
Abstract
The objective of the study was to examine how S100B, a biomarker of traumatic brain injury (TBI), contributes to outcome prediction after adjusting for known parameters, including age, Glasgow Coma Scale (GCS), pupil reaction, and computed tomography (CT) variables; to examine which parameters have the best correlation to elevated serum levels of S100B; and to investigate when to sample S100B to achieve the strongest association to outcome. This retrospective study included 265 patients with TBI admitted to the neurointensive care unit, Karolinska University Hospital Solna, Stockholm, Sweden. Univariate and multivariate proportional odds regressions were performed to determine parameters most closely related to outcome, and how S100B adds to prediction accuracy. Age (p<0.0001), pupil reaction (p<0.0001), and levels of S100B (p<0.0001) had the strongest statistical correlation to outcome. The area under curve of S100B, the first 48 h after trauma, yielded an additional explained variance of 6.6% in excess of known outcome parameters, including age, GCS, pupil reaction, and CT variables, themselves exhibiting an explained variance of 29.3%. S100B adds substantial information regarding patient outcome, in excess of that provided by known parameters. Only CT variables were found to be significant predictors of increased levels of S100B in uni- and multivariate analysis. Early samples of S100B, within 12 h after trauma, appear to have little prognostic value, and S100B should likely be sampled 12–36 h following trauma to best enhance TBI outcome prediction.
Introduction
T
An early and accurate prediction of outcome is important, not only to guide treatments, but also to assess novel treatment regimens in future randomized controlled trials using outcome versus predicted outcome as end-points.
Unfavorable outcome for patients with TBI has been shown to correlate with low Glasgow Coma Score (GCS), unresponsive pupil reaction, older age, hypotension, hypoxia, abnormal computed tomography (CT) findings and pathological laboratory parameters. 6 –19 Multicenter efforts, such as the IMPACT study groups, increase sample size, and robust prediction models can be constructed using multiple factors that are known to influence outcome. 20,21
Biomarkers, used to monitor progression of pathology and response to treatment, are widely used in many areas of medicine, and are now gradually entering the field of neurotraumatology. The use of biomarkers has been found to add important information in TBI and, specifically, the protein S100B has also been shown to increase in serum in patients with severe TBI. 22 –28 The half-life of the neurotrophic protein S100B is relatively short, with an in vivo duration of between 30 and 90 min. 29,30 Sustained levels will consequently reflect ongoing damage, and it is, therefore, used in some neurointensive care units (NICUs) as a monitoring tool. 31
There are known extracerebral sources of S100B. The protein has been found in adipose tissue, Langerhans cells, melanoma cells, chondrocytes, and cardiac muscle fibers, but has the highest concentration in astrocytes. 32
Serum levels of S100B have been shown to range between 0.3 and 1.6 μ/l in patients with favorable outcomes (Glasgow Outcome Score [GOS] 4–5) and between 1.1 and 4.9 μ/l in those with unfavorable outcomes (GOS 1–3). 23,27,33 –35 Both peak- and area under the curve (AUC) concentrations of S100B have been found to correlate to outcome after TBI. 22,36
The optimal time between trauma and sampling of S100B in serum has been widely discussed. The initial samples of serum concentration S100B have been considered the most important in predicting outcome, but time frames ranging between 6 and 84 h have been suggested to achieve the best specificity-sensitivity in outcome prediction. 23 –25,37 –42 Furthermore, the temporal profile of S100B has been shown to correlate to unfavorable outcome, where increasing levels of S100B are correlated to worse outcome, as compared with low or decreasing levels. 22 –27
Objectives
The primary aim of this study was to analyze how S100B contributes to outcome prediction compared with, and adjusted for, other known predictors of TBI outcome. A secondary aim was to examine which variables are best correlated to elevated serum levels of S100B. In addition, the optimal sampling time of S100B was investigated in relation to outcome prediction.
Methods
The present project was approved by the local ethics committee in Stockholm County (reference number 2009/1668-31/2).
This retrospective study includes patients (n=265) with TBI who were admitted to the NICU at the Karolinska University Hospital Solna, Stockholm, from January 1, 2005 to December 31, 2009.
Study criteria
Patients were included if they were ≥15 years of age, had traumatic intracranial lesions, and were admitted to the NICU after having been assessed by the neurosurgeon on call to be in need of neurocritical monitoring or intensive care support (see demographics, Table 1). A first serum sample of S100B obtained within the first 48 h after the reported trauma, and at least three samples obtained within 72 h after trauma, were required. Out of 388 admitted patients, 265 patients matched these criteria and were used for analysis. Among those excluded the mortality rate was 16%, including patients who died before three samples could be acquired (n=5). Other reasons for exclusion include not being admitted to the NICU within 48 h (n=50), too short duration at the NICU (not in need of intensive care) (n=30), or missing samples because of changes in sampling routine (n=38).
