
Abstract
Sports-related concussion (SRC) is typically associated with functional, as opposed to structural, injury. The results of traditional structural neuroimaging techniques used to assess SRC tend to be normal in many athletes, and are only clinically helpful in ruling out a more serious injury. Diffusion tensor imaging (DTI) has increasingly been touted as a method offering greater clinical potential in mild traumatic brain injury (mTBI). Despite this, the utility of DTI as a clinical tool for diagnosing and managing SRC has received considerably less attention than it has in the general TBI research literature. The aim of this article is to conduct a systematic review of DTI in SRC, and to provide a focus and overview of research findings using this MRI technique in SRC. A systematic review of articles published in the English language, up to February 2012, was retrieved via PsycINFO®, MEDLINE®, EMBASE, SPORTDiscus™, Scopus, Web of Science, and Informit; using the key search terms: diffusion tensor imaging, diffusion magnetic resonance imaging, diffusion weighted MRI, diffusion MRI, fractional anisotropy, tractography, apparent diffusion coefficient, magnetic resonance imaging, mild traumatic brain injury, mTBI, traumatic brain injury, concussion, sport, athletic and athlete. Observational, cohort, correlation, cross-sectional and longitudinal studies were all included in the current review. Results of the review found eight articles that met inclusion criteria, which included data on 214 athletes and 96 controls. Seven of eight studies reported some type of DTI abnormality, although the neuroanatomical sites involved varied. Although considerable methodological variations exist across studies, the current review suggests that DTI may possess adequate diagnostic sensitivity to detect SRC in affected athletes. Further longitudinal studies are required to demonstrate its discriminate validity and prognostic capacity within this field.
Introduction
It is a well-established notion that the majority of SRCs tend to fall at the mild end of the traumatic brain injury (TBI) continuum. 2 Although SRC can result in overt problems such as acute headache, dizziness, confusion, and nausea, in many instances the signs of concussion are more covert, manifesting as mild cognitive deficits 3 that may not be detected via traditional clinical assessment.
Structural neuroimaging is one method typically used to establish pathophysiological diagnosis of SRC, albeit that it focuses on only one of the multi-faceted presentations of the condition. 4,5 Ideally it informs acute clinical management post-injury, and may also be predictive of functional recovery at chronic stages. 6 However, because of the nature of SRC, which involves functional rather than structural injury, results of traditional structural neuroimaging techniques (i.e., CT, and MRI) are predominantly normal in many athletes. 7,8 These conventional structural imaging techniques may, therefore, have little utility in diagnosing or assessing SRC, beyond ruling out a more serious injury, such as intracranial hemorrhage or small cerebral contusions, 9 and do not adequately detect more subtle or even widespread microstructural traumatic axonal injury (TAI), such as those that may be observed in SRC. As a result, conventional CT and MRI have not reliably correlated with patient symptoms of SRC and are inconsistent in predicting functional outcome following mild TBI (mTBI). 10,11 Advances in neuroimaging technology and the improved capacity of neuroimaging techniques to examine tissue at a microstructural level is required, and is especially important in cases of chronic post-concussive symptoms. 12
Diffusion tensor imaging (DTI) is a less conventional and relatively new MRI modality that provides noninvasive, in vivo indices of tissue microstructure. Characterization of the microstructure of white matter connections is achieved by assessing the degree of water diffusion in the brain. 13 –15 DTI exploits the fact that myelin sheaths and cell membranes of white matter tracts hinder the movement of water molecules. 12,16 Although DTI has been used primarily as a research method for assessing structure and function following TBI of all severities, it has increasingly been touted as a method offering great clinical potential, as well as holding some promise as a means of predicting recovery (i.e., prognosis) in cases of mTBI. 12 A growing body of literature suggests that certain DTI parameters may serve as a biomarker for microstructural white matter changes in mTBI at both acute and chronic stages. 6,17 DTI may be a promising approach for characterizing microscopic damage to specific white matter pathways following mTBI. If DTI can reliably detect subtle, but clinically relevant, changes in brain microstructure in ways that exceed the capabilities of conventional imaging methods, it may be crucial in redefining the diagnosis, prognosis, and management of mTBI patients.
