
Abstract
Significant cardiovascular and autonomic dysfunction occurs after spinal cord injury (SCI). It is now recognized that cardiovascular disease is a leading cause of morbidity and mortality in SCI. Patients with SCI may also suffer severe orthostatic hypotension and autonomic dysreflexia. Baroreflex sensitivity (i.e., the capability of the autonomic nervous system to detect and respond effectively to acute changes in blood pressure) has been recognized as having predictive value for cardiovascular events, as well as playing a role in effective short-term regulation of blood pressure. The purpose of this article is to review the mechanisms underlying effective baroreflex function, describe the techniques available to measure baroreflex function, and summarize the literature examining baroreflex function after SCI. Finally, we describe the potential mechanisms responsible for baroreflex dysfunction after SCI and propose future avenues for research. Briefly, although cardiovagal baroreflex function is reduced markedly in those with high-level lesions (above the T6 level), the reduction appears to be partially mitigated in those with low-level lesions. Although no studies have examined the sympathetic arm of the baroreflex in those with SCI, despite this being arguably more important to blood pressure regulation than the cardiovagal baroreflex, nine articles have examined sympathetic responses to orthostatic challenges; these findings are reviewed. Future studies are needed to describe whether dysfunctional baroreflex sensitivity after SCI is due to arterial stiffening or a neural component. Further, measurement of forearm vascular conductance and/or muscle sympathetic nerve activity is required to directly evaluate the sensitivity of the sympathetic arm of the baroreflex in those with SCI.
Introduction
The autonomic nervous system is comprised of both sympathetic and parasympathetic divisions. Parasympathetic nervous outflow occurs from cranial nerves III, VII, IX, and X superiorly, and S2–S4 inferiorly. As the cranial nerves do not transmit through the spinal cord, vagal (cranial nerve X) control of the heart rate is preserved after SCI. 4 Sympathetic nervous outflow occurs from the T1–L2 level into the sympathetic paravertebral ganglia (sympathetic chain). 8 After SCI, sympathetic control in regions below the lesion level are severely disrupted. 4 Drastic changes in cardiovascular regulation occur in those with lesion levels above the T6 spinal segment. Lesions above T6 are associated with a loss of supraspinal control over the heart and splanchnic blood vessels, 9 both of which are required for effective long- and short-term blood pressure regulation. 10
The baroreflex is a complex and multi-factorial negative feedback system that is integrated in concert with respiration and circulating blood gases. Arterial stretch receptors provide surrogate information on current blood pressure to the nucleus tractus solitarius, which then influences efferent autonomic nerve traffic. 11 This system employs both the sympathetic and parasympathetic autonomic divisions to regulate blood pressure within a narrow range over a wide variety of environmental conditions and body positions. 12 The importance of the baroreflex system to cardiovascular regulation has been supported by studies showing that when sino-aortic autonomic control is interrupted, there is an increase in blood pressure variability, as well as frequent bouts of orthostatic hypotension. 13 Cerebral oxygen delivery, which is the final common pathway leading to syncope, relies on effective blood pressure maintenance through the baroreflex (as well as cerebral autoregulation) in order to maintain sufficient cerebral blood flow. 14,15 Another case for the necessity of a functional baroreflex system can be made through evidence from evolutionary biology showing that the system (although in a more rudimentary form) is even present among the simplest vertebrates, and has a complexity similar to our own in reptiles. 16
The purpose of this review is to summarize and evaluate the current literature examining baroreflex function in those with SCI. Further, we evaluate SCI-related changes in baroreflex function in relation to lesion level, with specific emphasis on those with lesions above and below the T6 spinal segment.
Physiology of the Baroreflex
It is pertinent to first understand the normal functioning of the baroreflex in order to appreciate alterations occurring after SCI. Currently, it is well established that the baroreflex is comprised of two interdependent systems, 17,18 that work in concert as one reflex system to provide short-term regulation of blood pressure. The first, a low-pressure system, is made up of cardiopulmonary stretch receptors located in the heart and lungs, which augments sympathetic nervous system activity in response to reductions in central venous pressure and volume. 19 The second, a high-pressure baroreflex system, consists of stretch receptors located in the tunica adventitia of the aortic arch and carotid bulbs. 20 These spray-like nerve endings generate a more rapid rate of depolarization, and hence increase the frequency of action potentials in afferent nerves during periods of increased wall distension. 21 The signal is transmitted from the carotid bulb via the glossopharyngeal nerve (cranial nerve IX), and the aortic arch via the vagal nerve (cranial nerve X), to the nucleus of the solitary tract in the medulla oblongata. 11 This transmission, which provides surrogate information on systemic blood pressure, is integrated with other afferent information in order to modulate efferent nervous activity transmitted through the vagal nerve and sympathetic chain to target organs, with the aim of rapidly maintaining blood pressure at a set point. 21 Specifically, increases in blood pressure lead to increased vagal tone and sympathetic inhibition, which consequently results in decreased vascular tone, venous return, cardiac contractility, and heart rate (while the reverse actions occur in response to reductions in blood pressure). 22 Baroreflex sensitivity (BRS), describes the rate and magnitude by which the system outputs (e.g., heart rate and vasomotor tone) respond to changes in system input (e.g., blood pressure and stretch-receptor loading/unloading). 23 Thus a more sensitive baroreflex system will have more rapid and greater responses to the same change in blood pressure, and will more effectively maintain blood pressure within the desired range.
