
Abstract
Chronic pain is a highly prevalent post-concussion symptom occurring in a majority of patients with mild traumatic brain injury (mTBI). About half of patients with mTBI report sleep–wake disturbances. It is known that pain can alter sleep quality in this population, but the interaction between pain and sleep is not fully understood. This study aimed to identify how pain affects subjective sleep (Pittsburgh Sleep Quality Index [PSQI]), sleep architecture, and quantitative electroencephalographic (qEEG) brain activity after mTBI. Twenty-four mTBI patients complaining of sleep–wake disturbances, with and without pain (8 and 16, respectively), were recruited 45 (±22.7) days post-trauma on average. Data were compared with those of 18 healthy controls (no sleep or pain complaints). The PSQI, sleep architecture, and qEEG activity were analyzed. Pain was assessed using questionnaires and a 100-mm visual analogue scale. Patients with mTBI reported three times poorer sleep quality than controls on the PSQI. Sleep architecture significantly differed between patients with mTBI and controls but was within normal range. Global qEEG showed lower delta (deep sleep) and higher beta and gamma power (arousal) at certain EEG derivations in patients with mTBI compared with controls (p<0.04). Patients with mTBI with pain, however, showed greater increase in rapid EEG frequency bands, mostly during REM sleep, and beta bands in non-REM sleep compared with patients with mTBI without pain and controls (p<0.001). Pain in patients with mTBI was associated with more rapid qEEG activity, mostly during REM sleep, suggesting that pain is associated with poor sleep and is a critical factor in managing post-concussion symptoms.
Introduction
A
Sleep–wake disturbances are common consequences of TBI. For example, excessive daytime sleepiness was found in patients with mTBI. 6,7 High prevalence (72%) of sleep–wake disturbances was found in patients with TBI during the first 6 months. 8 After 3 years, 67% of patients still reported sleep–wake disturbances (mainly hypersomnia and insomnia). 9 Whereas the presence of sleep disorders did not correlate with trauma severity, conflicting results were found for depression and anxiety. 4,10 Sleep disorders reported in the mTBI population are referred to as sleep and wake disturbances because the major complaint is post-traumatic hypersomnia and the second major complaint is insomnia. 3,10 –13 The etiology of sleep disorders in mTBI remains poorly understood.
Polysomnographic recording of biophysical changes of sleep parameters that occur during sleep (including sleep stages, arousals during sleep) were performed in patients with mTBI. Few mTBI studies have obtained conflicting results on sleep stage 1 duration (lighter sleep), sleep efficiency, or rapid eye movement (REM) sleep duration, or finding no differences from healthy controls. 4,6,14,15 Therefore, polysomnographic recording could not confirm subjective sleep complaints.
Studies on quantitative electroencephalogram (qEEG) power during sleep also found conflicting results, mainly because of whether sleep was recorded in the acute or chronic post-trauma phase. qEEG power is a useful tool to extend the analysis of the EEG and to decompose the signal into a voltage and frequency power spectrum. Low frequency bands represent deeper sleep, and high frequency bands are associated with awakening and arousal. Thus, patients with mTBI showed lower delta (slow waves, important for sleep homeostasis) and higher alpha and beta power (faster bands that represent arousal) during non-REM sleep than controls 1 week post-trauma. 15 A significant power reduction in low qEEG frequency bands (0.5–9.75 Hz) during non-REM sleep was also found in adolescents post-mTBI in the acute phase. 16 Conversely, no differences in sleep qEEG were reported in a general sample of patients with mTBI or in athletes with mTBI compared with healthy subjects and control athletes. 17,18 Even with a technique able to detect subtle differences that polysomnography is unable to detect, no conclusion could be reached regarding changes that occur during sleep after mTBI.
