
Abstract
The pathophysiology of traumatic brain injury (TBI) is complex and not well understood. Because pathophysiology has ramifications for injury progression and outcome, we sought to identify metabolic cascades that are altered after acute human mild and severe TBI. Because catabolism of branched-chain amino acids (BCAAs; i.e., valine, isoleucine, and leucine) leads to glucose and energy metabolism, and neurotransmitter synthesis and availability, we investigated BCAA metabolites in plasma samples collected within 24 h of injury from mild TBI (Glasgow Coma Scale [GCS] score >12), severe TBI (GCS ≤8), orthopedic injury, and healthy volunteers. We report decreased levels of all three BCAAs in patients with mild TBI relative to healthy volunteers, while these BCAAs levels in patients with severe TBI were further reduced compared with all groups. Orthopedic patients exhibited reductions in BCAA comparable to those in patients with mild TBI. The decrease in patients with mild and severe TBI persisted for derivatives of BCAA catabolic intermediates. Only plasma levels of methylglutarylcarnitine, a derivative of a leucine metabolite, were increased in patients with severe TBI compared with all other groups. Notably, logistic regression combination of three BCAA metabolites whose levels were changed by 24 h post-injury provided prognostic value (area under the curve=0.92) in identifying patients with severe TBI in whom elevated intracranial pressure (≥25 mm Hg) developed. These changes suggest alteration of BCAA metabolism after TBI may contribute to decreased energy production and neurotransmitter synthesis and may contribute to TBI pathophysiology. Supplementation of BCAAs and/or their metabolites may reduce TBI pathology and improve outcome.
Introduction
V
The brain is extremely sensitive to shifts in cellular metabolism, because it has a high metabolic rate and does not store glucose. Both clinical and experimental studies have reported that the injured brain undergoes a metabolic crisis—an acute period of enhanced glucose utilization followed by a sustained period of reduced glucose utilization. 2 –6 Because of the importance of BCAAs in energy metabolism and neurotransmitter synthesis, experimental studies have supplemented BCAAs after moderate-severe traumatic brain injury (TBI) 7,8 and have observed improved cognitive outcome. A study by Aquilani and associates 9 reported that BCAAs supplement in patients with severe TBI may improve outcome from a vegetative or minimally conscious state. However, a recent study reports that increased plasma levels of isoleucine and leucine were associated with increased intracranial pressure (ICP) and decreased cerebral oxygen consumption. 10 While these are interesting results, it has not been determined if human TBI alters BCAA metabolism and whether the extent of alterations is related to injury severity.
Thus, in this study, we measured plasma levels of the BCAAs and their metabolites in patients with either mild (Glasgow Coma Scale [GCS] score >12) or severe (GCS ≤8) TBI within 24 h of injury and compared with that of healthy volunteers (HV) and patients with orthopedic injury. Patients with mild TBI had decreased levels of valine, isoleucine, and leucine relative to HV, while BCAA levels in patients with severe TBI were further reduced compared with all groups. The decrease in patients with mild and severe TBI persisted for derivatives of BCAAs catabolic intermediates. Only plasma levels of methylglutarylcarnitine, a metabolite of leucine used to help diagnose lyase deficiencies, were increased in patients with severe TBI compared with all other groups. The levels of three BCAA metabolites, combined by logistic regression, were an excellent prognostic predictor of subsequent elevated ICP in patients with severe TBI.
Methods
Recruitment and sample collection
The Committee for the Protection of Human Subjects at The University of Texas Health Science Center at Houston approved the human subjects protocol in accordance with the Declaration of Helsinki. In total, 73 participants were recruited and consented for the study, which included 18 with mild TBI, 20 with severe TBI, 15 with orthopedic injury, and 20 HV. All were between 14–62 years of age, had no other known inflammatory process or active infection, no known history of psychiatric disorders necessitating hospitalization, or alcohol or drug dependency, and provided informed consent or proxy consent. HV with no significant medical history, fever, or recent history of orthopedic injury or head injury consented to a one-time blood sample donation. All other participants provided a blood sample within 24 h of injury.