Application of DTI in TBI
Although DTI has been used primarily as a research method for assessing structure and function following TBI of all severities, it has increasingly been touted as a method offering great clinical potential, as well as holding some promise as a means of predicting recovery (i.e., prognosis) in cases of mTBI. 12
In the acute stage of a traumatic lesion, the axonal swelling is believed to increase fractional anisotropy (FA) and decrease apparent diffusion coefficient (ADC). In the chronic stage, this effect appears to reverse as the membrane degradation and cellular lysis allow more space for water to diffuse, increasing ADC and decreasing FA. 17
DTI analysis methods in TBI
Whole brain distributional analysis
In this approach, a histogram of the diffusion MR parameter (such as the mean diffusivity) is calculated for every voxel in the entire brain. In previous approaches, 18 a set of three Gaussians is fitted to the histogram, to represent three distinct compartments: 1) “tissue,” 2) non-tissue and CSF, and 3) partial volume voxels containing both tissue and non-tissue/CSF contributions to the signal. The “tissue” Gaussian is used to infer the diffusion properties of the brain, typically by characterizing the peak height, peak location, and the width of the Gaussian.
From a practical standpoint, the approach is simple to implement. as no user interaction is required, and the fact that the measurement is “global” means that there is no need to correct for multiple comparisons, as would be needed in voxel-based or forms of region of interest (ROI)-based analyses, and there is no need for a priori hypotheses relating to anatomical location of group differences. On the other hand, any information on the location of damage is lost and any changes are averaged across the whole brain. Therefore, one can miss subtle effects that may be detected by other analysis methods. For a more detailed discussion of the pros and cons of histogram analysis, the reader is referred to Cercignani. 19
Whole brain voxel-based analysis
Whole brain voxel-based DTI analysis also assesses the entire brain volume in the absence of a priori hypotheses pertaining to anatomical location but, in contrast to histogram analyses, tries to identify the specific locations of any group differences. There are two main approaches used in the neurotrauma literature: 1) those based on voxel-based morphometry approaches, 20 in which the data sets from individuals are first aligned, then smoothed before statistical inferences are drawn at each voxel of the smoothed image; and 2) those based on skeleton-projection-based approaches 21 in which, after alignment, a skeleton of the mean of the aligned images is derived and the data are projected onto this skeleton to correct for residual misalignment.
One of the limitations of this method is the difficulty associated with assigning significant cluster attributes to a single tract, 22 –24 in addition to issues with choice of smoothing kernel (in the first method), 20 heterogeneity of statistical power (in the second method), 25 and other biases that avoid the detection of pathology. 26
Despite this shortcoming, DTI in mTBI cases has indicated microstructural alteration in comparison with controls, 27,28 with reduced FA detected in the genu of corpus callosum, posterior limb of internal capsule, superior longitudinal fasciculus, superior fronto-occipital fasciculus, and centrum semiovale in the mTBI group. Further, FA values within the corpus callosum, posterior limb of the internal capsule, superior longitudinal fasciculus, corticospinal tract, superior fronto-occipital fasciculus, and inferior occipitofrontal fasciculus, are negatively correlated with severity of injury as determined by Glasgow Coma Scale (GCS) scores. 29 However, as noted previously, the association between DTI indices and injury severity or other measures of impairment relies upon whether imaging is performed during the acute or the more chronic phase of TBI recovery.
ROI analysis
With the ROI approach, the anatomical structures of interest to be compared across groups are predetermined. TBI samples typically show lower ADC and higher FA values during the acute stage of injury when compared with controls using ROI methods. 30 Analysis of ROIs has also demonstrated that FA values of the genu, stem, and splenium of the corpus callosum, and the columns of the fornix, were lower in patients with TBI than in healthy controls. 31 Attentional control has also been shown to positively correlate with FA in the anterior part of the left corona radiata, and FA in the uncinate fasciculus positively correlated with memory performance in TBI samples. 32 The advantage is that the method is transparent and readily interpretable, and by definition requires less correction for multiple comparison than a whole-brain voxel-by-voxel search. As several voxels are averaged with the ROI, this approach will confer greater sensitivity than voxel-by-voxel searches. The disadvantages are the laborious nature, and the inability to detect changes that were not previously hypothesized. Moreover, it is well known that there is subjectivity in hand-drawn ROI placement, 26 which can confound analyses, although using atlas-defined ROIs can ameliorate this problem. Maximum sensitivity will be had when the size of the ROI matches the size of the abnormality. If the ROI is too large, for example, subtle effects will be missed.
In vivo tractography
In vivo tractography provides “virtual dissections” or an architectural representation of the major white matter pathways. 33 Unfortunately, many of the TBI studies that have used tractography have limitations, including single case studies, 33 –35 assessing a limited number of tracts such as the corpus callosum 31,36 or including only moderate/severe TBI cases. 37
The tractography-based approach may be more sensitive in revealing FA differences than the voxel-based or small-ROI-based approach, as many more averages of the parameter of interest are used in deriving a mean value for the tract. This notion is supported by the findings of Keedwell and colleagues 38 who reported highly significant tract-specific results, whereas the tract-based spatial statistics revealed no significant results. Further, Kanaan and colleagues 39 reported differences using tract-based approaches that were not observed with ROI-based approaches. Moreover, for white matter pathways that take a tortuous route in and out of the plane of the screen, a tractography-based definition of an ROI will clearly be superior to a hand-drawn approach. The downsides are shared with those of ROI-based approaches, in that unexpected differences will not be revealed. As with the non-tractography ROI-based approaches, if the effects are highly localized (such as to a small portion of a tract), then averaging over the whole tract may obscure these differences.
