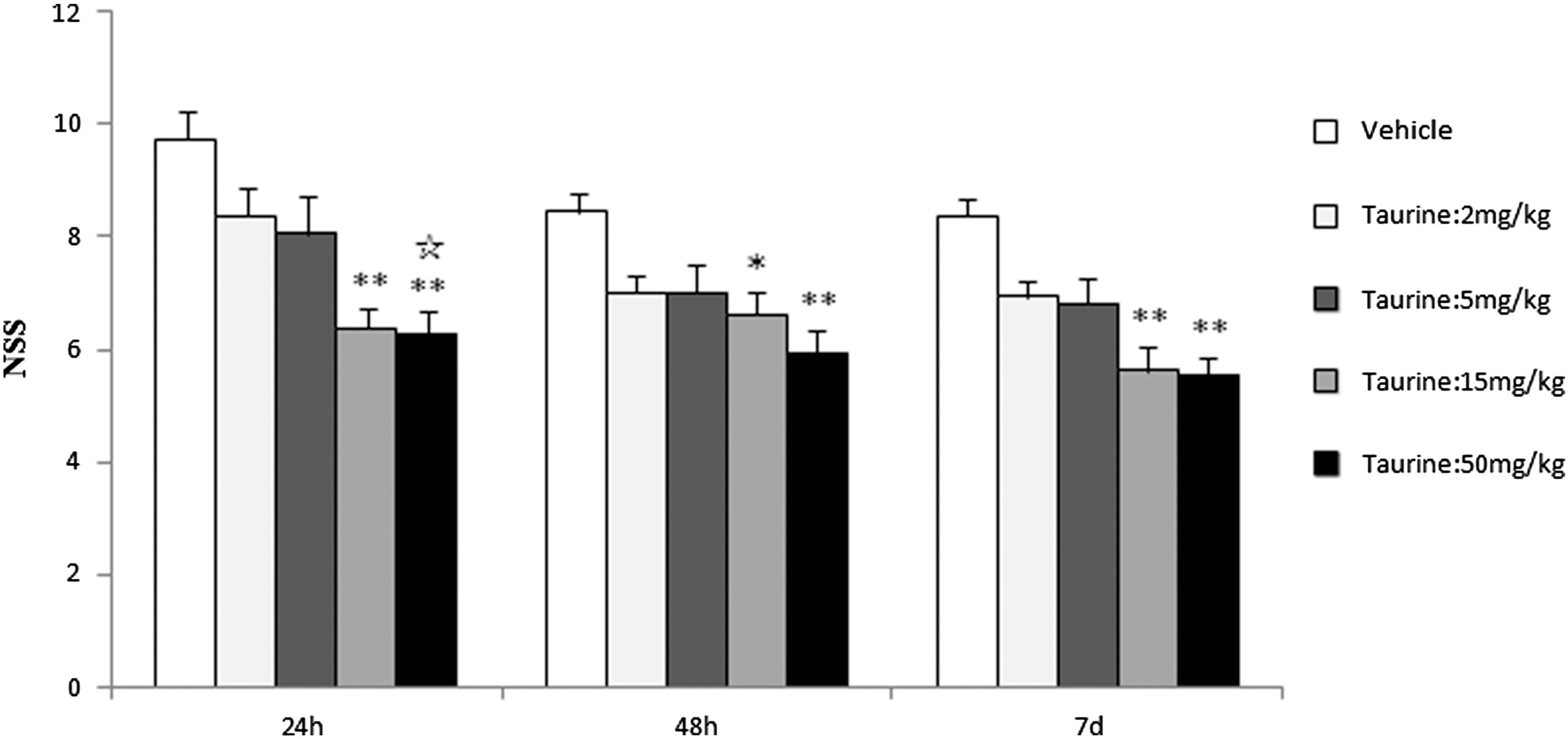
Effects of taurine on neurological deficits after CHI, closed head injury. Vehicle or taurine was injected intravenously 30 min after closed head injury. Data are presented as mean±standard error of the mean (n=16). *p<0.05 and **p<0.01 versus vehicle; ☆ p<0.05 versus 2 mg/kg of taurine. NSS, neurological severity score; CHI, closed head injury.
