
Abstract
The primary goal of this study was to compare clinically relevant doses of progesterone and nicotinamide within the same injury model. Progesterone has been shown to reduce edema and inflammation and improve functional outcomes following brain injury. Nicotinamide has also been shown to be an effective neuroprotective agent in a variety of neurological injury models. In the current study, nicotinamide was administered beginning 4 h post-cortical contusion injury (CCI) with a loading dose (75 mg/kg, i.p.) combined with continuous infusion (12 mg/h/kg, s.c.) for 72 h post-injury. Progesterone was administered beginning 4 h post-CCI at a dose of 10 or 20 mg/kg, i.p. every 12 h for 72 h. This resulted in the following groups: Injured-nicotinamide treated, Injured-progesterone-10 treated, Injured-progesterone-20 treated, Injured-vehicle treated, and Sham. Functional recovery was assessed with two spatial memory tasks in the Morris water maze (MWM) the acquisition of a reference memory task and a reversal learning task. Neuropathological assessments were conducted in the cortex and hippocampus. It was found that both progesterone (10 mg/kg) and nicotinamide improved reference memory acquisition and reversal learning in the MWM compared with vehicle treatment. The lower dose of progesterone and nicotinamide also reduced tissue loss in the injured cortex and ipsilateral hippocampus compared with vehicle. The beneficial effects of progesterone appear to be dose dependent with the lower 10 mg/kg dose producing significant effects that were not observed at the higher dose. Direct comparison between nicotinamide and low dose progesterone appears to suggest that both are equally effective. The general findings of this study suggest that both nicotinamide and progesterone produce significant improvements in recovery of function following CCI.
Introduction
T
Nicotinamide, a broad spectrum neuroprotectant, is a soluble B-group vitamin that has been successfully tested in pre-clinical models of TBI to improve functional recovery following injury. Much work has demonstrated that treatment with nicotinamide significantly reduced injury volume, decreased glial fibrillary acidic protein (GFAP)+ activation, reduced blood–brain barrier (BBB) breach, reduced acute edema formation, improved motor performance, and generally reduced behavioral impairments and improved outcomes following cortical contusion injury (CCI) and fluid percussion injury (FPI). 4 –12 Direct comparisons between a 50 mg/kg and a 500 mg/kg dosing regimen have resulted in some minor dose differences, but in general, both dosing regimens have been shown to be effective in facilitating recovery of function following FPI. 9 More importantly, we have also shown that the window of opportunity for the 50 mg/kg dose is between 6 and 24 h post-CCI, depending upon the task and treatment regimen. 7,8 Therefore, there is substantial pre-clinical evidence in young animals (3–6 months) that nicotinamide significantly improves functional recovery and reduces many pathophysiological variables following TBI. We have also examined continuous delivery of nicotinamide (via osmotic mini-pumps) in order to establish steady state serum levels of nicotinamide following injury, and have also found significant improvements in behavioral recovery. 12,13 It appears that continuous administration of nicotinamide for several days post-TBI may be the optimal dosing regimen.
Another promising treatment for TBI is progesterone, which has been studied in pre-clinical models of TBI for several decades, 14 –17 and is currently in clinical trials. A systemic review of progesterone treatment in experimental TBI concluded that progesterone reduced lesion volume in a dose-dependent manner if administered immediately following injury or no later than 6 h post-injury. 18 In male rats receiving a progesterone dose of 4 mg/kg (i.p.) at 1, 6, and 24 h after CCI, serum progesterone concentrations were shown to correlate with decreased cerebral edema. 19 These serum concentrations ranged from 0–38 ng/mL and 5–12 ng/mL at 1 and 6 h, respectively. This is consistent with the original observation that male rats had significantly more edema than female rats after cortical contusions. 20 Even with significant pre-clinical work with progesterone, there have been some concerns with dosing regimens. A dose-response study evaluated progesterone at either 8, 16, or 32 mg/kg administered at 1, 6, and 24 h post-CCI with repeated administrations every 24 h for an additional 4 days following CCI. 21 The initial dose was administered i.p. and all subsequent injections were subcutaneous. It was found that the 8 and 16 mg/kg doses improved water maze performance compared with the 32 mg/kg group, and none of the doses significantly decreased lesion size. 21 Similarly, a study in older rats also found that the 32 mg/kg dose resulted in significantly fewer beneficial effects on inflammatory factors than 8 mg/kg and 16 mg/kg at 48 h post-injury. 22
Nicotinamide and progesterone would make ideal candidates for direct comparison, given their substantial pre-clinical histories. Therefore, the main object of this study was to compare clinically relevant doses of nicotinamide and progesterone (both low and high) to each other following unilateral CCI, utilizing a 72 h dosing regimen. The dosing regimens of progesterone that were examined in the present study were selected based on our previous pharmacokinetic study 23 and are similar to some in the published literature. 19,22 Drug concentrations were confirmed by serum analysis 72 h post-TBI, and the animals were tested with a battery of behavioral tests and then assessed for tissue loss.