Hypoxia at SoA: Yes=assessed by the pre-hospital trauma team as insufficient airway or O2 saturation <90% at the site of accident; no=assessed by the pre-hospital trauma team as sufficient airway or O2 saturation >90% at the scene of accident; not known=insufficient pre-hospital trauma charts. Hypotension at SoA: Yes=systolic blood pressure <90 mm Hg at the SoA; no=systolic blood pressure >90 mmHg at the SoA; not known=insufficient pre-hospital trauma charts. Admission Glasgow Coma Score (GCS): best GCS obtained at the first examination by a neurosurgeon at the trauma center. Admission pupil reaction: pupil response during the first examination by a neurosurgeon at the trauma center. Extracranial injury: if the patient had multitrauma as defined by Advanced Trauma and Life Support (ATLS) (Acker et al., 2004). Midline shift: midline deviation caused by intracranial mass lesions as defined by neuroradiologist on the first computerized tomography (CT) scan performed (in mm). Presence of subarachnoid hemorrhage: the presence of subarachnoid hemorrhage on first CT scan performed. Progression of hematomas: progression of intracranial hemorrhages between the first and second CT scan. Hypodense lesion present: presence of hypodense lesion verified during the first 48 h on any CT scan. No surgery: no surgery performed. Monitoring surgery: placement of extraventricular drain, microdialysis catheter, and/or other intracranial monitoring devices without any evacuation of mass lesions during the first surgery. Evacuation surgery: evacuation of intracranial mass lesions during first surgery. Hemicraniectomy: hemicraniectomy performed during first surgery. Peak serum level: the highest level of serum S100B acquired during the first 48 h (μg/L). Area under curve (AUC): serum concentration of S100B the first 48 hours (μg/L/48 h).
Treatment
Basic clinical routine management and monitoring of TBI patients in the NICU was employed as described: those with severe TBI were intubated, mechanically ventilated, and sedated with morphine, midazolam, or propofol. Mass lesions were evacuated as deemed appropriate by neurosurgeons. Intracranial pressure (ICP) was measured predominantly with ventricular catheters or, in some cases, with intraparenchymal pressure monitors (Codman & Shurtleff inc. Raynham, MA or Rehau AG+CO, Rehau, Germany). Mean arterial pressure (MAP) was measured invasively, commonly in the radial artery. Cerebral perfusion pressure (CPP) was calculated as MAP-ICP, with both transducers placed at the midlateral ventricular level. Patients' heads were elevated at 30 degree angles. ICP was targeted at ≤20 mm Hg and CPP was targeted at 50–70 mm Hg. Targets were achieved with intravascular infusions (Ringer's acetate and albumin), vasopressors (norepinephrine), osmotic therapy (hypertonic NaCl and mannitol), intermittent cerebrospinal fluid (CSF) drainage from ventricular catheters, ventilation and temperature control, and decompressive craniotomy as needed. If traumatic subarachnoid hemorrhage (trSAH) was identified, nimodipine treatment and monitoring with transcranial Doppler ensued. When ICP could not be controlled with other measures, sodium thiopental was infused, limited by burst suppression and monitored with continuous electroencephalography. Cerebral microdialysis was used where appropriate. Partial pressure of carbon dioxide was targeted at 4.5 kPa. When mild hyperventilation was employed for ICP control, it was guided by venous jugular bulbar saturation and arterial-jugular lactate difference. Temperature was regulated at 37°C with paracetamol or external wrapping cooling systems. Mild hypothermia (35–36°C) was used for high refractory ICP. Blood glucose was targeted at 4–8 mmol/L, and hemoglobin was targeted at ≥90 g/L.
Definition of parameters
Pupil reaction was defined as either responsive, unilateral unresponsive, or bilateral unresponsive at admission to Karolinska University hospital. Multitrauma was assessed according to existing definitions by Advanced Trauma and Life Support (ATLS) system, and included thoracic and abdominal injuries and skeletal fractures (dichotomized as present or absent). 43 All CT scans were evaluated by a neuroradiologist analyzing midline shift (mm) on the first CT scan. trSAH, epidural hematoma (EDH), acute subdural hematoma (SDH), and cerebral contusions were noted as present or absent. Any detectable hypodense lesion visualized on a subsequent CT scan, compared with the initial CT scan, was noted. Progression of traumatic intracranial hematomas (contusions or subdural or epidural hematomas) between the first and second head CT scan, were noted, if present. Multiple types of intracranial pathologies were usually present in each patient. GCS (3–15) was assessed at admission to Karolinska University Hospital Solna. GOS was evaluated 6–12 months post-trauma either by a questionnaire regarding quality of life and/or a follow-up visit at the neurosurgical department. GOS 1 indicates death, GOS 2 a vegetative state, GOS 3 a severe, dependent state, GOS 4 a moderate, independent state and GOS 5 a full recovery. 44
S100B analysis
Serum samples of S100B were regularly obtained at admission to Karolinska University Hospital and approximately every 12 h (6:00 AM and 6:00 PM). The serum samples were mainly arterial, but a small number were venous, with both methods providing similar results. 45 All serum S100B samples up to those from September 2008 were analyzed at Karolinska University Hospital, Department of Clinical Chemistry, using a quantitative automated luminometric immunoassay (LIAISON-mat S100 system, Diasorin, Sangtec, Italy). In September 2008, the Department changed to an automatic electrochemiluminescence immunoassay (Elecsys S100B®; Roche Diagnostics, Penzberg, Germany) analyzing method, and a good unanimity between the two methods has been shown. 46 The serum levels of S100B and clinical data were acquired using the medical files from the hospital database system Take Care® (CompuGroup Medical Sweden AB, Farsta, Sweden) for each patient. The S100B peak levels and the AUC were calculated using ICU-Pilot® (Dipylon Medical, Solna, Sweden). All S100B levels were set to 0 μg/L at “time of trauma” in the AUC calculations. The highest level of S100B as well as AUC the first 48 h after trauma was used. S100B AUC the first 48 h was not calculated if only one sample was within the 48 h limit; 19 patients were excluded from AUC calculations because of this.
