
Abstract
In this single-center, double-blind, randomized, sham-controlled, prospective trial at the U.S. Air Force School of Aerospace Medicine, the effects of 2.4 atmospheres absolute (ATA) hyperbaric oxygen (HBO2) on post-concussion symptoms in 50 military service members with at least one combat-related, mild traumatic brain injury were examined. Each subject received 30 sessions of either a sham compression (room air at 1.3 ATA) or HBO2 treatments at 2.4 ATA over an 8-week period. Individual and total symptoms scores on Immediate Post-Concussion Assessment and Cognitive Testing (ImPACT®) and composite scores on Post-traumatic Disorder Check List-Military Version (PCL-M) were measured just prior to intervention and 6 weeks after completion of intervention. Difference testing of post-intervention means between the sham-control and HBO2 group revealed no significant differences on the PCL-M composite score (t=−0.205, p=0.84) or on the ImPACT total score (t=−0.943, p=0.35), demonstrating no significant effect for HBO2 at 2.4 ATA. PCL-M composite scores and ImPACT total scores for sham-control and HBO2 groups revealed significant improvement over the course of the study for both the sham-control group (t=3.76, p=0.001) and the HBO2 group (t=3.90, p=0.001), demonstrating no significant HBO2 effect. Paired t-test results revealed 10 ImPACT scale scores in the sham-control group improved from pre- to post-testing, whereas two scale scores significantly improved in the HBO2 group. One PCL-M measure improved from pre- to post-testing in both groups. This study showed that HBO2 at 2.4 ATA pressure had no effect on post-concussive symptoms after mild TBI.
Introduction
S
Following mTBI, the persistence for more than 3 months of injury-related symptoms is known as post-concussion syndrome (PCS). 4 While the incidence of PCS in civilians is typically 15% at 3 months and 3–5% at 1 year, preliminary findings indicate it is considerably higher in SMs and veterans from the current Middle East conflicts. 5 While the causes of this increased incidence are probably multifactorial and remain under investigation, the challenges of treatment for this significant percentage of the military and veteran populations have resulted in a number of proposed interventions varying from comprehensive algorithmic guidelines to single-modality treatments. 6 One potential therapy that has gained advocacy is hyperbaric oxygen. Hyperbaric oxygen (HBO2) administration involves breathing high levels of oxygen, usually 100%, at an increased pressure of at least 1.4 times greater than the atmospheric absolute pressure at sea level (1 atmosphere absolute or ATA, which is equivalent to 760 mmHg partial pressure of oxygen). 7 Unlike oral or intravenous medications measured in milligrams, individual dosages of hyperbaric oxygen are measured in partial pressures of oxygen multiplied by time for each treatment. Unless otherwise specified, 100% oxygen is assumed as the breathing gas. For example, air composed of 21% oxygen will have an oxygen partial pressure of 160 mmHg at sea level (760 mmHg×0.21×1.0), but breathing 100% oxygen at 2.0 ATA would have a partial pressure of 1520 mmHg (760 mmHg×1.0×2.0).
The intent of HBO2 therapy is to increase the oxygenation of the blood and tissues of the patient to supraphysiological levels. The partial pressure of oxygen will increase proportionally with an increase in the hyperbaric chamber compression pressure. The arterial oxygen tension in patients receiving this therapy may exceed 2000 mmHg, and oxygen tension in the tissues may reach 400 mmHg compared to the normal levels of 40–95 mmHg at sea level pressure breathing air. 7 The use of HBO2 in treating TBI is based on the still unproven theory that functionally retrievable neurons, adjacent to severely damaged or dead neurons, exposed to hyperbaric oxygen may return to normal function or near normal function by reactivating metabolic or electrical pathways. Other possible mechanisms of benefit to TBI patients include stem cell mobilization to sites of injury, immune modulation, and impact on fundamental neurotransmitters such as nitric oxide. Anecdotal reports suggest the benefits of treatment may diminish post-injury, as the interval from injury to HBO2 increases, but the optimal “therapeutic” window is unknown as is the optimal oxygen dose. Harch and colleagues 8 reports treating PCS patients at 1.5 ATA for 60 min. A typical HBO2 clinical treatment uses oxygen at 2.0–3.0 ATA for durations of 90–120 min. The dose, the total number of treatments per patient, and the time elapsed between treatments vary widely depending on the clinical indication. 7 Some advocate the use of lower treatment pressures for traumatic brain injury. 8 –10
Serious side effects are rare, and individuals with TBI have been successfully studied using HBO2 safely. 11 Potentially adverse effects include barotrauma to the middle ear or sinuses, temporary myopia, claustrophobia, and oxygen toxicity seizure (incidence of 0.03%). Pulmonary barotrauma is extremely rare and generally has been reported only in patients with severe underlying lung disease. 7
This investigation examined the effects of HBO2 on a population of active-duty SMs with PCS resulting from combat-related mTBI in a randomized, blinded, sham-controlled trial and is the first such study in patients with PCS. This study is part of a comprehensive DoD and Department of Veterans Affairs (VA) collaborative initiative involving three ongoing independent, randomized, blinded trial efforts utilized to develop hypotheses for a definitive Phase III clinical trial. 12 These trials utilize varying HBO2 doses and clinically relevant, consistent measures of outcome addressing physical, cognitive, and behavioral functioning. Given the large numbers of individuals experiencing these injuries and the paucity of proven treatments, the current study and its companion studies take on added clinical significance and military relevance.
