
Abstract
Prior pre-clinical and clinical studies indicate that early decompression of the spinal cord (≤24 h post-trauma) may have benefits regarding clinical outcomes and neurological recovery after spinal cord injury (SCI). This study examines the benchmarking of management of patients with acute traumatic cervical SCI in order to determine the potential barriers and ideal timelines for each step to early surgical decompression. We reviewed patient charts and the Surgical Trial in Acute Spinal Cord Injury Study (STASCIS) forms regarding the time and reasons for delay of each step in the management of patients with SCI. The reasons for delays were classified into: 1) health care-related (“extrinsic”) factors and 2) patient-related (“intrinsic”) factors. The cases were grouped into patients who underwent early surgical decompression of spinal cord (early-surgery group) and individuals who underwent later decompression (later-surgery group). Whereas both groups showed comparable time periods related to intrinsic factors, patients in the early surgery group had a significantly shorter time period associated with extrinsic factors when compared with the later surgery group. Both groups were comparable regarding pre-hospital time, time in a second general hospital prior to transfer to a spine center, and time in the trauma emergency department. Patients in the early surgery group had a significantly shorter waiting time, shorter waiting time for assessment by a spine surgeon, and a shorter waiting time for a surgical decision than did the later surgery group. Our benchmarking analysis suggests that health-related factors are key determinants of the timing from SCI to spinal cord decompression. Time in the general hospital and time of waiting for a surgical decision were the most important causes of delay of surgical spinal cord decompression. Early surgery is possible in the vast majority of the cases.
Introduction
T
Over the past three decades, there has been reported an increase in the life expectancy of individuals after SCI in North America. 4 Extensive implementation of prevention measures, safety legislation, and public education initiatives as well as improvements in and wider availability of emergency and trauma systems are among the major reasons for the decrease in death and disability following SCI. 5 Despite all this progress in the prevention and management of spinal cord injury, further improvements in the care of spinal cord injured patients seems tangible prior to any potential breakthrough from promising pre-clinical neuroprotective and regenerative strategies.
Based on the emerging evidence from pre-clinical and clinical studies, the early surgical decompression of spinal cord after SCI could potentially improve clinical and neurological outcomes and reduce health care costs. 6 Recently, the results of the Surgical Treatment for Acute Spinal Cord Injury Study (STASCIS), which is a multicenter, prospective study comparing early (up to 24 h from the trauma) versus later surgical decompression of spinal cord in the management of acute traumatic cervical SCI, have been reported. 7 This prospective, multicenter, comparative effectiveness study demonstrated that that early (within 24 h of injury) surgical decompression of the spinal cord is associated with improved neurological outcomes. This study and recent consensus statements from AOSpine and the Spine Trauma Study Groups, would suggest that early surgical decompression for patients with cervical SCI should be considered a best practice, because it reduces the degree of neurological impairment. 7,8
Given this background, we sought to examine the process benchmarking of the management of acutely spinal cord injured patients in order to determine the potential barriers in patient care leading to delayed surgical decompression following acute traumatic cervical SCI. Process benchmarking is a function whereby a specific process is compared against a gold standard. Here, we sought to determine the processes in care by which acute traumatic cervical SCI patients ended up undergoing a delayed surgical decompression, and compare them against the processes in care by which other patients with a similar injury underwent an early decompression, the latter representing a proposed best practice. From this, we sought to identify potential barriers and correctible delays in the management of patients with acute traumatic cervical SCI.
Methods
The University Health Network Research Ethics Board approved this study protocol. All data for this study were collected from charts and the STASCIS forms from the patients that were treated at the Toronto Western Hospital. The main data included the periods of time for each step in the management of spinal cord injured patients as well as the reasons for delay to a decision for surgical decompression of the spinal cord.