At 1 year post-trauma, the excessive daytime sleepiness complaint was equivalent in patients with TBI and patients with trauma other than in the brain, suggesting that bodily pain plays an important role in sleep–wake disturbances. 19
Pain is defined as an unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage. 20 Pain is a highly prevalent post-concussion symptom in patients with mTBI, occurring in more than 75% of cases. 5 Acute post-traumatic pain presents under several forms, mostly musculoskeletal pain, widespread pain, post-traumatic headache, or vascular, neurogenic, visceral, and iatrogenic pain. 21 Patients with mild TBI reported more pain than did patients with severe TBI. 5,22
Up to 70% of patients with pain reported poor sleep quality or unrefreshing sleep. 23 Studies have indicated that the pathways that regulate sleep, arousal, and nociception overlap and interact. 24 Therefore, pain is important in sleep studies because of the linear relationship between the two states. The literature has associated pain with sleep problems in mTBI, based on questionnaires and reports. 22,25 The presence of pain was associated with twice as many complaints of insomnia in mTBI. 22 Patients with mTBI presenting with sleep complaints reported more headaches at 6 weeks post-trauma. 25 Pain as well as post-traumatic stress disorders were also shown to contribute significantly to sleep problems known as the “polytrauma clinical triad.” 26
The presence of pain was crucial when interpreting patients' physical, psychological, and cognitive complaints after TBI. 27 In fact, in clinical settings, comorbidities including anxiety, depression, and pain catastrophizing are becoming very frequently assessed in patients with pain. 28 A large study that included more than 400 patients with mTBI, revealed that patients presenting sleep–wake disturbances also have concomitant depressive symptoms and irritability. 25 Patients with mTBI with pain reported more depressive and anxiety symptoms. 29,30 Pain catastrophizing was also related to the threatening nature of pain after injury or illness. 31 To our knowledge, however, no studies have investigated sleep changes in the presence of pain in an mTBI population with attention to other comorbidities.
Because the exact nature of this deleterious interaction remains unknown, it was relevant to investigate the relationship between sleep and pain in patients with mTBI. Although pain has been widely cited as an important factor affecting sleep in mTBI, no studies to date have investigated the contribution of pain to sleep parameters in this population. Moreover, because of the important impact of comorbidities on sleep and pain, anxiety, depression and pain catastrophizing will be considered in this article.
To characterize how pain affects sleep in mTBI patients, two primary objectives and one secondary objective were proposed. Primary objectives were: (1) to compare subjective sleep, sleep architecture, and qEEG between patients with mTBI and controls; and (2) to compare subjective sleep, sleep architecture, and qEEG between patients with mTBI with pain, patients with mTBI without pain, and controls; and the secondary objective was: (3) to explore the effects of depression, anxiety, and pain catastrophizing on the relationship between pain and sleep in patients with mTBI.
We hypothesized that qEEG pattern variability during sleep would be associated with pain in mTBI.
Methods
Study sample
Patients were screened from about 300 mTBI visits per year to the trauma unit of a tertiary hospital center. We recruited 29 patients 6 weeks after trauma. The mTBI diagnosis was confirmed by a trauma neurosurgeon (JFG) according to the 2004 World Health Organization Task Force on mTBI. 32 Inclusion criteria were (1) score of 13–15 on the Glasgow Coma Scale; (2) loss of consciousness and post-traumatic amnesia for <30 min; (3) age 18–60 years; and (4) self-reported sleep complaints. Participants were also asked to undergo two nights of sleep recordings in the laboratory.
Patients were excluded for (1) gross cognitive or speech dysfunctions; (2) use of psychotropic medication or other drugs known to influence sleep or motor behavior; (3) presence of major neurological or psychiatric disorders or alcohol abuse; (4) history of chronic pain or fibromyalgia before mTBI; and (5) history of sleep disorders, including circadian disruption.
Because five patients refused the second night of sleep assessment, the final sample comprised 24 patients.
Eight patients with mTBI were classified as mTBI with pain based on the following criteria: (1) persistent pain since the accident at different body sites (head, neck, back, or jaw); (2) report of trouble sleeping because of pain on the Pittsburgh Sleep Quality Index (PSQI), item 5, three or more times a week; and (3) moderate to severe intensity pain on awakening on a scale of 0–4 (0=no pain, 4=severe pain). None of these participants had sustained a new injury that caused pain after the initial traumatic injury. Sixteen patients with mTBI who did not meet these pain criteria were classified as mTBI without pain.
Eighteen healthy subjects free of pain and sleep complaints were recruited as controls. All patients and controls provided written consent to participate. The study protocol was approved by the ethics board of the Hôpital du Sacré-Coeur de Montréal.