Methods
As part of the DoD-VA collaborative research program, the Air Force Medical Support Agency Medical Modernization Directorate and the 711th Human Performance Wing sponsored this single center, single-blind, randomized, controlled trial of HBO2 exposure on symptomatic mTBI that commenced in 2009. Although originally designed as a single-blind study, it was successfully administered as a double-blind study with both the separate teams administering the hyperbaric chamber interventions and the outcome measures blinded to the intervention group (hyperbaric oxygen or sham-control). The logistics of the challenges of double-blinding hyperbaric chamber interventions are described elsewhere. 11 The study received appropriate institutional review board and governmental approvals prior to initiation of research activities. Fifty active-duty military SMs with post-concussion syndrome were recruited from United States military bases. The appropriate sample size estimates were calculated for the cognitive test outcomes, which required 20 subjects in each group (Rho=0.84, power 0.80, effect size=0.66). Inclusion criteria were neurologist-confirmed TBI diagnosis based on the DoD definition of TBI, 13 cognitive disruption (as demonstrated by diagnosis and therapies), injury occurrence more recent than October 2001, psychiatric status (if any) stable for 2 months, stable psychotropic medication history for at least 1 month, and ability to use computerized testing. The diagnosis of TBI was confirmed by the study neurologist's history, physical examination, and review of all acute medical records, including battlefield information (when available), from the time of the traumatic event to the present, using the DoD definition of TBI. The only exclusion criteria were the presence of a disorder that contraindicated hyperbaric exposure or previous exposure to HBO2. Forty-three (86%) of the subjects were Marines from Camp Lejeune Marine Base (NC), Quantico Marine Base (VA), and Twenty-nine Palms Marine Base (CA). The remaining participants were from U.S. Army or U.S. Air Force from other bases. Most participants received temporary duty orders to relocate to Ft. Sam Houston, Texas, for 2 months to receive the investigative chamber sessions at the U.S. Air Force School of Aerospace Medicine (Brooks City-Base, TX). Demographic information; clinical parameters; and baseline physical, cognitive, and behavioral functioning measures were obtained (“pre-exposure” assessment; Figs. 1, 2). Participants were randomly assigned to either a sham-control or HBO2 exposure group. Randomization to the exposure groups was done using a computer-generated number assignment (randomizer.org). The sham-control simulated a placebo exposure.