Methods
Subjects
Male Sprague–Dawley (Harlan, Indianapolis, IN) rats ∼3.5 months of age at the time of the injury (mean body weight=330.00) were used in this study. All animal and surgical procedures were adhered to as described in the NIH Guide for the Care and Use of Laboratory Animals. The Southern Illinois University Institutional Animal Care and Use Committee reviewed and approved all experimental procedures. Before and after injury, animals were housed in a university-maintained, Association for Assessment and Accreditation of Laboratory Animal Care (AAALAC) accredited vivarium, with a 12 h light/dark schedule and a controlled environmental temperature of 22°C in standard housing with food and water available ad libitum. A power analysis performed based on the experimental design indicates that groups of n=9 result in a power score>0.85 and are more than adequate to detect significant differences among groups in the behavioral studies. One animal in the sham group died following surgery and was not replaced. Specific group sizes are shown in Table 1.
NAM, nicotinamide; CCI, cortical contusion injury; PROG, progesterone.
Surgery
All surgeries were performed under aseptic conditions. The CCI model utilized in the present study was based on previous studies.
8,11
Animals were anesthetized using a mixture of isoflurane (2–4%) and oxygen (0.8 L/min). When the animal became unresponsive (no ocular or pedal reflexes) the head was shaved and scrubbed with 70% alcohol followed by betadine and placed into a stereotaxic device. A midline incision was made in the skin as well as through the underlying fascia. A circular craniotomy (5.0 mm) was centered 2.4 mm posterior to and 2.4 mm lateral (left) to bregma. The contusion injury was created with a sterile stainless steel impactor tip (4.0 mm in diameter) that was attached to the Benchmark™ stereotaxic impactor (
The mini-pump implantation procedure occurred following the first surgery. 12,13 The rat was allowed to recover motor behavior following CCI surgery. Then, 4 h post-CCI, osmotic mini-pumps (Alzet #2ML1) were implanted (s.c.). Using similar procedures as before, gas anesthesia was administered, the surgical site was sterilized, and a midline incision was made in the back halfway between the forelimb and hindlimbs. After the incision was made, the underlying fascia and connective tissue was separated from the skin and the osmotic mini-pumps were placed within the “pocket.” Afterwards, the incision was closed with skin staples. With the animal under anesthesia, pumps were explanted 3 days later and the incision sutured closed.
Drug administration
Progesterone (Sigma #P3972, St. Louis, MO) was administered at either a dose of 10 mg/kg, i.p. (Prog-10) or 20 mg/kg, i.p. (Prog-20), and nicotinamide (Sigma #N5535, St. Louis, MO) was administered with osmotic pumps (Alzet, Cuperzino, CA), which allow for continuous infusion. An initial loading dose was administered (75 mg/kg, i.p.) and the pumps delivered a continuous dose of (12 mg/kg/h). To control for effects following injections and/or pump implantation, all animals were injected and implanted with osmotic pumps. Progesterone was diluted in peanut oil (Crisco, Orrville, OH). All animals received an injection 4 h post-injury and an additional injection every 12 h for 72 h post-injury. Following the 75 mg/kg loading dose (diluted in saline) of nicotinamide 4 h post-injury, nicotinamide-administered animals received injections of peanut oil for the remaining injection time points. Both the Sham and Vehicle groups were administered with i.p. injections of peanut oil and osmotic pumps filled with 0.9% sterile saline (Sigma #14190, St. Louis, MO) for all injection time points. See Table 1 for specific treatment regimens administered to each experimental group. All behavioral and anatomical analyses were performed without knowledge of group assignment and rats were randomly assigned to surgical and treatment conditions.
Serum analyses
Blood samples (750 μL) were collected from the tail vein 1 h post-final injection. Blood serum was separated by microcentrifuge and stored at −80°C. Nicotinamide levels were analyzed in serum using high-performance liquid chromatography (HPLC) with UV detection at 254 nm on a Varian Pro Star 210 HPLC system using a modification of a previously developed assay to measure nicotinamide adenine dinucleotide (NAD). 12 The progesterone samples were analyzed using an enzyme linked immunoassays (ELISA) (R&D Systems Inc, Minneapolis, MN, and VWR International, West Chester, PA). 23
MWM: Reference memory acquisition
All animals were tested in the MWM using a reference memory paradigm that has been widely used to assess cognitive performance following TBI. 4,7,24 The apparatus consisted of a circular, 183 cm diameter blue plastic pool partially filled with water (22°C) to a depth of ∼ 41 cm. A clear plastic platform (10 cm×10 cm) was submerged ∼ 2 cm below the surface of the water. The animal's progress on the task was recorded by a video camera affixed above the pool, and these data were processed using the MWM specific computer software SMART (San Diego Instruments, San Diego, CA).
