
Abstract
We conducted a survey of individuals living with spinal cord injury (SCI) to determine their receptivity to participating in clinical trials of drug therapies or stem cell therapies, their anticipation of therapeutic benefits, and their tolerance to risk. A 46-item questionnaire was administered to individuals with cervical or thoracic SCI identified through a provincial database. The average age was 42 years and the individuals were, on average, 5.5 years post-injury. Receptivity to neuroprotective drug trials in the acute setting was very high, but somewhat less so for stem cell trials in the subacute or chronic (current) setting. With respect to expectation of functional benefit, approximately one third of the respondents indicated that they would want a 5–25% chance of achieving some functional recovery if enrolling in a stem cell therapy clinical trial in the current, chronic injury state. Whereas the majority typically would require the risk of spinal cord damage, cancer, infection, and nerve pain from invasive cell transplantation trials to be ≤1%, 15–30% would participate regardless of the risk of these complications. The factors associated with this high risk tolerance were gender (males>females), age (elderly>young), and self-reported knowledge of SCI research (greater knowledge>less knowledge). Injury severity or chronicity did not have a significant correlation with risk tolerance. Whereas previous studies have shown that the understanding of stem cell science is limited among individuals with SCI, here we show that many still have high hopes for the possibility of neurological benefit, are anxious to participate in invasive stem cell trials, and, in many cases, have high tolerance for risk in such trials. Taken together, the data underscore the need for careful communication with individuals with SCI to avoid unrealistic expectations and therapeutic misconception in experimental trials.
Introduction
T
The translation of novel treatments from the laboratory into clinical trials is a complex process that involves a full spectrum of collaboration among scientists, clinicians, granting agencies, regulatory bodies, and commercial entities. The voices of individuals living with SCI remain somewhat peripheral in this context and are, arguably, typically overlooked. 3 As was demonstrated almost a decade ago in the seminal survey conducted by Kim Anderson, the opinions of individuals living with SCI can provide a valuable perspective for the scientific research community. 4 This survey revealed how individuals living with SCI identified the recovery of function that “would dramatically improve (their) life,” and highlighted the distinction between the scientific community's emphasis on locomotor recovery in rodent studies and the emphasis on hand function, sexual function, and bowel/bladder control in humans with SCI.
Given the rise of stem cell technologies into the forefront of potential neurorestorative treatments for SCI, we conducted a series of group and one-on-one interviews with individuals with SCI to garner their opinions on stem cell treatments and the potential to participate in clinical trials. 5 This qualitative initiative revealed a number of perspectives that could inform the progression of stem cell therapies into clinical trials, and, in particular, highlighted a potential gap between the timing of enrolment in subacute stem cell trials and an individual's readiness to enter such trials.
To expand upon the insights about participating in stem cell clinical trials that were revealed from these group and one-on-one interviews, we subsequently conducted a large-scale questionnaire survey to address specific questions about the receptivity to clinical trials and the risks that individuals would deem acceptable if they were to participate in such studies. This quantitative initiative complements our previous qualitative efforts to insert the voice of individuals with SCI into the dialogue on translating stem cell therapies into clinical trials. Specifically, we addressed the following issues: 1. What expectations do individuals with SCI have for functional recovery if they were to participate in clinical trials of stem cell therapies? 2. How low do the risks of complications related to stem cell therapies need to be in order for individuals with SCI to participate in clinical trials of stem cell therapies?
Methods
A survey consisting of 46 questions was distributed to individuals with SCI who were identified through a provincial SCI registry of >1000 patients. Inclusion criteria were: 1. SCI caused by an acute, traumatic event (e.g., motor vehicle accident, fall). 2. Injury resulting in immediate paralysis graded as American Spinal Injury Association Impairment Scale (AIS) A, B, C, or D upon admission to Vancouver General Hospital. 3. Injury within the cervical or thoracolumbar spine, C0-L1. 4. Resident of British Columbia
Exclusion criteria were: 1. SCI caused by non-traumatic pathology (e.g., tumor, infection, vascular anomaly). 2. Injury in the lumbar spine (L2-Sacrum) 3. Non-English speaking (the questionnaire was only available in English)
The survey included 19 questions related to individuals' receptivity to clinical trials. Six questions were asked to characterize the respondents' willingness to participate in clinical trials in three different scenarios: 1. Studying an experimental drug in the acute setting, hours after injury (e.g., an experimental acute neuroprotection trial) 2. Studying a subacute stem cell transplantation 7–14 days post-injury, which was the time frame used in the now-terminated Geron trial of human embryonic stem cell based oligodendrocyte precursors
6,7
and the Proneuron trial of autologous activated macrophages
8
3. Studying a chronic stem cell transplantation
Some questions addressed what individuals would expect in terms of the chance of benefitting functionally from the experimental (and as yet unproven) treatments. For example, the respondents were asked “If you would participate in such a trial, what would you want your chances to be for getting some functional recovery back?” Additional questions were asked about what the individuals' priorities for functional recovery would be in an experimental stem cell trial if they chose to participate in such a trial in their current state. We provided 13 choices for “functional improvement” and asked respondents to rank up to four of the most important to them that they “would want to achieve from the therapy.” These functions included: “improved hand function, improved leg function, improved balance, improved trunk control, independent breathing ability, decreased pain, improved sensation, decreased spasticity, fewer pressure sores, less autonomic instability, sexual function, bowel control, and bladder control.”
Further questions were asked regarding the acceptable limits of risk for various adverse events potentially related to stem cell transplantation, such as neuropathic pain, neurological injury, cancer, and meningitis. The survey specified that this stem cell transplantation would require an additional surgical procedure in which the cells would be directly implanted into the injured spinal cord. For each of these specific complications, respondents were asked “To undergo the stem cell transplant, I would need the risk of this adverse event to be less than: 0.1%, 1%, 3%, 5%, 10%, ‘Other’ (please specify),” or “I would participate regardless of the risk of this adverse event.”