Given that SRCs are typically in the mild range of TBIs, 2 and the abovementioned results are from DTI studies in more general mTBI samples, it follows that this imaging technique may be useful in the detection and management of the unique sequelae associated with SRC. What is particularly relevant in terms of SRC is whether there are more lasting or cumulative changes that are measurable using DTI following repeated head trauma. The current systematic review examines the growing literature on the use of DTI with SRC in children and adults.
Objectives
In the current review, studies that used DTI to investigate brain injuries in athletes were considered. The aim of this review was to systematically evaluate the currently available evidence on the utility of DTI in the diagnosis and prognosis of SRC, and to determine whether the promising findings within general mTBI groups translate to SRC in athlete samples. To examine this question, observational, cohort, correlation, cross-sectional, and longitudinal studies were all included in the current review.
Methods
The review was conducted in three stages:
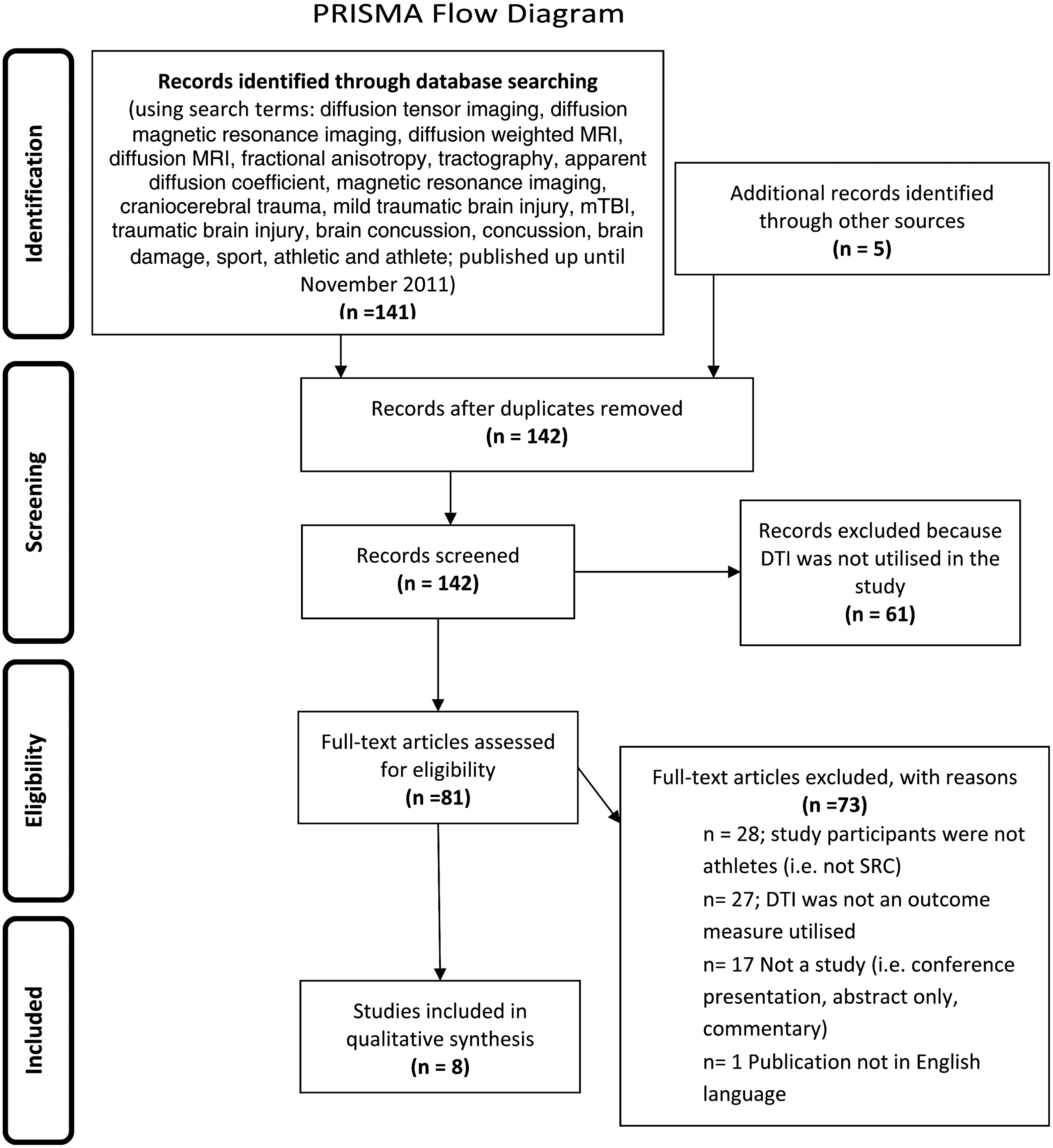
In stage 1, articles were retrieved via online database searching, hand-searching reference lists, and performing cited reference searches (see Fig. 1). The online databases of PsycINFO®, MEDLINE®, EMBASE, SPORTDiscus™, Scopus, Web of Science, Informit, dissertations, and theses were searched. Keywords and combinations of these words were used to search the databases comprehensively: diffusion tensor imaging, diffusion magnetic resonance imaging, diffusion weighted MRI, diffusion MRI, fractional anisotropy, tractography, apparent diffusion coefficient, magnetic resonance imaging, craniocerebral trauma, mild traumatic brain injury, mTBI, traumatic brain injury, brain concussion, concussion, brain damage, sport, athletic, and athlete. Articles were limited to those that were published in English-language journals up to February 2012, although several articles reported later in 2012 that were part of a special issue on mTBI (Brain Imaging and Behavior, June, 2012) were also reviewed. The reference lists of articles retrieved for inclusion in the review were hand searched to identify other relevant articles. Key articles retrieved via online databases and through hand searching reference lists were also used for further searches using the Web of Science Cited Reference function. The results of cited reference searches were narrowed using the key words diffusion tensor imaging or DTI; concussion or sports-related concussion; sport; and athletic or athlete. This was undertaken to capture the most relevant articles for further evaluation and critical appraisal.
Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA).
During stage 2, the titles and abstracts of articles were reviewed to assess eligibility for inclusion in this review. Articles were regarded as relevant, and warranting inclusion in the review if they were experimental studies using diffusion tensor imaging to determine the presence (or absence) of neurological abnormality in concussed athletic samples. Studies were included whether they were conducted with acute or long-term concussed athletes (i.e., there were no restrictions placed on time elapsed since injury) and whether or not they also used other measures of neurological function (i.e., conventional MRI, CT, symptom checklist, balance testing, or neuropsychological testing). Where there was uncertainty about whether a study should be included based on the review of the title and abstract, the full article was retrieved.
