
Abstract
Epidural hemorrhage (EDH) that develops remote from the decompressed hemisphere can be associated with devastating morbidity after hemicraniectomy for traumatic brain injury (TBI). In this study, we investigated the incidence, risk factors, and outcome influence of post-craniectomy remote EDH. For this retrospective study, we enrolled 139 patients undergoing unilateral hemicraniectomy for TBI. The patients were subdivided into two groups based on whether EDH remote from the site of bone decompression was present (n=11) or not (n=128). We identified the intergroup differences in clinical parameters and outcomes. Multivariate odds regression was used to adjust for independent risk factors of the development of EDH. The incidence of remote EDH following decompressive hemicraniectomy for TBI was 7.9%. There were two independent risk factors for remote EDH, including absence of contusional hemorrhage (odds ratio, 95% confidence interval=6.158, 1.090–34.802; p=0.040) and presence of remote skull fracture (odds ratio, 95% confidence interval=19.770, 2.194–178.152; p=0.008) in preoperative computed tomography scans. The mean Glasgow Outcome Scale did not differ between the patients with and without EDH. In conclusion, remote EDH in patients undergoing unilateral decompressive hemicraniectomy for TBI is not uncommon. The absence of contusional hemorrhage and presence of remote skull fracture are independent risk factors. Although postcraniectomy remote EDH is devastating, timely computed tomography scanning and immediate hematoma evacuation are efficient and crucial for patient outcomes.
Introduction
In this study, we retrospectively collected data and analyzed the clinical parameters and neuroimaging findings of patients undergoing unilateral decompressive hemicraniectomy for TBI. The goals of this study were to determine the frequency of remote EDH following decompression, to identify the possible risk factors for subsequent EDH, and, finally, to compare neurological outcomes between craniectomized patients with or without development of remote EDH.
Methods
After obtaining consent from the Institutional Review Board of Kaohsiung Chang Gung Memorial Hospital, we reviewed the records of 201 TBI patients requiring decompressive craniectomy from January 2006 through December 2008. Among them, 176 patients who underwent unilateral hemicraniectomy for isolated cerebral hemisphere lesions at initial surgery were identified. We excluded 37 patients who had incomplete medical records or lacked postoperative images of the brain. Therefore, a total of 139 patients were enrolled for analysis. The characteristics of the patients were documented, including demographic information, Injury Severity Score (ISS), Glasgow Coma Score (GCS), and pupil reactivity.
The patients received computed tomography (CT) of the brain soon after arrival at the emergency room. Follow-up CT scans were obtained in cases of neurological deterioration and absent neurological improvement, and in routine examination after operations. The individual features on CT scans before craniectomy were interpreted as follows: 1) the presence of subdural hemorrhage, subarachnoid hemorrhage, intraventricular hemorrhage, contusional hemorrhage (parenchyma lesion with mixed hypo- and hyperdensity regardless of number, size, or location), or skull fracture; 2) the status of basal cisterns subdivided into normal, compressed, or absent; and 3) the degree of midline shift measured as deviation of the septum pellucidum from the central position. Remote EDH or remote skull fracture was defined as an occurrence away from the site of hemicraniectomy, and the locations of the lesion included the contralateral frontotemporoparietal region, bilateral occipital region, or posterior fossa. In addition, the characteristics on CT scans before hemicraniectomy were scored according to the Rotterdam CT classification. 9
The indications in which craniectomy for TBI was performed were as follows. 10 Primary craniectomy was defined as surgical decompression in patients primarily for the evacuation of any type of intradural lesion. The aim of prophylactic craniectomy was to avoid expected post-surgical increases in intracranial pressure. Secondary craniectomy was defined as the procedure performed in patients in whom high intracranial pressure was refractory to medical treatment. Unilateral hemicraniectomy was performed for brain swelling limited to one cerebral hemisphere. The hemicraniectomy limits included 1) superior, 2 cm of the lateral edge of the superior sagittal sinus; 2) inferior, at level of the middle cranial fossa floor at the origin of the zygomatic arch; 3) anterior, frontal to the midpupillary line; and 4) posterior, 3 cm posterior to the external acoustic meatus. The dura mater was opened, and the opening was extended to the bone margins in a stellate or semicircular fashion. The brain surface was covered loosely by the remaining dura or artificial dural substitutes without a watertight closure. A postoperative intracranial pressure monitoring system was used in selected cases, based on the neurosurgeons' decision.