Subjective sleep assessment
All participants completed the PSQI, a self-rated questionnaire that assesses subjective sleep quality over the past month. A global PSQI score greater than 5 indicates sleep disturbance, as previously validated in patients with TBI. 33,34 Sleep quality on awakening was reported on a 100-mm visual analogue scale (VAS) (0=worst sleep, 100=best sleep).
Polsomnography
All patients with mTBI and controls slept for two consecutive nights in a light- and sound-attenuated room at the hospital's sleep laboratory. The first night was used for habituation and the second night for data collection and analysis.
Recordings were performed using a 32-channel Grass polysomnograph with 0.1–100 Hz filter bandpass. The montage comprised 11 leads for EEG derivations placed according to the international 10–20 system (C3-A2; C4-A1; F3-A2; F4-A1; F7-A2; F8-A1; Fp1-A2; Fp2-A1; Fz-A1; O1-A2; O2-A1); bilateral electrooculograms; chin, masseter, and tibialis electromyograms; and three electrocardiogram (ECG) derivations. Thoracic and abdominal straps, a nasal airflow cannula, and a pulse oximeter were used to monitor respiration. Signals were digitalized at a 256 Hz and 512 Hz sampling rate for EEG and ECG, respectively. Continuous audio and infrared video recordings were performed to detect abnormal movements and behaviors during sleep.
Sleep stages were visually scored off-line on 20-sec epochs using Rechtschaffen and Kales' criteria. 35 Arousals, periodic leg movements, and respiratory disturbances were scored using standard criteria. 36 Sleep latency was determined as the time between bedtime and sleep stage 2, and persistent sleep latency as the time between bedtime and 10 consecutive minutes of uninterrupted sleep. REM sleep latency was defined as the time between bedtime and the first stage of REM sleep. Sleep duration is the number of minutes spent sleeping. Sleep efficiency is the percentage of time in bed that comprises sleep. The percentage of time spent in each sleep stage (1, 2, 3, and 4 and REM sleep) is provided. REM sleep efficiency is the percentage of REM sleep free of awakening. The micro-arousal index is the number of micro-arousals (<3 sec) per hour. The index of periodic leg movements during sleep is the number of leg movements per hour of sleep. The apnea-hypopnea index is the number of sleep-disordered breathing events per hour of sleep.
qEEG spectral analysis
Spectra were analyzed off-line using IGOR Pro 6.12A (WaveMetrics) software on artefact- and wake-free signals for the 11 EEG derivations. Fast Fourier transform (FFT) was applied to consecutive 1-minute epochs over the night. Data were normalized to min per stage. Frequency bands were defined as follows: delta (0–4 Hz), theta (4–7 Hz), alpha (9–11 Hz), sigma (12–15 Hz), beta (16–30 Hz), and gamma (30–50 Hz). 37
Self-report data
Questionnaires were administered to all participants to collect demographic, medical, and psychological data. Hospital medical records for patients with mTBI were consulted to confirm diagnoses. Pain intensity was reported on a 100-mm VAS. Participants were asked to rate their current pain (0=no pain, 100=worst pain ever felt), using the question, “At this moment, how much pain do you feel?” We compiled scores on the Beck Depression Inventory (BDI), the Beck Anxiety Inventory (BAI), and the Pain Catastrophizing Scale (PCS). Each Beck questionnaire includes 21 items to assess depression and anxiety symptoms on a self-rated scale varying from 0 to 3. Higher total scores indicate more severe depression and anxiety symptoms. 38,39 Both Beck inventories have previously been used in participants with mTBI. 40 The PCS is composed of 13 questions rated on a scale of 0 to 4 (0=not at all 4=all the time). It is widely used to assesses three components of catastrophizing: rumination, magnification, and helplessness. 41 It was previously validated in patients with whiplash. 42
Statistical analysis
Statistical analyses were performed with PASW Statistics 18 (SPSS Inc, Chicago, IL) with statistical significance at p<0.05. Results are reported as means with standard deviations (SD). Normality of data distribution was assessed with a Shapiro-Wilks test. A Student t test was used to compare differences between mTBI and controls for normally distributed data and a Mann Whitney U test to compare non-parametric data. A chi-square test with odds ratio determination and a 95% confidence interval (CI) were applied to PSQI scores. Analysis of variance (ANOVA) was performed to compare qEEG between groups (mTBI with pain, mTBI without pain, controls). A post-hoc Tukey test was applied to the ANOVA to determine between-group differences. A simple and a multivariate stepwise regression were applied to the self-reported questionnaire data and the PSQI global score.