In stage 3, all retrieved articles were independently assessed for quality using a standardized quality assessment checklist selected for its generic comprehensiveness and currency. 40 The methodological quality of the included studies was scored according to the criteria lists developed for both primary research and review articles. 40 The criteria list included questions pertaining to both study relevance and validity. Validity questions considered a number of dimensions including: the research question and aims; participant and control selection criteria; prevention or acknowledgement of potential biases; exposure and intervening factors; appropriateness of statistical analyses; and whether conclusions were supported by results. The criteria answer format included designation of studies as positive, neutral, or negative. A study qualified for a positive score if: 1) it included an appropriate selection of study participants and matched controls, 2) intervention(s) were described in detail, and 3) the measures used were valid and reliable. Negative criteria were assigned to studies in which at least 6 of the 10 validity questions were not met. The neutral criteria were assigned to studies that had not fully met the positive criteria abovementioned, but nevertheless offered some valid information.
The checklist included such items as whether the research question was clearly stated, whether the selection of study subjects/patients was free from bias, whether the study groups were comparable, was the method of handling withdrawals described, was blinding used to prevent introduction of bias, were interventions or procedures and any comparison(s) described in detail, were outcomes clearly defined and the measurements valid and reliable, were statistical analyses appropriate for the study design and type of outcome indicators, were conclusions supported by the results with biases and limitations taken into consideration, and was the potential bias caused by the study's funding or sponsorship disclosed (see Table 1).
Y, yes; N, no; P, positive; O, neutral.
Data extraction
Initially, one reviewer extracted data from the identified studies, including 1) participant demographics (athletes and control subjects), 2) characteristics of participants (sport, exposure to concussion, concussive history), 3) DTI paradigms (technique and data extraction), 3) time lapsed (acute versus delayed assessment), 4) anatomical structures studied, 5) results of the study, and 6) study comments (see Tables 2 –7 for data extraction results).
PCS, post-concussion symptoms; SRC, sports-related concussion; GCS, Glasgow Coma Scale; PTA, post-traumatic amnesia; LOC, loss of consciousness; TBI, traumatic brain injury; S, subject group; C, control group; yr, year; CIS, concussion in sport; N/A, not applicable; NR, not reported; PCS, post-concussion symptoms; SRC, sports-related concussion; GCS, Glasgow Coma Scale; PTA, post-traumatic amnesia; LOC, loss of consciousness; TBI, traumatic brain injury; S, subject group; C, control group; conc., concussion; Ax, assessment; CIS, concussion in sport; N/A, not applicable; NR, not reported.