The survey questions as they were presented to the individuals with SCI are included in the supplemental questionnaire (see supplemental questionnaire at
Statistical analysis
To analyze these data, risk-tolerance indices were derived from responses in both subacute and chronic timeframes. Linear regression models including all potential explanatory demographic variables such as age, gender, level of injury, severity of neurological impairment, chronicity of injury, level of highest formal education, and perceived knowledge of SCI research were fit to the two indices. Backwards elimination (BE) model selection was then performed; dropping the least significant variable on each iteration, to determine any significant modeling of high risk tolerance (type III p-value>0.05). Two sets of logistic regression models were generated then selected by BE to further delineate any association between demographic variables and highest (i.e., participating regardless of risk) risk tolerance compared with all other tolerances, and highest compared with minimal risk tolerance, for each possible adverse event. Odds ratios were generated to determine which demographic variables would predict higher risk tolerance. All final logistic regression models passed the Hosmer–Lemeshow goodness of fit test (∝= 0.05).
Results
Demographic characteristics of respondents
In total, 214 individuals with SCI responded to the survey (response rate of 29%). The average age of the respondents was 42 years, with a mean time of 5.5 years between injury and survey completion; 74% were male, and 62% had had injuries of the cervical spinal cord. At the time of admission 48% were AIS A, 15% were AIS B, and 37% were AIS C/D, as determined from the registry. Respondents self-reported to be 33% AIS A, 12% AIS B, and 55% AIS C/D at the time of the survey.
Information about the educational background, self-reported level of knowledge about SCI research, and sources of information about SCI research are illustrated in Figure 1. A wide spectrum of educational backgrounds was observed among the respondents, with a little more than half having had some form of postsecondary education. The Internet was, not surprisingly, the most commonly accessed source of information regarding SCI research. Interestingly, “healthcare providers” were only fifth on the list, behind the Internet, word of mouth, television, and SCI associations. On a scale of 1–10 to describe how informed they were about SCI research and emerging treatments, the majority (62%) listed themselves to be in the lower half of the spectrum of being informed (from 1 to 5); 13% described themselves as being well informed (scores of 8, 9, or 10), whereas 41% described themselves as being poorly informed (scores of 1, 2, or 3).
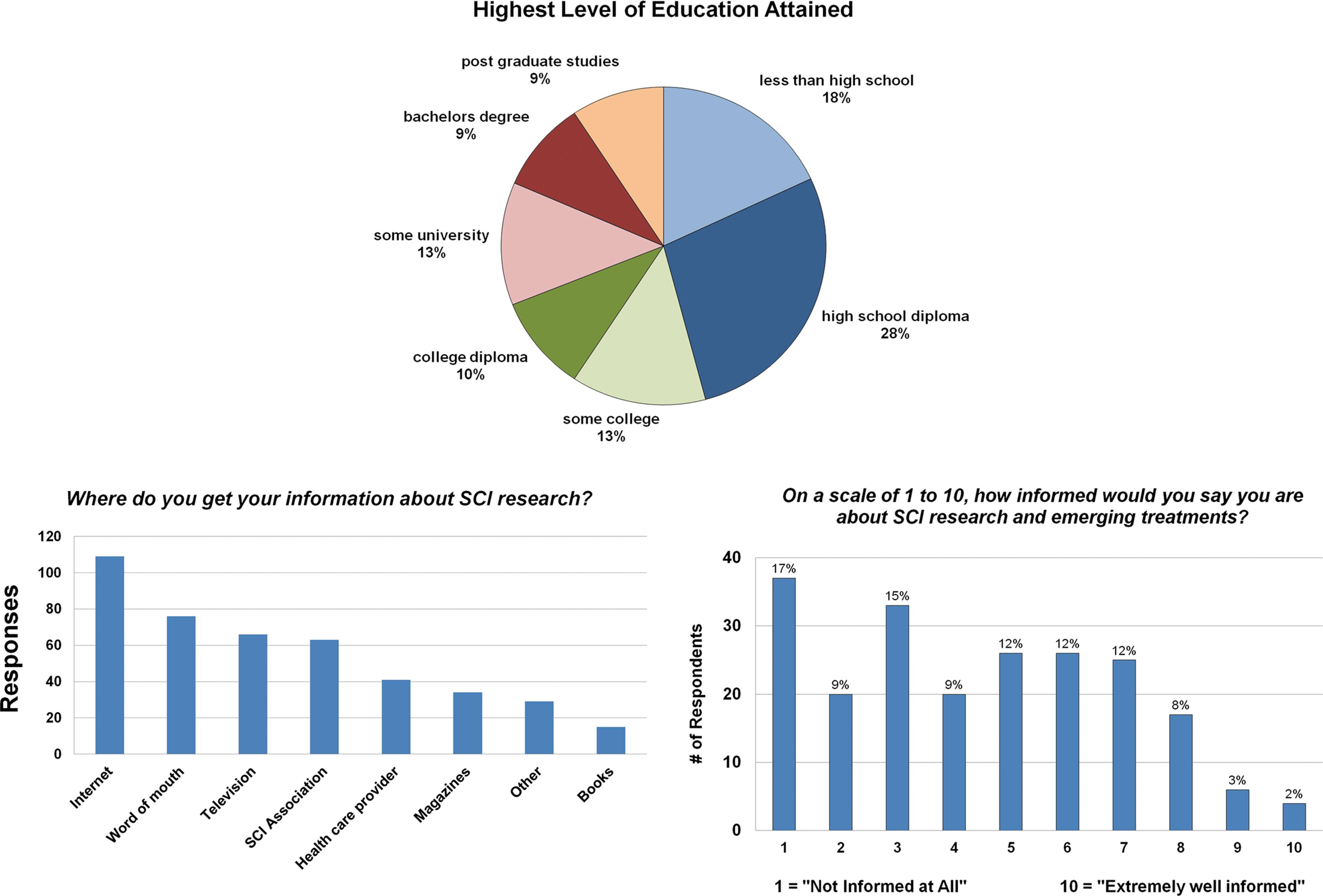
Educational level and knowledge of spinal cord injury (SCI) research. More than half of the respondents had had some form of postsecondary education. The most common source of information about SCI research was the Internet. Individuals generally reported their level of knowledge about SCI research and emerging research to be quite low. Color image is available online at
Receptivity to clinical trials and expectations of benefit
Respondents were asked to consider whether they would participate in an experimental clinical trial in three different scenarios: acute, subacute, and chronic/present day. For the acute scenario, 86% indicated that they “definitely” or “probably” would have participated in a clinical trial of a drug therapy offered within hours of injury, 57% indicated that they would have participated in a subacute stem cell transplantation trial within 1–2 weeks of injury, and 62% responded that they would participate in a stem cell transplantation clinical trial in their current state (Fig. 2); 17% of the respondents for the subacute and chronic stem cell trial indicated that they “didn't know” if they would participate, but only 7% expressed this uncertainty for the acute drug trial.