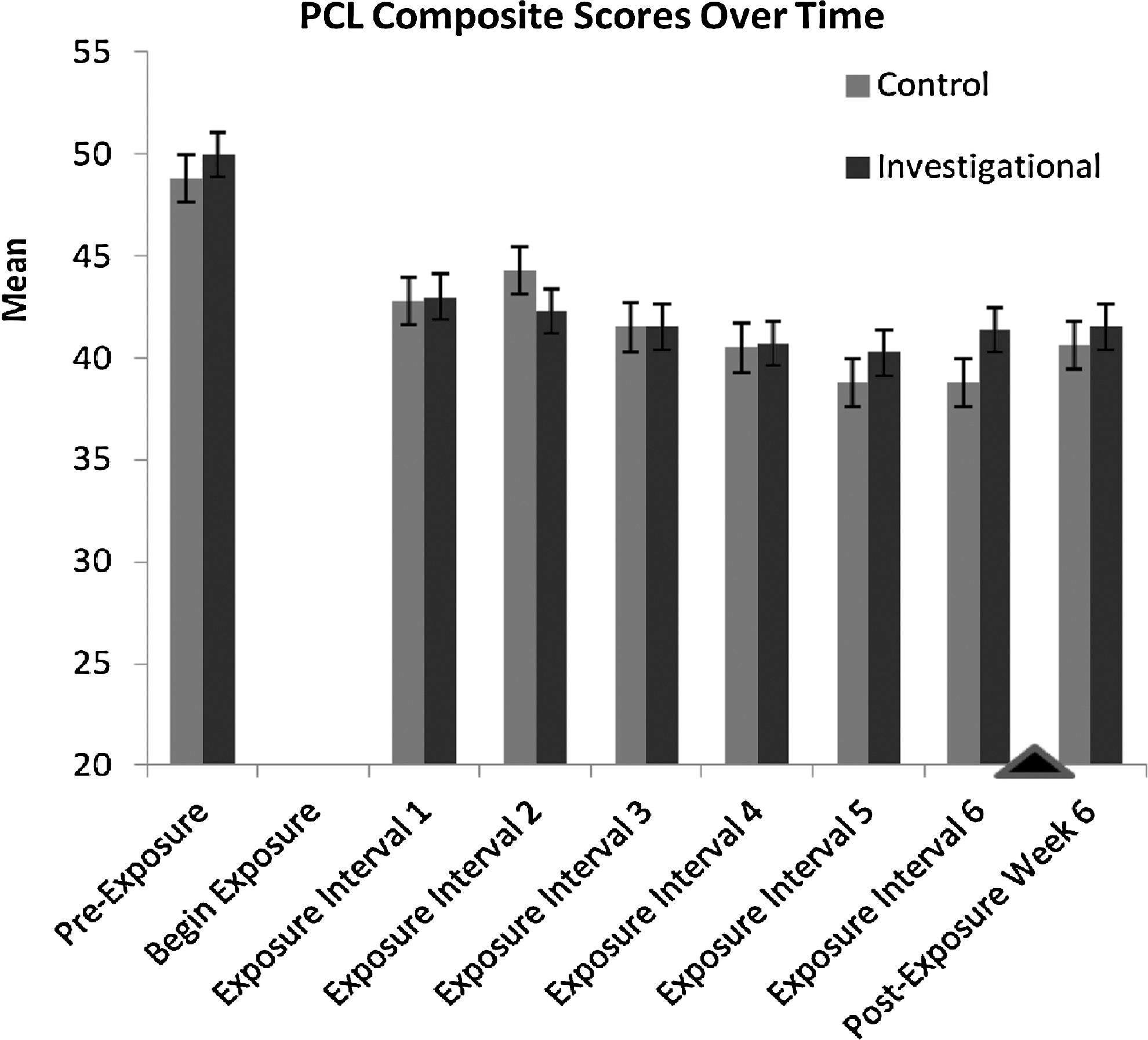
PCL composite score over time. “Pre-exposure” to “begin exposure” interval and all six exposure intervals were between 7 and 10 days, depending on participant availability and tolerance of successive chamber exposure. Post-exposure assessment was performed 6 weeks after last chamber exposure.