Based on the flow chart in Figure 1, the periods of time for each step in the management of spinal cord injured patients were determined. The reasons for delays in the management steps were classified into: 1) health care-related (“extrinsic”) factors and 2) patient-related (“intrinsic”) factors (Fig. 1). The extrinsic factors included any barrier to the early spinal cord decompression that is related to the health care process of patient's management (e.g., delayed transfer to spine trauma center, tardy specialist assessment, late access to imaging evaluation). The extrinsic factors can be potentially modified by changes in clinical practice guidelines, modification in hospital policy and, more extensively, implementation of health care policy that enhances the health care process to favor early spinal cord decompression strategy. In contrast, the intrinsic factors are associated with the clinical condition (e.g., hemodynamically unstable patient) and decision process that are specific to patients.
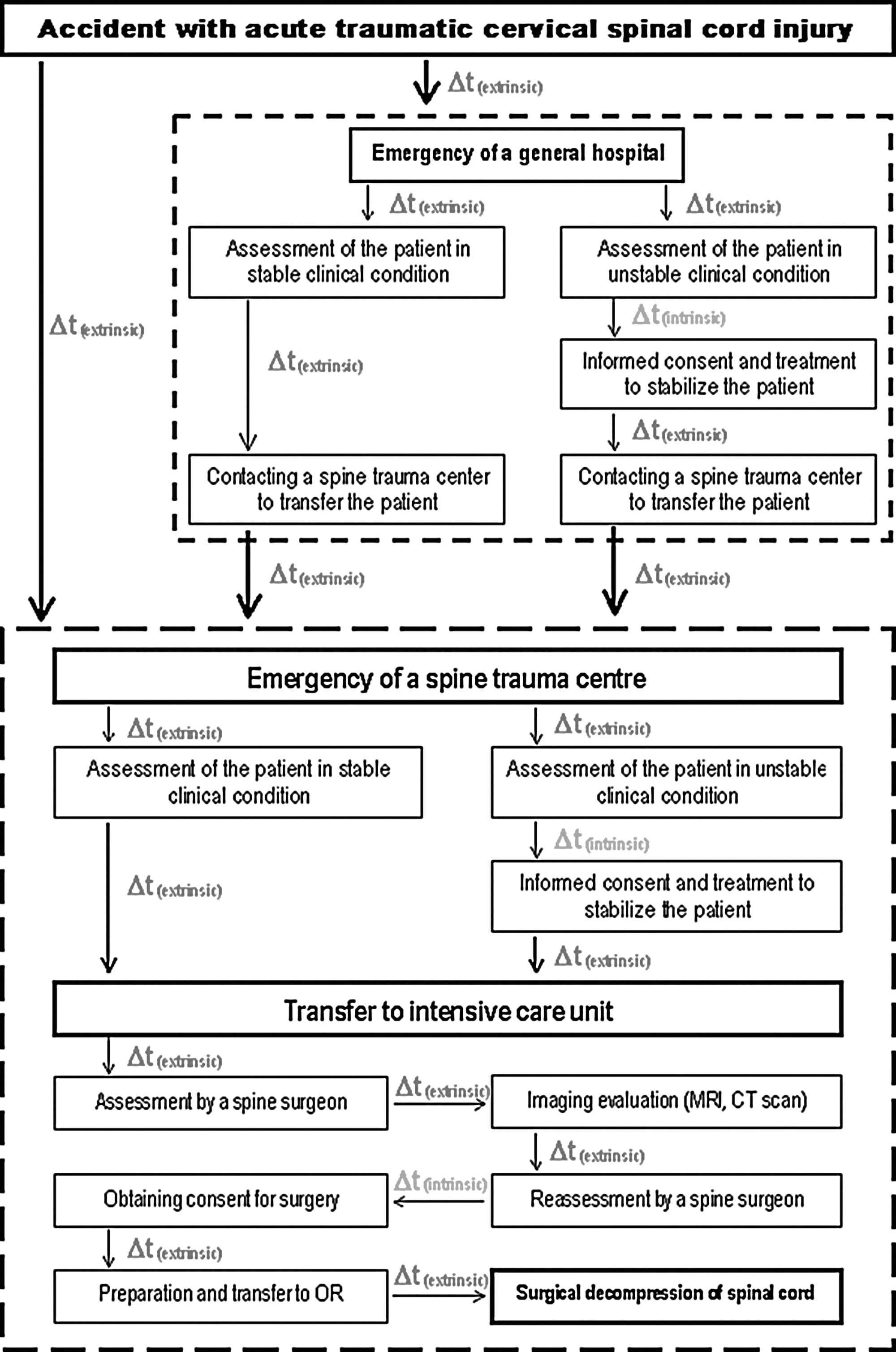
Flow chart of the management of spinal cord injured patients from injury to surgical decompression of spinal cord.