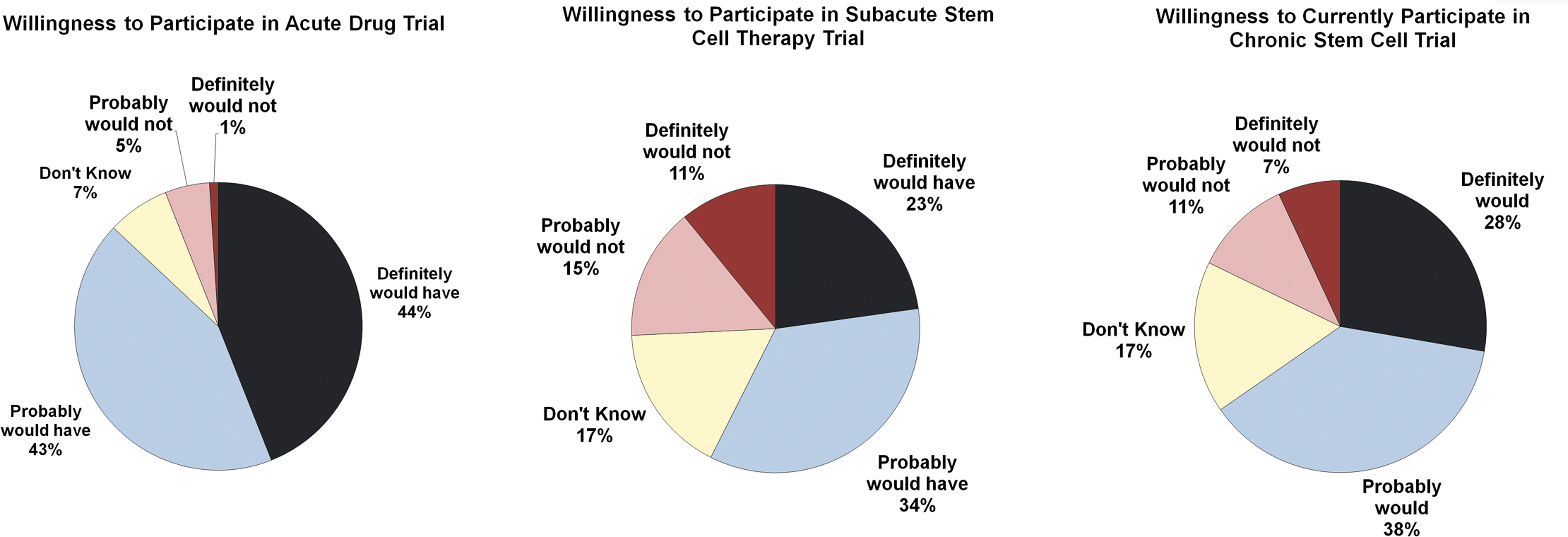
Willingness to participate in clinical trials. Respondents were asked to indicate whether they would or would not participate in an “acute drug trial,” or a stem cell therapy administered either during the subacute time frame or during the current chronic time frame. There was very high receptivity to acute drug trials, and somewhat less receptivity for stem cells in the subacute and chronic/current time frame. Slightly more of the respondents (66%) expressed willingness to participate in a stem cell trial in their current chronic state of injury than in the subacute time frame post-injury (57%). Color image is available online at
Individuals who responded that they “definitely would not” or “probably would not” participate in a stem cell clinical trial (26% for the subacute scenario 1–2 weeks post-injury, 18% for the current scenario) were asked to identify the reason(s) for this reluctance (Fig. 3). The two most commonly cited reasons for not entering a stem cell transplantation trial in the subacute and the chronic setting was the risk of developing cancer and the need for a second surgery for the cell transplantation procedure (>70% of respondents who “would not” participate in a stem cell trial). Concern about losing current neurological function and/or losing the potential to recover neurological function were cited as reasons for not participating by 42–45% of those who would decline participation in a stem cell trial. For these individuals, only 13% in the subacute setting indicated that skepticism of the therapeutic potential of stem cells was a reason for not participating. However, 42% in the chronic setting indicated that skepticism of the therapeutic potential of stem cells was a reason for not participating. Whereas this might suggest the development of skepticism about stem cell therapies over time among “non-participating” individuals, it is worth noting in Figure 2 that the percentage of respondents who indicated that they “definitely” or “probably” would participate in a stem cell trial increased from 57% in the subacute scenario to 65% in the current setting.