Patients with mild TBI had non-penetrating trauma manifesting in one or more of the following: loss of consciousness, post-traumatic amnesia, altered mental status, focal neurologic deficits, or seizure. Patients with mild TBI had a GCS score >12 and were excluded if they had abnormalities on a head CT scan other than contusion, operative lesions, or expected length of hospital stay of greater than 48 h. Patients with severe TBI had GCS scores ≤8 and non-penetrating TBI necessitating placement of an ICP monitor for clinical care. ICP was measured continuously from the time of monitor placement. Elevated ICP was defined as a ≥25 mm Hg measurement for at least 5 min that occurred either twice in a 24-h period or on two consecutive days, whereas no ICP elevation was defined as <25 mm Hg throughout the 5-day period. Orthopedic injury patients required a radiographically confirmed fracture and no head trauma.
Blood samples, coded to maintain confidentiality, were obtained at the earliest possible time after presentation, patient stabilization, and informed consent. Relevant medical data were recorded and coded to match the extracted blood sample, which was collected in K2EDTA tubes (Becton Dickinson, Franklin Lakes, NJ), placed on ice, and processed within an hour. Plasma was isolated by centrifugation at 4°C as described by the vendor. Aliquots were prepared and frozen at −80°C until needed.
Patient assessments and classifications
Data were collected on several physiological scoring systems to classify injury and the level of treatment patients received: Acute Physiology and Chronic Health Evaluation II (APACHE II), GCS, injury severity score (ISS), and therapeutic intensity level (TIL). APACHE II is designed to measure the severity of disease for newly admitted intensive care unit (ICU) patients; 11 to calculate APACHE II, we collected the worst value of each of its components within the first 24 h of ICU admission. GCS is a standard, brief neurological assessment of response to stimuli for eye opening, verbal and motor criteria routinely used in clinical care and neurosurgical research. 12 All injuries were classified according to body region and given an abbreviated injury score (AIS) from 1 to 6 according to the established definition. The worst three AIS scores in different body regions were squared and summed to calculate the ISS. The ISS correlates linearly with mortality, morbidity, length of hospital stay, and other measures of injury severity. 13
Sample preparation
Sample preparation was conducted by Metabolon, Inc. (Durham, NC) using a proprietary series of organic and aqueous extractions to remove the protein fraction while allowing maximum recovery of small molecules. The resulting extract was divided into two fractions—one for analysis by liquid chromatography (LC) and one for analysis by gas chromatography (GC), both followed by mass spectrometry (MS). Samples were placed briefly on a TurboVap® (Caliper Technologies Corp., Hopkinton, MA) to remove the organic solvent. Each sample was then frozen and dried under vacuum.
Sample analysis
BCAAs and their metabolites were identified by comparison with library entries of purified standards or recurrent unknown entities. The combination of chromatographic properties and mass spectra gave an indication of a match to the specific compound or an isobaric entity. For quality assurance/quality control purposes, a number of additional samples were included with each day's analysis. Further, a selection of quality control compounds was added to every sample, including those under test. These compounds were carefully chosen so as not to interfere with the measurement of the endogenous compounds. Relative levels of each metabolite were quantified using Metabolon's proprietary peak integration software. The integrated peak values from all participants were averaged and used for normalizing the values for each participant.
Receiver operator characteristic (ROC) analysis
Sigma Stat was used to generate ROC curves and to calculate area under the curve (AUC). Sensitivity (defined as true positives/[true positives+false negatives]) was calculated using values for metabolites measured in samples obtained from patients with severe TBI with subsequent ICP elevation (ICP ≥25 mm Hg). Specificity (defined as true negatives/[true negatives+false positives]) was calculated using values for metabolites measured in samples obtained from severe TBI patients without subsequent ICP elevation (ICP <25 mm Hg). Sensitivity and specificity were calculated at various cutoff values and plotted as sensitivity vs. 1-specificity. The area under the resultant curve was calculated and used as a measure of diagnostic accuracy of the biomarker to correctly classify patients based on their ICP status. To find a biomarker signature predictive of future ICP status, plasma levels of BCAAs and their metabolites were included in a logistic regression with stepwise removal of poor predictors until maximum predictability was obtained. These were subjected to ROC analysis.
