
Abstract
Mild traumatic brain injury (mTBI) has gained considerable notoriety during the past decade of conflict in Afghanistan and Iraq. However, the relationship between combat-related mTBI and residual mTBI symptoms, post-traumatic stress disorder (PTSD) symptoms, and neurocognitive deficits remains unclear. The purpose of the study was to compare residual mTBI and PTSD symptoms, and neurocognitive deficits among U.S. Army Special Operations Command (USASOC) personnel with diagnosed blunt, blast, and blast–blunt combination mTBIs. This study involved a retrospective medical records review of 27,169 USASOC personnel who completed a military version of the Immediate Post-Concussion Assessment Cognitive Test (ImPACT), Post-Concussion Symptom Scale (PCSS), and PTSD Checklist (PCL) between November 2009 and December 2011. Of the 22,203 personnel who met criteria for the study, 2,813 (12.7%) had a diagnosis of at least one mTBI. A total of 28% (n=410) of USASOC personnel with a history of diagnosed mTBI reported clinical levels of PTSD symptoms. Personnel with a history of diagnosed blunt (OR=3.58), blast (OR=4.23) or combination (OR=5.73) mTBI were at significantly (p=0.001) greater risk of reporting clinical levels of PTSD symptoms than those with no history of mTBI. A dose-response gradient for exposure to blast/combination mTBI on clinical levels of PTSD symptoms was also significant (p=0.001). Individuals with blast/combination mTBIs scored higher in residual mTBI (p=0.001) and PTSD symptoms (p=0.001), and performed worse on tests of visual memory (p=0.001), and reaction time (p=0.001) than those with blunt or no mTBI history. Individuals with combination mTBIs scored lower in verbal memory (p=0.02) than those with blunt mTBIs. Residual PTSD and mTBI symptoms appear to be more prevalent in personnel with blast mTBI. A dose-response gradient for blast mTBI and symptoms suggests that repeated exposures to these injuries may have lingering effects.
Introduction
P
The lifetime prevalence for mTBI in U.S. military personnel is estimated to be 19.5%. 5 Mild traumatic brain injuries result in acute functional symptoms that include headaches, memory loss, confusion, fogginess, dizziness, coordination problems, sleep disturbances, and motor and neurocognitive impairments, 6 and are similar to the sequelae observed in sport-related concussion. 7 Computerized neurocognitive assessment represents one tool in a comprehensive approach to mTBI management that includes symptom assessments, clinical evaluation, and balance and vestibular assessment. This testing allows for the individualized management of mTBIs by comparing post-concussion neurocognitive performance and symptom reporting to baseline levels.
Sport-related mTBIs typically resolve within 7–10 days when appropriately managed. 7 In sport populations, if mTBIs are managed improperly or the athlete has certain risk factors (e.g., history of mTBI), long-term sequelae such as an increased risk for another mTBI 8 or post-concussion syndrome (PCS) 9 may result. Similarly in military populations mTBIs have been associated with post-traumatic stress disorder (PTSD). 10 PTSD symptoms are reported to occur acutely in up to 40% of U.S. military personnel following an mTBI. 10 These symptoms may also persist, as 42% of recent Afghanistan and Iraq veterans with a history of mTBI concurrently report PTSD symptoms. 11
The presence of PTSD-related symptoms following an mTBI can be attributed to one or more underlying causes: 1) pre-morbid PTSD symptom levels, 2) co-morbid PTSD symptoms from simultaneous traumatic events (e.g., explosion, exposure to death/loss) or injury, 12 3) direct structural damage to the brain (i.e., amygdala, hippocampus, and medial pre-frontal cortex) with simultaneous disruption of serotonergic pathways, 13 and 4) post-injury frustration and anxiety from uncertain recovery. 14 Peripheral exposure to blast forces with concomitant fogginess, dizziness, and headaches is often unreported by soldiers and may be a contributing factor to the subsequent development of PTSD. 15 The pathophysiology of a pure blast injury without acceleration or penetration appears to be different than a pure blunt injury in animal models and involves functional changes in brain cells. 16 In contrast to blast injuries, blunt injuries involve a direct mechanical impact to the skull (e.g., blunt weapon, flying debris, violent impact with ground, vehicle, or other structure) with subsequent force displacement in the brain. The rapid force acceleration or deceleration on the brain from a blunt impact may result in axonal shearing, contusion, and intracranial hemorrhage. Blast–blunt combination injuries involve two or more of the aforementioned injury mechanisms.