In addition to the integration of the low- and high-pressure baroreflex systems, it is important to understand that the baroreflex is integrated with chemoreflex and pulmonary afferent information in order to produce a suitable efferent response. As such, the baroreflex is influenced by both respiration and arterial blood gases. For example, inspiration decreases the cardiovagal baroreflex response, whereas the opposite is true for expiration. 24 In fact the magnitude of baroreflex resetting (adjusting blood pressure around a new set point) is related to inspiratory time, suggesting a fundamental gating relationship between baroreflex adjustment and respiration. 25 Furthermore, hypoxic peripheral chemoreflex activation leads to a resetting of both the sympathetic and parasympathetic baroreflex to a higher blood pressure, but this may or may not affect the sensitivity of the baroreflex per se. 25,26 These examples highlight that chemoreceptor, baroreceptor, and pulmonary afferent information are tightly regulated, leading to a complex interdependent relationship in which baroreceptor (and pulmonary) afferents modulate the chemoreflex influence on autonomic function. 27
The recent proliferation of studies examining baroreflex function is in large part due to clinical interest stemming from evidence showing that cardiovagal BRS holds prognostic value for cardiovascular events in a number of clinical populations. 28,29 Furthermore, long-term disruption of the cardiovagal baroreflex function has led to increases in blood pressure variability, with little or no influence on mean arterial blood pressure. 30 Resting measures of cardiovagal BRS are also relatively simple to carry out, requiring concurrent recordings of beat-to-beat blood pressure and R-R intervals. As such, the literature is disproportionally represented by studies examining the cardiovagal branch of the baroreflex. However, there is limited value of the cardiovagal branch of the baroreflex in preventing syncope or orthostatic hypotension. Although those individuals with complete autonomic failure show severe and marked reductions in blood pressure during orthostatic challenges, blood pressure responses to orthostatic challenges are similar, if not identical, before and after complete vagal efferent blockade. 30,31 Considering Poiseuille's law, blood pressure is affected to the fourth power by arterial diameter, and only linearly by increases in flow (heart rate-derived changes in cardiac output). As such, it is not surprising that the vasomotor branch of the baroreflex is much more important than the vagal branch for the maintenance of mean arterial blood pressure.
Techniques To Measure Baroreflex Sensitivity
Although it is likely impossible to study so called low-pressure or high-pressure systems in isolation, 17,18 several techniques are available to measure baroreflex function, some with considerable limitations for use in SCI. Spontaneous techniques such as 3- to 5-min recordings of resting values tend to be the most common due to inexpensive software and their non-invasive nature. Two options exist for evaluating spontaneously-occurring baroreflex function. First, cross-spectral analysis of an input and output (for example systolic blood pressure and R-R interval for cardiovagal BRS) can be evaluated in the low frequency range (0.04–0.15 Hz), with the gain and phase used to determine the sensitivity and timing of the relationship between the measures 32 (Fig. 1). The second, commonly referred to as the sequence technique, involves calculating linear regressions between spontaneously occurring changes in input and the resulting output 33 (Fig. 2). With no external perturbation of blood pressure, however, it is debatable whether resting (i.e., closed-loop) measures of arterial blood pressure are accurately detecting baroreflex function, or are the result of oscillatory influences from other factors independently influencing blood pressure and heart rate. 5

A minimum of 5-min-long recordings of resting (

From continuous recordings of (
Convincing evidence against spontaneous transfer analysis was demonstrated in a recent article by Kamiya and associates. 34 These authors used an animal model to characterize and compare the open-loop and closed-loop baroreflexes. To simulate the open-loop characteristics carotid sinus pressure (CSP) was perturbed using random white noise, thereby isolating the carotid pressure from the arterial pressure. To simulate the closed-loop characteristics the CSP was matched to the aortic pressure (AP). In both situations they simultaneously measured renal sympathetic nerve activity (SNA) and AP. This enabled them to independently examine the neural (CSP to SNA) and peripheral (CSP to AP) arcs of the baroreflex, which reflect the feedback and feedforward components of the baroreflex, respectively, as well as the total arc (neural and peripheral). In brief, their results indicated that the spontaneous baroreflex as assessed under closed-loop conditions predicted the peripheral but not the neural arc, whereas the open-loop condition could predict both. Given that the baroreflex is a feedback mechanism, they subsequently argued that the spontaneous baroreflex bore no resemblance to baroreflex function. Moreover, the lack of reliability of the spontaneous baroreflex led them to advocate the use of open-loop methods for assessing baroreflex function. In this context the open-loop methods, which involve large and dynamic perturbations of blood pressure sufficient to overcome internal noise and engage the baroreflex, are deemed a more reliable method of assessing baroreflex function. To overcome this limitation, other more invasive techniques also exist. The modified Oxford technique, for example, likely the most accurate method, involves bolus injections of phenylephrine and sodium nitroprusside to increase and then decrease blood pressure over a 2-min trial 35 (Fig. 3). Alternatively, manipulation of the carotid baroreceptors using positive and negative pressures using a modified neck collar is a non-pharmacological approach. 20,36 Both these techniques involve potential risk for the participant, including carotid stenosis rupture, and transient hypo- and hypertension. The neck cuff technique also does not allow for measurement of the aortic baroreceptors 20 (Fig. 4), although differentiation between the carotid and aortic stretch receptor afferent signals cannot be made with the Oxford technique either. Another technique to evaluate baroreflex function in an open-loop model involves using cross-spectral analysis during relatively large oscillatory blood pressure changes at 0.05 and 0.1 Hz (either by repeated squat stands or by repeated short bouts of lower body negative pressure; Fig. 5). 37 These large oscillatory perturbations of blood pressure provide similar or greater coherence between blood pressure and heart rate, but appear to show different information compared to spontaneous indicators. Specifically, reduced gain (i.e., baroreflex sensitivity) during the squat-stand maneuver suggests that feedforward mechanisms may play a role in spontaneously derived baroreflex gain. Also, enhanced gain in the 0.05-Hz frequency of perturbation compared to the faster 0.1-Hz frequency provides evidence that the cardiovagal baroreflex may be more active in mitigating blood pressure changes at specific frequencies. 37 Collectively, the lack of reliability of the spontaneous baroreflex 15,38 supports the use of open-loop methods for assessing baroreflex function. In this context the open-loop methods, which involve large and dynamic perturbations of blood pressure sufficient to overcome internal noise and engage the baroreflex, are deemed a more reliable method of assessing baroreflex function. A final way in which baroreflex sensitivity can be evaluated involves using the Valsalva maneuver. Briefly, this technique involves evaluating the blood pressure and heart rate response during phase II and IV of the maneuver. 39,40 Most commonly, Valsalva estimates of BRS involve calculating the slope between the blood pressure and heart rate changes during phase IV; 41 however, blood pressure responses during phases II and IV can help indicate vasoconstrictor effectiveness 39,40 (Fig. 6). Changes in both the sympathetic and parasympathetic wings of the autonomic nervous system can be measured using any of these techniques with simultaneous recordings of vascular resistance, or muscle sympathetic nervous system activity (MSNA) with blood pressure and heart rate. 42 These techniques can evaluate the baroreflex-mediated output response to either or both increasing (Gup) and decreasing (Gdown) blood pressure.