Animals were assessed on the acquisition of a reference memory task beginning on post-CCI day 20, and were tested for 3 subsequent days. On every testing day, each animal was given four trials during which to locate the submerged platform in the pool, starting at one of four release points in random order. In this reference memory task, the platform remained in the same place for each trial on every testing day. The trial was terminated when the rat reached the submerged platform in the northeast quadrant or when 90 sec had elapsed. If the rat did not find the platform within the 90 sec, it was gently guided to the platform and remained on it for at least 10 sec. Each rat remained on the platform for 10 sec, after which it was placed in a warm holding cage for at least 15 min before the next trial.
MWM: Reversal learning task
Additionally, all animals were tested on a reversal learning task in the MWM on post-CCI day 26. 25,26 The platform was submerged in the southwest quadrant, opposite to its initial location in the reference memory task. Each rat was given four trials per day, starting from one of four randomly selected release points (inter-trial interval was 15 min). Each trial was terminated when either the animal located the platform, or 90 sec elapsed. Each animal's performance was evaluated on the latency to reach the submerged platform.
Histology
At 30 days post-CCI, the rats were euthanized with Euthasol (Virbac Animal Health; 0.3 mL i.p.) (3.0 g/kg, 0.5 g/mL, i.p.) and transcardially perfused with 0.9% phosphate-buffered saline (PBS), followed by 10% phosphate buffered formalin (PBF). Brains were postfixed in PBF following removal from the cranium. A 30% sucrose solution was used to cryopreserve the brains 3 days prior to frozen sectioning. Serial, coronal sections (40 μm thickness) were sliced using a sliding microtome on a frozen stage, and collected into a cryopreservative solution and stored at −20°C.
Lesion analysis
A series of sections were brush-mounted on gelatin-subbed microscope slides, stained with cresyl violet, dehydrated, and cover-slipped. The extent of the lesion was analyzed with an Olympus microscope (BX-51) and an Olympus 13.5 megapixel digital camera (DP-70). Images of sections throughout the extent of the injury coordinates were captured using the digital capturing system, and area measures of the lesioned tissue were determined using the ImageJ software package (1.43u, NIH). The Calvalieri method was used to calculate the volumes of the ipsilateral cortex and the contralateral cortex. 27 Five stereotaxic coordinates throughout the lesion, at ∼−0.80, −1.80, −2.80, −3.80, and −4.80 mm relative to bregma, were selected for lesion analysis. The number of sections and the section thickness (40 μm) were multiplied by the mean area of the remaining cortex. The extent of cortical injury was measured by calculating the percent reduction in the injured ipsilateral cortex compared with the contralateral cortex at each level using the formula: [1 – (ipsi/contra)×100] and we have reliably shown that this technique is sensitive enough to detect treatment-induced reductions in injury size. 8.9.27.28
Statistical analysis
Behavioral data was analyzed using a Mixed Model Factorial ANOVA or one-way between-subjects ANOVA. Treatment was the between factor and, if applicable, day of testing was the within group factor (SPSS v. 15 for Windows). The between factor was treatment (nicotinamide-treated, progesterone 10-treated, progesterone 20-treated, vehicle, and sham-injured) and the within-group factor was day of testing. Both the main effects and the interaction effects were considered. Huynh-Feldt correction and Tukey's Honestly Significant Different test (Tukey's HSD) were used to control for type I error in the repeated measures and post-hoc means comparison, respectively. Planned comparisons using a t-test were performed when the interaction effects were not significant, in order to examine differences in performance on each test in the MWM. A significance level of p≤.05 was used for all statistical analyses.
A one-way ANOVA was completed where the between-subject factor of treatment (nicotinamide-treated, progesterone 10-treated, progesterone 20-treated, vehicle, and sham) was used to analyze the anatomical data. Tukey's HSD was used to control for type I error and a significance level of p≤.05 was used for all statistical analyses. Inter-rater reliability measures were evaluated using the bivariate correlation of scores obtained between the two raters.