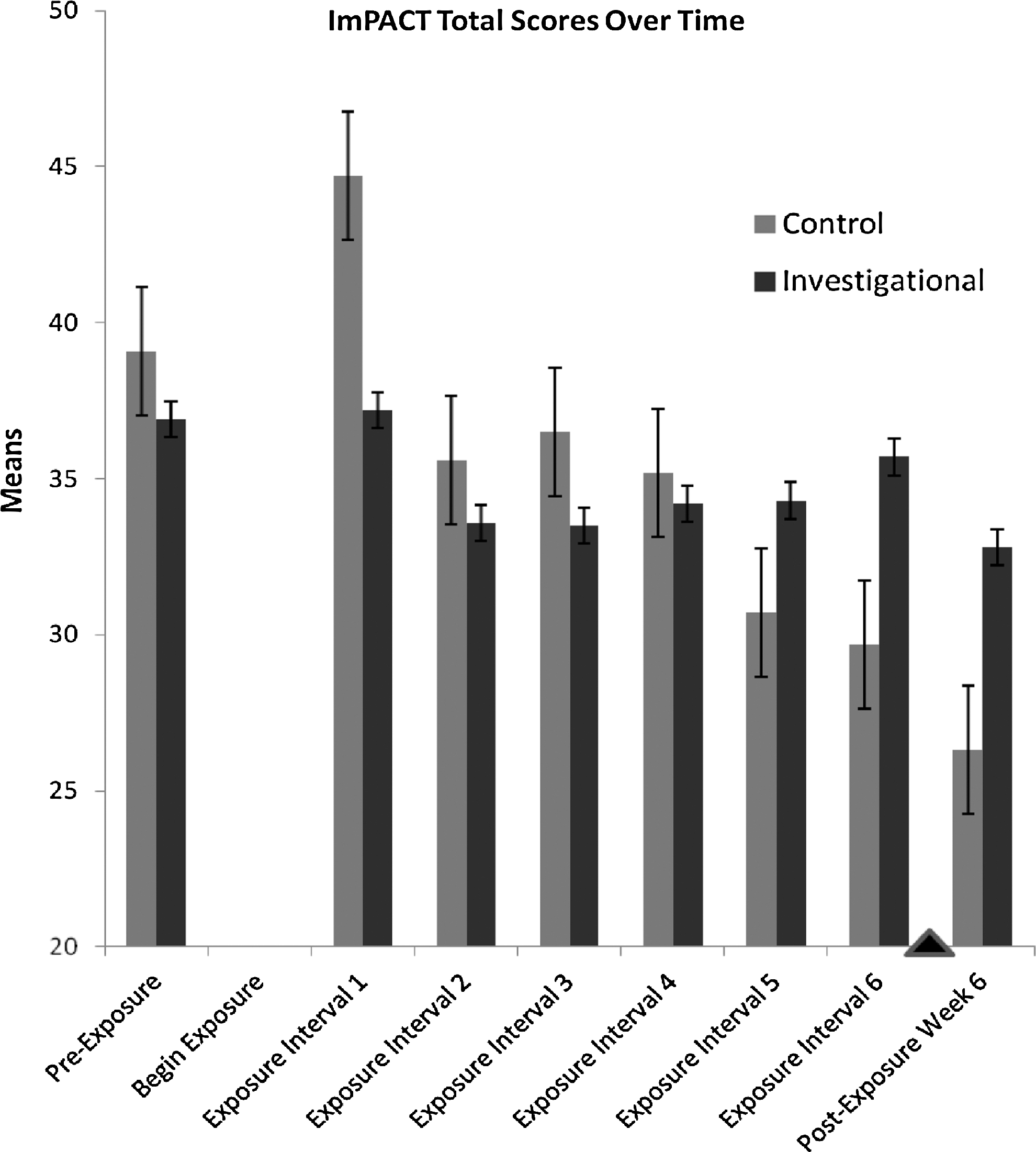
ImPACT total scores over time. “Pre-exposure” to “begin exposure” interval and all six exposure intervals were between 7 and 10 days, depending on participant availability and tolerance of successive chamber exposure. Post-exposure assessment was performed 6 weeks after last chamber exposure.
The intervention dosing used in this study was chosen based on a clinical HBO2 dose recommended as appropriate for most conditions endorsed by the Undersea and Hyperbaric Medical Society. 7 The intervention group breathed 100% oxygen at 2.4 ATA for 90 min, 7 and the sham-control group breathed air (21% O2) for 90 min at 1.3 ATA (about the pressure at 11 feet of sea water) with a slow drift to 1.2 ATA. Exposures were conducted in a multi-place chamber with the breathing medium delivered using an oxygen treatment hood (Amron International, Vista, CA) once the exposure pressure was reached to ensure a consistent dose. Blinding techniques using hyperbaric chambers are difficult and require diligence to accomplish. This study used previously published techniques as a basis. 11,14,15 The exposures had a 7-min compression time followed by 90 min of oxygen or air inhalation broken into three 30-min periods. Intermittent 10-min air breaks were given by removing the hood. Air breathing periods are often used during many HBO2 exposures to reduce oxygen toxicity. 7,16 Exposures were done on weekdays only. Participants completed five exposures followed by 1 day given to complete other aspects of the study. The cycle was repeated for a total of 30 exposures over an 8-week period.