Post-traumatic stress disorder symptoms are also influenced by age, 17 sex, 18 and mTBI history. 10,11 Additionally, deployment status (i.e., combat personnel, support personnel, state-side) and length of deployment may influence PTSD symptoms among military personnel (Mental Health Advisory Team-IV (MHAT), 2006. 19 Although researchers 20,21 have examined the biomechanical forces associated with blast and blunt injuries and effects on the brain in animal models, little is known about the relationship of each type of injury to PTSD symptoms among U.S. military personnel.
The purpose of this study was to examine the relationship between blunt, blast, and blast–blunt combination mTBIs and residual mTBI symptoms, clinical and subclinical PTSD symptoms, and neurocognitive performance deficits among USASOC personnel. This population includes Special Forces “Green Berets,” Army Rangers, and other unconventional units involved in high-risk training, multifaceted global operations, and challenging combat missions. We hypothesized that personnel previously exposed to blunt, blast, or combination mTBIs would be at greater risk for clinical levels of PTSD symptoms, report higher levels of mTBI and subclinical PTSD symptoms, and score lower on neurocognitive performance testing than those not exposed to these injuries.
The type of event that leads to an mTBI may also influence the development of PTSD symptoms. 10 Mild traumatic brain injuries resulting from high-energy and more-intense traumatic events such as those accompanying an IED blast are more likely to result in PTSD symptoms than low-energy and less-intense traumatic events such as falls. Therefore, we expected that PTSD scores would be higher and neurocognitive scores would be lower for personnel exposed to blast and combination mTBIs when compared to those exposed to blunt mTBIs. We also anticipated a dose-response gradient for exposure to blast and combination mTBIs for risk of clinical levels of PTSD, as well as mTBI and subclinical PTSD symptoms, and neurocognitive performance.
Methods
From November 1, 2009 to December 31, 2011, a total of 27,169 USASOC personnel (representing all available USASOC personnel) completed web-based, standardized baseline evaluations for mTBI symptoms, PTSD symptoms, and neurocognitive performance; however, only 22,203 met study inclusion criteria. Individuals were excluded from the study if they had a history of diagnosed moderate to severe TBI, brain surgery, major psychiatric disorder, or neurological disorder. Additionally, any individual whose neurocognitive assessment was deemed invalid based on a score on any test composite lower than 2 SDs below the total sample mean or per the manufacturer's criterion (i.e., Impulse Control score > 20) was also removed from the study. Consequently, a total of 4,966 (18.3%) of the original 27,169 personnel were excluded from this study. The resultant population of 22,203 represented a response rate of 81.7%, and was comprised of 21,294 (95.9%) males and 909 (4.1%) females, with a mean age of the 29.52±6.84 years.
A military version of the Immediate Post-Concussion Assessment Cognitive Test (ImPACT) was used to assess neurocognitive performance. The neurocognitive assessment is comprised of six modules: 1) verbal memory, 2) design memory, 3) X's and O's, 4) symbol matching, 5) color matching, and 6) three-letter memory. These six neurocognitive assessment modules are collapsed into four composite scores for verbal memory, visual memory, visual motor processing speed, and reaction time (RT). It is important to note that both RT and motor visual processing speed scores in the military version of ImPACT vary slightly from those in the civilian/sport version. As such, the data from these two composite scores cannot be directly compared to those from studies involving civilian/sport populations. In addition to the neurocognitive component, the military version of the ImPACT test comprised the following: 1) a demographic section, 2) the Post-Concussion Symptom Scale (PCSS), and 3) the PTSD Checklist (PCL). Demographic data include age, sex, migraine history, deployment status, testing location, military rank, and military occupational specialty. The Post-Concussion Symptom Scale (PCSS) contains 22 self-report symptoms rated on a 0 (none) to 6 (severe) point Likert scale. The PCL encompasses 17 items and requires individuals to indicate on a scale of 1 (not at all) to 5 (extremely) how much each item bothered them during the past month. The PCL yields a PTSD symptom score that ranges from 17 to 85.