Effects of taurine on the water contents and the blood–brain barrier integrity in injured hemisphere after closed head injury
Figure 2 depicted the percentage of water content and concentration of EBD (μg/g dry weight) in the injured hemisphere 24 h after CHI in sham-, vehicle-, and taurine-treated rats. Percentage of water content and concentration of EBD in vehicle-treated rats increased significantly after CHI versus sham-operated rats (both p<0.01). Treatment with 2 mg/kg of taurine reduced the percentage of water content and the concentration of EBD in the injured hemisphere after CHI, but it did not reach statistical significance. Taurine at a dose of 5, 15, or 50 mg/kg markedly reduced the percentage of water content and the concentration of EBD in the injured hemisphere (water content, all p<0.05 vs. vehicle-treated rats; EBD, p<0.01, 0.01, and 0.05 vs. vehicle-treated rats, respectively). However, there were no significant differences in the percentage of water content and the concentration of EBD among the groups treated with different doses of taurine.
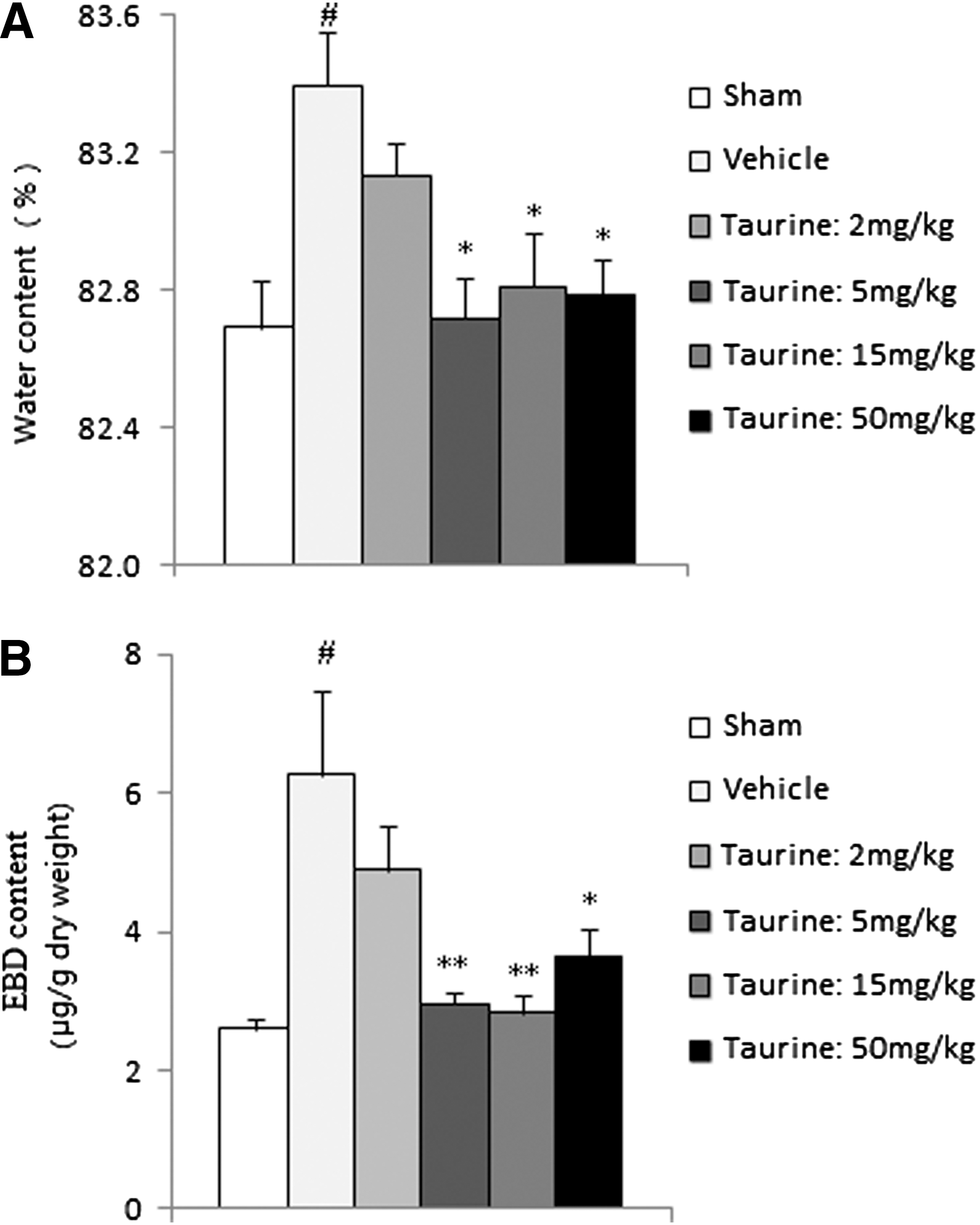
Effects of taurine on the percent of water contents and the content of EBD in traumatic tissue after closed head injury. Vehicle or taurine was injected intravenously 30 min after closed head injury. (
Effects of taurine on levels of malondialdehyde, glutathione, and lactic acid, and the activities of superoxide dismutase
Figure 3 shows the levels of MDA, GSH, and lactic acid, as well as the activities of SOD, in all groups. CHI was found to produce a significant reduction of the activities of SOD and levels of GSH (p<0.05 and 0.01, respectively), as well as an elevation in levels of MDA and lactic acid in the injured hemisphere (both p<0.01). Treatment with taurine at the dose