Statistical analysis
Data were initially evaluated using a Shapiro-Wilk normality test, followed by a one-way analysis of variance (ANOVA) across the four subject groups. Any data found to not have a normal distribution were analyzed using a Kruskal-Wallis ANOVA on ranks. Groups with differences were identified using a Dunn pairwise comparison as the post-hoc test. Differences were considered significant at p<0.05, with groups with altered levels identified using critical p values calculated after compensation for multiple comparisons.
Results
We measured the levels of BCAAs and their key metabolites in the plasma of patients with mild (GCS score >12) or severe (GCS ≤8) TBI within 24 h of their injury. Plasma samples used as controls were obtained from HV and patients with orthopedic injury but no indication of head trauma. Table 1 presents the demographic, injury mode, and clinical data for the participants. The mean age of participants for each group did not significantly differ, nor were any differences determined in their height, weight, or racial composition. Patients with severe TBI had significantly worse GCS scores (first 24 h) and ISS compared with all other groups. The worst recorded GCS score (within the first 24 h) did not differ between the mild TBI and orthopedic injury groups.
TBI, traumatic brain injury; NR, not recorded; GCS, Glasgow Coma Scale; NA, not applicable; ISS, injury severity score; TIL, therapeutic intensity level; APACHE II, Acute Physiology and Chronic Health Evaluation II. Values in mean±standard deviation.
The summary of our plasma BCAA metabolite measurements is depicted in Figure 1. BCAAs and their metabolites whose levels decreased after TBI are shown in red, increased shown in green, and unchanged shown in blue. Metabolites listed in black were not measured.

Branched-chain amino acid metabolic pathways. (
When the plasma level of valine was assessed in the four groups, a significant change was detected across groups (F=16.76, df=3, p<0.001). Post-hoc analysis revealed that levels of valine were significantly decreased in the group with mild TBI compared with those observed in HV, but not compared with persons with orthopedic injuries (Fig. 2A). A further reduction in valine levels was detected in plasma of patients with severe TBI compared with all other groups examined. While the plasma levels of 3-methyl-2-oxobutyrate, the direct metabolite of valine, did not differ across groups (Fig. 2B), its metabolite's derivative, isobutyrylcarnitine, did differ across groups (one-way ANOVA on ranks: H=31.06, df=3, p<0.001). Isobutyrylcarnitine was significantly decreased in the plasma of patients with severe TBI relative to all other groups (Fig. 2C).
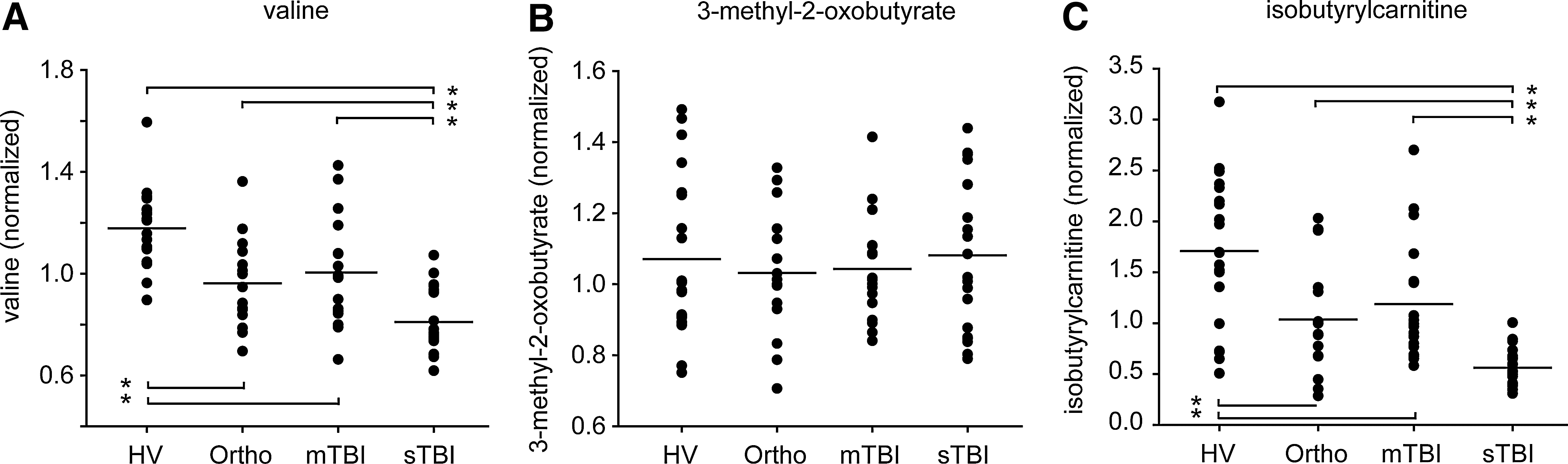
Relative plasma levels of valine (