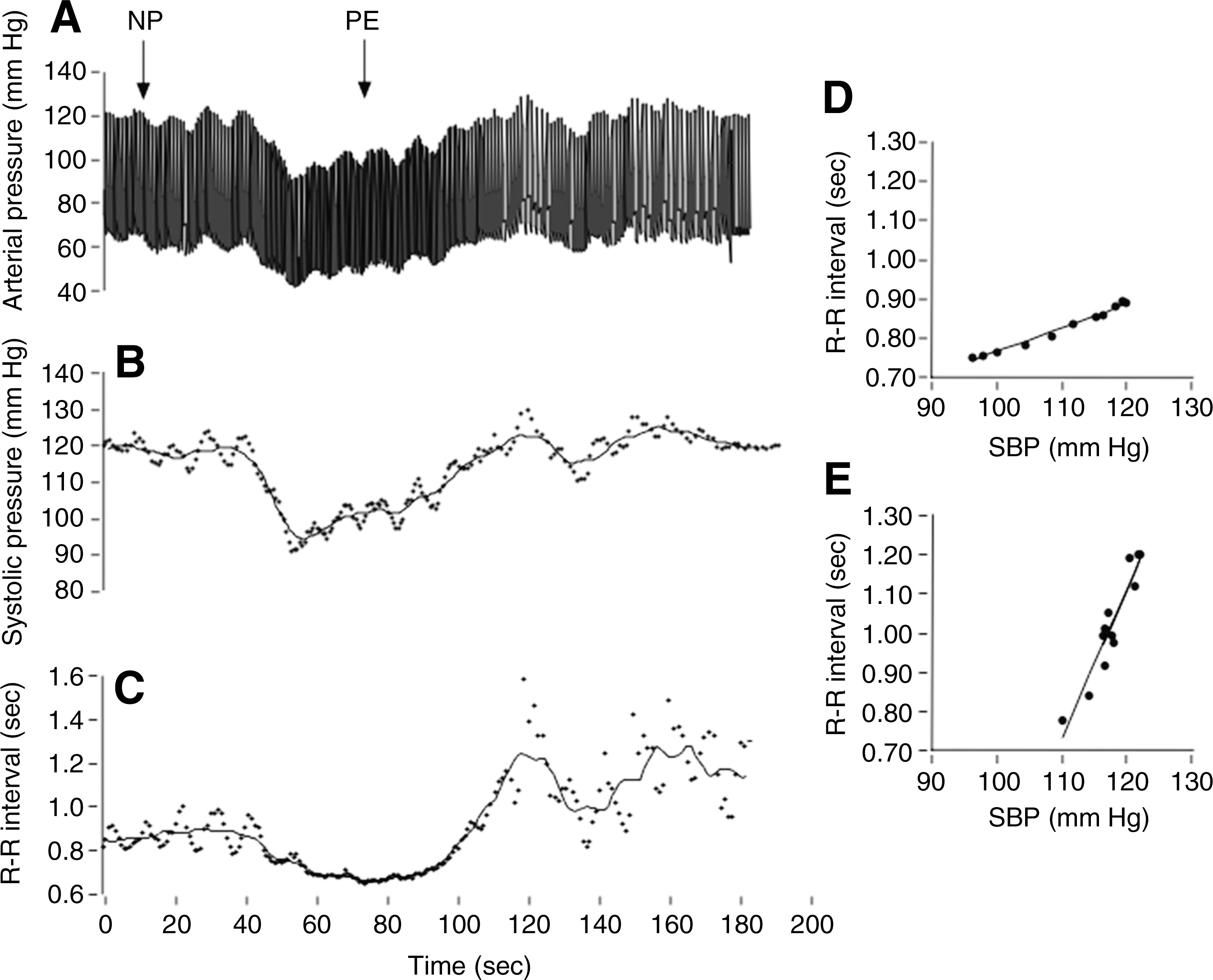
Arterial pressure (
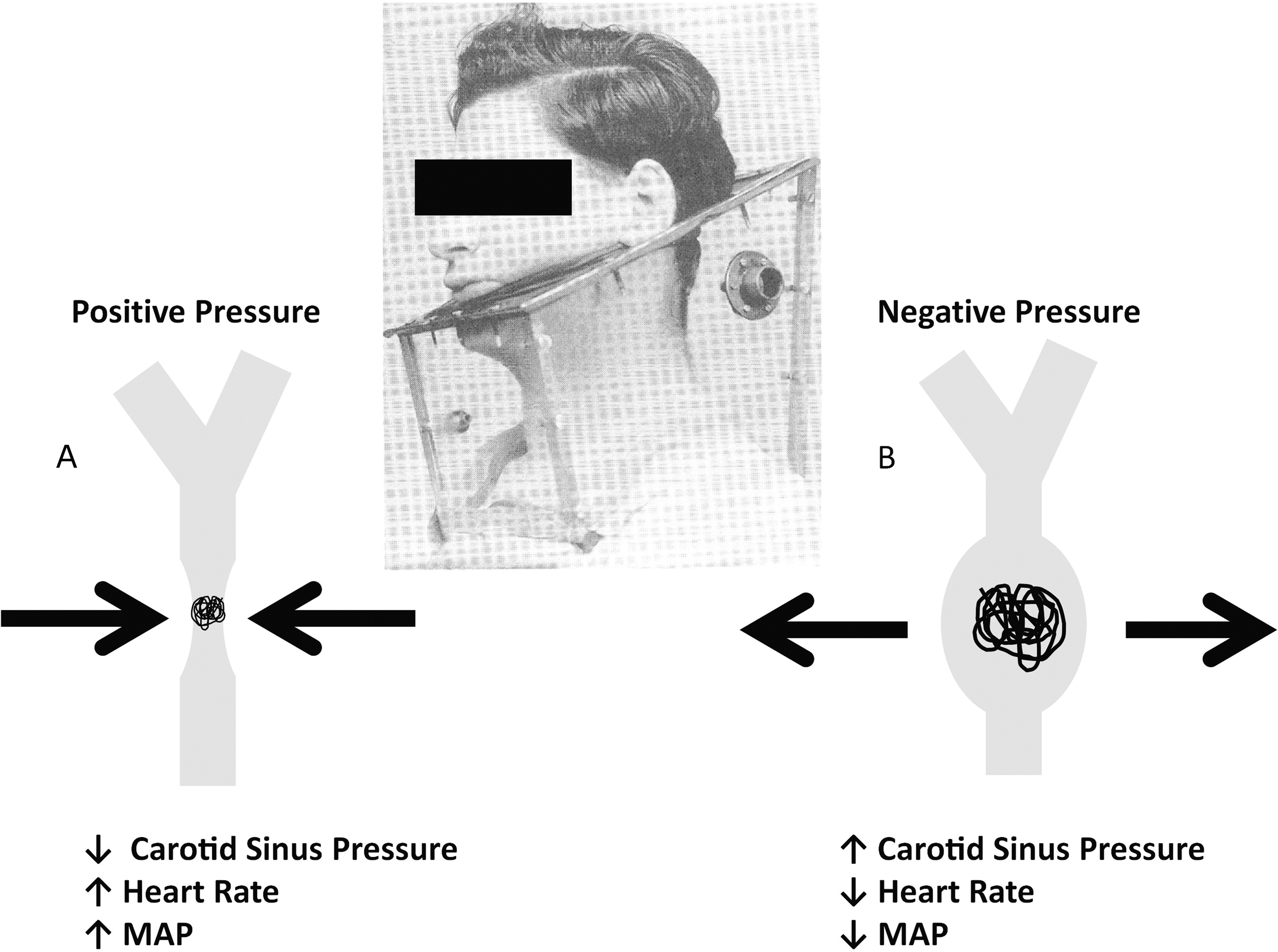
Positive (
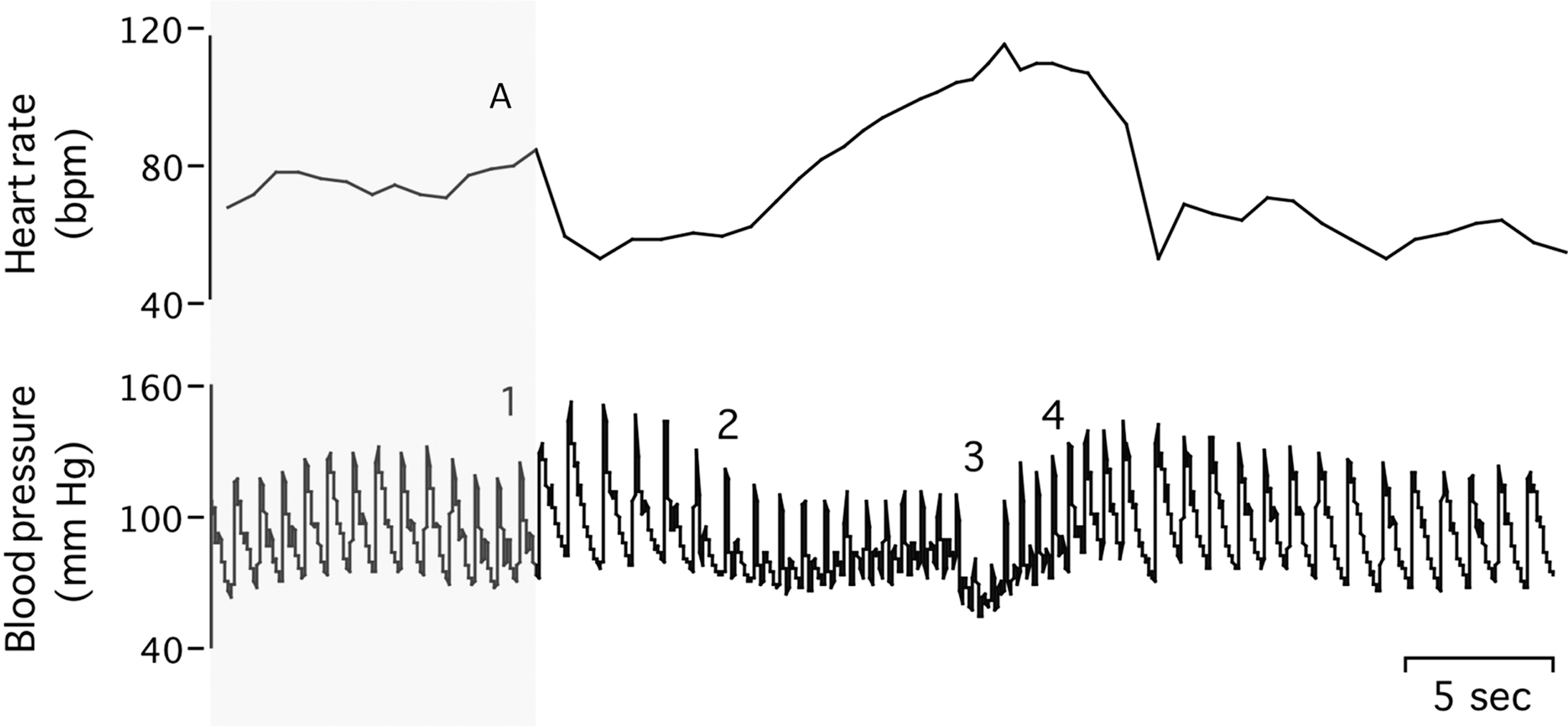
The quantitative Valsalva maneuver is performed by blowing with an open glottis into a mouthpiece connected to the mercury column of a sphygmomanometer with an air leak (grey-shaded portion). A 40- to 50-mm Hg pressure level is maintained for 15 sec (

Changes in arterial blood pressure (ABP), heart rate (HR), and end-tidal CO2 in a young subject under resting conditions (
Baroreflex Function after Spinal Cord Injury
After SCI, a significant disruption of the autonomic nervous system occurs. Similarly to motor deficits after SCI, the level of the spinal lesion greatly influences the amount of cardiovascular regulation possible after injury. Although vagal influence on chronotropy is maintained after SCI, 43 several reports have shown that the sensitivity of the cardiovagal baroreflex is impacted (Table 1). As cardiovagal BRS has shown predictive value for future cardiovascular events in able-bodied individuals, these findings support epidemiological studies indicating that cardiovascular risk is increased in those with SCI. 29,44,45 As mentioned previously, the cardiovagal baroreflex is unlikely to influence the overall absolute mean arterial blood pressure response to orthostatic challenge. However, evidence indicates that in able-bodied individuals, the vagal influence on heart rate (and therefore cardiac output) plays an important role in the short-term regulation of blood pressure (100% in the first 2–3 sec after a stimulus), but only a minor role after that (23%). 