of 2, 5, or 15 mg/kg, 2 or 5 mg/kg, and 2 mg/kg had no significant effects on activities of SOD, levels of GSH, and levels of MDA and lactic acid, respectively. However, treatment with 50 mg/kg of taurine, and treatment with 15 or 50 mg/kg of taurine, markedly enhanced activities of SOD and levels of GSH after CHI, respectively (Fig. 3A,B; SOD, p<0.05 vs. vehicle-treated rats; GSH, p<0.01 and 0.05 vs. vehicle-treated rats, respectively). Moreover, 5, 15, or 50 mg/kg of taurine significantly reduced levels of MDA and lactic acid after CHI (Fig. 3C,D; MDA, all p<0.05 vs. vehicle-treated rats; lactic acid, all p<0.01 vs. vehicle-treated rats). In addition, levels of lactic acid in rats treated with 5 mg/kg of taurine showed a significant reduction, compared with that in rats treated with 2 mg/kg of taurine (p<0.05). There were no statistical differences in levels of SOD, GSH, or MDA among groups receiving different doses of taurine.
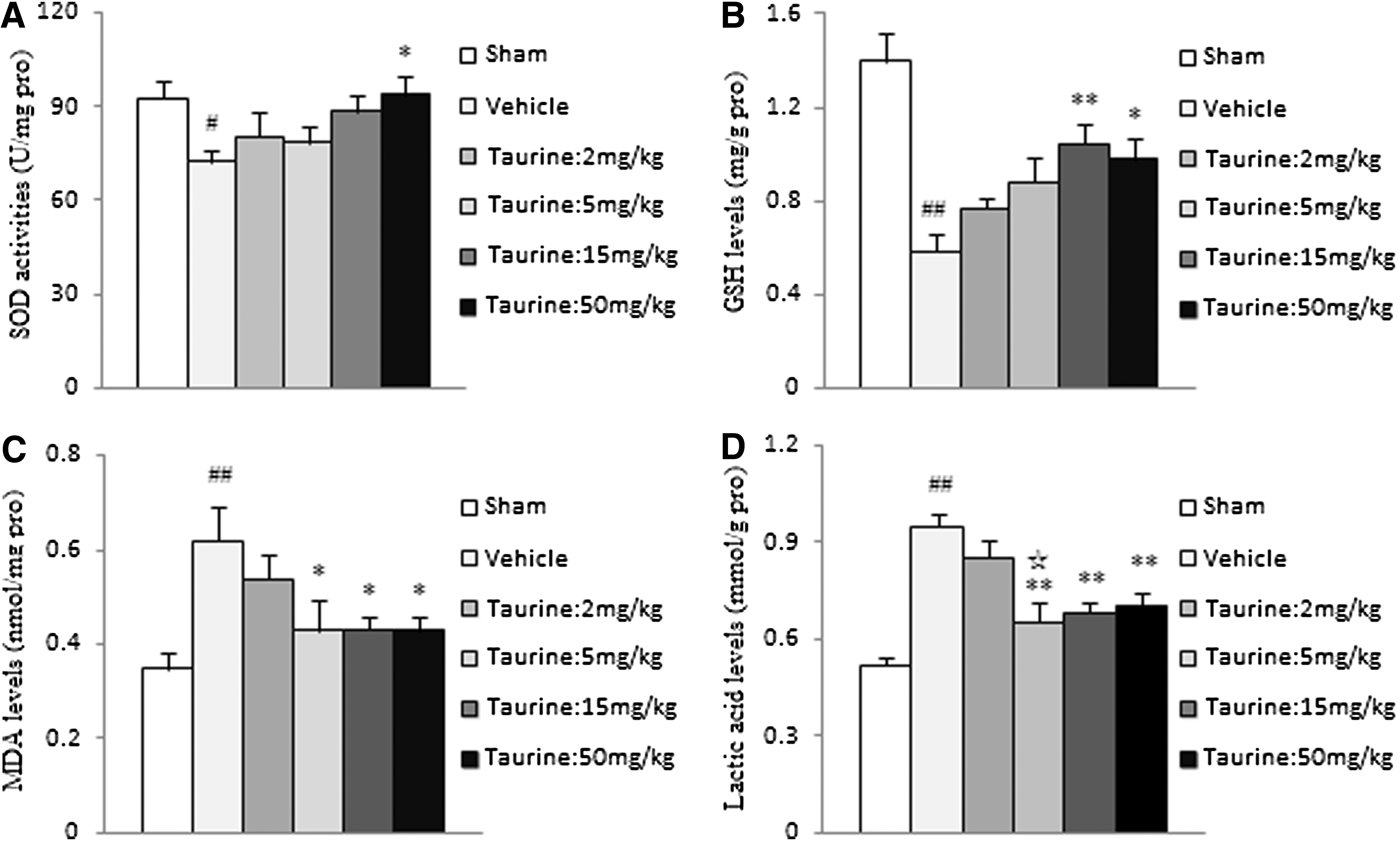
Effects of taurine on activities of SOD, as well as levels of GSH, MDA, and lactic acid, in traumatic tissue after closed head injury. Vehicle or taurine was injected intravenously 30 min after closed head injury. (
Effects of taurine on the neuronal cell death in hippocampal CA1 and CA3 subfields
Histological analysis revealed that 11 of the 14 rats treated with vehicle had scattered neuronal degeneration in the cortex, and 3 others had no significant cortical lesion. All of the vehicle-treated rats showed various degrees of neuronal damage in hippocampal CA1 and CA3 subfields and corpus callosum injury. Degenerative neurons in the cortex and hippocampus showed chromatolysis, nuclear pyknosis, eosinophilic cytoplasm (red neuron), or lacking cellular structure (ghost neuron). Moreover, H&E-stained sections revealed