We found both the levels of isoleucine (F=22.46) and its keto acid metabolite, 3-methyl-2-oxovalerate (F=14.98, both df=3, p<0.001), were significantly different across groups. Analogous to changes in valine, isoleucine and 3-methyl-2-oxovalerate levels were reduced in patients with mild TBI compared with HV (Figs. 3A, 3B, respectively). These decreases were more pronounced in patients with severe TBI, resulting in a significant difference compared with all other groups examined. Measurement of 2-methylbutyrylcarnitine showed its plasma levels to be significantly decreased in patients with severe TBI compared with patients with mild TBI and HV (one-way ANOVA on ranks: H=23.39, df=3, p<0.001, Fig. 3C). The levels of the breakdown product of tiglyl-CoA, tiglylcarnitine, did not differ across groups (Fig. 3D).

Relative plasma levels of isoleucine (
Valine and isoleucine degradation both generate propionyl-CoA and subsequently succinyl-CoA, the latter of which participates in both gluconeogenesis and the citric acid cycle for the production of glucose and energy, respectively. We therefore measured the derivatives of propionyl-CoA and succinyl-CoA and found their plasma levels to differ across cohorts. Uniquely differentiating all groups, propionylcarnitine (F=21.70, df=3, p<0.001) was significantly reduced in each patient cadre compared with HV, yet more so in patients with severe TBI than the other groups, and orthopedic injury more than patients with mild TBI (Fig. 4A). Succinylcarnitine (one-way ANOVA on ranks: H=10.97, df=3, p<0.001) only differed with a decrease in severe TBI compared with orthopedic injury patients (Fig. 4B).

Relative plasma levels of propionylcarnitine (
Plasma levels of leucine were different across groups (F=13.17, df=3, p<0.001), decreased in patients with severe TBI compared with patients with mild TBI and HV, but not orthopedic injury patients. Similar to the other BCAAs, leucine was also decreased in orthopedic patients and patients with mild TBI compared with HV (Fig. 5A). Leucine's keto acid, 4-methyl-2-oxopentanoate, was decreased in patients with severe TBI and orthopedic injury compared with HV (F=6.58, df=3, p<0.001, Fig. 5B). Isovalerylcarnitine was found to be significantly different across groups (one-way ANOVA on ranks: H=29.17, df=3, p<0.001), with the levels of this isovaleryl-CoA derivative significantly reduced in the plasma of patients with severe TBI (Fig. 5C). A reduction in hydroxyisovaleryl carnitine was found exclusively in patients with severe TBI compared with HV (one-way ANOVA on ranks: H=11.19, df=3, p<0.001, Fig. 5D). In contrast to the levels of all BCAAs and their metabolites, plasma methylglutarylcarnitine was found to be significantly increased in patients with severe TBI compared with the three other groups (one-way ANOVA on ranks: H=25.27, df=3, p<0.001, Fig. 5E).