Results
Reference memory acquisition
In the reference memory task, the latency to reach the platform was averaged over the four trials for each testing day during reference memory acquisition. The animal's latencies to reach the platform were evaluated using repeated measures ANOVA, with the within-subjects factor of day (20, 21, and 22) and the between-subjects factor of treatment (nicotinamide-treated, progesterone-10-treated, progesterone-20-treated, vehicle-injured, and sham). The interaction of day×treatment was not significant (F [8, 78]=1.32, p=0.25). Both the main effect of day (F [2, 78]=61.37, p<0.001) and treatment (F [4, 39]=8.83, p<0.001) were significant, see Figure 1. Given the lack of an interaction, planned comparisons were performed and showed that there were significant differences among the groups on post-CCI day 20. The comparison of the progesterone-10-treated group to the vehicle group was significant (t [16]=2.19, p<0.04). The nicotinamide-treated group was also significantly different than the vehicle group (t [16]=2.16, p<0.05]); however, the progesterone-20 group was not (p>0.05). On day 21, post-CCI planned comparisons also showed that there were significant differences between progesterone-10-treated group and the vehicle group (t [16]=4.50, p<0.001), and that the nicotinamide-treated group was also significantly different than the vehicle group (t [16]=5.35, p<0.001); however, the progesterone-20 group was not (p>0.05). On the last day of reference memory testing, the planned comparisons also showed that there was a significant difference between the nicotinamide-treated group and the vehicle group (t [16]=3.23, p<0.005); however, the progesterone-10-treated and progesterone-20 group comparisons to vehicle were not significant (p>0.05).
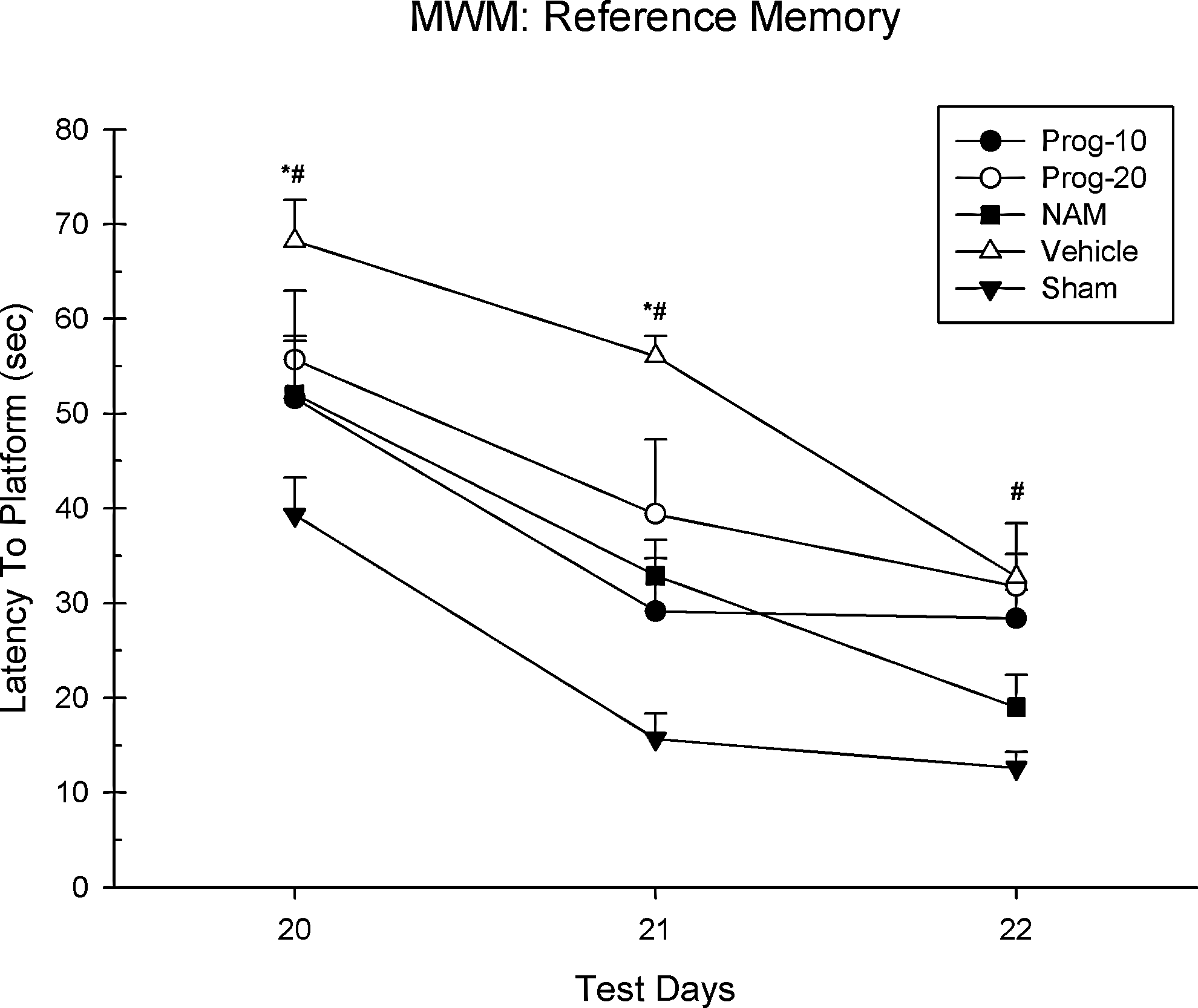
Morris Water Maze: Reference Learning. The average latency (+SEM) to reach the platform for the reference learning phase (days 20–22) (* represents significant differences [p<0.05] between the progesterone-10 and vehicle-injured group; # represents significant differences [p<0.05] between the nicotinamide [NAM] and vehicle-injured group).