rarefied white matter, vacuolization, and increased cell reactions in the corpus callosum (Figs. 4 and 5). These results indicated that the damage in the hippocampus and corpus callosum was more reproducible than that in the cortex in our model. Because damage quantification in the cortex and corpus callosum in H&E-stained sections was more difficult than that in the hippocampus, we primarily investigated the protection of taurine against the neuronal damage in hippocampal CA1 and CA3 subfields after CHI. CA1 and CA3 neurons in sham-operated rats were normal, possessing a clearly rounded appearance with intact well-defined membranes, a clear nucleus, distinct nucleoli, and a clear cytoplasm (Fig. 5A), and the numbers of survival neurons in CA1 and CA3 subfields were 92±3 (range, 78–112) and 59±1.3 (range, 49–66) per HPF, respectively. In vehicle-treated rats, the numbers of normal neurons in the hippocampal CA1 and CA3 subfields were 61±4 (range, 31–84) and 43±1.5 (range, 30–52) per HPF, respectively, and which were significantly decreased versus that in sham-operated rats (Fig. 5B; both p<0.01 vs. sham-operated rats). Normal neurons in the CA1 or CA3 subfield in rats treated with 2 or 5 mg/kg of taurine had no statistical differences, compared to vehicle-treated rats. However, treatment with 15 or 50 mg/kg of taurine markedly enhanced the numbers of normal neurons in CA1 or CA3 subfields (Fig. 4B; 15 mg/kg of taurine, both p<0.05 vs. vehicle-treated rats; 50 mg/kg of taurine, both p<0.01 vs. vehicle-treated rats). Moreover, the protection of treatment with 50 mg/kg of taurine on neurons in CA1 and CA3 subfields was better than treatment with 2 mg/kg of taurine (both p<0.05), and there were no significant differences among the other groups receiving different doses of taurine.