Results
Sample
Twenty-four patients with mTBI (15M/9F) with a mean age (±SD) 38.33±11.39 years and with post-traumatic sleep complaints were recruited. Sleep was recorded at 48.71±22.69 days post-trauma on average (range 19–117 days). Hospitalization was less than 24 h for 79.2% of patients, with an average of 42 h and a range of 05–456 h. Injuries resulted from a fall in nine patients, a motor vehicle accident in eight patients, and a sports-related incident in four patients. Two patients were pedestrians hit by motor vehicles, and one was involved in a fight. Patients with mTBI scored significantly higher on the Beck Depression Scale (mTBI:15.14±10.0; controls:1.23±1.96), the Beck Anxiety Scale (mTBI:9.89±10.50; controls:1.08±1.44), and the PCS (mTBI:19.08±13.25; controls:9.08±5.73) than controls (p<0.01 for all). All differences were statistically significant (Table 1a).
Values are given as mean (standard deviation); age range in brackets; a Student t test was used to compare the two groups.
mTBI, mild traumatic brain injury.
Patients with mTBI with pain rated pain intensity on a VAS at 49/100 (±30.98) compared with patients with mTBI without pain at 19.38/100(±16.74) (p<0.001). Figure 1 shows painful body sites in patients with mTBI with pain: 75% had back pain; 37.5% had frontal headache and neck and shoulder pain; 25% had sternum, knee, and pelvic pain; and 12.5% had occipital headache, hip, and foot pain. Patients with mTBI with pain scored at least twice as high on the BDI (mTBI with pain: 24.80±12.50; mTBI without pain: 12.13±7.13; p=0.01), the BAI (mTBI with pain: 19.50±11.21; mTBI without pain: 7.14±7.38; p=0.02), and the PCS (mTBI with pain: 30.57±9.22; mTBI without pain: 15.00±11.35; p=0.004) than mTBI without pain (Table 1b). All differences were statistically significant.
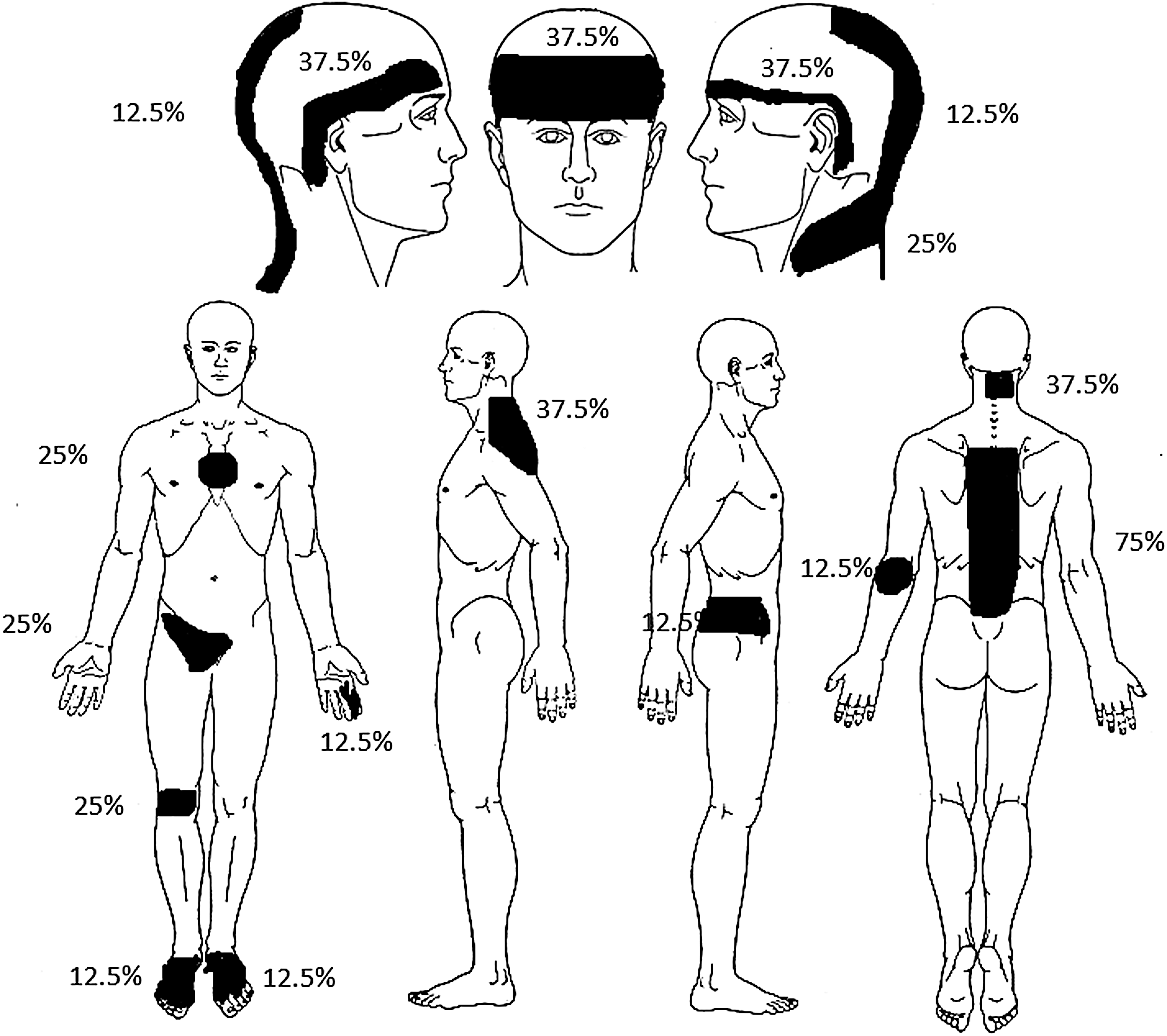
A pain diagram showing places where subjects were asked to mark painful body sites. Marked sections correspond to the sum of painful body sites indicated by patients with mild traumatic brain injury (mTBI) with pain. Percentages represent the percentage of patients with mTBI with pain who identified the area as painful.
Values are given as mean (standard deviation); age range in brackets; analysis of variance was used to compare the three groups.