Uni, university; ImPACT, Immediate Post-Concussion Assessment and Cognitive Testing; MRI, magnetic resonance imaging; fMRI, functional magnetic resonance imaging; BOLD, blood-oxygen-level-dependent; HAVLT, Hopkins auditory verbal learning test; TMT, trail making test; SDMT, symbol digit modalities test; WM, white matter.
DTI, diffusion tensor imaging; NP, neuropsychological; ImPACT, Immediate Post-Concussion Assessment and Cognitive Testing; SCAT, Sports Concussion Assessment Tool; Ax, assessment; RT, reaction time; VRSN, virtual reality spatial navigation task; PCSx:, Post Concussive Symptoms Checklist; SAC, Standardized Assessment of Concussion; MRI:,magnetic resonance imaging; fMRI BOLD, functional magnetic resonance imaging, blood oxygen level-dependent; SWI, susceptibility weighted imaging; MRS, magnetic resonance spectroscopy; MR PCA, phase contrast angiography; LH, left hemisphere; WM, white matter; FA, fractional anisotrophy; MD, mean diffusivity; ADC, apparent diffusion coefficient; BDav, brain diffusivity average; NR, not explicitly reported; DL-PFC, dorsolateral prefrontal cortex; IC, internal capsule; SLF, superior longitudinal fasciculus; CC, corpus callosum; CST, corticospinal tract; SRC, sports-related concussion; CSP, cavum septum pellucidum; DTI Analysis Method A, voxel-based approach; B, region of interest; B1, statistical parametric mapping (SPM) / voxel-based statistics (VBM); B2, tract-based spatial statistics (TBSS); C, tractography; ROI, region of interest.
MD, mean diffusivity; FA, fractional anisotropy; ADC, apparent diffusion coefficient; DAI:, diffuse axonal injury; DTI, diffusion tensor imaging; GCS, Glasgow Coma Scale; DL-PFC, dorsolateral prefrontal cortex; SRC, sports-related concussion; fMRI, functional magnetic resonance imaging; BOLD, blood-oxygen-level-dependent; mTBI, mild traumatic brain injury; NP, neuropsychological; CSF, cerebral spinal fluid; BDav, brain diffusivity average; FA, fractional anisotropy; CC, corpus callosum; IC, internal capsule; DTI, diffusion tensor imaging; MRI, magnetic resonance imaging; SD, standard deviation; CTE, chronic traumatic encephalopathy; CST, corticospinal tract; MD, mean diffusivity; FA, fractional anisotropy; AD, axial diffusivity; WM, white matter; ROI, region of interest; DTI, diffusion tensor imaging; ImPACT, Immediate Post-Concussion Assessment and Cognitive Testing; MRI, magnetic resonance imaging; SWI, susceptibility weighted imaging; MRS, magnetic resonance spectroscopy; CBF, cerebral blood flow; mTBI, mild traumatic brain injury; VBA, voxel-based approach; SHB, subconcussive head blows.
ROIs, regions of interest; T, tesla; MRI, magnetic resonance imaging; fMRI, functional magnetic resonance imaging; MD, mean diffusivity; FA, fractional anisotropy; TR, repetition time; TE, echo time; DTI, diffusion tensor imaging; EPI, echo planar imaging; GRAPPA, generalized auto calibrating partial parallel acquisition; iPAT, integrated parallel acquisition techniques; MP-RAGE, magnetization prepared rapid gradient echo; ETL, echo train length; NSA, number of signal averages; FOV, field of view; WB, wildbootstrapping; min, minute; MS, millisecond; CC, corpus callosum; IC, internal capsule; (L), left; (R), right; mm2, millimeters squared; mm3 millimeters cubed.
TBSS, tract-based spatial statistics; FA, fractional anisotropy; ADC, apparent diffusion coefficient; BDav, brain diffusivity average; MRI, magnetic resonance imaging; fMRI, functional magnetic resonance imaging; SMP, statistical parametric mapping; WM, white matter; GM, gray matter, MRI, magnetic resonance imaging; MDT, minimal deformation target; FA, fractional anisotropy; MD, mean diffusivity; ROIs, regions of interest; DTI, diffusion tensor imaging; WB, wild bootstrapping; SnPM, statistical nonparametric mapping; cm2, centimeters squared.