This study was approved under exempt de-identified medical records review protocols by both the University of Pittsburgh and Womack Army Medical Center institutional review boards for human subject research. Each study participant individually completed the web-based military version of the PCSS, PCL, and ImPACT tests. Although the parameters of the preceding computerized assessment test remained the same throughout the study, multiple deployed and nondeployed testing sites dictated some environmental variability. However, all designated testing rooms were supervised and located in the quietest areas available.
For data analysis, the independent variable was exposure to diagnosed blast, blunt, or blast–blunt combination mTBI. For the current study, an mTBI is defined as a head injury with a Glasgow Coma Scale (GCS) score of 13–15 and no associated pathology identified through common neuroimaging techniques (i.e., CT, MRI). Personnel studied were divided into four mutually exclusive groups based on history of mTBI diagnosis since joining the military: 1) blunt mTBI (at least 1 blunt with no blast or combination), 2) blast mTBI (at least 1 blast with no combination), 3) combination mTBI (at least 1 combination), and 4) no mTBI. Any mTBIs incurred prior to joining the military were not included in the analyses in the current study. Additionally, a dose-response gradient (i.e., significant increase in symptoms or decrease in neurocognitive performance with each additional exposure level) was investigated by comparing individuals with 0, 1, 2, and 3+ blast and/or combination mTBIs. For this dose-response gradient, it is important to note that the “none” group included individuals with a history of diagnosed blunt mTBI. Dependent variables were test scores from the PCSS, PCL, and ImPACT. A series of ANOVAs with Bonferroni correction for multiple comparisons was used to compare and contrast test scores in the context of diagnosed mTBI history. Chi-square and odds ratio (OR) analyses were used to compare clinical levels of PTSD symptoms in the mTBI groups and blast dose-response groups. Data were analyzed using SPSS, version 19, IBM. Statistical significance was set at a Bonferroni-corrected p<0.01.
Results
Of the 22,203 personnel in the study, 19,390 (87.3%) had no history of diagnosed mTBI, and 2,813 (12.7%) had a diagnosis of at least one mTBI. Of those with at least one diagnosed mTBI, 1,700 (7.7%) were from blunt trauma, 861 (3.9%) were from blasts, and 252 (1.1%) resulted from a blast–blunt combination. A total of 1476 (6.6%) of USASOC personnel in the current study reported clinical levels of PTSD symptoms (i.e., total PCL score ≥28). Approximately 28% (n=410) of individuals reporting clinical levels of PTSD symptoms also had a history of diagnosed mTBI. Within mTBI exposure groups, 10.4% (n=177) of individuals with blunt, 19.7% (n=170) of those with blast, and 25% of those with combination mTBI reported clinical levels of PTSD symptoms.
Residual mTBI symptoms, PTSD symptoms, and neurocognitive performance results are depicted in Table 1. Individuals with a history of diagnosed blast and blast–blunt combination mTBI reported more mTBI symptoms (F[3; 22,203]=271.85, p=0.001, η2 =0.04) and PTSD symptoms (F[3; 22,203]=297.47, p=0.001, η2 =0.04) than subjects with a history of diagnosed blunt or no mTBI. Individuals with a history of diagnosed blunt mTBI reported more mTBI and PTSD symptoms than those with no history of diagnosed mTBI. Individuals with a history of diagnosed blast and blast–blunt combination mTBI performed worse on visual memory (F[3; 22,203]=13.27, p=0.001, η2 =0.01) and reaction time (F[3; 22,203]=11.59, p=0.001, η2 =0.01) than those with a history of diagnosed blunt mTBI and those with no mTBI history. Subjects with a history of diagnosed blast–blunt combination mTBI performed worse on verbal memory (F[3; 22,203]=3.33, p=0.02, η2 =0.01) and visual motor processing speed (F[3; 22,203]=10.72, p=0.001, η2 =0.01) than those with a history of diagnosed blunt mTBI. Subjects with a history of diagnosed blunt mTBI performed better on visual memory, visual motor processing speed, and reaction time than those with no mTBI history.