Relative plasma levels of leucine (
Previously, the circulating levels of valine, isoleucine, and leucine were found to be significantly reduced during the first week after injury in patients with severe TBI. Further, a significant relationship between plasma levels of isoleucine and leucine and ICP value was detected. 10 Because our samples were collected within the first 24 h, and ICP elevations (≥25 mm Hg) in our patients with severe TBI were not observed until 48 h post-injury, we questioned if the plasma levels of these BCAAs (or any of their metabolites) can predict the future presence or absence of elevated ICP (for demographic and clinical data of these patients by ICP status, see Jeter et al., 2012). 14 ROC curves of isoleucine and leucine showed their plasma levels to be poor predictors of future ICP elevation, with AUC of 0.71 and 0.54, respectively. While no other individual metabolite's AUC was valuable in predicting forthcoming elevated ICP (Table 2), a logistic regression analysis of the levels of propionylcarnitine, 2-methylbutyrylcarnitine, and 4-methyl-2-oxopentanoate resulted in an excellent prognostic biomarker signature for subsequent ICP elevation (AUC=0.92; Fig. 6).

Plasma levels of propionylcarnitine, 2-methylbutyrylcarnitine, and 4-methyl-2-oxopentanoate combine to differentiate those patients with severe TBI in whom elevated intracranial pressure (ICP) (≥25 mm Hg) later developed from those in whom it did not (ICP <25 mm Hg), as shown by a receiver operator characteristic (ROC) curve, proving the biomarker signature to have excellent prognostic value. AUC, area under the curve.
AUC, area under the curve.
Discussion
BCAAs are essential amino acids and have important roles in energy metabolism and protein and neurotransmitter synthesis (Fig. 1). Alterations in their circulating levels are observed in neurological disorders such as Huntington's disease, amyotrophic lateral sclerosis, and severe brain injury. 10,15,16 Measurement of valine, isoleucine, and leucine and their metabolites in patients with TBI generated three key findings: (1) The plasma levels of all three BCAAs and specific metabolites (in red in Fig. 1) were found to be reduced in the plasma of the group with severe TBI compared with HV and orthopedic groups. Only plasma levels of methylglutarylcarnitine were increased after severe TBI. (2) The circulating levels of valine, isoleucine, and leucine, and several of their key metabolites were significantly reduced in patients with mild TBI compared with HV, although to a lesser degree than that seen acutely after severe TBI. (3) The circulating BCAA levels in the plasma of persons with orthopedic injuries were reduced compared with HV, and these reductions were comparable to levels measured in mild TBI samples. Because BCAAs participate in a number of important cellular and metabolic processes, our findings suggest that supplementation of these amino acids may be of behavioral and cognitive benefit not only to patients with severe TBI as suggested by Aquilani and colleagues, 9 but also to patients with mild TBI and orthopedic injury.
It has been reported recently that patients with severe TBI have reduced levels of valine, isoleucine, and leucine in their bloodstream for at least 1 week after injury. 10 In agreement with these findings, our measurements indicated significant reductions in these three amino acids within the first 24 h (in red in Fig. 1). We further demonstrate that these reductions are not restricted to severe forms of injury, but, to a lesser degree, can also be observed in patients with mild TBI. The extents of reduction are comparable to those with orthopedic injuries. In addition to decreases in the plasma levels of the BCAAs, we measured eleven metabolites of these amino acids. Of these, three of the eight metabolites found to be decreased in the plasma of patients with severe TBI were also found to be reduced after mild TBI. While the reason for the reductions of BCAA metabolism in patients with TBI is not known at present, breakdown of all three BCAAs involves the same two initial enzymatic steps: reversible transamination by branched-chain aminotransferase (BCAT) and irreversible dehydrogenation by branched-chain α-keto acid dehydrogenase (BCKDH). Thus, it is not surprising that the catabolism and, thus, plasma levels of valine, isoleucine, and leucine and their metabolites correlate with one another. 17
As essential amino acids, BCAAs must be obtained from the diet. The majority of ingested BCAAs bypass hepatic metabolism and enter the bloodstream, raising the possibility that the effects we observed may be related to differences in the period of fasting between the different groups examined. The reported time since last meal before sample collection, however, only differed slightly across groups (mild TBI, 7.6±4.63 h; orthopedic injury, 10.41±5.13 h). Although patients with severe TBI were comatose on hospitalization and could not report time since last meal, we estimate the time as similar to the other injury groups based on time of injury to time of sample acquisition. Fasting HV confirmed no oral intake for greater than 8 h (18/20; 2 with unknown time of last meal).