Reasons for “definitely” or “probably” not participating in a stem cell trial. Those who indicated that they would not participate in a stem cell clinical trial were asked to indicate the reasons. The most commonly stated reason was aversion to the risk of getting cancer. Skepticism about the efficacy of stem cells was cited more often as a reason for not participating in the current chronic state than in the subacute time frame. Color image is available online at
Two additional aspects of the survey highlight the optimism that individuals with SCI have toward stem cell therapies. The first is that if given the choice of enrolling in either a noninvasive drug trial or a stem cell transplantation trial, more responded that they would choose a stem cell trial (32%) than a drug trial (28%); with 29% not having any preference between the two. Only 10% would not participate in either a drug or stem cell trial. When asked “what would you want your chances to be for getting some functional recovery back?” if they were to participate in a stem cell transplantation trial at the current time, approximately a third of the individuals listed between 5 and 25%, and a quarter listed between 25 and 50% (Fig. 4).
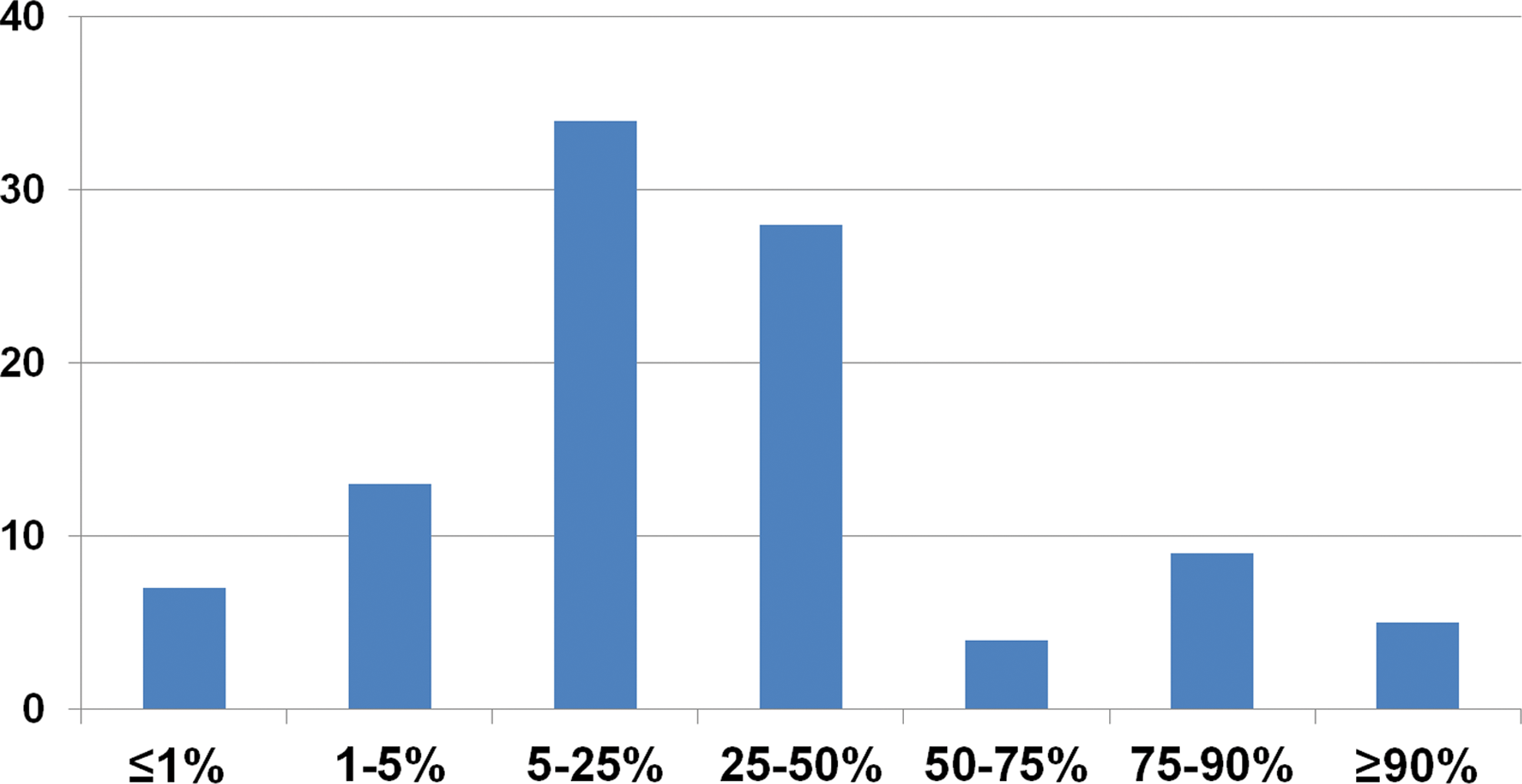
The minimal chance of functional recovery required for entering a stem cell clinical trial. Respondents were asked “what would you want your chances to be for getting some functional recovery back?” if they were to participate in a stem cell tranplantation trial in their current chronic state of injury. Approximately half of the respondents indicated that they would want their chances to be at least between 5 and 50%. Color image is available online at
Lower expectation for the percent chance of recovery was correlated with greater severity of neurological impairment (AIS) in patients with cervical SCI (Spearman rank correlation coefficient 0.16183 [p=0.0269]). This correlation between injury severity and expectations for recovery was not observed with thoracic SCI. A lower expectation for the percent chance of recovery was also correlated with a higher self-perceived knowledge of SCI research (Spearman rank correlation −0.14153 [p=0.0502]). No significant correlation was found between expectation for percent chance of recovery and age or level of formal education. In short, those who were AIS A quadriplegics (i.e., complete motor and sensory loss with no sacral sparing) and those who felt that they were extremely well informed about SCI research had the lowest expectations for functional recovery.