mTBI, mild traumatic brain injury; VAS, visual analogue scale; BDI, Beck Depression Inventory II; BAI, Beck Anxiety Inventory; PCS, Pain Catastrophizing Scale.
Subjective sleep
On awakening after laboratory recording, patients with mTBI and controls reported their sleep quality on a 100-mm VAS. Patients with mTBI reported poorer sleep quality (44.96/100±23.96) compared with controls (72.53/100±15.70; p<0.001). No statistically significant difference on the sleep quality VAS was found between mTBI with pain (49.00/100±20.70) and mTBI without pain (43.19/100±25.70) (Table 1b).
Patients with mTBI reported sleep complaints based on the global PSQI score; 84.6% of patients with mTBI scored greater than 5 on the global PSQI score. Patients with mTBI showed a statistically significant difference on the global score (p<0.001) and on all component scores (p<0.05) compared with controls, except for the use of sleep medication. Using the chi-square test (p=0.001), patients with mTBI had an odds ratio (OR) of 38.5 (CI: 4.7-318.5) to score greater than 5 on the global PSQI score (Table 2).
Data shown as mean (standard deviation). The Mann-Whitney U test was used to compare the two groups.
mTBI, mild traumatic brain injury; ns, non-significant.
Sleep architecture
Sleep architecture showed statistically significant differences between patients with mTBI and controls for sleep latency, persistent sleep latency, and sleep efficiency (p=0.03). Although patients with mTBI presented sleep complaints, all the above sleep parameters fell within a clinically normal range according to American Academy of Sleep Medicine criteria. 36 No other sleep architecture parameters showed differences between patients with mTBI and controls (Table 3a).
Values are given as mean±standard deviation. A Student t test was used to compare the two groups for variables with normal distribution and a Mann-Whitney U test when distribution was non-parametric.
mTBI, mild traumatic brain injury; ns, non-significant; REM, rapid eye movement.
No statistically significant differences between mTBI with pain, mTBI without pain, and controls were found for all sleep architecture parameters (Table 3b).