The cases were grouped into patients who underwent early surgical decompression of the spinal cord (up to 24 h since the injury) and individuals who underwent later surgery (>24 h after injury). Mann–Whitney U test and Fisher's exact test were used for the comparisons between the two groups of patients regarding continuous variables and categorical variables, respectively.
Statistical analysis
All data analyses were performed using the SAS program (version 9.03; SAS Institute Inc., Cary, NC).
Results
There were no statistically significant differences between both groups of patients with regard to their age at the time of SCI, gender distribution, severity of SCI, and length of stay in the acute care SCI unit (Table 1).
SCI, spinal cord injury; SEM, standard error of mean; AIS: American Spinal Injury Association (ASIA) Impairment Scale.
No intrinsic factor was found in either study group and, hence, both patient groups showed comparable periods of time related to intrinsic factors (Fig. 2). However, the group of patients who underwent early surgical decompression of the spinal cord had a significantly shorter period of time associated with extrinsic factors when compared with individuals who underwent later surgical decompression (19.16 vs. 71.28 h, respectively; Fig. 2). In addition, the group of patients who underwent early surgical decompression was comparable with the group of patients who underwent later surgical decompression with respect to the pre-hospital period of time (137 vs. 185.5 min, respectively; Fig. 3), period of time in a second general hospital prior to