In terms of priorities for functional recovery if they were to participate in a stem cell clinical trial at this time, respondents indicated up to four priorities and ranked them from 1 through 4. Many did not include a third or fourth priority; therefore, we combined the total number of times that a specific functional recovery was listed as either the first or second priority. The responses were stratified according to cervical or thoracic SCI, and motor complete versus motor incomplete SCI. The results are shown in Figure 5. For cervical SCI, hand function was the top priority for both complete and incomplete quadriplegics, followed by bowel or bladder control, leg function, trunk control, and decreased pain. For thoracic SCI, bowel or bladder control was the top priority followed by leg function, trunk control, sexual function, and decreased pain.

Priorities for functional recovery in a stem cell clinical trial. Respondents were asked to rank the top four functional improvements they would wish to achieve as participants in a stem cell clinical trial. The bar graphs indicate the percentage of total responses in which the given functional improvement was listed as either the first or the second priority. For example, for motor complete cervical SCI, 31% of all the first or second priorities for functional recovery were for “improved hand function.” Color image is available online at
Risk tolerance in stem cell transplantation clinical trials
What degree of risk would individuals accept in a stem cell trial?
Respondents were asked to indicate the level of risk they would tolerate in a stem cell transplantation trial during the subacute (1–2 weeks post-injury) and in the chronic/current time frame. Specific complications included cerebrospinal fluid (CSF) leak, meningitis, neuropathic pain, neoplasm, and neurological injury (which in a subacute intervention could either cause worse function or limit their subsequent recovery). For the most part, the majority of individuals required these risks to be <1–<5% in order to participate in the trials. However, with the exception of the risk of neuropathic pain in the chronic time frame, 15–30% of individuals indicated that they would participate regardless of the risk of all complications (Figures 6 and 7).

Risk tolerance for a stem cell trial conducted during the subacute time frame. Respondents were presented with the scenario of a stem cell clinical trial offered to them within the first week post-injury, and were asked “how low would these risks need to be in order for you to have participated” in such a trial. Color image is available online at
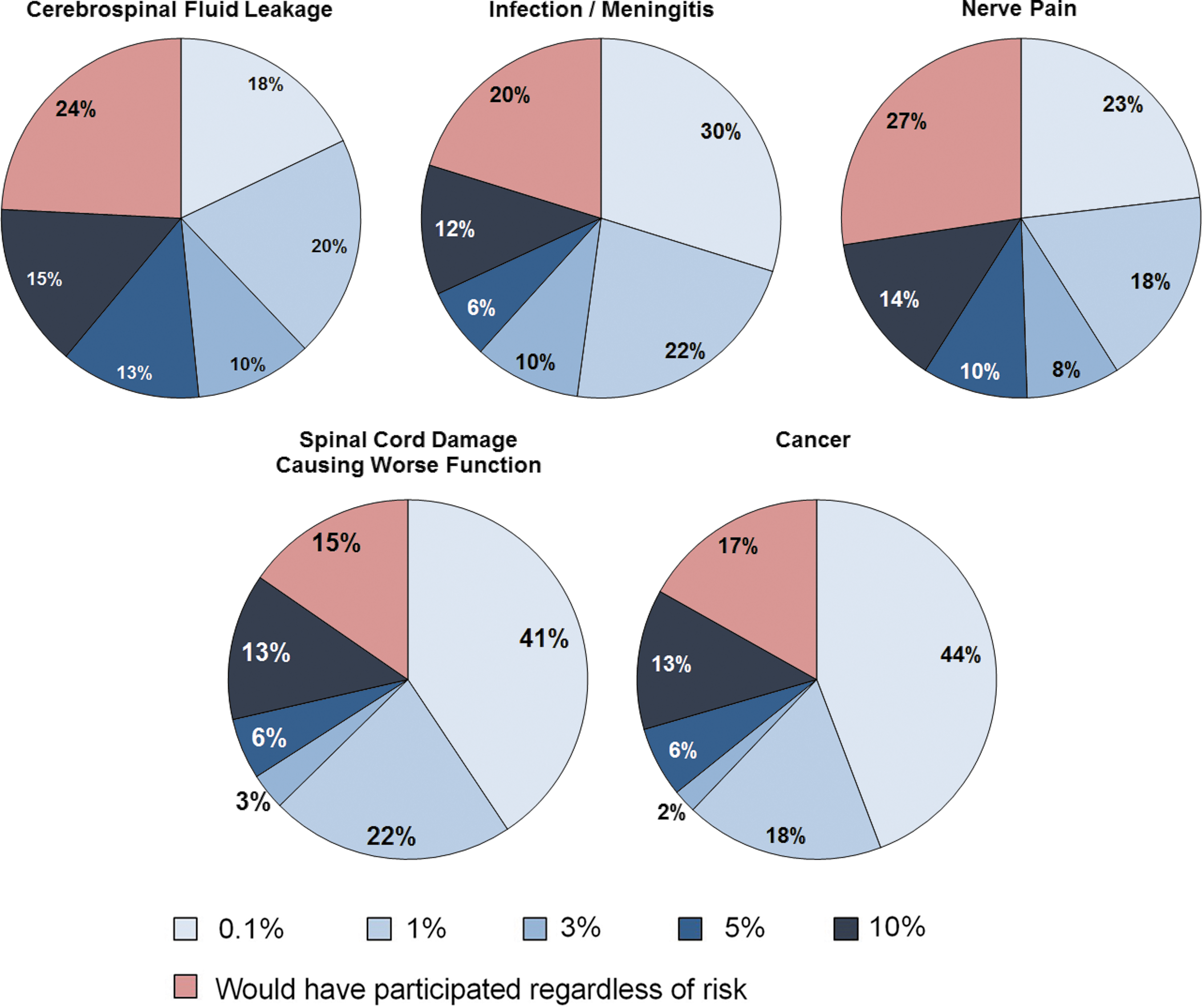
Risk tolerance for a stem cell trial conducted during the chronic time frame. Respondents were presented with the scenario of a stem cell clinical trial offered to them in their current, chronic state of injury, and were asked “how low would these risks need to be in order for you to have participated” in such a trial. Color image is available online at
What factors predict the individuals who would accept “any risk”?