p<0.05, ** p<0.001.
different from no history, bdifferent from blunt mTBI, cdifferent from blast mTBI.
A comparison of subjects with a history of 0, 1, 2, and 3+ diagnosed blast (including both blast and blast–blunt combination) mTBIs supported a dose-response gradient for reported mTBI symptoms (F[3; 22,203]=209.04, p=0.001, η2 =0.03) and PTSD symptoms (F[3; 22,203]=224.73, p=0.001, η2 =0.03). Specifically, both mTBI and PTSD symptom scores increased significantly with each increase in exposure to diagnosed blast mTBI (Fig. 1 and 2). For neurocognitive performance, a dose-response gradient was not supported by verbal memory (F[3; 22,203]=2.47, p=0.06, η2 =0.001), visual memory (F[3; 22,203]=0.66, p=0.58, η2 =0.001), or visual processing speed (F[3; 22,203]=1.27, p=0.28, η2 =0.001); however, individuals with a history of 3+ diagnosed blast mTBIs had slower reaction time than those with no history of diagnosed blast mTBI (F[3; 22,203]=3.98, p=0.008, η2 =0.001) (Table 2).

Total baseline mTBI symptoms reported for blast exposure groups. Total mTBI symptom scale ranges from 0 to 132. Upper error bars represent standard deviation for each group.
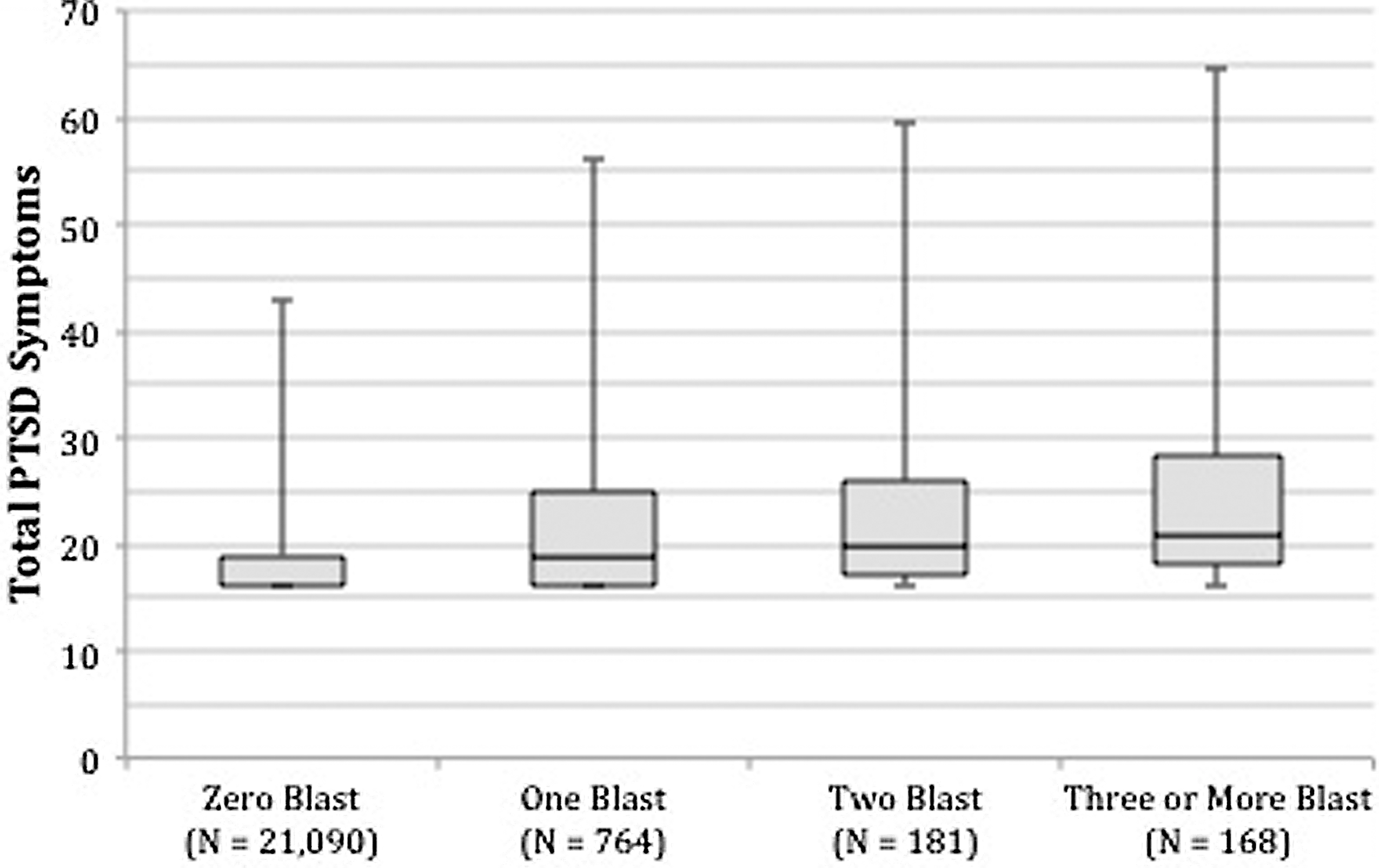
Total baseline PTSD symptoms reported for blast exposure groups. PTSD symptom scores on the PCL range from 17 to 85. Upper error bars represent standard deviation for each group.
p<0.05, adifferent from no history.
The results of the chi-square and OR analyses supported significant differences in clinical levels of PTSD symptoms for blunt, blast, and combination mTBI exposure groups (Table 3). Specifically, the blunt mTBI group was at 3.6×, the blast mTBI group was at 4.2×, and the combination mTBI group was at 5.7× greater risk for clinical levels of PTSD symptoms than the group without a history of mTBI. In addition, the blast mTBI group was at 2.1× greater risk than the blunt mTBI group to present with clinical levels of PTSD symptoms. The combination mTBI group was at 2.9× greater risk than the blunt mTBI group and 1.4× greater risk than the blast mTBI group for clinical levels of PTSD symptoms. The results of the chi-square and odds ratio analyses for the dose-response gradient for blast and combination mTBI also supported