Neurological outcome was assessed at discharge and by the end of follow-up using the Glasgow Outcome Scale (GOS) as follows: 1=death; 2=persistent vegetative state with inability to interact with the environment; 3=severe disability with inability to live independently, but the ability to follow commands; 4=moderate disability with the ability to live independently but inability to return to work or school; and 5=mild or no disability with the ability to return to work or school.
Statistical analysis
Data were analyzed using SPSS version 12.0 (SPSS Inc., Chicago, IL). The categorical variables were analyzed using the χ2 test or Fisher's exact test. The continuous variables were assessed using the Student's t test or Mann–Whitney U test. Multivariate logistic regression was performed to adjust for independent risk factors of remote EDH in patients after unilateral decompressive hemicraniectomy. A p value of<0.05 was considered to be statistically significant.
Results
Patient characteristics
The 139 patients who underwent unilateral hemicraniectomy for TBI included 98 male and 41 female subjects. The mean age was 46.80±19.42 years (range, 1–88 years). The mechanisms of brain injury were as follows: 106 traffic accidents, 31 fall accidents, and 2 other causes. At admission, the mean ISS was 27.75±9.37 (range, 16–75). Neurological assessment before operation showed the mean GCS was 7.40±3.03. Pupillary examination identified 75 patients with both reacting pupils and 64 patients with one reacting or both non-reacting pupils. A total of 136 patients underwent primary craniectomy accompanied with evacuation of traumatic mass lesions, and 3 patients underwent secondary craniectomy for the control of refractory intracranial hypertension. A total of 114 patients were treated with emergency surgery within 24 h after head trauma, and 25 patients were treated with delayed surgery>24 h later.
CT features and classification
According to the CT scans obtained before hemicraniectomy, the individual features included 119 (85.6%) subdural hemorrhage, 116 (83.5%) subarachnoid hemorrhage, 11 (7.9%) intraventricular hemorrhage, 79 (56.8%) contusional hemorrhage, and 57 (41.0%) skull fractures that were remote to the site of hemicraniectomy. The status of the basal cistern was normal, compressed, and absent in 19 (13.7%), 83 (59.7%), and 37 (26.6%) patients, respectively. The mean midline shift was 9.09±5.61 mm (range, 0–25.24 mm). According to the Rotterdam CT classification, the number of patients with scores 2, 3, 4, 5, and 6 were 9 (6.5%), 15 (10.8%), 28 (20.1%), 54 (38.8%), and 33 (23.7%), respectively. The mean Rotterdam CT score was 4.63±1.15.
Post-craniectomy remote EDH
Remote EDH after unilateral hemicraniectomy occurred in 11 of the 139 patients, and the overall incidence was 7.9%. Three of the 11 patients had intraoperative brain swelling during decompression and immediate CT scans showed EDH. Six presented with GCS deterioration, pupil dilatation, or increased intracranial pressure postoperatively. The other two patients had no change in symptoms or signs, and EDH was discovered by routine CT scans. Most of the remote EDH was newly developed, except one that was expanded. The locations of the remote EDH included nine in contralateral regions and two in occipital regions as well as the posterior fossa. Remote skull fractures overlying or nearby EDH were identified in CT scans of 10 patients. The mean volume of hematoma was 99.82±52.26 mL (range, 20–168 mL). Because of the significant mass effect, all patients required a second surgery for EDH evacuation. There was no pre-existing bleeding disorder or abnormal coagulation profile in these patients. The characteristics of the 11 patients with postcraniectomy remote EDH are summarized in Table 1. Figures 1 and 2 show the representative CT scans of remote EDH after decompression.