The self-reported risk tolerances described previously for clinical trials for stem cell therapies revealed quite a spectrum of perspectives. We specifically analyzed those individuals who responded that they would participate “regardless of risk” to determine what factors might predict this high risk tolerance. Linear regression models were generated by BE to assess each complication and determine if high risk tolerance (i.e., participating regardless of risk) could be modeled by any demographic variable.
For the stem cell transplantation in the subacute scenario, high risk tolerance was related to gender, age, and extent to which individuals felt informed about SCI research and therapies (eliminated variables: type III p-value>0.05). A greater acceptance of high risk was found in males than in females; in older individuals (>60 years of age) than in younger individuals (17–30 years); and in those who described their level of knowledge about SCI therapies to be high (7–10 on the scale where 10 is “extremely well informed”). The variables of injury severity, injury level (cervical vs. thoracic), or injury chronicity did not predict high risk acceptance in this regression modeling. Furthermore, in the analysis of responses for stem cell transplantation in the chronic (current) scenario, the regression modeling revealed that no demographic variable predicted this high risk tolerance. Specifically, the variables of gender, age, and level of SCI knowledge did not predict greater acceptance of high risk, as they did in the subacute stem cell transplantation scenario.
What factors distinguish the individuals who would accept “any risk” from those who would accept very low risk (<1%), or from the rest of the respondents?
Here, we conducted two comparisons: 1. Individuals with very high risk tolerance (accepting “any risk” for the potential complications) against all of the other respondents, and 2. Individuals with high risk tolerance against those at the other end of the spectrum with low risk tolerance (accepting <1%).
Logistic regression models were generated and subsequently selected by BE. All final logistic regression models passed the Hosmer–Lemeshow goodness of fit test (∝= 0.05). Odds ratios were generated to determine which demographic variables would predict higher risk tolerance.
The results of this analysis for the subacute stem cell clinical trial are similar to those of the previous linear regression analysis; as in our previous linear regression analysis, demographic variables did not predict high risk tolerance in the chronic/current stem cell trial setting. The demographic variables that predicted higher risk tolerance in the subacute stem cell setting for many of the complications were male gender, age>60 years, and high self-reported level of understanding of SCI research. The significant demographic variables and odds ratios are illustrated in Table 1. The comparisons between the highest risk tolerance individuals and all others revealed essentially the same predictive variables as the comparisons between the highest risk tolerance individuals and the lowest risk tolerance individuals. Again, injury severity did not predict tolerance to risk. The lack of relationship between injury severity and risk tolerance is evident when examining the proportion of injury severities (“motor/sensory complete,” “motor complete/sensory incomplete,” and “motor/sensory incomplete”) within the group who would accept “any risk” as compared with the group who would accept “<1% risk”; in these, the proportion of the three injury severities is almost identical.
What expectations of functional recovery do those who would accept “any risk” have in a stem cell trial?
Spearman's rank correlations between expected chance for recovery and derived risk tolerances in the subacute and chronic time frames revealed statistically significant negative correlations of −0.19854 (p<0.0069) and −0.26971 (p<0.0002), respectively. In other words, individuals who had the highest risk tolerance (i.e., would participate regardless of risk) also had the lowest expectations for functional recovery.
Discussion
Accompanying the increased understanding of the biological obstacles that impede recovery after SCI is a rapidly growing list of potential neuroprotective and neuroregenerative strategies that show promising results in the laboratory setting. 9 –11 This progress has not gone unnoticed by the many individuals living with SCI who anxiously wait for the research community to deliver on the promise of novel therapies to improve neurological function. The visibility of these possibilities has exerted significant pressure on the SCI research community to aggressively translate such therapies, and has contributed to the growing number of clinical trials that are being launched.
This process of translating novel treatments from bench to bedside has occurred largely in the absence of the perspectives of the very people they are intended to benefit. We and others have previously argued for the inclusion of all stakeholders – including people with SCI – in the trajectory of translational research, in order for the science to be applied for the maximum health good. 5,12 Building on our previous research that engaged individuals living with SCI in one-on-one and group interviews, 5 here we conducted a survey of 214 individuals living with SCI to examine their receptivity toward clinical trials of acute neuroprotective drugs and stem cell therapies, and discern their tolerance for risk in stem cell clinical trials. It is recognized that many of the cellular substrates that have been investigated as potential therapies for SCI are in fact not “stem cell” therapies. In this regard, we acknowledge that we used the term “stem cell” broadly as a generalization for cellular transplantation therapies. We contend, however, that most individuals with SCI view cellular transplantation therapies as “stem cell treatments” and we felt that it was not imperative for the purposes of our study to distinguish the “stem cell” from “non-stem cell” strategies.
With respect to the willingness to participate in clinical trials, we asked respondents to put themselves into one of three scenarios: 1. The acute setting immediately after injury, at which time a neuroprotective drug trial was offered 2. The subacute setting a few days after injury, at which time a stem cell trial was offered 3. The present, with a stem cell trial being offered
The fact that>85% of respondents felt that they would have participated in a drug trial in the acute injury setting was not all that surprising. It was interesting that whereas 56% of the respondents “definitely” or “probably” would have participated in a stem cell trial in the subacute time frame, the receptivity to such a trial was higher in the chronic/current setting, with 66% indicating that they “definitely” or “probably” would participate if such a trial were now offered to them. In our qualitative study, 5 persons with SCI indicated that whereas their desperation might have encouraged them to enroll in a stem cell trial during the subacute time period, at the time of their interview many months post-injury, they felt that they would be much more reluctant to jump in to such an experimental treatment. Based on that data, we expected in our current survey that individuals looking back at the initial days post-injury would be much more willing to participate in a subacute stem cell clinical trial than they would be in their current chronic state of injury. However, the results of this current quantitative study indicate that receptivity to stem cell clinical trials remains high in individuals with SCI, even in their current state of chronic paralysis. Methodological differences in how responses were obtained in the qualitative interview process from our previous work, 5 compared with the questionnaire format of this current survey, could explain this discrepancy. In the interview process, the discussion is more open and free flowing and participants can express many positive and negative perspectives about stem cell trials that can then be picked up in the recorded transcriptions. In contrast, the questionnaire demands relatively precise answers and, as a result, nuances about how individuals feel about stem cell trials might not be captured. Nonetheless, the context of “looking back” at the time when they were recently injured and making a decision to participate in a stem cell trial was similar between our past qualitative interview/focus group study 5 and this current quantitative survey initiative.