None of the patients in the current study received total parenteral nutrition, and enteral feeding was started for our patients with severe TBI on day 3.16±0.71, beyond the sample collection time. Although we cannot rule out differences in gut absorption, it does not appear that the time since last meal was a dictating factor in the results we observed. This is consistent with the conclusion offered by Vuille-Dit-Bille and colleagues, 10 whose sample collection in patients with severe TBI and HV was performed after periods of overnight fasting.
A caveat of the present study is that BCAAs and their metabolite levels were measured in blood plasma, not the injured brain tissue, making it difficult to directly implicate these changes in TBI pathology. Experimental studies using a rodent model of TBI, however, have found that the levels of valine, isoleucine, and leucine are decreased in the injured brain. 8 This is consistent with previous reports that have shown the dietary supplementation (or restriction) of BCAAs changes not only the plasma levels of these amino acids, but their concentrations in the brain as well. 1
Although a direct link between plasma BCAAs levels and altered brain function cannot be concluded from the present study, several mechanisms have been identified that support this possibility. BCAAs are transported across the blood-brain barrier by transporters located on the luminal surface of capillary endothelial cells. 1 These transporters also regulate the entry of large neutral amino acids (LNAAs), such as tryptophan, tyrosine, and phenylalanine, 18 and are almost fully saturated at normal serum amino acid concentrations. 19 It has been suggested that decreases in the levels of plasma BCAAs can increase the uptake and brain concentrations of LNAAs, thereby increasing serotonin (from tryptophan) and catecholamine (from phenylalanine and tyrosine) synthesis. 20,21 Excesses in these neurotransmitters have been proposed to underlie some of the behavioral and cognitive dysfunctions associated with phenylketonuria, bipolar disorder, and schizophrenia. 22 –24 In addition to altering the levels of these modulatory neurotransmitters, lowered brain levels of leucine may cause reductions in the synthesis of the excitatory neurotransmitter glutamate. Using radiolabeled BCAAs, it has been estimated that approximately 50% of the glutamate present in the brain is derived from leucine. 25 Although glutamate excitotoxicity is a feature of acute TBI pathophysiology, glutamate plays an essential role in synaptic activity and plasticity, and long-term reductions in its synthesis could contribute to cognitive and behavioral abnormalities.
In addition to their possible influences on neurotransmitter levels, BCAAs have been shown to play key roles in energy production by glucogenic (valine and isoleucine) and ketogenic (leucine and isoleucine) pathways. Leucine catabolism, for example, has been demonstrated to provide an endogenous supply of oxidatively produced energy to replace glucose in the brain. 26 Because a prolonged period of metabolic suppression has been observed after moderate-severe TBI, 6,27 reductions in plasma BCAA levels may compromise the ability of the injured brain to use this alternate energy source.
Interestingly, the leucine catabolic product methylglutarylcarnitine was the only metabolite we found to be increased in plasma levels of patients with severe TBI. Accumulation of this metabolite also occurs in HMG-Co lyase deficiency, a rare disease resulting in the inability to process leucine or produce ketones. 28 Thus, our paradoxical increase of plasma methylglutarylcarnitine is in line with reduced availability of ketogenic energy sources after severe brain injury. Further, it is possible that BCAA levels, specifically leucine, can indirectly affect metabolism in the brain through leucine-mediated insulin production. 29 Insulin can cross the blood-brain barrier to facilitate glucose utilization, 30 and various brain areas 31,32 and genes encoding metabolic enzymes 32 have been demonstrated to be sensitive to insulin.