46 Further, the cardiovagal baroreflex is intimately related to the brain's ability to maintain effective perfusion (cerebral autoregulation). 47,48 As such, it is reasonable to suggest that abnormal cardiovagal baroreflex function after SCI is associated with the reduced orthostatic tolerance seen after injury. 30
Effect size values were calculated from graphical estimates and not numerical data.
↑=Significant increase compared to able-bodied controls;↓= significant decrease compared to able-bodied controls;≈= no difference compared to able-bodied controls.
High lesion denotes those with injuries at or above the T6 spinal segment; low lesion level denotes those with injures below the T6 level unless otherwise stated.
SCI, spinal cord injury; BRS, baroreflex sensitivity; SCI, spinal cord injury; HUT, head-up tilt; AB, able-bodied; ES, effect size; d, Cohen's d value; Gup, increasing blood pressure; Gdown, decreasing blood pressure.
The loss of the sympathetic branch of the baroreflex is far more detrimental to blood pressure regulation after SCI, as the descending sympathetic pathway becomes disrupted and results in significant reductions in the control of vasomotor tone below the lesion level (Fig. 7). 4,8,49 Those with lesions above the T6 spinal level have more severe autonomic dysfunction compared to those with lesions below this level. 43 This is partially due to decreased sympathetic activity within the sympathetic post-ganglionic fibers, which innervate the splanchnic vascular bed, and originate from below the sixth thoracic segment, and therefore do not have supra-spinal descending communication. 