Statistical analysis
The statistical program R® (R Foundation for Statistical Computing, Vienna, Austria;
Additionally, linear regression was performed to determine what parameters were most closely correlated to levels of S100B.
The temporal relation between sample time and the strength of correlation between S100B and outcome was investigated using a sliding time window of 100 samples analyzed with a proportional odds model predicting GOS. If any patient contributed more than once in this window, S100B values were averaged, allowing no more than one value per patient in any window.
A p value<0.05 was considered statistically significant.
Missing data
The missing data in this study was imputed with MI using the Multivariate Imputations by Chained Equations (MICE) package in R, using seven imputations as suggested by the IMPACT investigators. 48 MI exchanges missing values sets of estimates drawn from a distribution, retaining the uncertainty of the imputed data in following analyses. The parameter “pupil reaction” was missing in four patients (1.5%). Because of incomplete pre-hospital trauma charts 62, (23.4%) patient journals lacked information regarding hypotension at the scene of accident (SoA), and 48 patients (18.1%) had missing information regarding hypoxia. AUC calculations could not be performed in 19 patients (7.2%), from whom only one sample of S100B was obtained within the first 48 h.
Results
Demographics
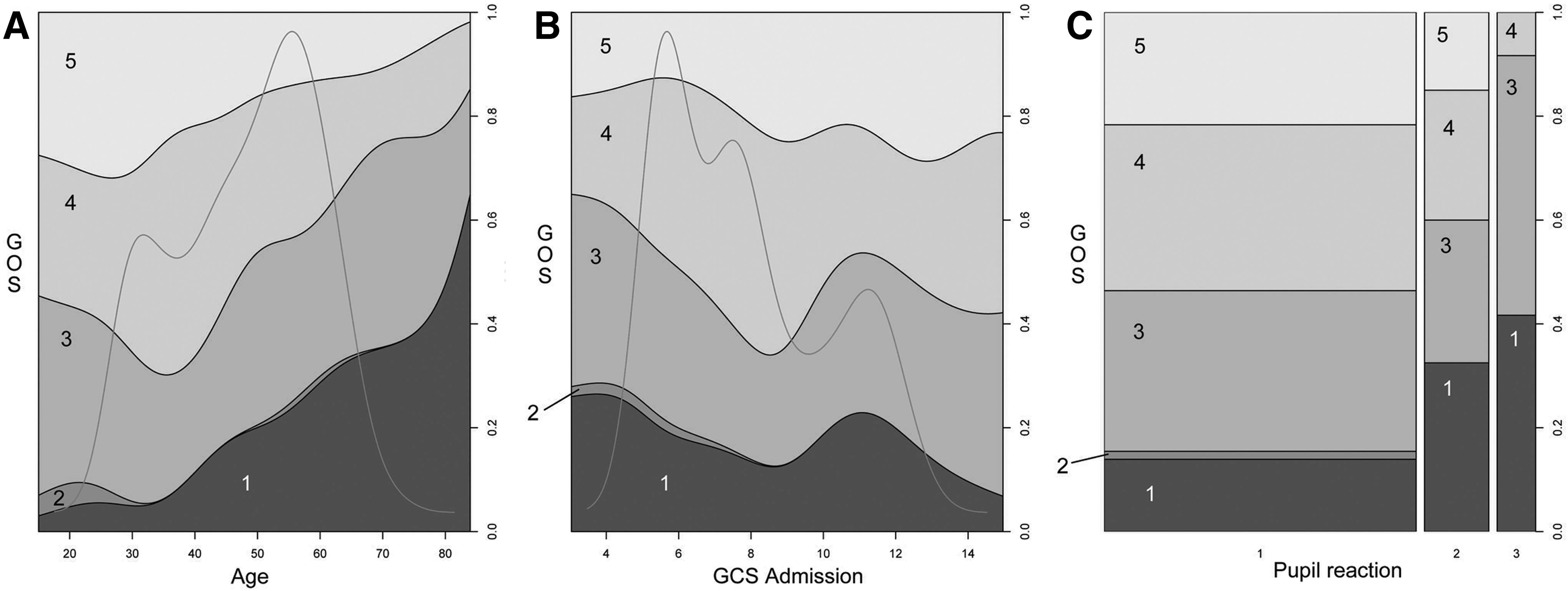
For the 265 patients meeting inclusion criteria between 2005 and 2009, the demographics are described in Table 1. Eighty percent were male and the median age was 50 years (Fig. 1A). The population had severe-to-mild TBI as distributed in Figure 1B, showing a predominance of severe TBI (69%) as seen in Table 1. Pupil reactions (Fig. 1C) were either unilateral or bilateral unresponsive in 41%. Extracranial trauma was present in 41% of all patients. Several different types of intracranial pathology were present in almost all patients. Evacuating surgery was performed in 49% and hemicraniectomy in 2%, whereas 35% underwent only monitoring surgery. Peak serum levels of S100B ranged between 0.1 and 22.00 μg/L (median 0.74 μg/L) while the AUC level ranged between 1.98 and 649.3 μg/L/48 h (median 20.65 μg/L/48 h). Outcome is shown in Table 2, indicating 20% mortality and a 48% favorable outcome.