transfer to a spine center (369.5 vs. 730.8 min, respectively; Fig. 3), and period of time in the emergency department of a spine center (221.7 vs. 226.4 min, respectively; Fig. 3). Moreover, the group of patients who underwent early surgical decompression had a significantly shorter waiting period of time in the first care general hospital (577.6 vs. 1982.1 min, respectively; Fig. 3), a shorter waiting time for assessment by a spine surgeon (73.5 vs. 274.4 min; Fig. 3) and a shorter waiting time for a decision regarding surgical management (241.7 vs. 832.3 min; Fig. 3).
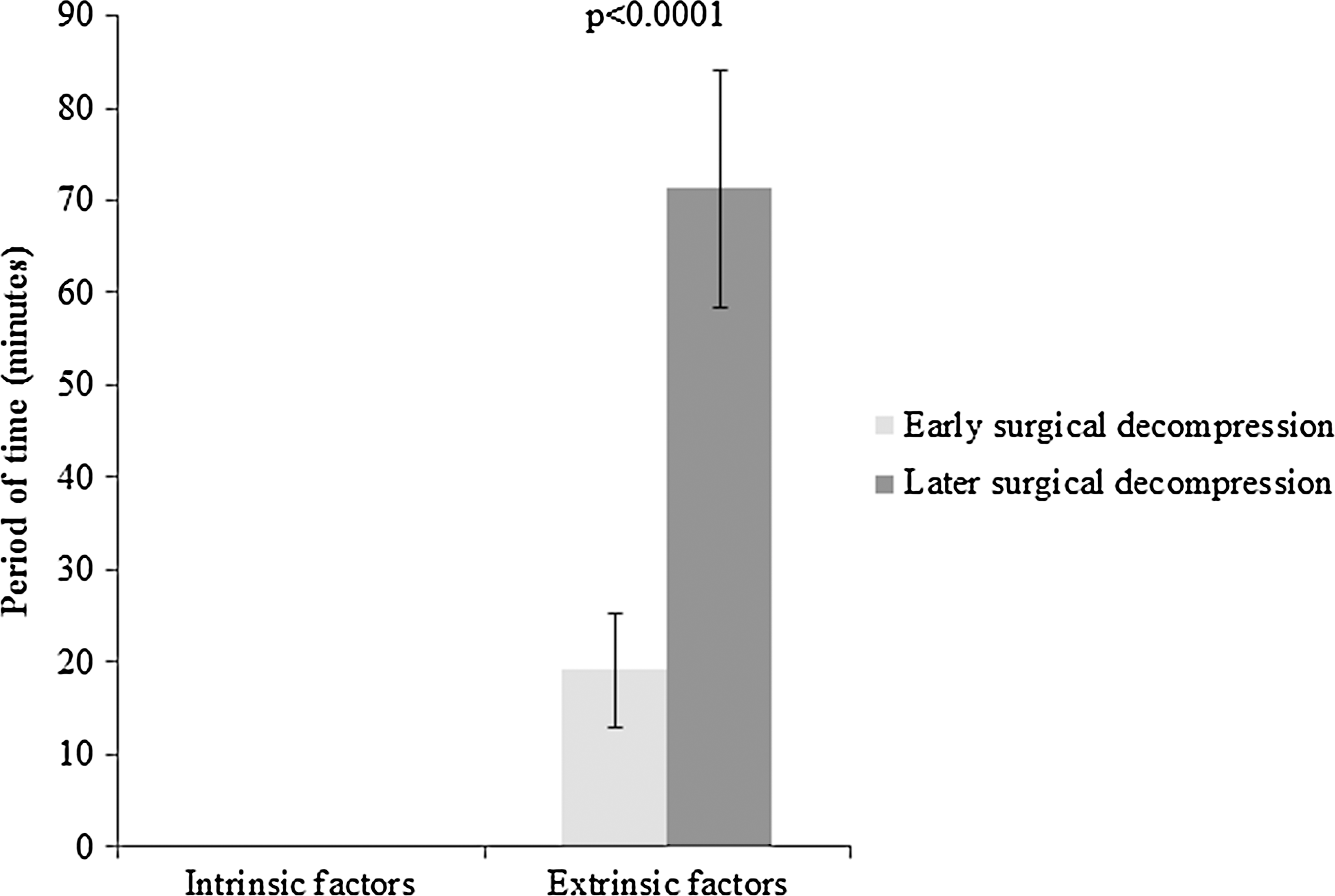
Comparisons between both patient groups with regard to the periods of time related to intrinsic factors and the periods of time related to extrinsic factors. Only the significant p value was included.

Comparisons between both patient groups with regard to the periods of time related to different extrinsic factors identified in our study. Only the significant p value was included.
The proportion of patients who were seen in one general hospital, two general hospitals, or three general hospitals prior to being transferred to a spine center in either study group is shown in Figure 4. The majority of the cases in either study group were seen in two general hospitals before being transferred to a spine center (Fig. 4). Nonetheless, there were no significant differences between both groups with regard to the percentage of cases that were seen in one general hospital, two general hospitals, or three general hospitals prior to being transferred to a spine center (Fig. 4).