As for reasons for not wanting to participate in a stem cell treatment in either the current, chronic state of injury, or during the past subacute scenario, the risk of developing cancer was a major factor, as was the aversion to having another surgery. In general, the reasons for not participating in stem cell trials were very similar between the subacute and chronic scenarios. Where they differed was in the perception of “don't think stem cells would work to improve my function.” This skepticism about the efficacy of stem cells was cited three times more often as a reason for not participating in the current, chronic state of injury than in the subacute setting. This suggests that the respondents recognized that they would have had much higher hopes for the efficacy of stem cells during the early subacute stages of injury, but now view this technology with more pessimism. Alternatively, they may see their current chronic state of paralysis as a much more difficult condition in which to achieve therapeutic efficacy, reflecting the fact that they have become more educated about their life with SCI after the initial psychological shock, and have become more realistic about their potential for recovery. It should be noted that this analysis included only those who answered that they would not participate in a clinical trial of stem cell therapies, and that these “non-participants” were actually fewer in the chronic stem cell trial setting. The apparent optimism that persons with SCI have toward stem cell therapies is generally reflected in the fact that slightly more responded that they would prefer an invasive stem cell therapy over a drug treatment if given a chance to enroll in a clinical trial of either. The moderate preference for the stem cell intervention over the drug trial is striking, given that the former would require an invasive surgical intervention and the latter is noninvasive.
With respect to risk tolerance in the subacute scenario, age, gender, and the extent to which individuals felt informed about SCI research and therapeutics were the only variables that correlated with high risk tolerance. It was surprising to us that such variables as injury severity, injury level (cervical vs. thoracic), or injury chronicity did not predict high risk acceptance. We had anticipated that those with the complete paralysis, for example, would predominantly populate the group that would “accept any risk.” This, however, was not the case. Additionally, we had anticipated that the younger individuals would be the greater risk takers, but were then surprised that in fact the older individuals were more likely to have the high risk tolerance than the younger individuals. The chronicity of injury (i.e., how long ago the injury occurred) also did not prove to be a significant predictor of high risk tolerance. The observation that no variable correlated with risk tolerance in the “chronic” scenario suggests that there is an evolution over time in the way individuals view potential complications and their tolerance to them.
Whereas early stem cell trials for SCI are ostensibly focused on safety and feasibility, it is hard to deny that individuals who enroll in such experimental trials do not cling to some hope that they might accrue some functional benefit from the technology. The negative correlation between risk tolerance and expected chance for recovery is likely an indicator of desperation in both subacute and chronic settings. In other words, the individuals who indicated that they would accept any risk of, for example, neurological deterioration, tended to have relatively low expectations for functional recovery. Expectations for the minimal percent chance of accruing functional benefit in a clinical trial of an experimental stem cell therapy ranged from<1% to >90%, with a third indicating a minimum threshold between 5 and 25% and a quarter indicating between 25 and 50%. The fact that the majority of individuals indicated that they would want at least a 5–50% chance of getting some functional recovery back raises an intriguing question to the research community: does the research community believe that the “promising results” observed in cell transplantation animal studies would translate into a 5–50% chance of functionally improving an individual with SCI? There is obviously no definitive answer to that question, and it would be fascinating to obtain the scientists' perspectives on this topic (which regrettably we did not seek in our initial survey of the research community). Interestingly, complete quadriplegics and those who reported themselves to be the most informed about SCI research and emerging therapies had the lowest expectations regarding functional recovery. These are important considerations in the management of expectations for individuals who are approached for stem cell clinical trials, as the potential for therapeutic misconception is high, even in phase 1 clinical trials. 13
As for the specific functional benefits that individuals with SCI would most want to gain through a stem cell trial, we were somewhat surprised at our results. The question we asked respondents to address was “If you were to participate in (a stem cell clinical trial), please rank in the order of importance to you up to 4 functional improvements you would want to achieve from the therapy. Out of the following 13 choices for “functional improvement,” please indicate the 4 most important ones to you, by writing a 1, 2, 3, or 4 beside the improvement.” This question is similar although not identical to that asked by Anderson in her survey, in which the respondents were asked “what gain of function would dramatically improve your life?” and then were provided seven functional recoveries to rank. 14 In our survey, we provided similar functional recoveries, but divided up “upper body/trunk strength and balance” into “improved balance” and “improved trunk control,” and “bladder/bowel function, elimination of dysreflexia” into “bowel control,” “bladder control,” and “less autonomic instability” (although for the purposes of our analysis, we combined bowel and bladder control). Instead of “walking movement” our survey offered “improved leg function.” As was done in Anderson's analysis of “shared priorities” between quadriplegic and paraplegic patients, we combined first and second priorities as well, to compare between motor complete and incomplete paralysis after cervical or thoracic SCI.