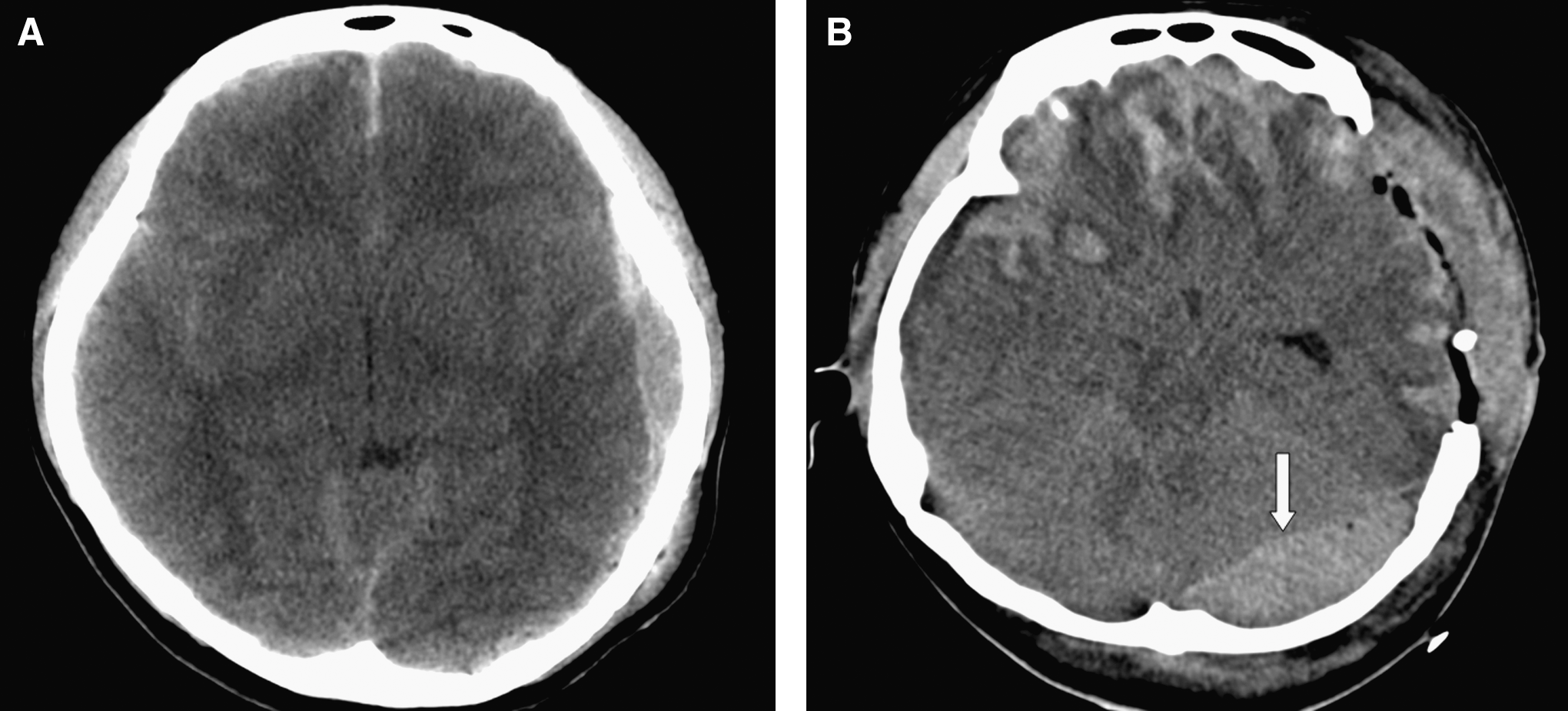
Case 7.
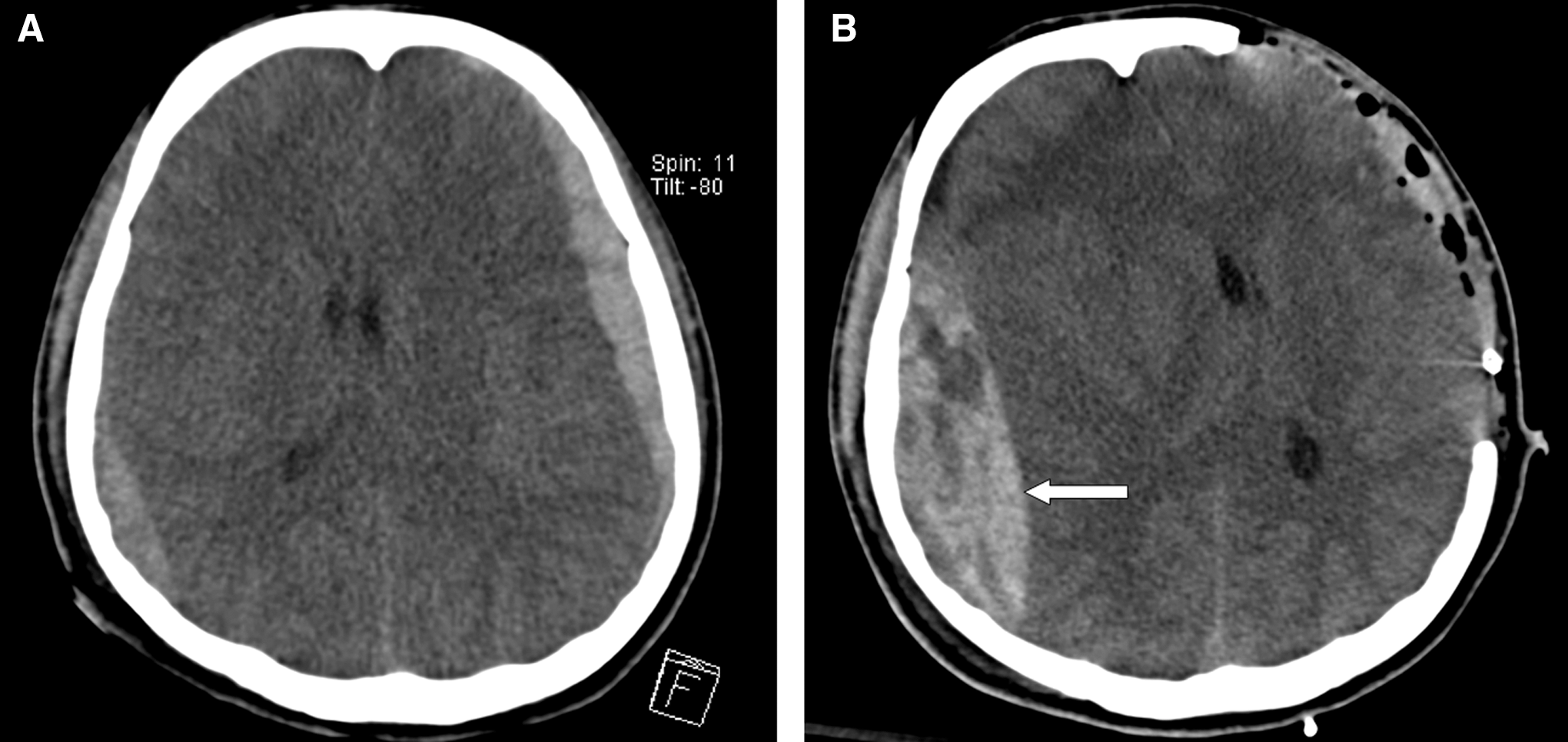
Case 9.
GCS, Glasgow Coma Score; GOS, Glasgow Outcome Scale; CT, computed tomography; EDH, epidural hemorrhage; RE, routine examination; BS, brain swelling; ND, neurological deterioration; PD, pupil dilatation; IICP, increased intracranial pressure; PF, posterior fossa; CL, contralateral region; OC, occipital region.
Risk factors for remote EDH
Table 2 shows the comparison of demographic and imaging data in patients with or without postcraniectomy remote EDH. Statistical analysis identified the significant intergroup differences in clinical parameters as follows: age (p=0.002), mean ISS (p=0.04), pre-craniectomy contusional hemorrhage (p=0.01), and remote skull fracture (p=0.001).
EDH, epidural hemorrhage; ISS, Injury Severity Score; GCS, Glasgow Coma Score; GOS, Glasgow Outcome Scale.
Table 3 presents the multivariate regression analysis that was used to investigate the value of potential risk factors and adjust for the confounding effect of other parameters. The occurrence of remote EDH in patients after unilateral hemicraniectomy was independently associated with contusional hemorrhage (odds ratio, 95% confidence interval=6.158, 1.090–34.802; p=0.040) and remote skull fracture (odds ratio, 95% confidence interval=19.770, 2.194–178.152; p=0.008) in preoperative CT scans. In other words, patients with absence of contusional hemorrhage and presence of remote skull fracture had ∼6 and 20 times higher risk, respectively, of remote EDH than those with opposite CT features. Age and mean ISS were not significantly relevant in this multivariate model.
EDH, epidural hemorrhage.
Remote EDH versus patient outcomes
The mean hospital stay was 45.18±34.57 and 34.79±34.02 days for patients with and without remote EDH, respectively (p=0.333). After discharge, all of the patients were followed up at the outpatient department for a period ranging from 1 to 68 months. There were no intergroup differences in the mean GOS at discharge or at the end of follow-up. Comparisons of the clinical outcomes of patients with or without remote EDH are demonstrated in Table 2.