Reversal learning
In the reversal learning task, the latencies to reach the platform were averaged over the four trials on day 26 post-CCI. The animal's latencies to reach the platform were evaluated using one-way ANOVA with a between-subjects factor of treatment (nicotinamide-treated, progesterone-10-treated, progesterone-20-treated, vehicle-injured, and sham). There were significant differences among the groups (F [4, 39]=9.94, p<0.001). Post-hoc analysis indicated that the progesterone-10-treated group (HSD [16]=22.90, p<0.001) and the nicotinamide-treated group (HSD [16]=19.48, p<0.01) performed significantly better than the vehicle-injured group. However, the progesterone-20-treated group showed no significant improvement compared with the vehicle-injured group (HSD [16]=16.60, p>0.05), see Figure 2.
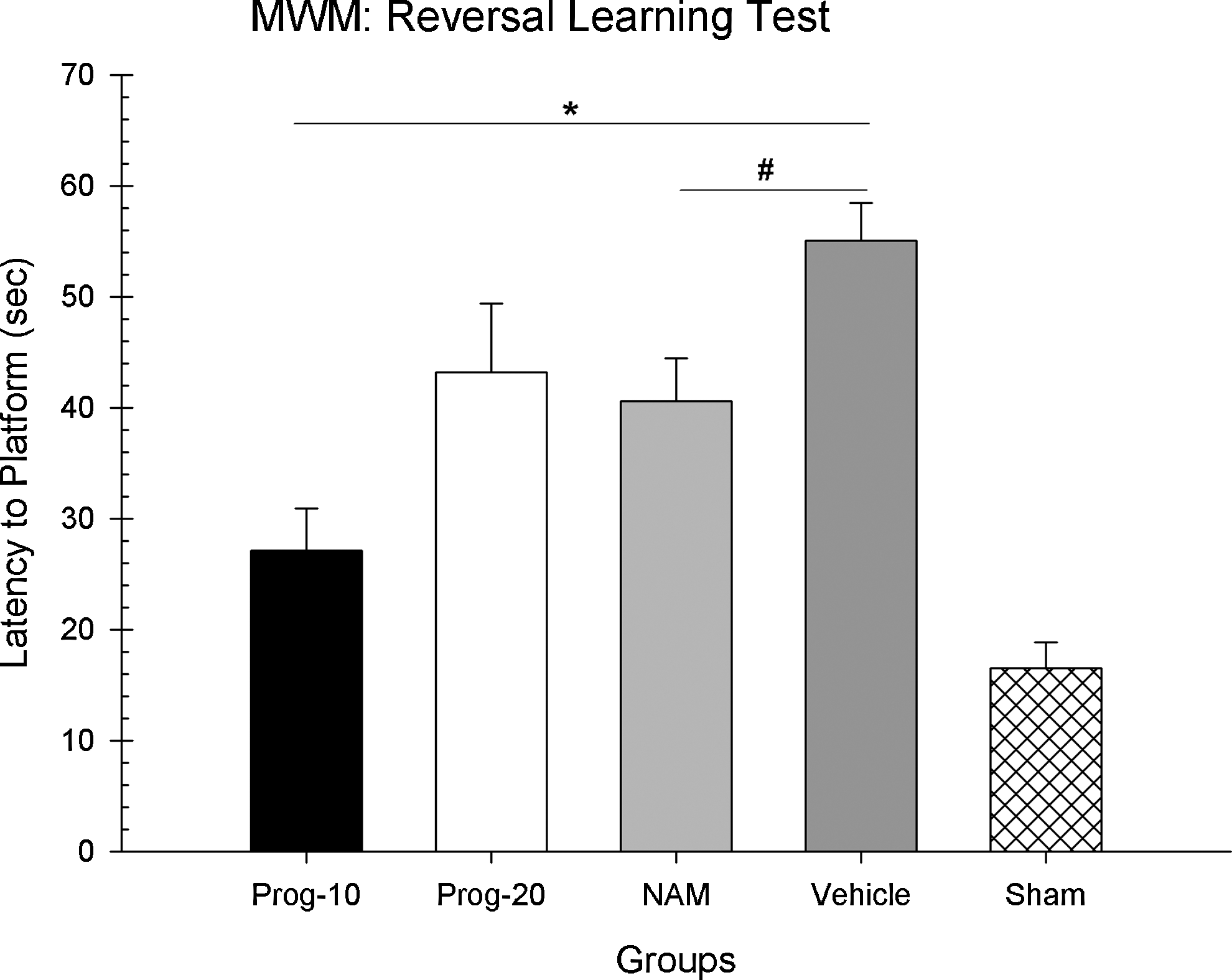
Morris Water Maze: Reversal Learning Test. The average latency (+SEM) to reach the platform on day 26 (*represents significant differences [p<0.05] between the progesterone-10 and vehicle-injured group; # represents significant differences [p<0.05] between the nicotinamide [NAM] and vehicle-injured group).