The most striking difference between our results and those of Anderson relate to the recovery of sexual function and leg function. The fact that sexual function “would dramatically improve” life for individuals with SCI was revealed in Anderson's work as the second highest priority for quadriplegics (behind arm/hand function) and the first priority for paraplegics. In our survey, the return of sexual function was ranked quite low: seventh for quadriplegics, fourth for paraplegics. Also, the return of ‘walking movement’ was a relatively low priority in Anderson's survey (fifth for quadriplegics, and fourth for paraplegics). In our survey, this was referred to as “improved leg function,” which we recognize is not exactly the same as “walking movement.” Nonetheless, if one assumes that “improved leg function” would in turn result in “improved walking movement,” then it is interesting that improved leg function in our survey was the third priority for quadriplegics and the second priority for paraplegics. We propose that the differences noted between our survey and Anderson's work are largely attributable to the subtle difference in how the question was phrased. An individual could conceivably answer the question of “the recovery of what function would dramatically improve your life?” differently from “what function would you most want to get back in an experimental clinical trial of stem cells?” It is also acknowledged that our study included a limited cohort of 214 individuals with SCI all living within the province of British Columbia. Cultural differences between our Canadian study sample and the American individuals who were surveyed by Anderson might also contribute to some of the differences that we observed in the responses.
In slight contrast to the Anderson data, our survey illustrates the importance that SCI individuals place on novel experimental therapies promoting increased motor function in the form of improved hand function (for quadriplegics) or leg function (for both quadriplegic and paraplegic individuals). Nevertheless, there are important similarities between our survey and that conducted by Anderson. First, the importance of bowel/bladder control was evident in both surveys, and this again highlights the importance of pre-clinical basic scientific studies that address this aspect of the SCI condition. Second, as mentioned, regaining hand function is of paramount importance to individuals with cervical SCI. This observation strengthens the need for conducting pre-clinical studies in cervical models of SCI and specifically targeting forelimb recovery. The importance of such experimental studies is reflected in our recently developed objective grading system for evaluating pre-clinical SCI literature, in which studies of cervical SCI are given more weight in the overall score than studies of thoracic SCI. 15 Finally, whereas recovering leg function was the second and third most important priority in our survey for individuals with cervical and thoracic SCI, respectively, this was still not the number one priority for either. Despite this, the recovery of locomotor function remains the most common outcome measure in pre-clinical studies. As was initially pointed out by Anderson, the pre-clinical science in SCI could certainly be better oriented and aligned with the priorities of the population it seeks to help.
Predicting and assessing risk tolerance could play an important role in the informed consent process as it pertains to cell transplantation technologies, and insights into how individuals with SCI view such risks may be useful for researchers who are designing such invasive interventional trials. Given that numerous individuals with SCI have traveled great distances and paid considerable sums of money for unproven cell transplantation therapies, 16 we anticipated that a certain proportion would participate in such clinical trials regardless of the risk of specific complications such as cancer and neurological injury. Indeed, the proportion of respondents willing to participate regardless of risk of such adverse events ranged from 15% to 30% in subacute and chronic stem cell transplant scenarios. Surprising, however, were the factors that did and did not predict who would be in this category of “extreme” risk tolerance for the subacute stem cell clinical trial. It would seem reasonable, for example, to predict that young individuals with complete AIS A injuries of the cervical spinal cord would accept the highest risk of complications. However, older individuals had the highest risk tolerance, and injury severity clearly did not predict high risk tolerance. In fact, the proportion of AIS A, B, and C individuals who would have participated regardless of the risk of a specific complication was no different than the proportion who would only participate if the risk were ≤1%. This speaks to the well-known fact that individuals with incomplete SCI frequently experience significant morbidity, disability, and decreased quality of life that leads to much desperation. Individuals with a high risk tolerance also had the lowest expectations for functional recovery, also reflecting this element of desperation that is well recognized. Interestingly, no variables were found to be significant predictors of high risk-tolerance in the analysis for a current, chronic stem cell transplant, indicating an evolution over time in the perspective that individuals have about potential complications and their tolerance to them.
Anderson's survey provided pivotal insights into the priorities of individuals with SCI with respect to the recovery of functions most important to their quality of life. 17 For a scientific community rather fixated on restoring walking ability, this survey forced those of us endeavoring to develop treatments for SCI to consider the greater importance that many patients place on such things as bowel/bladder continence and sexual function. Indeed, the voice of SCI patients in this regard had an important effect on the research community, and in many ways “validated” the importance of laboratory research initiatives to improve functional outcomes other than locomotion. Whereas the Anderson survey revealed how individuals with SCI prioritize functional recovery, we now propose to include their voice in the discussion of how experimental therapies for SCI get moved from the laboratory and into the clinic. Interestingly, the results of our survey contradict the natural assumption that young individuals with complete cervical level SCI would be willing to accept extreme risk in experimental therapies. Age>60 years, male gender, and high self-reported knowledge of SCI research predict high risk tolerance. Ultimately, we believe that guidelines for the movement of experimental treatments “from bench to bedside” should reflect not just the expertise of the researchers but also the values of the individuals with SCI whose lives are most affected by this injury. By informing the scientific community about the perspectives of individuals with SCI on experimental therapies developed for their injury, we believe a more effective road map for translation can be established.
Footnotes
Acknowledgments
The authors are grateful for the assistance of Lani Reichl, Allan Aludino, and Brenda Brisson in conducting this survey, and to Dr. Eric Sayre for statistical analyses. Dr. Kwon is the Canada Research Chair in Spinal Cord Injury and is a Scholar of the Michael Smith Foundation for Health Research. Dr. Dvorak holds the Paetzold Chair in Clinical SCI Research. Dr. Tetzlaff is the Rick Hansen Man in Motion Chair in SCI Research. Dr. Illes is the Canada Research Chair in Neuroethics. This work was supported in part by NCE/Research 9/5251 (CT8) (F. Miller; J. Illes, and B.K. Kwon, University of British Columbia joint principal investigators).
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.