Values are given as mean±standard deviation. An ANOVA with a Tukey's post-hoc test was used to compare the three groups.
mTBI, mild traumatic brain injury; ns, non-significant; REM, rapid eye movement.
qEEG
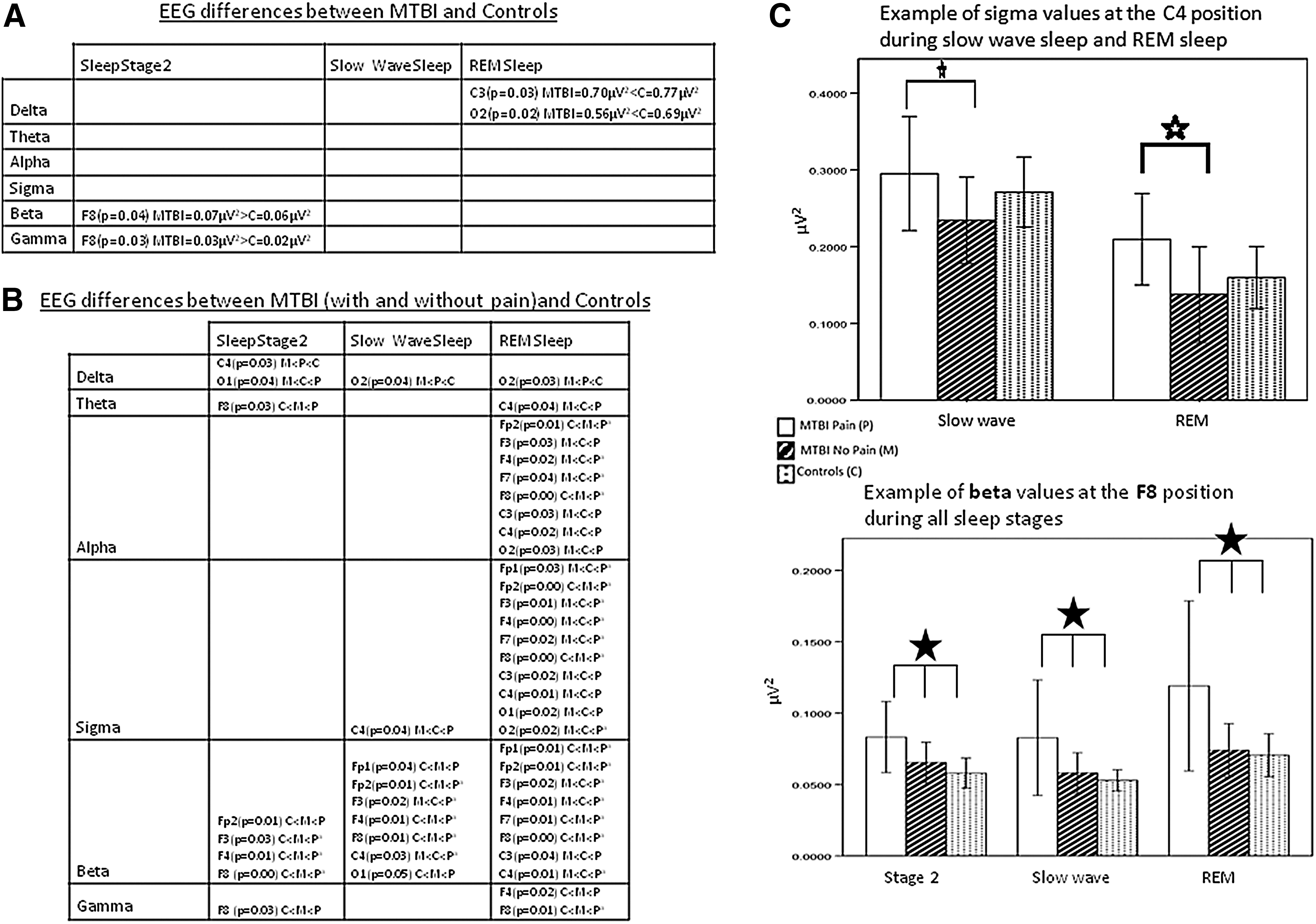
During REM sleep, lower delta frequency power was observed in mTBI (with and without pain combined) at C3 (mTBI=0.70μV2; controls=0.77μV2; p=0.03) and at O2 (mTBI=0.56μV2; controls=0.69μV2; p=0.02). Higher activity was observed at the F8 derivation during sleep stage 2 in mTBI for beta (mTBI=0.07μV2; controls=0.06μV2; p=0.04) and gamma (mTBI=0.03μV2; controls=0.02μV2; p=0.03) frequency bands. When these results were controlled for age and sex, neither co-variable affected the above-mentioned qEEG results (data not shown). Comparison between mTBI and controls showed no statistically significant differences in theta, alpha, or sigma bands for all non-REM and REM sleep stages (Fig. 2a).