Factors affecting outcome
Univariate analysis
S100B can be seen to have the highest pseudo R2 of any predictor in univariate analyses (Table 3), where the second (p<0.0001) and third samples (p<0.0001) of S100B have the highest pseudo R2 (0.151 and 0.165, respectively). Later sampling of S100B is, therefore, more highly correlated to outcome, and the first acquired sample of S100B (Fig. 2), albeit significant (p<0.05), exhibits an R2 of only 0.012. The log S100B peak levels (p<0.0001) and log S100B AUC (p<0.0001), both within the first 48 h, also corresponded significantly to outcome.
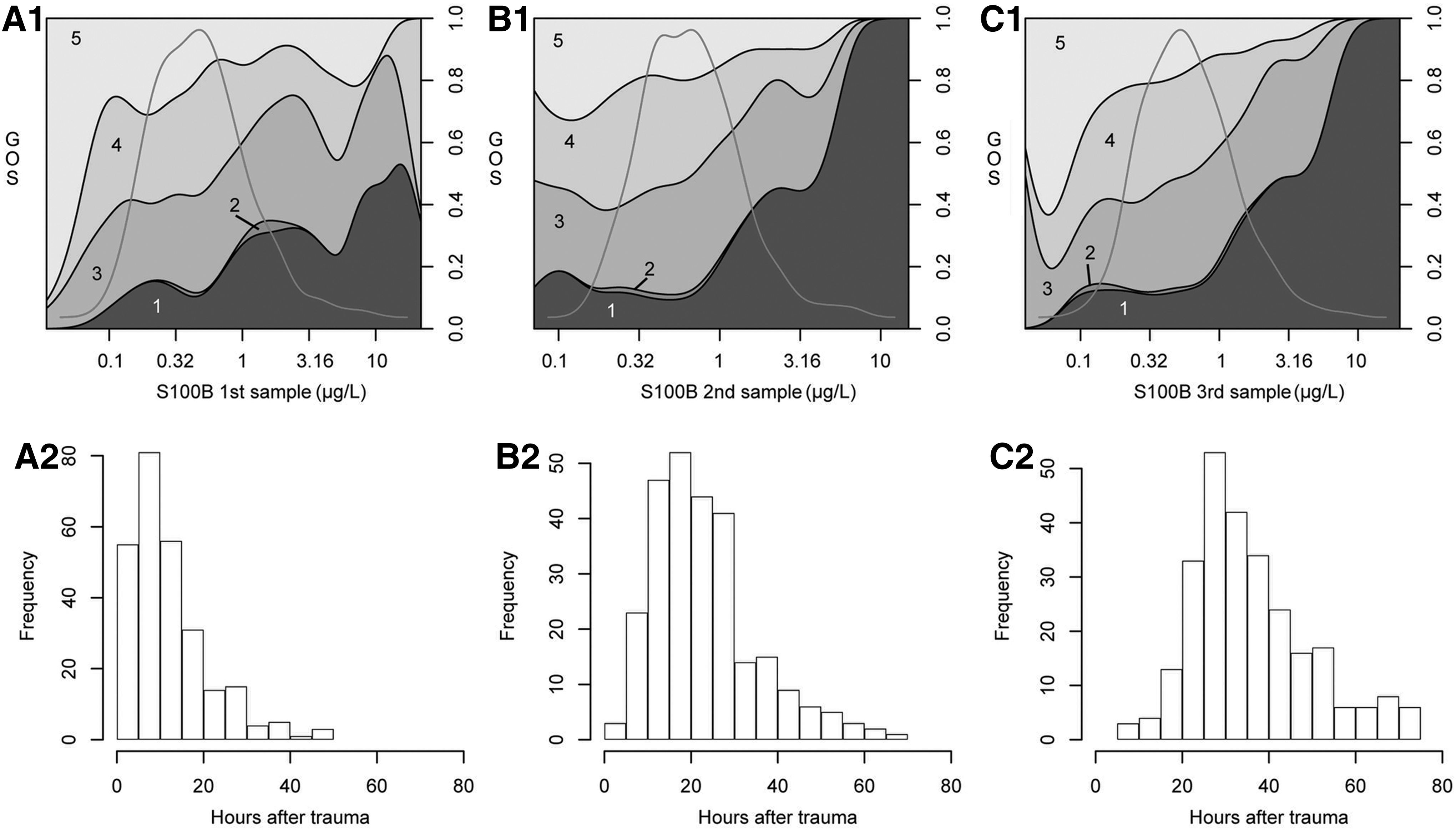
S100B (μg/L) versus outcome (Glasgow Outcome Score [GOS]) is shown using conditional density (CD) plots for the first three serum samples (
S100B levels are seen to exhibit the highest level of significance and pseudo R2 values. p value<0.05 was considered statistically significant.