One mechanism important to consider is that our observed decrease in plasma BCAAs, especially in patients with severe TBI, may be indicative of increased BCAA utilization in the brain, thereby exacerbating TBI-associated glutamate excitotoxicity. Recent glutamate-sensitive microelectrode studies have shown a persistent increase in brain extracellular glutamate levels in the fluid percussion injured rat brain, apparent after mild to moderate injury and even more pronounced after moderate to severe TBI. 34 While this would suggest that BCAA supplementation could be deleterious, our results suggest that BCAAs supplementation may be a potential avenue for therapeutic intervention.
In support of this conclusion, dietary BCAA supplementation has been evaluated for its safety and efficacy in neurological disorders such as phenylketonuria, mania, schizophrenia, and severe TBI. 7,35 –37 For example, BCAAs (60 g) administered daily for 7 days was found to significantly reduce the occurrence of manic symptomology, an effect thought to be because of a reduction in brain catecholamine synthesis. 38 In patients with TBI, intravenous infusion of BCAAs for 15 days after admission to the rehabilitation department prompted more than two-thirds of patients with severe TBI to exit a posttraumatic vegetative or minimally conscious state, as measured by the Disability Rating Scale, compared with none in the control group. 9 Similarly, cognitive benefits have been observed in patients with severe TBI not in a vegetative state treated with BCAAs supplementation, 7 as well as in mice subjected to experimental brain injury. 8 While these studies support the use of BCAAs as potential therapeutics, dose-response studies will be critical because elevations in BCAAs levels in HV have been associated with cognitive dysfunction, as measured using a spatial recognition memory task. 39
Elevated ICP is a major contributor to morbidity and mortality associated with TBI. A recent study reported that plasma levels of isoleucine and leucine in patients with severe TBI are correlated with ICP value. 10 The value of these BCAAs in predicting subsequent ICP elevation, however, has not been examined. In the present study, the levels of these amino acids were also found to decrease in the first 24 h in severe TBI samples, but were found to have poor prognostic value in identifying those patients at risk for development of elevated ICP (Table 2). When we investigated the predictive power of BCAA metabolites, however, a biomarker signature of propionylcarnitine, 2-methylbutyrylcarnitine, and 4-methyl-2-oxopentanoate was an excellent prognostic indicator of future ICP increase. Propionylcarnitine can be associated with acute hepatic encephalopathy, which confers a propensity for increases in ICP, 40 with the latter metabolites linked to BCAA metabolic disorders. 41,42 Whereas these metabolites are not routinely assessed in current clinical practice, our data motivate the development of a new test as a means of detecting and preemptively treating ICP elevation.
Conclusion
This metabolomic profiling study showed that the circulating levels of BCAAs and their major metabolites are decreased as a result of brain injury. Of particular interest is the observation that these changes could be observed in patients with mild TBI, suggesting that BCAA supplementation may attenuate some symptoms. Future studies will be needed to establish a link between the reductions in BCAAs levels and cognitive dysfunction, with the hope that identification of the causal pathways may help in the design of personalized therapies such as normalizing the levels of individual BCAAs or specific metabolites to pre-injury levels to treat associated TBI symptoms and improve outcome.
Footnotes
Acknowledgments
We would like to thank the nurses at Memorial Hermann Hospital-Texas Medical Center and Elizabeth B. Jones, MD, Toby T. Thomas, MD, and Brad Jacobson, MD, for assistance with recruiting patients. This study was supported by the Health Resources and Services Administration (R38OT10585), Mission Connect/TIRR Foundation, The Vivian L. Smith Foundation, and the Gilson-Longenbaugh Foundation.
Author Disclosure Statement
No competing financial interests exist.