Table
Overall, in a three-group comparison, mTBI with pain, mTBI without pain, and controls generally showed statistically significant differences on all derivations and sleep stages. The mTBI with pain group showed statistically significant larger spectrum values for theta, alpha, sigma, beta, and gamma frequencies than the two other groups on frontal, central, and occipital derivations. No statistically significant differences were found between mTBI without pain and controls, except for delta frequency bands during stage 2 at the C4 derivation and at O2 during slow wave and REM sleep. In the delta frequency band, both mTBI with and without pain showed statistically significant lower spectrum values than controls (p<0.04) (Fig. 2b).
Psychological symptom scales and PSQI
A simple regression showed that pain VAS (r2=0. 31, p<0.01), pain catastrophizing (r2=0.41, p<0.01), and depression (r2=0.57, p<0.01), but not anxiety (r2=0.07, p=0.23) were related to the global PSQI score and subscores (r2=0.14–0.62, p<0.05). With multivariate stepwise regression, only depression explained global PSQI scores (r2=0.50, p<0.001).
Discussion
The main finding of this study was the association of pain with qEEG changes during sleep in patients with mTBI. We first characterized an mTBI population with pain that reported more depression, anxiety, and catastrophizing than patients with mTBI without pain. Although subjective sleep reports, the PSQI, and the VAS showed sleep disruption, sleep architecture in acute patients with mTBI complaining of sleep–wake disturbances showed significant differences, but remained within normal range. Further, qEEG did not differ between mTBI and controls, except for the delta frequency band at C3 and O2 during REM sleep and one derivation (F8) in the beta and gamma bands during non-REM sleep. In the presence of pain, however, spectral values increased in rapid EEG frequencies (alpha to gamma) during REM sleep, and delta spectral values decreased in both REM and nonREM sleep.
Patients with mTBI with pain reported more depression, anxiety symptoms, and catastrophizing behavior than patients with mTBI without pain. Other results suggested that pain, depression, and pain catastrophizing were associated with poor sleep quality in patients with mTBI, and there appeared to be interrelation with sleep quality, with depression showing a strong association with sleep complaints.
Our sleep architecture findings corroborated well with previous findings. Williams and coworkers 17 found that patients with mTBI had lower sleep efficiency and shorter REM sleep latency, whereas qEEG showed no significant results. Other studies also found no differences in qEEG during sleep after mTBI. 18,43 Another study found that trauma severity did not affect sleep architecture in chronic TBI cases, but patients with mild TBI had more stage 1 sleep, increased sleep efficiency, and decreased wake time during sleep compared with patients with moderate and severe TBI. 4 The inclusion of other confounding factors such as pain and depression was proposed but not verified in these studies.
In the present study, discrepancies were observed between perceptions of poor sleep and sleep architecture within normal limits. One possible explanation for these discrepancies is the presence of other cofactors, such as pain, depression, and a tendency to catastrophize in this population. This interpretation is consistent with our data, because our mTBI group reported more depression, catastrophizing, and anxiety than healthy controls, especially in the presence of pain. In addition, depression appears to be strongly associated with subjective sleep quality.
The relationship between sleep and pain has been suggested bidirectional: a night of poor sleep triggered more pain the next day, and intense pain was followed by frequent awakenings. 23 A recent study found an interesting relationship between sleep and pain. Pre-sleep pain did not predict sleep quality, but poor sleep was a good predictor of next morning pain rating. 44 Similarly, patients with mTBI with pain reported the same quality of subjective sleep as patients with mTBI without pain. Even though the physiological interaction between sleep and pain in general—and in mild TBI in particular—remains unclear, it is possible that central thalamic processes play a role in both complaints, with diffuse nociceptive inhibitory control and inflammation suggested as potential mechanisms. 45
The literature strongly associates pain with sleep problems in mTBI, based on questionnaires and reports. 22,25 Pain as well as post-traumatic stress disorder were also shown to be significantly associated with sleep problems, known as the “polytrauma clinical triad.” 26 As a first step toward understanding this relationship in this population, we showed that pain in acute post-trauma affected both non-REM and REM sleep qEEG. This indicates that pain, along with depression, plays a physiological role in sleep disruption after mTBI. The dominance of rapid brain activity during sleep of patients with mTBI with, in comparison with sleep of patients with mTBI without pain and control subjects suggests an activation of arousal ascending systems and may be associated with complaints of poor sleep. We recognize that such a suggestion is limited by surface electrodes recording of brain activity and that further studies using brain imaging may help clarify the relevance of this suggestion.