Lesion analyses
The ratio of lesion volume in the cortices was compared in a one-way ANOVA (group [nicotinamide-treated, progesterone-10-treated, progesterone-20-treated, vehicle-injured, and sham]). There was a significant difference among the groups (F [4,39]=9.47, p<0.001). Post-hoc analysis showed that the progesterone-10-treated group (HSD [16]=11.93, p<0.04) and the nicotinamide-treated group (HSD [16]=12.23, p<0.03) had a significantly greater reduction in cortical volume loss compared with the vehicle-injured group. Additionally, the progesterone-20-treated group did not show a significant reduction of cortical volume loss compared with the vehicle-injured group (HSD [16]=7.73, p>0.05), (Fig. 3A). Inter-rater reliability calculations of cortical volume showed a positive correlation (r=0.910, n=10, p<0.001).

Lesion Analysis.
The ratio of lesion volume in the hippocampus was also compared in a one-way ANOVA (group [nicotinamide-treated, progesterone-10-treated, progesterone-20-treated, vehicle-injured, and sham]). There was a significant difference among the groups (F [4, 39]=8.68, p<0.001). The progesterone-10-treated group (HSD [16]=23.37, p<0.01) and the nicotinamide-treated group (HSD [16]=20.24, p<0.04) had a significantly reduction in hippocampal volume loss compared with the vehicle-injured group. Additionally, the progesterone-20-treated group did not show a significant reduction of hippocampal volume loss compared with the vehicle-injured group (HSD [16]=4.28, p>0.05) (Fig. 3B). Inter-rater reliability calculations showed a positive correlation of hippocampal volumes (r=0.967, n=10, p<0.001). See Figure 4 for representative lesion images for the experimental groups.

Histology Plate. Representative images of cresyl violet stained tissue throughout the injury coordinates; −0.08 mm, −1.8 mm, −2.8 mm, and −3.8 mm, relative to bregma. Scale bar=2.0 mm.
Serum analyses
In the present study, the loading dose of nicotinamide (75 mg/kg, i.p.) at 4 h post-CCI combined with 3 days of contiguous infusion (12 mg/kg, s.c.) resulted in a mean serum level of 107 μg/mL (SEM=5.5 μg/mL) when sampled 72 h post-CCI. The low dose (10 mg/kg, i.p.) progesterone treatment regimen beginning at 4 h post-CCI with repeated administration every 12 h for 3 days resulted in a mean serum level of 71 ng/mL (SEM=3.3 ng/mL) when sampled at 72 h post-CCI. The high dose regimen of progesterone (20 mg/kg, i.p.) resulted in a mean serum level of 146 ng/mL (SEM=11.3 ng/mL) when sampled at 72 h post-CCI (Fig. 5).