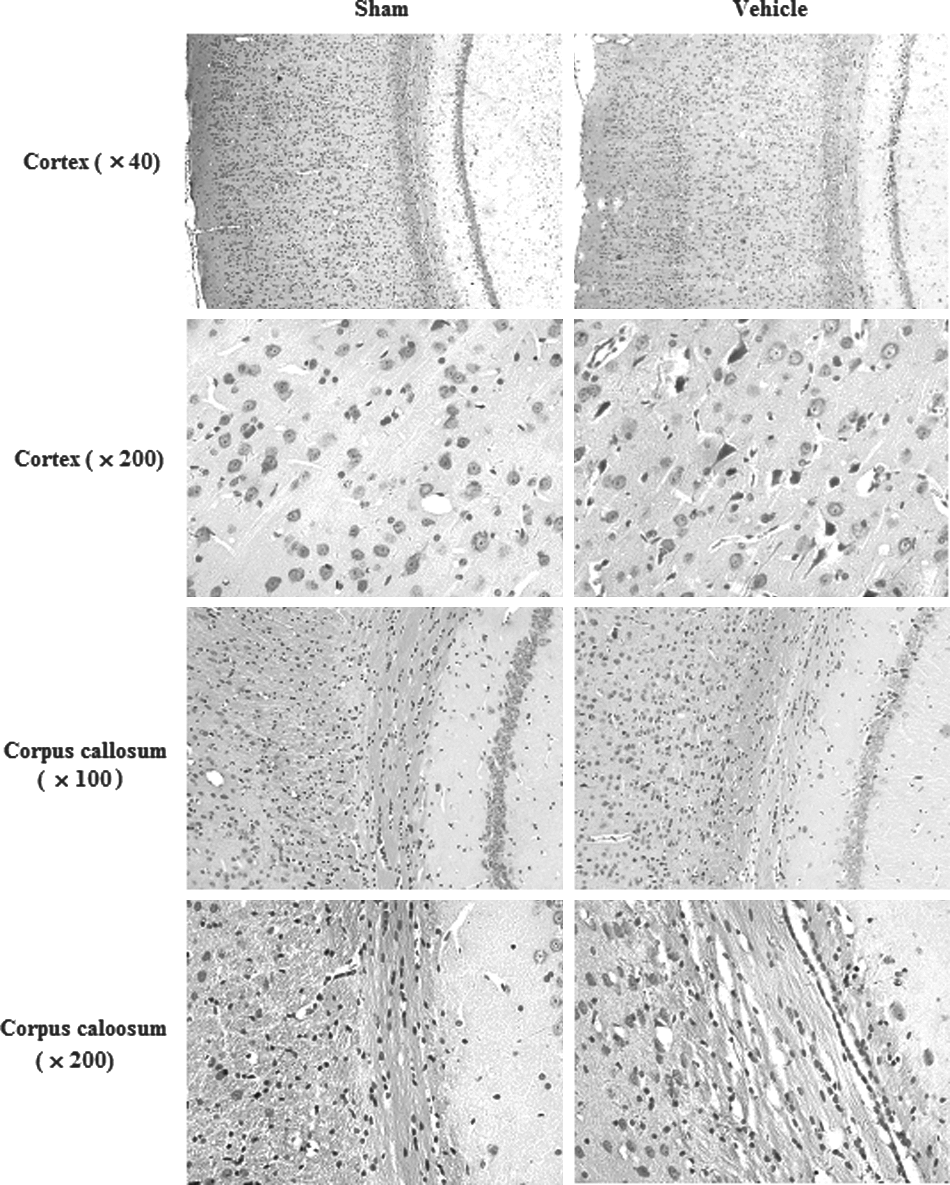
Representative photomicrographs from the cortex and corpus callosum showing histopathological changes 72 h after closed head injury. Hematoxylin and eosin (H&E)-stained sections revealed scattered neuronal degeneration in the cortex, which was characterized by chromatolysis, nuclear pyknosis, eosinophilic cytoplasm (red neuron), or lacking cellular structure (ghost neuron). Also, H&E-stained sections revealed rarefied white matter, vacuolization as well as increased cell reactions in the corpus callosum (cortex: original magnification, 40× and 200×; corpus callosum: original magnification, 100× and 200×).