In addition to the baseline measures, subsequent outcome measurements were obtained after 5, 10, 15, 20, 25, and 30 chamber exposures and 6 weeks after completion of the exposures (“Exposure intervals 1–6” and “Post-exposure week 6” assessments, respectively; Figs. 1, 2). While an array of outcome batteries was utilized for all participants, to derive clinically relevant information, this initial paper focused solely on the symptomatic effects of the chamber exposures measured by the self-report symptom scales included in Immediate Post-Concussion Assessment and Cognitive Testing
17
(ImPACT® Applications;
Results
One hundred and three SMs with PCS from presumed TBI volunteered for study participation. Fifty of the 103 candidates screened met the study criteria and were consented (49%). There were 22 candidates (21%) who did not qualify for the study, primarily due to the inability to confirm the diagnosis of TBI. Eight candidates (8%) agreed to participate but were deferred, usually due to medication changes or schedule conflicts, and the study closed out before they could be enrolled. Twenty-three candidates (22%) were eligible but later requested not to participate, primarily due to schedule conflicts or personal reasons. There was one withdrawal from each group for personal (i.e., family) reasons related to obtaining the needed time off for the protocol (Fig. 3).
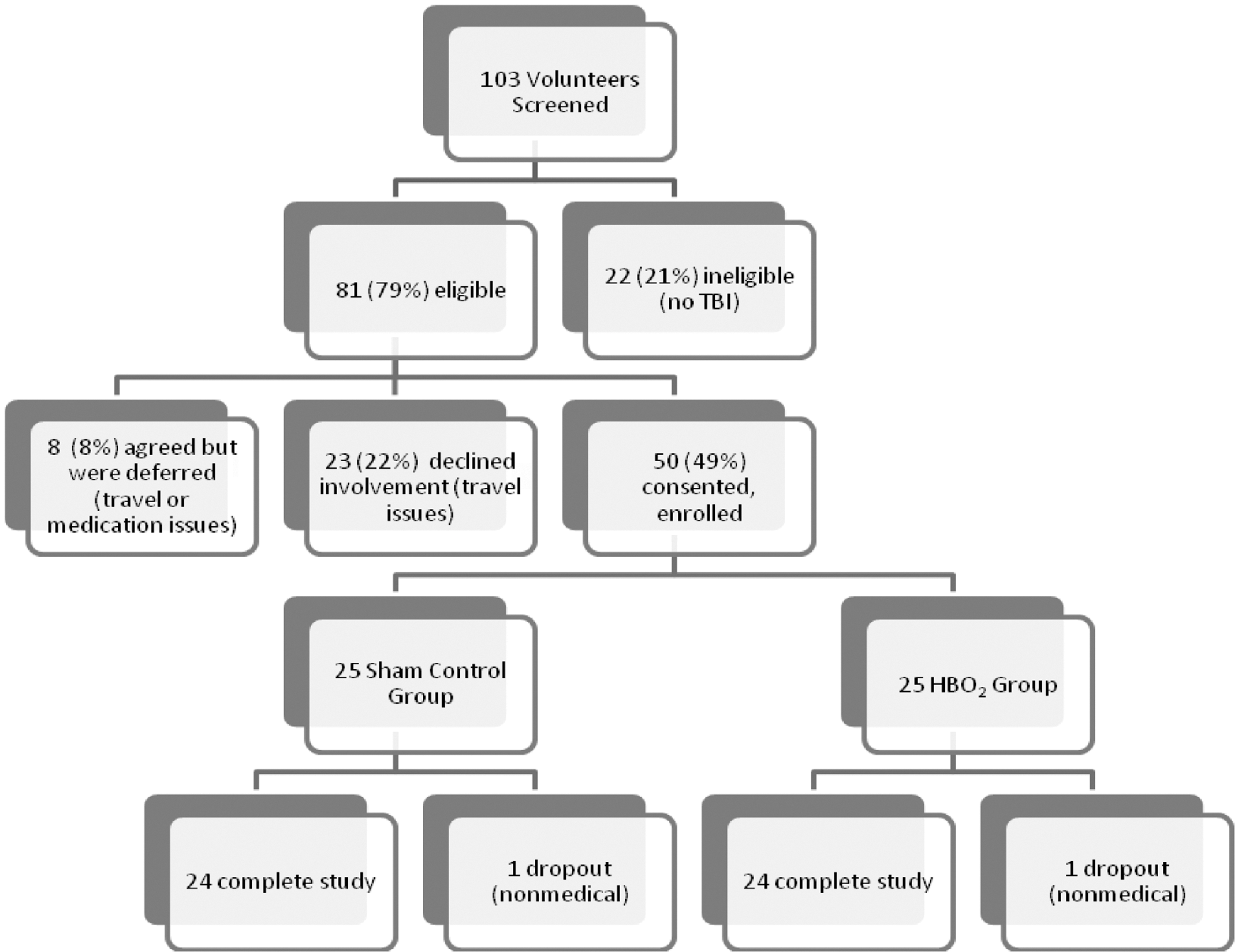
Recruitment, eligibility, and consent process for the 25 HBO2 subjects and the 25 sham control subjects. One non-medical dropout occurred in each group.