43 Additionally, autonomic dysfunction (e.g., autonomic dysreflexia) results from a lack of descending supra-spinal inhibition during periods of noxious or non-noxious stimuli reaching the spinal cord below the level of injury, such as catheterization, bladder distension, bowel evacuation, and even a tight shoelace. 8,9,43 As with motor impairment, there is a high level of variability in the level of autonomic dysfunction, even for individuals with the same lesion level, which is likely due to variability in the number of preserved descending autonomic pathways synapsing on sympathetic pre-ganglionic neurons below the level of injury. 4,9,43

Neural signals from the brain (central command), as well as afferent input from the aortic and carotid stretch receptors, central and peripheral chemoreceptors, and low-pressure pulmonary centers converge in the cardiovascular control center. The complex interplay of these factors regulates the blood pressure set point, and influences the rate and amplitude of the autonomic response to acute blood pressure changes (baroreflex sensitivity). This is achieved through rapid alterations of HR (heart rate), SV (stroke volume), and most importantly TVC (total vascular conductance), by adjusting autonomic outflow to cardiac and vascular tissue. denotes where baroreflex dysfunction may occur after spinal cord injury (1, arterial stiffening; 2, integration in the nucleus tractus soleus; 3, sympathetic descending pathway disruption; 4, sino-atrial node transmission). *Note that when a complete injury occurs, sympathetic vasomotor control is disrupted below the lesion level.