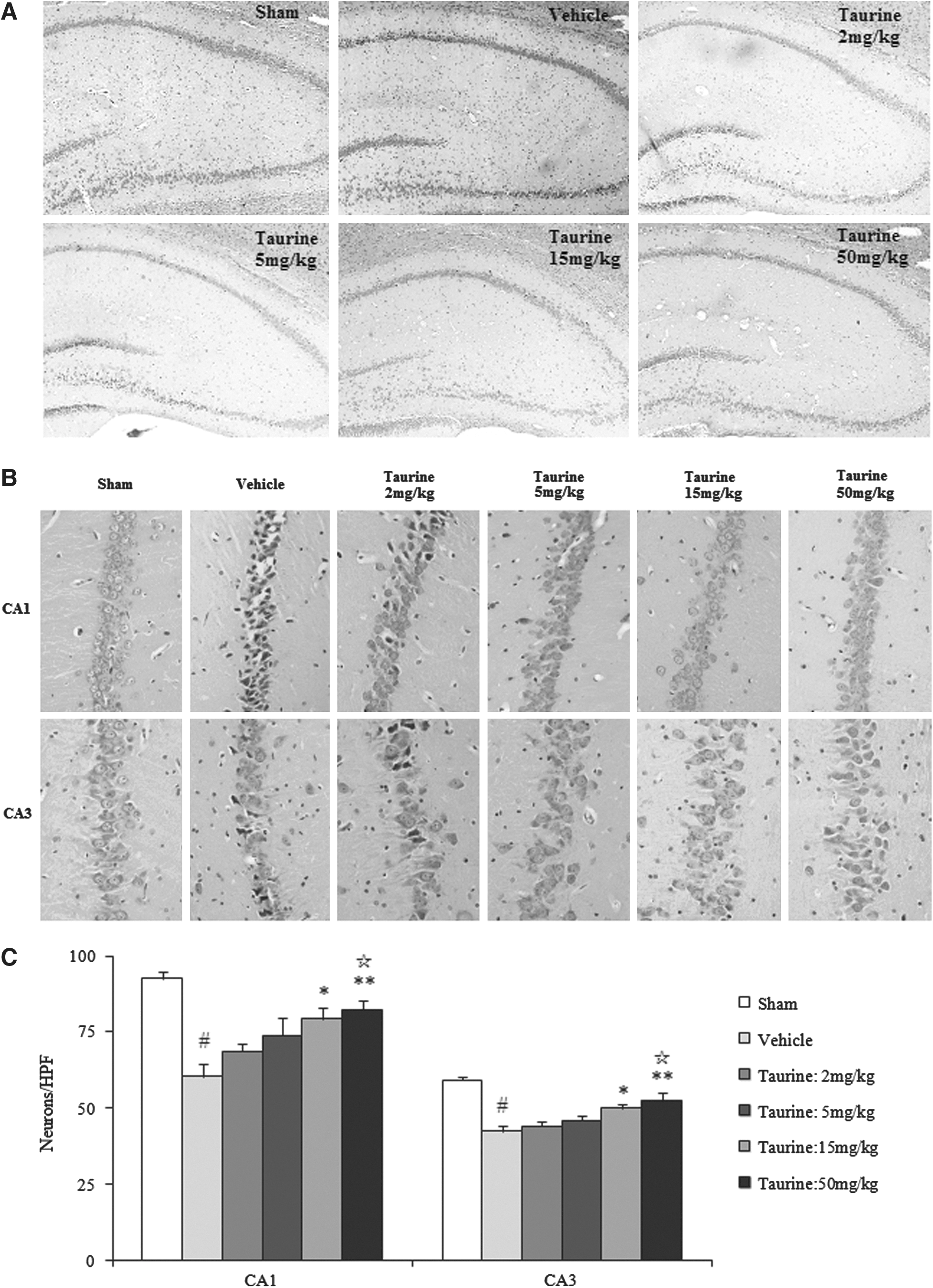
Effects of taurine on neuronal survival in CA1 and CA3 subfields in the hippocampus after closed head injury. Vehicle or taurine was injected intravenously 30 min after closed head injury. (
Discussion
Taurine concentration is very high in the brain. The intracellular/extracellular concentration ratio has been estimated at 400 in neurons 24 and is a functional equilibrium between active uptake, passive release, and biosynthesis from cysteine. Taurine is a key regulator of intracellular homeostasis or enantiostasis. 4,25 During TBI, extracellular taurine increases significantly in the hippocampus within a few hours and remains high 24 h after injury. 26 Increases in extracellular taurine could reflect trauma-induced brain injury. Meanwhile, decreases in intracellular taurine and loss of the intracellular/extracellular concentration ratio resulting from release of taurine may result in the disorder of intracellular homeostasis, leading to neuronal damage. Hence, release of taurine may be an obligatory self-protective mechanism under TBI. 27 During TBI, taurine may exert its neuroprotective function through both extra- and intracellular mechanisms. Extracellular action involves inhibition of calcium influx, which is attributed to suppression of taurine on glutamate-mediated depolarization through opening of the chloride channel. Intracellular action of taurine may be related to its protection of mitochondrial function by preventing mitochondrial dysfunction from calcium overload. 4,7,28 Other functions of taurine, such as antioxidation, anti-inflammation, and osmoregulation, are also contributed to its neuroprotective action. 4,5 Therefore, it is reasonable that exogenous administration of an adequate amount of taurine after TBI may enhance levels of extracellular taurine and reduce release of taurine, consequently contributing to recovery of intracellular homeostasis and reduction of TBI through both extra- and intracellular mechanisms. This speculation has been supported by our results in this study.