Methodological quality assessment
Three reviewers (A.G., F.K-L., and A.H.) independently scored the included articles according to the quality assessment criteria using the checklists described previously. Consistency was attained without further discussion across four of eight articles. The specifics pertaining to rating inconsistencies among the four other articles were resolved via discussion between the lead author (A.G.) and each individual reviewer (F.K-L. and A.H.) to obtain a consensus agreement.
Results
A total of 146 articles were identified using the search strategy outlined in Figure 1. The initial search strategy was extremely liberal, in order to capture all possible articles for inclusion in this review. Of identified citations, 142 were screened following removal of duplicates, with 81 retrieved and screened for eligibility. Because of the nature of the initial liberal approach to searching for relevant articles, 61 were immediately identified as not meeting criteria, as they had not used DTI. Of the remaining 81 articles, 28 were excluded on the basis that the participants were not athletes (i.e., they were not SRC cases), 27 studies on closer inspection also had not used DTI as an outcome measure, 17 were not research studies (i.e., conference presentation, abstract only, commentary), and one publication was not in English. The final outcome following this screening process resulted in the inclusion of eight articles for this review.
A total of 55 review articles on DTI in TBI samples were also identified through the current search strategy. Of these, only nine reviews were focused on SRC, with all but one providing only a brief overview. In addition to this, a Master's level dissertation was also identified but not included in the current review, as no manuscript of this work had been published in a peer-reviewed journal.
The quality assessment resulted in four studies with positive study quality ratings and four with neutral quality study ratings. None of the identified studies were rated with negative quality ratings when assessed against the pre-specified standardized criteria. 40 The neutral rating was assigned to studies because of participant selection bias and the use of control groups that were not comparable (see Table 1 for the quality assessment results).
The quality assessment of the one review article identified that met inclusion criteria, Davis and colleagues, 41 was assigned a neutral review quality rating because of the absence of a description of how the authors appraised the quality of the studies included in their review, making replication of their review impossible.
A total of 214 athletes participated across the eight studies, with the results of 96 “neurologically intact” control participants also reported. One study also included two moderate TBI and three severe TBI patients as a means of exploring the effects of severity on DTI data. 42 Four of eight studies involved only male samples. 43 –46 Of the four studies 1,42,47,48 that included a mixture of both genders, one 42 included a 50:50 split, and another 48 had one female as a control subject in their sample. Another comprised nine males and three females, 1 whereas another 47 reported a 70:30 (male:female) ratio for their overall sample but did not report whether the ratio was consistent across study groups. In total, 284 males and 26 females were represented in the overall sample, and sex differences in findings were not fully explored. In terms of the sports represented, three studies involved a strict cohort of boxers, 43 –45 whereas the other five samples included a mixed sample of contact sport athletes 1,42,46 –48 (see Tables 2 –4).
Findings within subject groups and across studies varied greatly with both increases and decreases in FA, and mean diffusivity (MD) measures reported. There was a trend across studies for ADC to increase post-SRC. 43 –45 The detected changes within voxels were located in a variety of neuroanatomical regions, with the corpus callosum, 44,49 internal capsule, 42 –44 the inferior longitudinal fasciculus, 42,43 and superior longitudinal fasciculus 42 the most common regions identified. In contrast, Maugans and colleagues 1 who also included the corpus callosum and internal capsules as ROIs, found no significant differences between the concussed sample and age-matched controls. Three studies used a whole brain analysis method 45,46,48 (see Table 5).
Although it is well recognized that concussion history, injury dynamics and severity, and clinical presentations in SRC samples are heterogeneous, the lack of reporting of detailed individual versus group data was notable (only two out of eight studies reported individual data; 1,20 see Tables 2 –4). This was particularly evident in terms of concussion severity, history of previous concussion, and reported post-concussion symptoms, all of which provide important information that could be correlated with the individual's DTI results. The difficulty with recall bias in obtaining valid retrospective data on the number and nature of the SRCs has been noted previously. 50 Only Maugans et al 1 reported individual data on number of previous concussions. Information pertaining to the exposure levels, such as years of play, position played, and number of bouts (in the boxing cases) were also often absent. Therefore, it is not known in some cases whether the DTI data acquired represent the sequelae of the current concussion, a previous history of concussions, or a combination of both. In all but one study that recorded the number of subconcussive hits sustained during a season, 48 there was no indication of the level of prior exposure to head trauma. Even in the one study that reported on the subconcussive hits, there was no prior history reported and the recording of the subconcussive hits relied on self-reported information, which has its own limitations. This is understandable, however, given that reporting of past subconcussive blows to the head would likely be even less reliable or valid than reports of past diagnosable concussions. Nonetheless, in examining current concussion or subconcussive blows to the head, often it is not known what the previous history might be.