The fifty volunteers who consented were randomly divided into the sham control or HBO2 exposure groups, 25 in each group. The two groups were examined for equality prior to treatment to assess the success of randomization, and an allocation questionnaire at the end of the study revealed a distribution that suggested the blind was maintained. All participants in the study suffered a TBI within the range of 3–71 months prior to the start of chamber sessions. Forty-eight were male. Three participants were not classified as mild TBI at the time of initial injury due to duration of loss of consciousness of >1 h. Mean period of loss of consciousness for both intervention groups was <15 min. All had sufficiently recovered to meet inclusion criteria. Etiology of concussion included 33 from improvised explosive device blast, 8 from direct head trauma, and 9 from both events. Participants self-reported a mean of 3.4 concussions (range, 1–50) prior to the injury, making them eligible for the study, with mean prior episodes of loss of consciousness of 1.6 (range, 0–9).
The entire range of subject ages was 20 to 51 years of age, with a mean of 28.3 years and a standard deviation (SD) of 7.7 years. There were 24 males in each group. The age range was 21 to 46 years in the sham-control group, with a mean of 28.4 years and an SD of 7.4 years. The age range was 20 to 51 years old in the HBO2 group, with a mean of 28.3 years and an SD of 8.1 years. Mean education level was slightly over 12 years. Nearly 90% were enlisted rank and the remainder was officers.
Descriptive statistics were used to calculate means and standard deviations for total ImPACT symptom inventory and PCL-M items, using SPSS, V.14.0 (SPSS Inc., Chicago, IL). No significant differences between groups were noted on the ImPACT scale scores or on the PCL-M at baseline testing, except for a greater degree of nausea at baseline in the sham-control group (t=0.244, p=0.009). Difference testing between the sham-control and HBO2 groups did not reveal any significant differences on the PCL-M composite mean score (t=− 0.205, p=0.84) or on the ImPACT total mean score (t=−0.943, p=0.35) at any time (Figs. 1, 2), including at 6 weeks post-exposure (Table 1). Graphs of PCL-M composite scores (Fig. 1) and ImPACT total scores (Fig. 2) for sham-control and HBO2 groups revealed significant downward trends over the course of the study for both the sham-control group (t=3.76, p=0.001) and the HBO2 group (t=3.90, p=0.001); however, these effects diminished on the PCL-M by the last two assessment periods (“Exposure interval 5” to “Exposure interval 6” and “Exposure interval 6” to “Post-exposure week 6” assessments, respectively; Figs. 1, 2).
p=significant.
Individual symptom scale pre-intervention testing was compared to the 6-week post-exposure testing for both the ImPACT and PCL-M (Tables 2 and 3). Paired t-test results revealed 10 ImPACT symptom scale scores in the sham-control group that differed from pre-exposure to 6-week post- exposure testing, whereas only two scale scores significantly changed in the investigational group. Two ImPACT items (sleep onset problems and sleeping less than usual) changed in both the sham-control and HBO2 groups. No improvement in headaches, concentration, or memory was noted in the HBO2 arm. In pre-exposure to 6-week post-exposure testing on the PCL-M, both the sham-control and HBO2 groups showed significant decrease in arousal-related symptoms but no differences on re-experiencing phenomena or avoidance behaviors. While there is overlap between the self-report symptoms measured by the PCL-M and ImPACT, there was not a statistically significant correlation found in this analysis (r=0.006, n=48, p=0.968). There was also no significant association between the severity of PCL-M scores and response to intervention. Additionally, there was not a significant association between the duration of symptoms or time since injury and the response to intervention.
p=significant.
p<0.05.