Discussion
The rationale behind decompressive craniectomy is to convert an injury within a closed box, with a fixed volume and limited reserve, into an open system with increased capacity to accommodate occupied mass. 11 This procedure is very effective in ameliorating the raised intracranial pressure of TBI patients, but one of the potential complications following craniectomy is a delayed EDH contralateral to or remote from the decompressed hemisphere. There have been several studies describing related issues. 5 –8,12 Most of the authors considered delayed contralateral EDH a rare or uncommon phenomenon, but these studies lacked a complete cohort analysis or follow-up. In this series, the incidence of post-craniectomy remote EDH that needed to be evacuated was 7.9%, which is not uncommon.
After removal of the skull bone, the drop in intracranial pressure and loss of the tamponade effect on the vessels in areas already injured, such as under the skull fracture, may lead to delayed EDH. Elevated blood pressure or rapid correction of hypovolemic shock after trauma resuscitation also contributes to the production of new hematoma. As remote EDH formation is a dynamic process, neurosurgeons should be careful and aware of the timing of hematoma development. In this series, over half of patients with remote EDH were recognized by neurological worsening
The absence of contusional hemorrhage before craniectomy increases the risk of remote EDH, and this is reasonably explained by the competitive relationship between intra-axial hemorrhage and extra-axial hemorrhage. Hemorrhagic expansion of contusions is inherent in the injury process and has been demonstrated in serial CT scanning. 14,15 Flint et al. found a remarkably high incidence of new or expanded hemorrhagic contusions following decompressive surgery. 16 As a result, the presence of initial contusional hemorrhage, representing severe parenchymal injury, indicates a greater chance of subsequent intraparenchymal bleeding or swelling, and a lesser chance of delayed EDH. A skull fracture contralateral to the side of decompression is a characteristic that is commonly encountered. 7,8 This contralateral or remote fracture implies the possibility of a tear of the dural vessels, but without obvious extra-axial hematoma collection caused by the tamponade effect. Based on our results, skull fracture overlying or nearby the site of remote EDH was identified in almost all of preoperative CT scans. Similar findings have been reported in previous studies.
Patients with delayed EDH have been relatively young, according to some published reports. 5 –8 The present study also showed all patients with post-craniectomy remote EDH were<50 years. This may be explained by the fact of the increased adherence of the dura to the inner skull table in the elderly, and the decreased patent planes responsible for blood collection. In addition, the mean ISS was higher in patients with delayed EDH. Even though these details seem to be important, neither age nor ISS was relevant in the multivariate regression analysis. However, one of the limitations in this retrospective study is the presence of the small sample size in one group. Therefore, non-significance should not simply be interpreted as non-relation, as the variables may have a genuine influence but be undetectable in this study.
Posttraumatic EDH is a dangerous intracranial lesion that is accompanied with a significant mortality rate in patients after surgery for evacuation of hematoma. 17, 18 In contrast, our results show that delayed EDH following craniectomy does not influence the outcomes of brain-injured patients. One reason is that the severity of the underlying brain damage may most strongly determine the prognosis, rather than the delayed extraaxial hematomas. Su et al. also considered that patients with severe and diffuse parenchymal injury, as evidenced by the poor neurological status from the onset of trauma, did poorly. 8 Another reason is that the effect of surgical timing is related to the outcomes of patients in whom the EDH causes compression of brain structures. 19 Time from neurological deterioration, as defined by the onset of coma or pupillary abnormalities, to surgery, is more important than time between trauma and surgery. As patients undergoing craniectomy for TBI are intensively monitored after operation, early detection of and rapid surgery for delayed EDH is feasible. As a result, neurological recovery is not impaired as long as the mass effect has not progressed to the stage of permanent brainstem dysfunction. In our opinion, despite the potential lethality of post-craniectomy remote EDH, timely CT scanning followed by rapid hematoma evacuation is effective in restoring neurological function.
Conclusion
In conclusion, the incidence of remote EDH in patients undergoing unilateral decompressive hemicraniectomy for TBI was 7.9%. The absence of contusional hemorrhage and presence of remote skull fracture in preoperative CT scans are independent risk factors for delayed EDH. Although post-craniectomy remote EDH is devastating, understanding the timing of hematoma formation, arranging CT scans without delay, and evacuating the hematoma immediately are efficient and crucial for patient outcome.
Footnotes
Author Disclosure Statement
No competing financial interests exist.