The MR demographics (manufacturer and magnet strength, head coil channels), data acquisition (e.g., number of directions) and post-processing procedures also varied considerably across studies (see Tables 6 and 7). Given this variation, it is not surprising that there is limited convergence of the results. Attempting to interpret the extent to which these methodological variations across studies contribute to the variation observed in the results is quite complicated, particularly, as noted previously, given that concussion is heterogeneous with respect to injury, depending upon where the injury occurred.
Three studies examined the acute effects of SRC, 1,46,48 and one of these also conducted a 2 week and >1 month follow-up, 1 whereas another conducted a 6 month follow-up examination, 46 one study at the subacute phase 47 and one study at the chronic (and still symptomatic) phase. 42 Three studies did not report on the time lapse between injury and DTI examination. 43 –45
Repeated or follow-up DTI was only conducted in three of the eight identified studies, 1,44,46 but in one of those studies only 2 of the subjects in the sample of 49 (∼4%) had follow-up imaging. 44 The results of these two cases demonstrated a decrease in trackable fibers in the whole brain and corpus callosum compared with the results of the initial scans. 44 However, interpretation of this result is limited because there were no control subjects imaged serially during the same time period, and therefore the possibility that the effects are caused by experimental instability cannot be excluded. A more comprehensive study reported follow-up results for both concussed and control samples. 46 The results of this study reported increased FA in dorsal regions of both corticospinal tracts and the corpus callosum in concussed athletes at the acute and chronic (6 months) time points compared to non-concussed controls. Additionally, elevated axial diffusivity (AD) values in the right corticospinal tract and decrease in MD values in the corticospinal tracts and the corpus callosum across both time points were also observed in the concussed group compared with the controls. 46 There was no report on the possible time×group effect (i.e., did the magnitude of group differences change with time). In contrast to these results, Maugans and colleagues, 1 who included the corpus callosum (genu, body, and splenium) and internal capsule (anterior or posterior limb) as regions of interest, found no significant difference across DTI metrics in concussed 11–15-year-olds compared with age-matched controls at 3, 14, and 30 days post-injury. Interestingly the authors reported group differences at 3 days post-injury on reaction time and total symptoms score on a computerized neuropsychological test that resolved at the 14 day follow-up, which arguably refutes any suggestion that the participants may not have sustained a concussion.
Discussion
This review identified only eight studies published through February 2012 that have used DTI within SRC samples. Following quality assessment of these studies, four were given a positive quality rating and four a neutral quality rating, with no study receiving a negative quality rating. 40 With the exception of one study in adolescents, 1 each of the other seven studies investigating DTI in athlete samples reported some type of DTI abnormality; however, the anatomical location was inconsistent. This variance in location is not surprising in view of the heterogeneity of concussion, in addition to the variability in these studies between time of injury and DTI scanning. Some regions, such as the corpus callosum, internal capsule, and longitudinal fasciculus, are reported more often than others, which may further suggest the vulnerability of these structures to axonal injury in concussion.
Acute phase
Diagnostic potential of DTI in SRC
In the general mTBI literature, DTI has been touted as more sensitive than other imaging techniques to the subtle changes observed post-injury. This advance in MRI acquisition and analysis may make it possible to better characterize the extent of brain abnormalities in mTBI within days of injury. 12
The results of the current review suggest that DTI is also a more sensitive method of detecting change in SRC than are conventional MRI techniques. All studies examining concussion in the acute stages that were included in this review identified significant group changes in their samples, suggesting that DTI can identify microstructural white matter abnormalities, and that therefore it is a potentially important diagnostic tool. Four studies 43 –45,47 found nonspecific white matter and periventricular changes on conventional MRI techniques, which were quantified in much greater detail by using DTI.
Prognostic potential of DTI in SRC
At the current time, data are limited regarding the prognostic ability of DTI in any concussion sample. Although follow-up data have been published, there has been no published longitudinal study conducted with SRC samples that correlated initial DTI results with long-term outcomes. For example, whether or not an observed change in FA in the acute phase following injury or, for that matter, at any time over the course of recovery is predictive of poorer outcome requires far more investigation.
Subacute/chronic phase
Further diagnostic potential of DTI in SRC
Some study results included in the current review suggest that, as is the case in the acute phase, DTI is a more sensitive method of detecting change even weeks to months post-injury in concussed individuals compared with conventional MRI techniques. All studies in this review examining SRC in the subacute and chronic stages identified significant group differences in DTI indices in their samples.
Further prognostic potential of DTI in SRC
As is the case in the acute phase post-injury, data are limited regarding the prognostic ability of DTI data collected in the subacute or chronic stages of recovery in concussion samples of any kind. Many of the identified DTI studies of SRC either examined subjects acutely after injury, or at a chronic time point. Again, there has been no published longitudinal study conducted with SRC samples that correlates subacute or chronic DTI indices with any long-term outcomes. In particular, the implications of early increases or subsequent decreases in FA, or reduced MD, for poorer outcome, remain unclear.