High lesion level
Our literature search revealed 12 studies that examined vagally-mediated baroreflex function in those with high-level SCI (above T6; Table 1). Five of these 12 articles reported a decrease in cardiovagal BRS, one showed an increase, and the remaining seven demonstrated no difference between individuals with SCI and able-bodied controls. As SCI is an uncommon condition, typically studies of reduced statistical power are published. The average Cohen's d value for effect size (i.e., the difference between the two means divided by the pooled standard deviation) is 0.29±0.7 in studies investigating cardiovagal baroreflex function in humans with high-level SCI. These values show that the SCI and able-bodied groups differed on average by approximately 0.3±0.7 standard deviations. Considering that a Cohen's d value of 0.29 is considered a small effect, and the variability between articles was more than twice the mean, these values do not compellingly illustrate that BRS is reduced in those with a high lesion. This is not surprising, considering not only the small sample sizes, but also the extreme heterogeneity of SCI. 3 Interestingly, the two studies using the neck-cuff technique reported very high Cohen's d values, at 1.8 and 0.99, suggesting greater sensitivity when using this technique. 50,51
If cardiovagal BRS is indeed reduced in high-level SCI, some consideration of this condition is deserved. Cardiovagal BRS is influenced by any of the following mechanisms: (1) arterial stiffening, reducing the input from stretch receptors; (2) a reduction in the signal transmission and integration in the nucleus tractus soleus; or (3) changes in the efferent signal transmission at the sino-atrial (SA) node 41 (Fig. 8). As neither the vagal or glossopharyngeal nerves are damaged during high-level SCI, we speculate that reductions in cardiovagal BRS are associated primarily with arterial stiffening in this population. Increased arterial stiffening leads to decreased activation of arterial stretch receptors for a given change in intra-arterial pressure, thus directly reducing the sensitivity of the system. 43,52,53 Arterial stiffening is enhanced by physical inactivity, which is highly prevalent in SCI. 54 These pathways are well known and have recently been reviewed. 55 However, studies have reported that arterial stiffness is increased in those with SCI, even when matched for physical activity patterns. 56 –58 The mechanisms responsible for increased stiffness specific to the SCI population include: reduced shear stress leading to reduced arterial caliber and increased wall thickness; endothelial cell glucose insensitivity; and sympathetic dysfunction. 59 –61 As further evidence, upon movement from supine to 45° of head-up tilt, high-level lesion SCI patients have greater reductions in carotid arterial diameter and blood flow velocity compared to both low-level lesion SCI and AB controls. 62

Summary of evidence from studies examining baroreflex function in those with high-level spinal cord injury. *Indicates that the region of dysfunction cannot be differentiated by the techniques used to examine cardiovagal baroreflex function. denotes where baroreflex dysfunction may occur after spinal cord injury. Numbers indicate references examining dysfunction in this pathway.
Alternatively, the neural component may also be influenced after SCI. Those with high-level SCI have chronically elevated renin concentrations, and this may impact sino-atrial vagal sensitivity. 63,64 Further, autonomic regulatory centers in the brain require sufficient perfusion to maintain effective blood pressure regulation. 65 Also, considering that individuals with chronic hypotension also have reduced cerebral perfusion, it is plausible that the neural BRS pathway is also disrupted in those with high-level SCI. 66 Indeed, a marked inability to maintain cerebral blood flow during orthostatic challenge has been shown in high-level SCI. 67 –69
The one study to show a paradoxically significant increase in cardiovagal BRS used a similar technique (power spectral transfer function analysis), and had a relatively large sample size (n=14, T3 and above). 70 The authors speculated that cardiovagal sympathetic afferent activity may be reduced during head-up tilt in the high-level injury group due to reductions in venous return and cardiac dimensions, thus decreasing sympathetic afferent and the subsequent efferent activity. However, it is well established that resting sympathetic nervous system (SNS) activity in a complete lesion above T6 is severely disrupted, and that outside of autonomic dysreflexia, sympathetic tone is essentially null. 71 As such, it is unlikely that the above theory explains this paradoxical finding, as sympathetic outflow to the heart typically occurs at the T4–T5 level, and all participants had complete injury levels at T3 or above. 70 Alternatively, these contrary spontaneous cardiovagal BRS results may be due to the uncommon technique of examining BRS gain from a broad frequency range, including both the low and mid-frequency ranges (i.e., 0.02–0.4). Also, Munakata and associates reported that 5/14 high-lesion level individuals had BRS gain generated in the high-frequency range, due to low coherence over the low and mid-range frequencies; they have been shown to have increased coherence due to respiration. 15 On the other hand, research has illustrated that when vagal tone is chronically increased in canines, cardiovagal BRS is increased. 72 In addition, our research group has demonstrated increases in supine cardiac vagal tone in those with high-level SCI. 73 These studies provide an explanation for the number of articles that reported preserved cardiovagal BRS in those with SCI, if we assume arterial stiffness was increased.
The T6 level has been shown to be an important lesion level due to the loss of descending supra-spinal sympathetic signals in the crucial splanchnic region. Accordingly, SCI above the T6 spinal segment leads to serious disturbances in autonomic cardiovascular regulation. After high-level SCI, sympathetic outflow is differentially influenced, depending on both the lesion level and the completeness of injury. It is important to note that sympathetic vasomotor innervation persists after high-level SCI. A combination of poor supra-spinal sympathetic regulation, and hypersensitivity to α1 and α2 agonists and angiotensin II after high-level SCI leads to inappropriate adrenergic responses. 43,74 To our knowledge, only eight articles have examined the sympathetic baroreflex response in those with high-level SCI, and none used established blood pressure-perturbing techniques known to provide the most accurate and reliable results (Table 2). 5 Sympathetic dysfunction below the lesion level has made measuring the sensitivity of the sympathetic baroreflex difficult. Several studies using indirect estimates derived from frequency analysis of heart rate and systolic blood pressure suggested a reduced sympathetic response to an orthostatic challenge in those with high-level SCI. These measures cannot be interpreted to directly relate to sympathetic activity, and the use of frequency analysis-derived measures to quantify sympathetic activation is contentious. While originally reported to be significantly related using group data during lower body negative pressure, 75 Ryan and associates recently showed that on an individual basis, low-frequency power of systolic blood pressure (SBPLF) does not correlate with recordings of MSNA. 76 Similarly, the low-frequency component of the ratio of low-frequency RRI power to high-frequency RRI power (LFRRI/HFRRI) was shown to be related to MSNA in two early articles, although both have limitations, in that either (1) the statistical analysis may not be suitable, 75 or (2) only 40% of participants reported a significant relationship. 77 Also in opposition of using LFRRI/HFRRI, Cooke and colleagues demonstrated in able-bodied individuals that the changes in LFRRI/HFRRI that occur during sympathetic activation are more due to decreases in the HF denominator (thought to arise primarily from respiratory-mediated increases in vagal efferent activity), and not the LF numerator. 79 Taking into consideration the controversy surrounding these measures, studies examining spectral-derived indicators of sympathetic tone in those with high-level SCI still deserve discussion, and indeed SBPLF and LFRRI/HFRRI are reduced in those with high-level SCI during orthostatic challenges (Table 2). As the amplitude of vagal withdrawal is usually the same, 64 or increased, 73 in this population, reduced LFRRI/HFRRI may indicate an attenuation of the sympathetic cardiac response during an orthostatic challenge. These studies, which employed indirect indicators of sympathetic activity, are supported more directly by work showing that the norepinephrine response to a nitroprusside bolus (rapid decrease in blood pressure) was severely reduced in high-level lesion SCI. Taken together, there is compelling evidence for a dysfunctional sympathetic response to blood pressure changes and orthostatic challenges in this population. 51 This evidence should be interpreted with caution, however, as these studies do not necessarily show a mitigated baroreflex-mediated sympathetic response (which would occur within 5 sec after orthostatic challenge), as much as they highlight the functional inadequacy of the sympathetic autonomic branch during hemodynamic challenges in those with high-level SCI.