significant differences in clinical levels of PTSD symptoms (Table 4). Specifically, the 1 blast/combination mTBI group was at 3.7×, the 2 blast/combination mTBI group was at 4.8×, and the 3+ blast/combination mTBI group was at 6.4× greater risk for clinical levels of PTSD symptoms than the no blast mTBI group. In addition, the 3+ blast/combination mTBI group was at 1.7× greater risk than the 1 blast/combination mTBI group for clinical significant PTSD.
Discussion
In the current study, approximately 28% of USASOC personnel with a history of diagnosed mTBI reported clinical levels of PTSD. This number is lower than the 44% of Army infantry personnel with an mTBI involving loss of consciousness that met clinical PTSD criteria as reported by Hoge et al. 10 The current findings indicate that USASOC personnel with a history of diagnosed blunt (OR=3.58), blast (OR=4.23), or combination (OR=5.73) mTBI were at significantly greater risk of reporting clinical levels of PTSD symptoms than those with no history of mTBI. Not surprisingly, the differences between the mTBI groups were progressive in nature, with those suffering blast mTBI at 2.1× greater risk for clinical levels of PTSD symptoms than blunt, and the combination group at 2.9× greater risk than blunt and 1.4× greater risk than blast. These findings may reflect the more dramatic and stressful nature of the injury mechanism (e.g., IED explosion) and environment (e.g., combat) associated with blast and combination mTBIs. In contrast, blunt mTBIs in military personnel may occur during training and recreational activities or from falls and accidents. The results also supported in part a dose-response gradient for blast exposure and increased risk of clinical levels of PTSD symptoms. A significant increase in risk for clinical levels of PTSD symptoms was associated with increased exposure to blast and combination mTBI in this sample. In fact, USASOC personnel exposed to 3+ blast or combination mTBIs were nearly twice as likely as those with only one exposure to have clinical levels of PTSD symptoms. Interestingly, the results suggest that exposure to 1 or 2 blast or combination mTBIs was not significantly different in regard to risk for clinical levels of PTSD symptoms.