GOS, Glasgow Outcome Scale; SoA, scene of accident; GCS, Glasgow Coma Score; trSAH, traumatic subarachnoid hemorrhage; EDH, epidural hematoma; SDH, subdural hematoma; AUC, area under the curve.
Age (p<0.0001), GCS at admission (p<0.01), and pupil reaction (p<0.0001) corresponded significantly to outcome prediction, with age having the highest pseudo R2 (0.102). GCS is noted to have an unexpectedly low pseudo R2 of 0.023. Other factors that correlate significantly (p<0.05) to outcome are midline shift on CT scans, the presence of epidural or subdural hematomas, the progression of intracranial hematomas, and the presence of intracranial hypodense lesions. Traumatic subarachnoid hemorrhage did, interestingly, not correlate significantly to outcome (p=0.055).
Multivariate analysis
Variable reduction of the parameters included in Table 1 was performed with Akaike information criterion, retaining age, pupil responsiveness, and log S100B AUC as significant, in proportional odds models predicting GOS. Unexpectedly, GCS was not retained in models.
A model including known important predictors such as age, GCS at admission, CT findings (presence of traumatic subarachnoid hemorrhage, subdural hematoma, cerebral contusion, epidural hematoma, midline shift), pupil responsiveness, hypoxia, and hypotension at the scene of the accident, provides an estimated explained variance of 29.3% in outcome prediction. If log S100B AUC is added to the model, it increases to 35.8%, exhibiting an added partial of 6.6%.
Factors related to elevated serum levels of S100B