Taurine, as a neurotransmitter, neuromodulator, and membrane stabilizer, is used in experimental therapy against neuronal damages caused by neurotoxical substances, hypoxia, epilepsy, and so on. 8 Taurine has been reported to antagonize seizures induced by hypoxia, cobalt, and kainic acid, and the range of an efficacious dose is from 1 to 50 mg/kg. 29 –31 Recently, we have reported the dose-dependent neuroprotection of taurine against experimental stroke, and taurine at 5∼50 mg/kg has significant protection. 9 These data indicate that taurine may protect the brain against CHI with a broad range of doses. Therefore, in this study, we evaluated the protection of 2, 5, 15, or 50 mg/kg of taurine against CHI and found that taurine treatment at the dose of 5, 15, or 50 mg/kg has marked therapeutic effects; however, taurine at the dose of 2 mg/kg only has a tendency to reduce CHI. Our data demonstrate the dose-dependent neuroprotection of taurine against CHI, and the range of the valid dose is similar to that reported in above-cited articles.
As a neuroprotective agent, taurine must pass through the BBB and enter into the brain under neuropathological conditions. Some researchers have found that radioactive taurine increases in the brain after radiolabeled taurine is administered systemically 32,33 as well as the linear increase of taurine concentration in rat brain after i.p. injection. 34 For example, extracellular taurine in the hippocampus increases at 20 min after i.p. injection of 50 mg/kg of taurine and remains elevation for 1 h. Moreover, a Na+ and Cl– gradient-dependent transport system for taurine is identified in both the luminal and antiluminal membranes of bovine brain capillary endothelial cells, and the carrier-mediated transport found by in vitro experiments is confirmed to function for translocation of the taurine molecule from the vascular space into the brain. 35 In addition, taurine has been used with varying degrees of success in the experimental and clinical therapy of seizure disorders, brain ischemia. 8,9,30,31 These studies provide convincing evidences that taurine may cross the BBB and reach the injured tissue to exert its cytoprotection when it is administered i.v. after TBI, although taurine in injured tissue was evaluated in this study.