↓=Significant decrease compared to able-bodied controls;≈= no difference compared to able-bodied controls.
High lesion level refers to those with injuries at or above the T6 spinal segment; low lesion level denotes those with injures below the T6 level unless otherwise stated.
SCI, spinal cord injury; RRI, RR-interval; RRILF/RRIHF, ratio of LF power of RRI to HF power of RRI; HUT, head-up tilt; SBPLF, spectral power of blood pressure in the LF region; AB, able-bodied; HF, high frequency; LF, low frequency.
Due to the loss of sympathetic vasomotor tone below the lesion level and the susceptibility to orthostatic hypotension, those with high-level SCI rely disproportionately on the renin-angiotensin-aldosterone system to regulate blood pressure.
78
As such, larger increases in renin have been found during orthostatic challenge in tetraplegics.
80
The increase in renin-angiotensin dependency, however, appears to be more related to blood pressure responses due to poor vasomotor response, and less to baroreflex function specifically. Improving blood pressure response through nitro-
It should be noted that one study did not find a reduced response of SBPLF during orthostatic challenge in high-level lesions, a finding potentially explained by a weaker orthostatic stimulus than that used in other studies. 68 Collectively, the overall findings in this field of study can be explained by the work done by Stjernberg and associates, which shows that resting MSNA in the peroneal nerve is extremely low and nearly non-existent in those with SCI. 71 This highlights that the ability to produce effective vasomotor tone is lost below the level of SCI. Severely reduced vasomotor control was also shown by the work by Houtman and colleagues, who demonstrated an essentially passive blood pressure and cerebral blood flow response to lower-body negative pressure in those with high-level SCI, while in able-bodied individuals with intact vasomotor control mean arterial pressure was well maintained. 67 In that study, it was illustrated that blood pressure and cerebral blood flow decreased in a remarkably linear fashion in relation to the suction applied to the legs. 67 The most interesting aspect of that article was the finding that cerebral oxygenation was markedly decreased in the high-lesion group compared to able-bodied individuals; however, both groups reported a similar prevalence of syncope, suggesting that downstream mechanisms related to the hypoxic threshold for syncope may have adapted. Other work from our group has highlighted this possibility, showing that subtle markers of cerebral hemodynamic adaptation (dynamic cerebral autoregulation as well as cerebral blood flow pulsatility index) occur in those with high-level SCI. 82 This association provides support for the fundamental inverse relationship between BRS and cerebral autoregulation. 48
It is unfortunate that so few studies have investigated the sympathetic branch of the baroreflex system in those with high-level lesions, as this would provide insight into the functioning of the baroreflex branch most important to the widespread orthostatic intolerance present within this population. Interestingly, sympathetic vasomotor tone of the brachial artery is innervated from the brachial plexus, which is a combination of spinal nerves C3–C6. As such, it would be possible to evaluate the sympathetic baroreflex sensitivity directly. More studies of this topic may shed light on why blood pressure is so drastically reduced after orthostatic challenge, and why α-agonist administration not only improves resting blood pressure, but also mitigates the blood pressure reduction seen during orthostatic challenge. 83
Low lesion level
Marked variability exists within the seven articles reviewed that examined cardiovagal baroreflex function in low-level SCI (Table 1). For example, three studies showed a reduction in cardiovagal BRS. Of these, two employed the Valsalva technique to measure BRS, while the remaining article used a spontaneous indicator of BRS. 84 As such, 80% of the studies using spontaneous indicators of BRS failed to show a significant reduction in those with low-lesion level SCI. The average Cohen's d value for effect size is 0.55±1.11 in studies investigating spontaneous baroreflex function in humans with low-level SCI. Taking into account the variability in the available evidence, it is still not clear if cardiovagal BRS is reduced in those with low-level SCI. Again, the two studies employing phase IV Valsalva for BRS evaluation reported high Cohen's d values of 2.3 and 1.0. 84,85
Similarly to high lesions, those with low-level SCI tend to be more physically inactive compared to able-bodied individuals. 54 Furthermore, lower resting supine vagal tone has been shown in those with low-level SCI. 73 Therefore, following the same principles outlined for the high-level lesion SCI group (i.e., physical activity and resting vagal tone), there is a strong rationale for finding reduced sensitivity of the baroreflex. 62 From a hemodynamic perspective, cerebral perfusion is likely maintained in low-level SCI, and cardiovagal tone is preserved. 67,68 Following this, the neural pathway of the baroreflex is likely not disrupted. 73 Both studies using phase IV Valsalva derived-values reported reduced BRS in low-level lesion SCI. It is difficult to synthesize these findings with the overall trends found using spontaneous BRS measures. Published work 86 comparing the Valsalva technique to the modified Oxford method have shown the two measures to be correlated, but not to provide similar results. When compared to spontaneous BRS techniques, the values from the Valsalva technique were not associated with those reported using the spectral method, and related significantly only to Gdown of the sequence method. 86 It has been suggested that BRS markers derived from the Valsalva maneuver provide different information regarding the baroreflex compared to spontaneous-derived markers. Spontaneous BRS is thought to be representative of tonic cardiovagal activity, whereas BRS measures derived from perturbed blood pressure (Valsalva and modified Oxford) are associated with the phasic relationship between vagal tone and blood pressure changes. 87 Therefore, it may be the case that phasic BRS is influenced after SCI, whereas tonic BRS is not. The clinical value of phasic versus tonic BRS has yet to be determined.