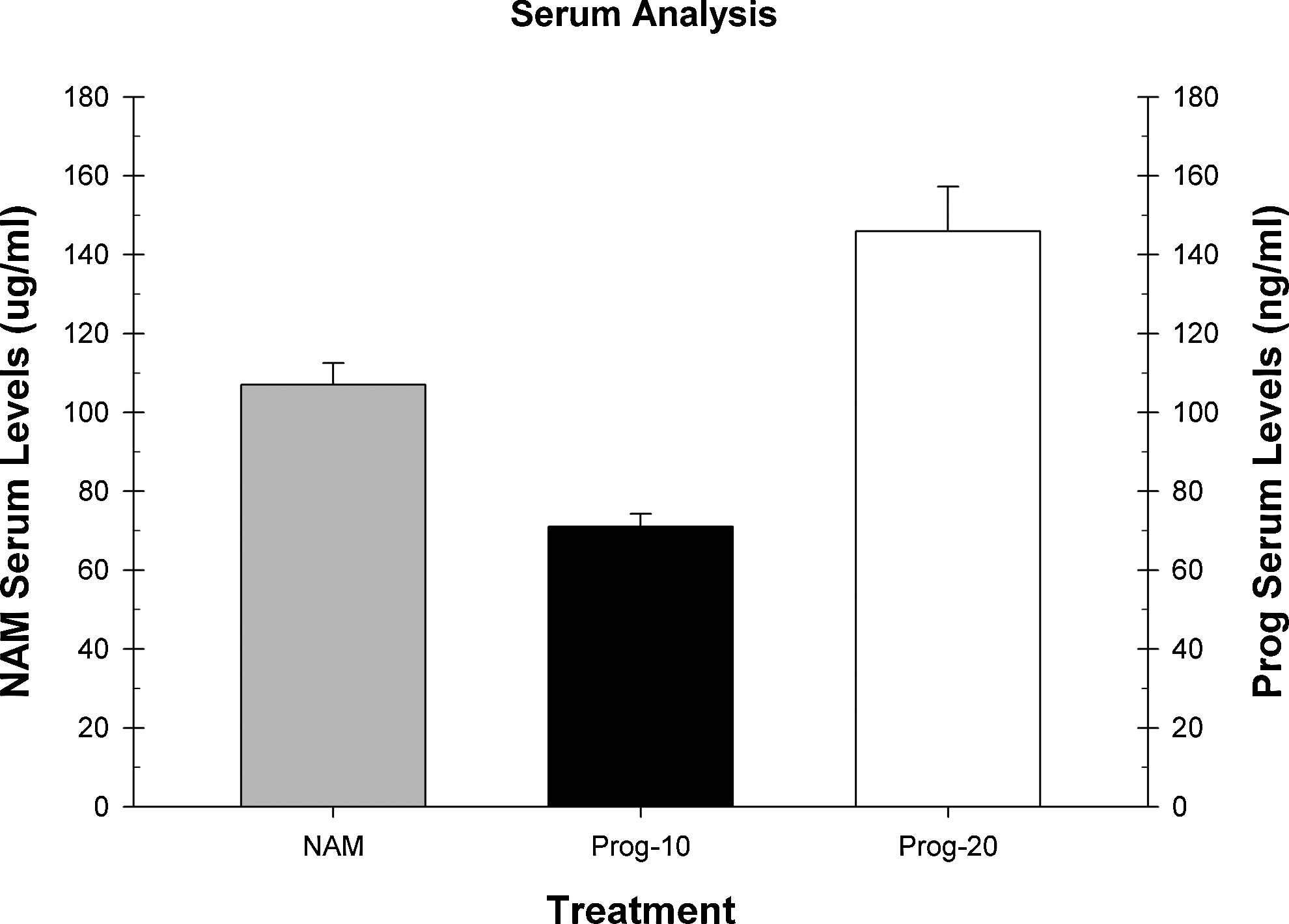
Serum Analysis. The average serum levels for nicotinamide and progesterone are shown for the corresponding treatment group.
Discussion
A plethora of pre-clinical studies are performed each year for drug discovery in TBI; however, very few, if any, of these studies directly compare the effectiveness of these therapies with each other within the same animal model paradigm. The goal of this study was to directly compare the pre-clinical efficacy of nicotinamide and progesterone therapies with each other, following CCI in the rat. Initial pharmacokinetic studies were employed to determine the optimal dosing of nicotinamide 30 and progesterone. 23 Specifically, the dosing regimen in the present study aimed to compare nicotinamide (75 mg/kg, i.p. loading dose, followed by continuous infusion 12 mg/kg/h, s.c. over 72 h) with progesterone (10 mg/kg, i.p. or 20 mg/kg, i.p .over 72 h) with all treatments starting 4 h post-injury. As expected, the various dosing regimens of nicotinamide and progesterone raised serum levels accordingly based on the particular dose administered. Therefore, it can be assumed that therapeutic levels of the drug were maintained during the treatment window of 72 h post-CCI.