In regard to the mechanism of taurine against CHI, it is more complicated because both the pathophysiological process of CHI and cytoprotective property are more complex. In this study, we primarily investigated whether taurine exerts neuroprotection through reducing OS, because taurine can act as an antioxidant. 36 –40
It is well known that OS plays an important role in the pathogenesis of TBI. 41,42 Reactive oxygen species (ROS) are highly reactive molecules, which are formed during normal cellular processes, but the production is tightly controlled by a scavenging system, including SOD, GSH peroxidase (GPx) and catalase (CAT), as well as low-molecular-weight (LMW) antioxidants, which can scavenge ROS by direct or indirect mechanisms. Major LMW antioxidants are ascorbic acid, (-tocopherols, GSH, melatonin, uric acid, and so on. Neuronal membranes are rich in polyunsaturated fatty acids, which are prime targets for ROS attack, and asource for lipid peroxidation (LPO) reactions. MDA is a main breakdown product of LPO in the brain. The reduction of the activities of SOD and GPx, and the levels of GSH, and the increases in the levels of MDA have been reported on after TBI. 42 –44 Moreover, ROS scavengers can protect the brain against experimental TBI. 41,42 In experimental and clinic studies, SOD, GPx, CAT, GSH, ascorbic acid, and MDA are used to monitoring the degree of antioxidative capacity and oxidative injury. 44,45 Our results further demonstrate the involvement of ROS in secondary damage after CHI. Taurine is reported to possess antioxidative activity and can protect tissues against OS. 36 –40 The present study suggests that restoring antioxidative defense systems and reducing OS may be one mechanism of taurine against CHI. Taurine could protect the brain against OS during CHI through one or more mechanisms as follows: 1) reducing the ROS production resulting from neutrophils, intracellular calcium overload, and dysfunctional mitochondria; 2) reducing ROS production resulting from metal-stimulated catecholamine oxidation; 3) lessening the LPO and restored the levels of enzymatic and nonenzymatic antioxidants; and 4) scavenging hypochlorous acid and hydroxyl radicals directly. 4,5,31,36,37,46
Contusions resulting from CHI are commonly associated with hemodynamic changes, including focal reductions in local cerebral blood flow. This “ischemia-like” pattern leads to accumulation of lactic acid resulting from anaerobic glycolysis, increased membrane permeability, and consecutive edema formation. 47 In vitro the involvement of lactic acidosis in the generation of ROS and lipid peroxidation has been demonstrated. 48,49 Therefore, it is reasonable that accumulation of lactic acid during CHI could contribute to OS. The present study showed that levels of lactic acid in injured tissue were increased and treatment with taurine reduced levels of lactic acid in injured tissue in the rat model of CHI, suggesting that taurine could not only improve energy metabolism, but also suppress lactic-acid–induced OS, because taurine can preserve mitochondrial function under pathological conditions. 7,10
Taurine, an amino acid found in tissues of most animal species, has not been reported to cause any severe adverse effects or toxicity to date. Taurine is reported to be safe when i.v. administered at a dose of 500 mg/kg/day for 13 weeks in dogs and rats. 50,51 Different investigational studies carried out on humans have shown a marked efficacy and safety of taurine when used in therapeutic doses, such as 6 g per day. 8,52 A recent risk assessment study designates the upper level of taurine supplementation at 3 g per day. This assessment is based on toxicological evidence from a review of all human clinical trials with taurine supplementation. 53 The only adverse effects noted after consuming a 3-g dose of taurine are gastrointestinal disturbances. Therefore, the doses of taurine used in this study are safe. However, direct assessment studies are needed to evaluate the safety, efficacy, and adverse effects of taurine when administered to humans.
In conclusion, this study reports that taurine, in a dose-dependent manner, lessens body-weight loss, improves neurological functions, reduces OS, and attenuates the neuronal death in hippocampus in the rat model of CHI. These results demonstrates the dose-dependent protection of taurine against CHI, and antioxidation may be one mechanism of taurine against CHI. Taurine treatment might be beneficial in preventing trauma-induced oxidative brain tissue damage, thus showing potential for clinical implications. Further studies are required to established the detailed mechanism by which taurine protects the brain against TBI.
Footnotes
Acknowledgment
The authors express their gratitude to Ms. Jingjing Yang for her help in the biochemical assay.
Author Disclosure Statement
No competing financial interests exist.