Several researchers have attempted to measure the sympathetic branch of the baroreflex system in those with low-level SCI. These articles have shown that the orthostatic response in SBPLF and LFRRI/HFRRI was also reduced in those with low-level SCI (Table 2). Those with low-level SCI also do not have tonic vasomotor outflow below the lesion level, and therefore would have reduced amplitude of SBP oscillations. Indeed, this group is expected to have more systemic vasomotor tone compared to those with higher lesion levels, as they have less vascular tissue undergoing disrupted sympathetic control. 71 Bluvshtein and associates reported that LFRRI/HFRRI was similar for low-lesion level SCI and able-bodied controls; however, the sample size was quite small, and the study may have been under-powered. 68 These findings highlight that the cardiac and vasomotor response to orthostatic challenge is disrupted, even after low-level SCI. Interpretation of these studies should be made with caution, as neither of the markers of SNS activity truly represents BRS, as they are simply measures of resting autonomic tone in different orthostatic positions.
In general, baroreflex dysfunction in those with low-level lesions is not as severe as in those with high-level lesions (Fig. 9). This is thought to be due to the aforementioned mitigating factors, such as greater physical activity levels, preservation of some sympathetic vasomotor tone, and maintenance of cerebral perfusion.

Summary of evidence examining baroreflex function in those with low-level spinal cord injury. *Indicates that the region of dysfunction cannot be differentiated by the techniques used to examine cardiovagal baroreflex function. Note that spontaneous estimates of cardiovagal baroreflex sensitivity did not detect differences in low-level spinal cord injury. denotes where baroreflex dysfunction may occur after spinal cord injury. Numbers indicate references examining dysfunction in this pathway.
Future Directions
To focus clinical and research efforts on improving BRS, the issue of whether dysfunctional BRS after SCI is due primarily to increases in arterial stiffening or to a more downstream neural component needs to be elucidated. The resolution of this issue would also aid in the development of new technologies, and the advancement of techniques currently undergoing testing such as a transcutaneous bionic baroreflex system. 88 It should be noted that a number of articles are insufficiently powered to assess baroreflex function in SCI. This issue should be more widely acknowledged and discussed in articles when sample size is an issue.
The physical activity levels of the low-level SCI groups were not mentioned in most research studies, and only one article attempted to control for physical activity levels. 89 In our experience, there is often much more access to, and participation from, SCI participants who are highly active, while it is exceedingly difficult to recruit SCI subjects with a more physically-inactive lifestyle. Physically-active individuals with SCI tend to have reduced arterial stiffness, and would also be expected to have increased gravitational challenge compared to their inactive counterparts (resulting from fewer orthostatic challenges in daily living). 58 As both of these factors are known to be related to reduced BRS, this selection bias may have led to a more similar cardiovagal BRS. 3 In addition, spontaneous techniques for evaluating BRS, especially those derived through the spectral method, are confounded by the feed-forward relationship between increasing heart rate and blood pressure. 5 As such, spontaneous BRS measures, particularly for the purpose of stratifying cardiovascular risk, should be used with caution, while non-spontaneous measures of BRS need to be more widely employed. 5
As those with chronic hypotension and SCI are thought to have decrements in cognitive function associated with reduced brain blood perfusion, the relationship between baroreflex function, cerebral hemodynamic regulation, and cognitive function in SCI also needs to be examined. Baroreflex sensitivity directly influences cerebral perfusion, and appropriate treatment of BRS after SCI may mitigate reductions in cognitive function. 90
In both high- and low-level SCI, direct measurement of the sympathetic branch of the baroreflex is warranted to evaluate the role reduced sensitivity plays in orthostatic hypotension. Although peroneal nerve MSNA is not viable, brachial nerve MNSA or brachial artery vascular resistance are potential sites to measure vasomotor responses to blood pressure and/or arterial diameter changes.
Conclusions
The available literature indicates that BRS is disrupted in those with both low-level and high-level SCI. Baroreflex function is more consistently disrupted in those with high-level lesions, due to severe dysfunction of the sympathetic as well as parasympathetic branches. The overall findings are hampered by small sample sizes, and several spontaneous and ramped BRS techniques that detect different components of the baroreflex. Baroreflex sensitivity in those with low-level SCI is less clear. Arterial stiffening has been shown to be increased in both high- and low-level SCI, although it is interesting that BRS is not consistently reduced in these populations. It is plausible that increased vagal tone, which has been shown to improve cardiovagal BRS, 72 may ameliorate the decline resulting from increased arterial stiffening. Our focus should be directed on examining the sensitivity of the sympathetic branch of the baroreflex due to the lack of information currently available.
Footnotes
Author Disclosure Statement
No competing financial interests exist.