Discussion
This investigation represents the first randomized, controlled clinical trial studying clinically relevant effects of HBO2 on PCS and is part of a comprehensive DoD-VA collaborative initiative to clarify the role of HBO2 in mTBI care. In this study, there were significant differences within groups on both the PCL composite score and the ImPACT total score from pre-intervention and 6-week post-intervention; however, there were no significant effect differences between the sham-control condition and the investigational intervention. Our results suggest the benefits may be due to placebo, Hawthorne effect, the natural resolution of symptoms over time, 21 –23 or possibly an effect from exposure to sham-control partial pressures of oxygen or nitrogen. If the sham pressure had remained at 1.3 ATA for the entire duration of the exposure, this would be equivalent to a partial pressure of 207 mmHg or similar to breathing enhanced oxygen of 27% at sea level, which is less than experienced in standard rebreather masks used in ambulances and hospitals. Additionally, as the eventual pressure for the sham-control group was 1.2 ATA, this is even less of a consideration. In addition, the potential effects of a change in living environment (i.e., not their permanent duty base) and daily routine (i.e., non-regular duties) may contribute to the improvements in symptoms (sleep onset and duration, arousal) seen over the 14-week period.
These results reproduced the overall clinical and statistical improvements seen in case reports and series of HBO2 and TBI, but this investigation offers significant advances over previous reports. 8,24 –27 First, prior studies did not include randomization, blinding, or control groups, which weakened scientific rigor and potentially induced both experimenter and selection bias. The inclusion of these methods in our study leads us to conclude that benefit is not attributable to the HBO2 intervention. One would expect a sizable placebo and/or Hawthorne effect on symptoms given the intense nature of the intervention as has been reported in depression, anxiety, and PTSD randomized sham-controlled trials. 28 –30 Secondly, while Harch's work did focus on mTBI, all other studies have focused exclusively on the effects of HBO2 on acute moderate-severe TBI. The symptoms seen after chronic mTBI tend to differ from those following acute moderate-severe TBI and may be less amenable to the potential treatment effects of hyperbaric therapy. PCS symptoms tend to be milder, and even in this population of individuals with chronic difficulties, there were low levels of self-reported symptoms. Given the mild symptom severity, there are limited amounts of potential improvements, and a proposed “ceiling effect” occurs. This ceiling effect may be challenging to detect in small sample sizes and, based on depression literature, may be more prone to a placebo response. 28
There is evidence from randomized trials to support that HBO2 may improve survival in acute severe TBI but does not affect functional outcomes. 10,27 Also, based upon considerable animal experiments and randomized trials, HBO2 improves outcomes following acute carbon monoxide poisoning. 7 Clinical support for using HBO2 for subacute or chronic traumatic brain injury has been primarily based on anecdotal case data, and there are no prior randomized clinical trials investigating HBO2 for post-concussion syndrome.
This trial represents the first randomized, double-blinded, sham-controlled, prospective study of HBO2 in the symptomatic chronic mTBI population and demonstrates no significant symptomatic improvements of HBO2 at 2.4 ATA over sham-control. While it is possible the sham-control condition had a “therapeutic” effect on brain recovery, relative to the oxygen partial pressures attained during clinical hyperbaric treatments at 2.0–3.0 ATA, it seems very unlikely such a minimal dose of oxygen and nitrogen could influence brain function favorably.
As with any phase II trial, this study has a number of inherent limitations. The small sample size limits the significance of the study. Since most participants had combat exposure, the possible influence of post-traumatic stress, depression, anxiety, substance abuse, and pain likely had confounding effects on HBO2. Gathering of prior TBI history also relied on participant self-reporting, which is sensitive to subjective patient interpretation, memory, social desirability, and other covariates such as personality factors and willingness to reveal problems. Accounting for the confounding role of PTSD symptoms may be especially important, as our study demonstrated a significant reduction of PCL-M total scores in both the sham-control and HBO2 groups over time. Better understanding of this influence and other possible variables, such as repetitive mTBI in post-concussion recovery, would allow for a greater refinement of treatment protocols.