Our qEEG results are in line with previous findings, showing that the increase in fast waves also persists during REM sleep. This may suggest lower sensory gating during sleep in patients with mTBI with pain and an imbalance in the arousal system in insomnia conditions. It was previously suggested that hyperarousal during the sleep of insomnia patients may interfere with emotional regulation, mainly causing depression. 46 More specifically, REM instability was proposed to play a major role in non-refreshing sleep complaints, which were not shown in the sleep architecture. 47 This theory appears to fit with the data obtained in this population: patients with mTBI with pain and presenting with sleep complaints show hyperarousal, mainly during REM sleep.
Change in qEEG activity leading to sleep disruption by physiological pain has been supported by previous experimental pain paradigms. One study using pregabalin as an analgesic identified slower brain oscillation as a biomarker of central analgesia. 48 Gamma oscillatory activity increased after nociceptive stimulus and was modulated by theta waves. Moreover, oscillations greater than 20 Hz were strongly related to pain perception rating, providing evidence that gamma oscillations play a role in pain perception. The exact role of gamma oscillations during slow wave sleep remains unknown, however, although they have been related to dreams in REM sleep. 21,49,50 Increased gamma band activity during REM sleep was also thought to be from continuous sensory input. 5
Nociceptive experimental heat pain evoked moderate cortical arousal during sleep in healthy subjects. 52,53 Delta frequencies have also decreased in patients with chronic widespread pain. 54,55 A noxious stimulus during slow wave sleep induced a decrease in delta and sigma bands but an increase in alpha and beta EEG frequencies. 56 Another study in depressed patients with chronic pain showed no difference in architecture but an increase in alpha and high beta frequency bands when compared with non-depressed patients and controls. 57
One limitation of this study is the absence of a group with chronic pain without mTBI. As shown in a previous study at our laboratory, qEEG changes during sleep in widespread pain conditions showed a decrease in delta waves during sleep. 55 Another limitation of this study is the absence of matching for age and sex, factors known to influence sleep structure. At each step of our analysis, however, we corrected for age and sex effects. Another limitation of this study is that the sample used is small, regardless of our efforts of recruitment. This limitation is of major concern in many mTBI studies because of the heterogeneity of patients and high refusal rates. 58
Finally, although the long-term consequences of post-concussion symptoms remain poorly understood, they should be considered as interacting factors. The effects and interactions of other symptoms (headaches, cognitive deficits, personality changes, pain) on sleep–wake disturbances post-TBI remain to be clarified in a chronic TBI population. Future studies should address changes in sleep qEEG after administration of pain medications such as pregabalin or duloxetin, along with perceptions of sleep quality, to confirm causality between pain and qEEG changes post-mTBI.
Conclusion
Our findings indicated that pain was associated with poor sleep quality and may be related to physiological qEEG changes during sleep. Pain treatment post-TBI may favor successful rehabilitation by managing not only the pain but also sleep problems, thereby contributing to long-term management of post-concussion symptoms.
Footnotes
Acknowledgments
The authors would like to thank Sophie Pelletier and Hajar El-Alaoui for sleep data analyses, and Ariane Demers, Christiane Manzini, and Isabel Roy for study coordination and subject recruitment. This study was funded by the FRQS's Quebec Pain Research Network, a hospital trauma fund, and the Research Centre at our hospital. Dr. Lavigne is a Canada Research Chair.
Author Disclosure Statement
Dr. Lavigne serves on the scientific advisory board for Pfizer, UCB Europe, ResMed USA-CDN. No competing financial link with this study exists. For the remaining authors, no competing financial interests exist.