The results of our study also support a link between blunt, blast, and combination blast–blunt mechanisms and residual mTBI symptoms and subclinical PTSD symptoms among USASOC personnel. More pronounced effects for mTBI and subclinical PTSD symptoms are associated with blast and combination blast–blunt mTBI, suggesting that these injuries affect either deeper cortical structures or involve more significant shearing of neurons resulting in more residual effects. The findings also support a dose-response gradient for blast mTBI and mTBI and subclinical PTSD symptoms, similar to that reported in the sports medicine literature. For example, athletes with a history of mTBI are at an increased risk for sustaining subsequent mTBIs, as well as for slowed recovery of self reported post concussion signs and symptoms, and cognitive and balance impairments. 22
By convention, the preface word “mild” in mTBI represents a degree of acute brain dysfunction that occurs immediately following a blunt, blast, or combined blast–blunt trauma. The term “mild” is misleading and can inadvertently prompt a neglect of care acutely and exacerbate the degree and duration of chronic sequelae. 6,23 Residual effects of mTBI are poorly understood and can exist even when standard neurological exams, structural neuroimaging, and electroencephalograph (EEG) are all within normal limits. In addition, residual effects of mTBI are often unrecognized, undocumented, under reported, or inadvertently misdiagnosed as purely psychological in etiology. In our study, 12.7% of USASOC personnel reported a history of at least one diagnosed mTBI. Previous reports by Tanielian and Jaycox 5 indicated that the lifetime prevalence rate for self-reported mTBI among United States military associated with deployments in Iraq and Afghanistan was 19.5%. However, when accounting for co-morbid disorders, the TBI-only prevalence rate in the Tanielian and Jaycox 5 study was only 12.2%, which is comparable to the rate reported in our study. 5
An absence of pathology on standard diagnostic testing (i.e., MRI, CT, EEG) combined with vague and inconclusive postconcussive and post-traumatic stress symptoms can prove misleading to many providers. The natural tendency to create a divergence between mTBI and PTSD in order to provide a singular and definitive diagnosis is also a confounder. As symptoms can overlap, this effort can prove futile. In addition to neurocognitive performance deficits noted in memory and concentration, soldiers can experience a wide range of dysfunction to include anhedonia, irritability, depression, anxiety, substance abuse, fatigue, and sleep disturbances. This unique military version of the ImPACT may prove useful as a tool for providers to distinguish between PTSD unrelated to or associated with head trauma. To meet criteria using the PCL, the Veteran's Association suggests using cut-off scores of 56 in specialty mental health clinics and 28 for active use for recent veterans of combat in Afghanistan and Iraq (National Center for PTSD). 24
In our study, it appears that there is also a link between PCL scores and mTBI symptoms. This finding is in contrast to previous research, which has reported that postconcussive symptoms are more associated with PTSD and depression than with a concussive injury. 10 Although the mean PCL scores in our study did not meet the cut-off for PTSD, the difference between soldiers reporting PTSD symptoms with and without mTBI was statistically significant. Symptoms of post-traumatic stress are an inevitable part of combat; however, they do not always manifest as pathology and a formal disorder. Therefore, it is imperative for proper identification, education, and treatment to maximize a soldier's adaptive combat stress behavior and minimize the possibility of developing dysfunctional behavior related to PTSD and/or mTBI.