Variable reduction of linear regression models predicting S100B levels (variables included in Table 1) retained solely CT variables in models (Table 4). In a multivariate analysis, progression of intracranial hematomas, hypodense lesions, trSAH, and midline shift were found to contribute significantly, with the best model exhibiting an R2 of 0.19.
Intracranial pathology visible on CT scan exhibits the highest level of statistical significance and pseudo R2 levels. p value<0.05 was considered statistically significant.
SoA, scene of accident; GCS, Glasgow Coma Score; trSAH, traumatic subarachnoid hemorrhage; EDH, epidural hematoma; SDH, subdural hematoma.
Time window for optimal sampling of S100B
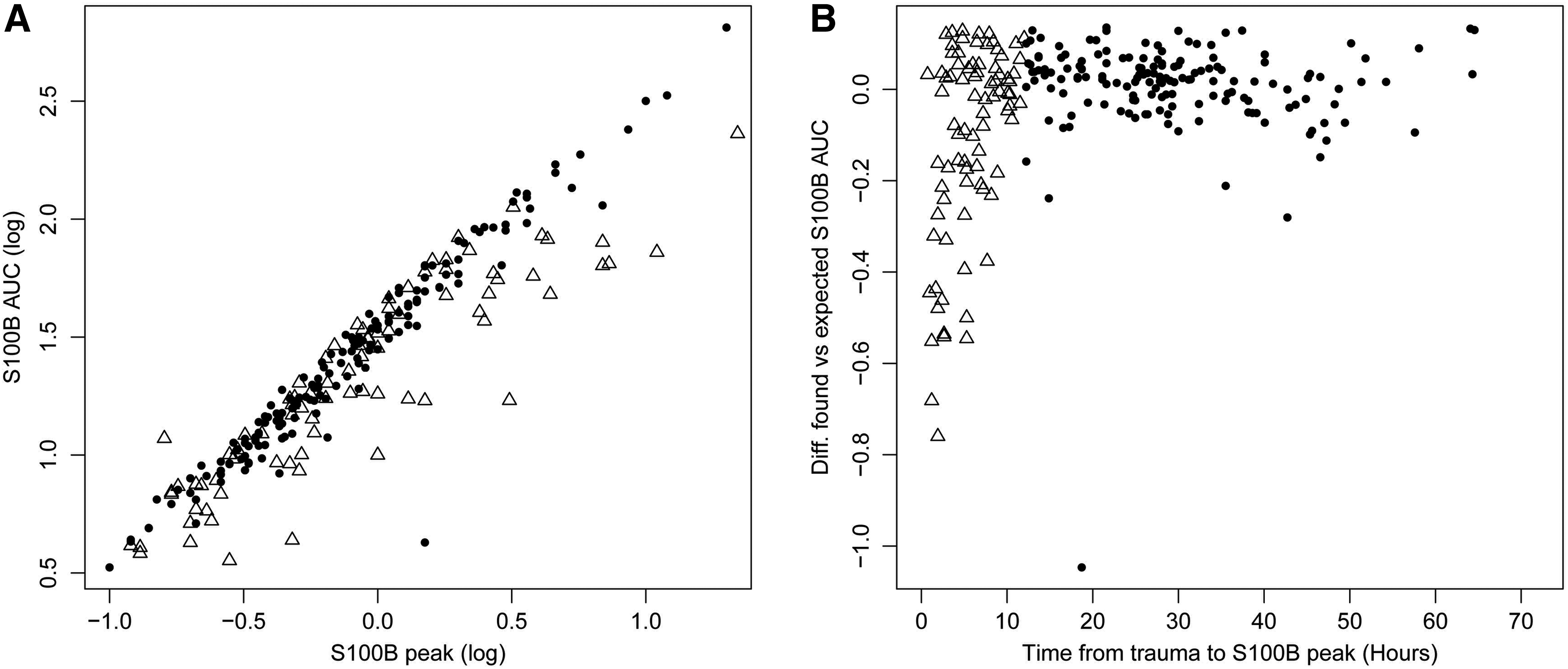
S100B peak and S100B AUC are highly correlated, R2 =0.86, and near co-linear (Fig. 3A). Samples of AUC that fall outside of this co-linearity (Fig. 3B), these being lower than expected, are found nearly exclusively up to 12 h after trauma. Early high peaks with levels that do not persist produce discrepancies of calculated AUCs that are lower than expected by the peak level. This might be caused by an extracranial origin of S100B, with early peaks and fast decay.
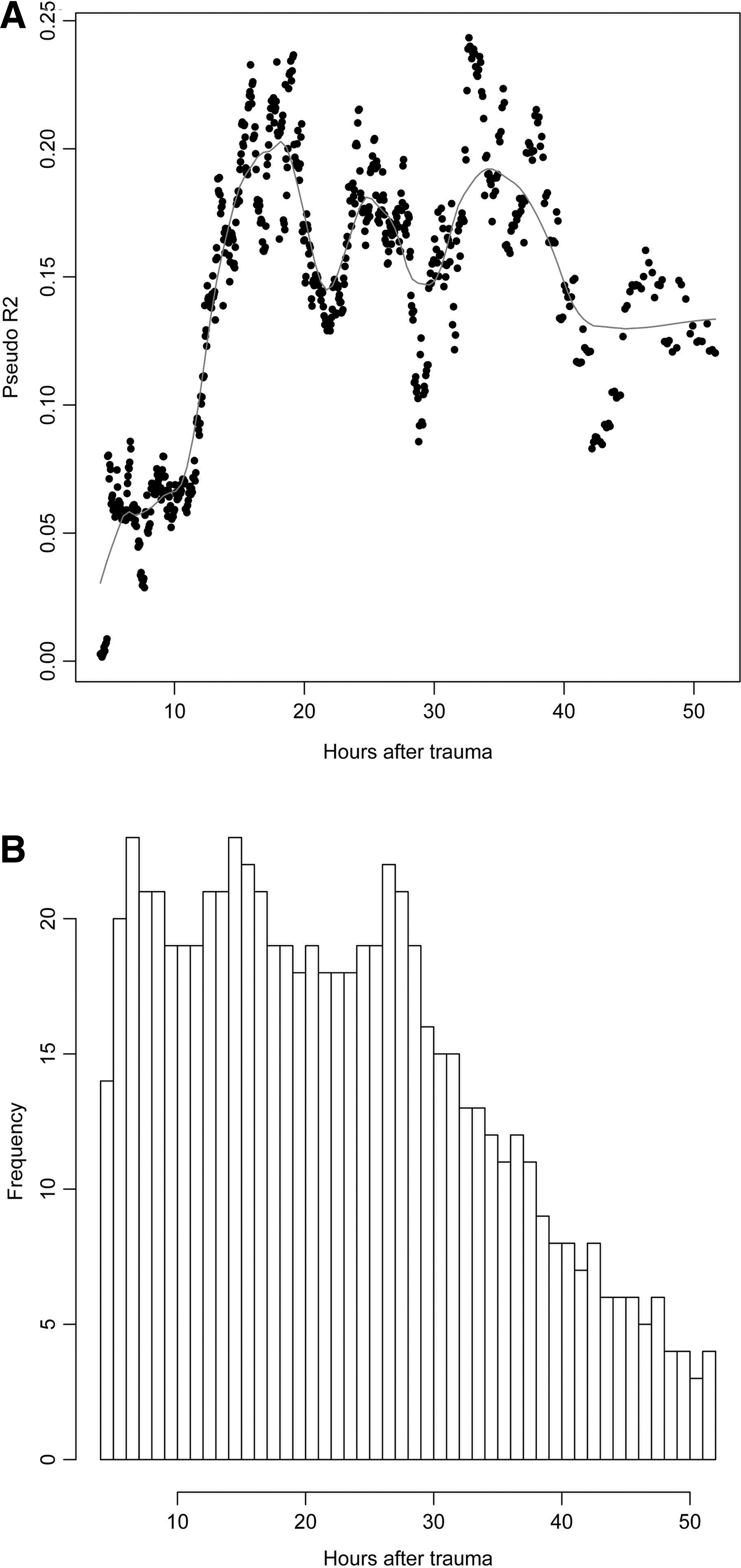
Early samples of S100B, <12 h after trauma, are shown to have lower predictive values toward outcome compared with levels sampled between 12 and 36 h after trauma (Fig. 4A). After 36 h, the predictive value of S100B cannot be evaluated in this study, because of limited data (Fig. 4B).