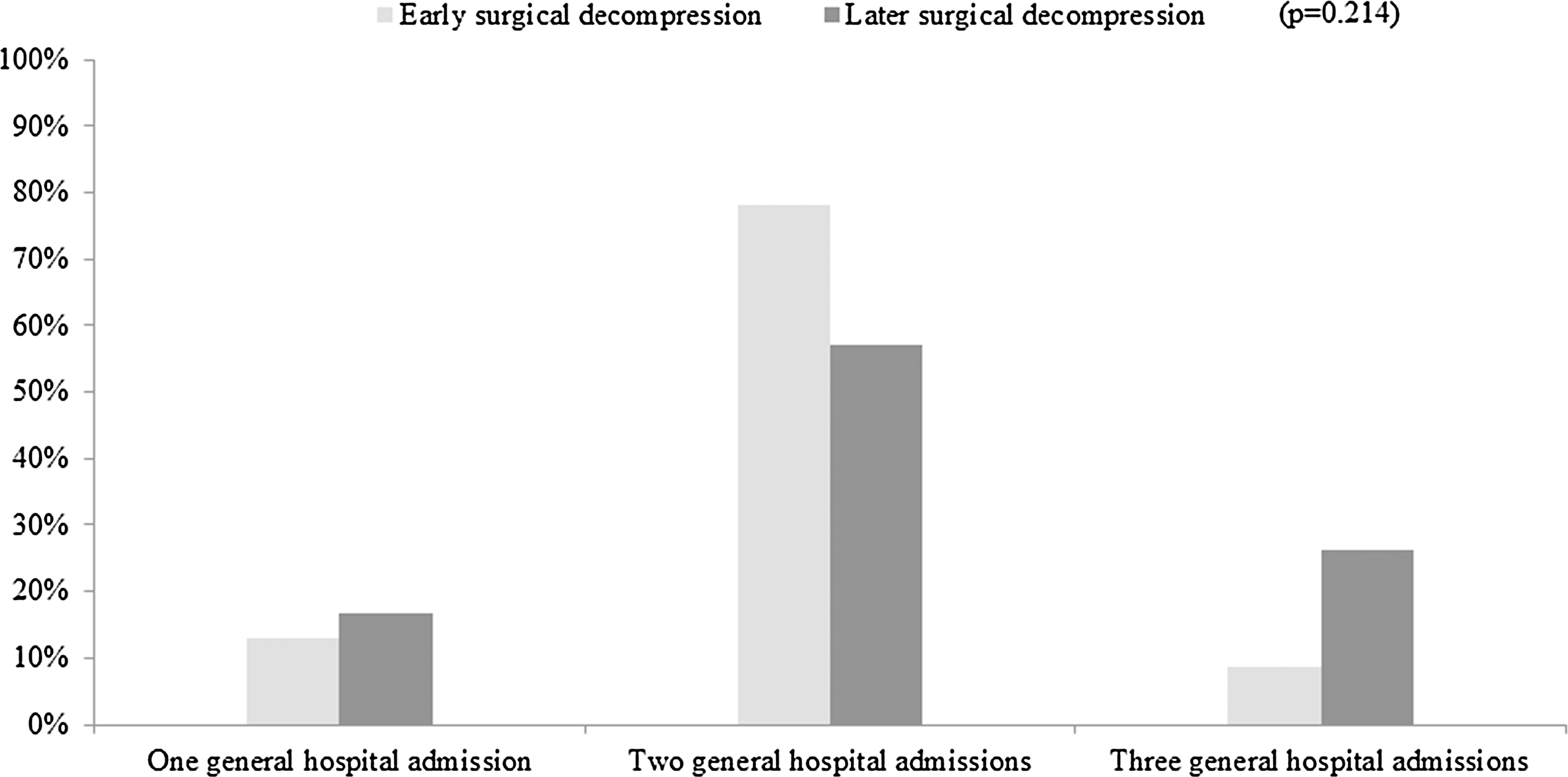
Comparisons between both patient groups with regard to the percentage of cases admitted to one, two, or three general hospitals prior of being transferred to a spine center.
Discussion
Our process benchmarking suggests that the group of patients who underwent early surgical decompression of spinal cord had significantly shorter periods of time related to extrinsic factors in comparison with the group of patients who underwent later surgical decompression. The period of time in a general hospital and the period of time waiting for a surgical decision were the most important causes of delays for surgical spinal cord decompression. However, both groups of patients were comparable with regard to the periods of time related to intrinsic factors. These data indicate that there are significant opportunities to correct systems-related issues that result in delays in transferring patients with an acute SCI to a center that can deliver definitive care. Given the emerging data from the STASCIS, such delays could impact on neurological recovery, degree of disability, and complications.