This study followed the recommendations of the Agency for Healthcare Research and Quality (AHRQ) review 26 to design studies that would add to the dose response aspect for the potential therapeutic use of HBO2 in treating mTBI. As such, it bracketed the pressure of 1.5 ATA seen in most anecdotal chronic mTBI case reports and series by using 1.3 ATA air and 2.4 ATA 100% oxygen. It is possible the dose of HBO2 used was excessive, 8 and thus the difference between groups in our study was less than it might have been with a different dose of HBO2. Future studies with lower dose HBO2 are needed to assess this and are planned as part of the DoD-VA cooperative group. 12 Other proposed treatment pressures (oxygen doses), individual treatment duration, and number of treatments may or may not have similar results. In this study, identifying subgroup cohorts, if any, that did improve may also point to more specific populations that are more likely to benefit from HBO2 therapy. As inferred in the AHRQ report, 26 HBO2 therapy to facilitate recovery for acute mild-to-moderate TBI is another area for investigation.
This study demonstrated that individuals with mTBI and PCS could be recruited and successfully tolerated the study protocol. Larger studies are planned to take into account covariates of co-morbid psychological conditions and to examine the effects of different dosing regimens. Future studies would also benefit from the addition of a waiting list or standard concussion care third arm to account for the nonspecific effects possible in sham-control treatment (such as time off from regular duties and expectational effects) and longer duration of follow-up to assess for the durability of any initial improvements.
Conclusion
Hyperbaric oxygen is a potent intervention for acute ischemic injuries that has a sound theoretical underpinning and demonstrated efficacy in dive-related injuries, soft tissue healing, and carbon monoxide poisoning. Human research trials with acute severe TBI have been inconclusive. The current study in participants with post-concussive syndrome from chronic mTBI demonstrates no efficacy in symptom relief with HBO2 at an exposure pressure of 2.4 ATA for 90 min given once daily for 30 treatments; however, both groups improved more than would be expected greater than 6 months after mTBI. Given that HBO2, in this controlled study, demonstrates no therapeutic value, requires long treatment series, is expensive, exposes patients to potential side effects, and has limited availability, clinical usage is not warranted for the management of symptoms of chronic mTBI at this treatment pressure. It is recommended that larger, multicenter, randomized, controlled (both sham-control and wait-list), double-blinded clinical trials be conducted at lower total oxygen doses as recommended by AHRQ.
Footnotes
Acknowledgments
The authors would like to recognize and thank Ms. Sheila Galvin, Traumatic Brain Injury Program Coordinator for the Wounded Warrior Regiment (USMC), for her superb service in coordinating participant requirements; Ms. Karen Guenther and the Injured Marine Semper Fi Fund for transportation support for participants; Dr. Jason Cromar (USAFSAM) for coordinating the protocol; and Drs. R. Scott Miller (U.S. Army Medical Material Development Activity, Ft. Detrick, MD), Lin Weaver (Hyperbaric Medicine, Intermountain LDS Hospital, Salt Lake City, UT), and Robert Michaelson (Southwest Center for Wound Care, Southwest General Hospital, San Antonio, TX) for reviewing the manuscript.
Author Disclosure Statement
The views expressed herein do not necessarily represent the views of the Department of Veterans Affairs, Department of Defense, or the U.S. Government.
Funding was provided by the Air Force Medical Support Agency Medical Modernization Directorate and the 711th Human Performance Wing for the primary study. The U.S. Navy Bureau of Medicine and Surgery provided contract funding for temporary duty requirements, and the U.S. Army Medical Materiel Development Activity provided funding for end of the study.
Dr. Cifu's efforts were supported, in part, through a Defense Advanced Research Projects Agency grant (N66001-09-2-206) and a contract from the U.S. Army Medical Materiel Development Activity. Dr. Carne's efforts were supported, in part, through contracts from the U.S. Army Medical Materiel Development Activity and the Defense and Veterans Brain Injury Center. The funding sources had no role in the study design, analysis, interpretation of the data, the writing of the paper, or the decision to submit the paper for publication.