It has been theorized that recurrent exposures to mTBI may contribute to residual sequelae. Residual cognitive impairments associated with increased exposure to mTBI (i.e., dose-response gradient) have been documented among former professional football players, 25,26 college athletes. 27 and high school athletes. 28 Covassin and colleagues 27 reported that a history of two or more concussions was associated with decreased neurocognitive performance in a sample of college-age athletes. Although these studies utilizing sport populations support the relationship between recurrent mTBI and decreased neurocognitive performance, other empirical reports do not supported this tenet. 29 –31 Iverson and colleagues 31 reported no differences in neurocognitive performance among groups of athletes with zero, one, or two previous concussions on neurocognitive performance. Researchers have also reported similar neurocognitive performance between athletes with and without a history of four or more sport-related mTBI. 30 However, to our knowledge, no published empirical reports outside of the present study have addressed this question in military populations.
Although the findings from the current study support a dose-response gradient for blast mTBI on both mTBI and subclinical PTSD symptoms, the effect for cognitive impairment was less pronounced and was specific to reaction time. The lack of support for residual dose-response in other cognitive domains may suggest that any cognitive deficits associated with additional exposures to blast mTBI are subtle. However, it is also possible that the deficits may be more individualized in nature, with substantial inter-individual variability based on the nature of each mTBI. The reported neurocognitive differences in this study between blast–blunt combination mTBI and blunt and no history groups supports this contention. Additional research on residual cognitive and other deficits following blast mTBI in military personnel is warranted.
Up to half of mTBIs in sport may go unreported. 32 Given the culture in which USASOC personnel train and operate, and the potential professional stigma associated with reporting mTBI, it is reasonable to assume that similar numbers of mTBIs are unreported in this population. As such, the higher cognitive scores reported among individuals with blunt mTBI compared to those with no history of mTBI in the current study may be the result of residual effects of unreported and undiagnosed mTBIs in the no history group.
It is important to note the limitations of the current study, as they may have influenced the results. Specifically, the study involved self-reported PTSD and symptoms data, which are subject to recall bias. The study was also limited by unequal group sizes, which may have affected the statistical results. Finally, although the differences in certain cognitive scores among the groups in the study were significant, they were of small magnitude.
The results of this study are novel in that they support differences in PTSD and mTBI symptoms among soldiers with history of diagnosed blunt, blast, and combination mTBIs, as well as depict a dose-response gradient for diagnosed blast-related mTBI and both PTSD and mTBI symptoms. From a clinical perspective, the findings suggest that a large percentage of soldiers with a history of diagnosed blast and combination mTBIs and those with higher exposure to blast mTBIs report clinical levels of PTSD. The results also provided tentative support for subtle cognitive differences among several of the exposure groups in the study. Identification of mTBI and associated clinical outcomes, including development of clinical and subclinical PTSD symptoms based on the mechanism of injury or exposure gradient, is critical for awareness and the development of optimal clinical practice guidelines and future treatment pathways. Future research should examine the mechanisms for the findings reported here, and the factors that might mitigate the development of residual PTSD and mTBI symptoms. Finally, research that explores the risk factors for development of clinical levels of PTSD following exposure to mTBI is also warranted.
Footnotes
Acknowledgments
The authors would like to acknowledge the contributions of Windsor D. Thompson, BSN, RN, whose time and assistance as the USASOC ImPACT program contracting officer representative was greatly appreciated.
Disclaimer: This research was funded by the U.S. Special Operations Command Biomedical Initiatives Steering Committee. The views expressed herein are those of the author(s) and do not reflect the official policy of the Department of the Army, Department of Defense, or the U.S. Government. Citations of commercial products or organizations do not constitute an official DoD endorsement or approval of the products or services of these organizations. This report was approved for public release by the U.S. Army Special Operations Command Operational Security Office and Public Affairs Office on March 27, 2012, and the U.S. Army Medical Department Public Affairs Office on March 27, 2012.
Author Disclosure Statement
No competing financial interests exist.