Discussion
In this study of 265 mild-to-severe TBI patients, we have shown a robust relation between S100B levels in serum and outcome. S100B was found to have a stronger relation to outcome in univariate analyses than known important TBI predictors including age, pupil response, GCS, and CT variables. In addition, the contribution of S100B remains, even after adjusting for these variables in multivariate analyses, adding 6.6% partial R2 to prediction models. Interestingly, this is similar to the partial R2 of pupil response and age in the IMPACT multivariate study. 21 Finally, we have shown that S100B should likely be sampled 12–36 h post-trauma, as early samples have little predictive value, and may reflect extra cranial sources of S100B. In aggregate, S100B appears to add important information both in the univariate and multivariate setting, and may benefit future TBI prediction models.
S100B has been shown to be related to outcome; however, a study explaining its contribution to outcome prediction in the multivariate setting has not been performed earlier. 13,25 The base model used in the present study included age, GCS at admission, CT findings (presence of traumatic subarachnoid hemorrhage, subdural hematoma, cerebral contusion, epidural hematoma, midline shift), pupil responsiveness, hypoxia, and hypotension at the scene of the accident. This choice was based on the TBI prediction models as proposed by the IMPACT group. 2 However, hemoglobin levels and Marshall CT classification were not available, and a direct comparison in the present study could not be made. Despite this, dominant CT variables were available and included in regression models. Although CT variables themselves were found to be the most important predictors of S100B, and, consequently, including them in models will weaken the contribution of S100B caused by covariate information, S100B was found to be a strong contributor toward outcome prediction. This indicates that S100B contains considerable information even in excess of the recorded CT visible changes, and suggests that the biomarker S100B should be further investigated as an outcome parameter in a multicenter setting.
Repeated studies have found GCS to be an important variable in outcome prediction of TBI, although exceptions to this have been observed. 13 Unexpectedly, our GCS was not a strong predictor of outcome. This may in part be because of the early timing of our GCS at admission before resuscitation, and to the fact that we have had access to only the full GCS, as opposed to the motor score, even in intubated patients. An admission GCS is, in part, subjective, and it will be affected by factors such as sedative medication, intoxication, multitrauma, speech impediment, or intubation. 49 A better GCS and the availability of motor score could lessen the predictive value of S100B in multivariate analyses, if they contain covariate information.
An increase of midline shift has been correlated to worse outcome following TBI as shown in (Table 3). 18,50 Midline shift did not show any statistical significance toward outcome in our multivariate analysis, although it was significant in the univariate analysis (p<0.05). Why midline shift was less correlated to outcome than might be expected cannot readily be explained, but it could be related to sample size. Another possible reason why an increasing midline shift is weakly correlated to outcome may be that epidural hematomas are present in 21% of all patients, which appears high compared with other studies. Epidural hematomas have been shown to generate midline shift and only a small contribution to S100B levels, and generally have better outcomes. 18,51
trSAH has been shown to be an important predictor of worse outcome. 52 It may lead to intracranial vasospasm in TBI with subsequent increased risk of ischemic injury. 53 Additionally, grading of trSAH may provide further prognostic information. 18 In the current study, trSAH was not graded but dichotomized, possibly missing significances. An additional potential reason why trSAH may not have been found highly related to outcome could be the use of nimodipine infusions. 54 However, a more recent multicenter review did not find any significant difference in morbidity or mortality between nimodipine infusion and placebo in TBI patients. 55
In this study, the presence of multitrauma did not show any correlation to outcome, even in the univariate analysis, or to increased levels of S100B. In contradiction, other studies indicate that there is an increased risk of unfavorable outcome in patients with a severe polytrauma. 56,57 Despite this, additional studies indicate that only critical extracranial injuries contribute to patient outcome. 58,59 Our definition of multitrauma uses a modified ATLS definition, in which patients with thoracic, abdominal, and skeletal injuries are defined as having sustained multitrauma. 43 This may result in comparably mild trauma, such as a costal fracture, being defined as multitrauma.
There are known extracerebral sources of protein S100B, and patients who sustain trauma, being diagnosed with multiple injuries without any identified damages to the central nervous system (CNS), have been shown to exhibit elevated S100B concentrations in serum. 60 –63 However, extracerebral release of S100B appears, to be limited to a shorter period of time compared with S100B released from the CNS, or not to affect the total serum concentration of S100B at all. 25,26,64,65 This could explain why multitrauma did not, as shown by other studies, translate to a statistically significant increase in serum S100B. 28,64 We do, however, identify high early levels of S100B which, in contrast to later values, do not contribute to outcome prediction, possibly suggesting an early noncerebral source.