The therapeutic benefits of nicotinamide in the present study replicated effects from previous studies with young animals following CCI or FPI. 4,7,8,11,12 Nicotinamide resulted in significant improvements in reference memory acquisition in the MWM when tested beginning 20 days post-TBI compared with the vehicle group. In addition, a significant improvement in an MWM reversal learning task was also seen when performed on day 26 post-CCI. The nicotinamide therapy also significantly reduced tissue loss in the ipsilateral cortex at the site of injury and in the underlying hippocampal formation compared with vehicle treatment. The only study not to find a therapeutic benefit with nicotinamide was one that examined a different dosing regimen in middle-aged rats. 31
The progesterone behavioral data analyses revealed that the 10 mg/kg dose of progesterone provided the greatest level of improvement on the reference memory task compared with the 20 mg/kg dose. The lower dose of progesterone also improved performance to a greater extent on the reversal learning task and was significantly different compared with vehicle treatment, whereas the high dose of progesterone was not significantly different from vehicle. The lower dose also provided a significant reduction in cortical and hippocampal loss compared with vehicle, which the higher dose failed to do. In general, our data suggest that the lower dose of progesterone studied here (10 mg/kg) outperformed the higher dose (20 mg/kg). As can be seen in the data, the high dose of progesterone had a much greater level of variability than the other treatments, and this resulted in the diminished treatment effect. In general, it is likely that the greater variability in neuroprotection in the cortex and hippocampus, provided by the high dose of progesterone, produced this reduced efficacy. It is unlikely that the 20 mg/kg dose produced any detrimental side effects, because these are generally shown with much higher doses. In addition, our serum analysis indicates that the high dose did hit our intended steady state and was proportionally increased compared with the low dose. This effect is generally supported in the literature, which shows that lower doses of progesterone generally have higher rates of efficacy than do higher doses. 21,22
Mechanistically, administration of nicotinamide is a potentially effective treatment because it protects against the neurotoxic effects of poly ADP-ribose polymerase (PARP), is a precursor of a cellular energy source nicotinanide adenine dinucleotide (NAD), and is a potent free radical scavenger. 32 A recent mechanistic review noted that the beneficial mechanistic effects of nicotinamide are through numerous pathways. 33 Nicotinamide is also an antioxidant, can block pro-inflammatory cytokines, and supports cellular energy sources through its promotion of NAD synthesis. In comparison, mechanistically for progesterone, it has been shown that the effects on inflammation reduction, swelling, and apoptosis have been proposed to be caused by regulation of gene transcription, the modulation of neurotransmitter receptors, and the activation of signaling cascades. 34 Progesterone has been shown previously to modulate the activity of neurotransmitters, including positive modulation of gamma-aminobutyric acid type A (GABAA) receptors, primarily by allopregnanolone, the active metabolite of progesterone. 35 Progesterone has also been shown to protect against lipid membrane peroxidation in an experimental TBI model 36 and to attenuate the production of the pro-inflammatory cytokines, interleukin (IL)-1β and tumor necrosis factor (TNF)α after TBI when given 1 h and 6 h after injury. 37
We have recently published a gene expression profiling study of progesterone therapy that examined the changes in gene expression at 24 h, 3 days, and 7 days post-CCI with the same doses examined in the present study. 23 At 24 h, the effect of low dose progesterone on differentially expressed genes was <20% the effect of higher dose compared with vehicle. Gene ontology (GO) analyses identified a significant effect of low and high dose progesterone treatment compared with vehicle on DNA damage response. At 72 h, high dose progesterone treatment compared with vehicle affected expression of almost twice as many genes as did low dose progesterone. Both low and high dose progesterone resulted in expression of genes regulating inflammatory response and apoptosis. At 7 days, there was only a modest difference in high dose progesterone compared with vehicle, with only 14 differentially expressed genes. In contrast, low dose progesterone resulted in 551 differentially expressed genes compared with vehicle. GO analysis identified genes for the low dose treatment involved in positive regulation of cell proliferation, innate immune response, positive regulation of anti-apoptosis, and blood vessel remodeling. Additionally, we have taken this same approach to examine the effect of nicotinamide on gene expression following CCI. 30 In general, treatment with nicotinamide resulted in significant effects on expression of genes involved in the immune and inflammatory processes and various signaling pathways. Despite similar efficacy with low dose progesterone and nicotinamide, there were noticeably different effects of treatment on gene expression. In general, nicotinamide treatment primarily counteracted gene expression changes caused by the TBI, where treatment downregulated genes that were significantly upregulated in the injured, vehicle-treated animals compared with sham. In contrast, progesterone treatment primarily affected genes that were not differently expressed in the TBI injured animals. 23
The direct comparison of nicotinamide to progesterone in the present study revealed that the low dose of progesterone and nicotinamide provided similar levels of therapeutic benefit on both behavioral measures and anatomical measures. Nicotinamide also provided improved efficacy compared with the high dose of progesterone. The low dose of progesterone also produced significant benefits compared with the high dose. Therefore, at least when examined within this CCI model of rodent TBI, nicotinamide and low dose progesterone provide similar degrees of pre-clinical efficacy. In addition, based on the reported mechanistic actions of nicotinamide 33 and progesterone in the literature, combined with our two recent gene expression studies with these compounds, it appears that these two treatments might make an excellent polytherapy for TBI. Future work is planned that will examine the pre-clinical efficacy of a polytherapy of progesterone and nicotinamide within the CCI and FPI models of rodent TBI. However, this does not preclude the examination of other potential pre-clinical therapies.
Footnotes
Acknowledgments
The authors thank Jacob Ward and Mahala Logue for their assistance on this project. The research was supported by a grant from the National Institutes of Health/National Institute of Child, Health, and Development (R01 HD061944-01).
Author Disclosure Statement
No competing financial interests exist.