To our knowledge, this is the first study focused on process benchmarking on the surgical decompression of spinal cord following traumatic cervical SCI. The properly conducted benchmarking can measure differences in clinical practice and can discern methods that can improve patient care delivery. 9 A genuine benchmarking provides consistent reference points, utilizes real time and current data, facilitates the establishment of new management tools, and is focused on organizational resources. 9 Our study is a legitimate and original benchmarking that indicates early surgical decompression of the spinal cord as a real option for the vast majority of the cases of acute traumatic cervical SCI. This study also identifies health-related factors that need to be modified in order to improve clinical practice and, consequently, quality of patient care. In our study, an important health-related factor was delay in the transfer of patients from general hospitals for different reasons, including wait for a specialist consultation, wait for investigations, and wait for transportation to the spine center. Delay in the surgical decision for patients admitted to a spine center was another significant health-related factor that caused delay in the management of some patients with acute traumatic cervical SCI. Those health-related factors were considered “modifiable,” as the patients were clinically stable and suitable for transfer, and, in theory, adjustments in the logistics prioritizing the management of patients with acute traumatic cervical SCI could reduce the timing from injury to spinal cord decompression.
Based on these data from a single institution in Ontario (Canada), one can speculate that two main policy changes would favor reduction of the timing from SCI to surgical decompression of spinal cord following acute traumatic cervical SCI. First, unnecessary delays in a general hospital could be avoided by a provincial policy that would mandate prompt transfer of a clinically stable patient with acute traumatic cervical SCI to a spine trauma center. The present guidelines for treatment of acute traumatic SCI reinforce this strategy because, as per current clinical evidence, patients with acute SCI who are treated in a spine trauma center by a team of specialists have more favorable outcomes. 10 Second, institutional policies should provide support for prompt assessment by a spine surgeon of those patients with acute traumatic SCI. It is of note that such a province-wide policy is currently being examined in Ontario based on the data from STASCIS.
Although process benchmarking is primarily designed to improve clinical practice, its customary use can also optimize time and save financial resources in participating organizations. 9 Given the improved neurological outcomes that are seen with earlier surgical interventions, it is likely that any incremental increases in costs associated with ensuring that early surgical intervention for SCI is undertaken would be offset by cost savings in terms of reduced health care expenditures to deal with secondary complications, as a result of improved neurological outcomes. Such cost-effectiveness analysis is currently being undertaken by our group.
Conclusion
In conclusion, our process benchmarking suggests that health-related factors are key determinants of the timing from SCI to spinal cord decompression. More specifically, period of time in a general hospital and period of time waiting for surgical decision were the most important causes of delays for surgical spinal cord decompression in our study. However, early decompression of spinal cord is possible in the majority of the cases of acute traumatic cervical SCI if the logistics for transfer from general hospitals and for management of those patients are modified in order to reduce the time from injury to spinal cord decompression.
Study limitations
The present study includes prospectively collected data that, for the first time, compares early versus later surgical decompression of the spinal cord after acute traumatic cervical SCI. However, only the 63 patients surgically treated at the Toronto Western Hospital were enrolled in this process benchmarking. This is a spine trauma center in Toronto (Ontario) where all patients had the coverage of the Ontario Health Insurance Plan (OHIP), which is a publicly funded insurer with universal and equal access to every insured. Whereas the number of cases would be considerably larger if all 313 cases enrolled into the STASCIS had been included, the results would be difficult to interpret, because different centers in North America participated in the STASCIS, and the health system is considerably different in other jurisdictions. Finally, the apparent difference between the two study groups regarding the median length of stay in the spine trauma center can be explained by the larger variation in the values of length of stay in the group of patients who underwent early surgical decompression. Whereas the smaller number of cases in that study group accounts for some of the variation, there are potentially other reasons that cannot be identified in our data.
Footnotes
Acknowledgment
This study was supported by a Spinal Cord Injury Solutions Network Rapid Response Award from the Rick Hansen Foundation.
Author Disclosure Statement
No competing financial interests exist.