CT variables indicative of structural pathology were the predictors most highly related to levels of S100B in this study. The parameters midline shift, trSAH, and development of hypodense lesions had the strongest correlation with increased S100B levels. Contusion volume has been shown to correlate to high levels of S100B; in compliance with this study, progression of intracranial hematomas yields significantly higher levels of S100B. 24,66
In aggregate, these findings support the brain-specific properties of the protein as representing structural damage, but also identify that the explained variance (R2 ) from CT parameters is merely 19%, leaving the dominant portion unexplained. More advanced monitoring of physiology such as brain tissue oxygen or microdialysis to detect and discriminate states, such as cerebral hypoperfusion and impaired metabolism, could possibly capture additional unexplained variance. A significant correlation between S100B and tissue hypoperfusion and increased serum lactate has been shown, also supporting S100B as a marker for ischemic injury. 63,67 Cerebral edema has, moreover, been shown to correspond to increased serum levels of S100B. 37 The additional unexplained variance could, in part, also be related to secondary insults, as, for example, increased intracranial pressure has been shown to correlate to increased levels of S100B. 31,40,68 In summary, additional work is needed to understand the unexplained variance of S100B.
The optimal time to sample S100B after trauma has been intensely discussed. In several studies, the initial samples of serum concentration S100B have been considered the most important in outcome prediction. 37 –40 Later time frames have also been suggested: within 6 h, 6–12 h, within 12 h, after 12 h, 24 h, within 42–79 h, within 48 h, 72 h, and, finally, up to >84 h after trauma. 22 –25,28,38,41,42,69 Our sliding-window analysis strongly suggests that the predictive value of S100B increases sharply after 12 h post-trauma, and remains so up to 36 h, being the limit that could be analyzed in this data set. Sampling of S100B, prior to 12 h after trauma, appears to be of limited predicative value, in our material of predominantly severe TBI patients. This finding might be difficult to translate to studies of mild TBI patients (GCS 14–15). 70
The limited value of early S100B may be explained by an extracranial origin. This study found high early peaks of S100B with fast decay to have a distinct pattern causing low AUC values. Values with this discrepency were found within 12 h of trauma. High early peaks have been observed earlier in a few patients. 39 We postulate that this pattern could be caused by extracranial sources of S100B, as soft tissue release of S100B has been shown to have a quick decay compared with cerebral lesions, probably because of a more prolonged release from intracranial processes. 26
Limitations
This study focuses on S100B the first 48 h after trauma, when we aim to concentrate on early biomarkers and their relevance in TBI outcome prediction. The influence of secondary insults or cerebral lesions after 48 h and their influence on later levels of S100B are not analyzed in this particular study, and will have to be subject of future research. 71,72 Some data were missing (see Missing Data section) and had to be imputed. This amount of information was relatively small; however, it provides a certain limitation to the study. An additional weakness is that our admission GCS was a poor predictor of TBI outcome, and using it may have contributed to an overestimate of the potential of S100B in prediction models, possibly more than if a post-resuscitation GCS had been used. GOS was assessed by a physician meeting the patient or by questionnaire. 73 These data were acquired between 6 and 12 months after trauma. Although improvement may continue up to 12 months, a prolonged duration may be preferable to use in prediction models, although the current consensus of 6 months will, perhaps, affect comparability to similar studies using the 6 month GOS. 74 The laboratory performing the samples switched procedures during the course of the study and analyzed S100B with two different methods. Studies have shown a good correlation between the two methods with an R value (Spearman correlation coefficient) as high as 0.932 between the two methods. 46,75 However, a study by Müller et al. did not support that the methods were interchangeable, because of a significant difference between the assays. They found that the mean difference between the LIAISON-mat S100 and the Elecsys S100B kit was 0.14 μg/L (+/- 2 SD, 0.39 μg/L). 76 In addition, the laboratory (Department of Clinical Chemistry, Karolinska University Hospital Solna) conducted a calibration between the two methods during a transition period of 6 months to minimize sampling error. In summary, we do not believe the change of assay kit to be a substantial limitation.
Conclusion
In this study, serum levels of S100B added substantial information regarding patient outcome, in excess of that provided by age, GCS, pupil reaction and CT variables. Elevated S100B levels are best correlated to CT-visible intracranial pathology, but much variance remains to be explained. Early samples of S100B, within 12 h after trauma, appear to have limited prognostic value, but the predictive value increases sharply after these 12 h, remaining at the higher level for at least 36 h.
Footnotes
Acknowledgments
We thank the staff at our NICU, especially Vivian Hambäck-Hellkvist and Birgitta Ohlgren; the Karolinska Univeristy Hospital, Department of Clinical Chemistry for analyzing the S100B samples; and Gunilla Malmborg-Bornhall for keeping track of the trauma database at the Karolinska NICU. The study was funded by grants from the regional agreement between Stockholm County Council and Karolinska Institutet (ALF).
Author Disclosure Statement
No competing financial interests exist.