Only one study in the current review reported follow-up imaging on their SRC sample, 46 whereas another reported follow-up imaging in only a small minority of their overall sample (n=2). 44 This has also been identified as a shortcoming in the general mTBI literature, where studies that have tended to include both acute and chronic time points either have a small number of subjects, 51 consist of separate acute and chronic groups not followed longitudinally, 11 consisted of separate cohorts of acutely and chronically injured patients, 52 or only had neuropsychological testing and no imaging at chronic phase follow-up. 53,54 As such, it is difficult to ascertain how DTI metrics change as the injury progresses or recovers. Of note is that 15–30% of mTBI (not necessarily SRC) patients develop chronic post-concussion syndrome, 55,56 and longitudinal studies will be critical in determining whether or not DTI can help predict which patients continue to experience chronic symptoms. A longitudinal study that investigates the course of injury over time would provide important information regarding the staging, progression, and, possibly, recovery and reversal of brain injury over time (see review by Shenton and colleagues 12 ).
Although cross-sectional DTI studies have been conducted, 57 –59 there is currently insufficient cross-sectional normative data for any DTI index in athlete samples, and no data on variables related to simply participating in contact sport. Basic research on these variables is also critical if we are to judge the value of DTI in detecting or predicting persistent effects of SRC or recovery. Data on the test–retest reliability of DTI indices in concussed and non-concussed participants at various ages is also critical in judging clinically significant change. 60 The inclusion of pre-participation and post-injury DTI data would be ideal, and better longitudinal quantification of both concussive and subconcussive head trauma would help clarify the very diverse findings and the DTI–neuropsychological outcome links.
Despite the small number of studies examining DTI in samples of concussed athletes, considerable variability with respect to the magnetic field strength, time period of scanning post-concussion, brain regions examined, methods of data acquisition and the post-processing techniques employed are apparent. The obvious methodological variations could easily account for the diverse findings, however most of the studies (seven out of eight) have reported radiological evidence of subtle brain injury in SRC. Surprisingly, the only study where nonsignificant DTI findings were observed used a sample of 12 11–15-year-olds. This may reflect the rapid maturation that occurs through this age range; therefore, the greatest spread of data may have been observed in this sample, and, as such, detection of group differences was more difficult.
Arguably the greatest limitation of this body of work to date is the absence of exposure/concussion history details and information on the severity of injury. A number of points are worth elaboration. First, a large amount of important individual information is inherently lost in group data analysis. The absence of individual data in combination with the small sample sizes in the majority of the identified studies in this review is a large limitation for generalizing these results. Second, without adequate history of exposure (i.e., a proxy measure for subconcussive blows) and a history of previous SRCs, it is not possible to accurately determine whether the DTI abnormalities observed are a consequence of the most recent concussion, a culmination of previous concussions, or a combination of both. Third, injury severity information was only presented in one study, 42 which limits the potential conclusion that can be drawn regarding the sensitivity of DTI in detecting changes post-SRC. This is a particularly important point when considering the results of those studies that used mixed (i.e., participants recruited from varying sports) samples, as exposure, cause, and severity of injury can vary considerably across sports. For example, it is acknowledged that boxing (where the aim of participation is to deliver knockout blows to an opponent's head and body), is a considerably different sport leading to different injury etiology than that of other contact/collision sports, such as American football, in which concussive injuries may be the result of unintentional/innocuous incidents. 61 In view of this distinction, the ability to make a comparison between the results in boxing samples and those in other collision sports is limited, and pooling data across sports appears unjustified. A further limitation to this body of work is the absence of any information pertaining to the mechanism of injury, that is, the site of impact and nature of the cause of the SRC (e.g., whiplash, blow to forehead). This level of detail would have been useful to correlate with the findings on DTI.
A number of further limitations exist that require consideration in interpreting these data. First, four studies were identified as possessing control groups that were not comparable. 43 –45,48 This presents a considerable limitation to interpretation of any observed group differences, because such differences may be unrelated to the variable of interest (in this case, SRC). Second, within the field of SRC, it is known that gender differences are apparent in terms of susceptibility and recovery from concussive injury. 62 –65 Therefore, it is likely that merging male and female data introduces another variable that is hidden in discussing group data.
In addition, there is no agreement as to the best method to analyse DTI data (i.e., post-processing procedures). 19 This is not surprising, given that the field is in its relative infancy, and that novel methods are developed rapidly in this field. Comparing data extraction and processing methods head-to-head and determining their relative strengths in test–retest reliability and concurrent or predictive validity is certainly indicated as another important fundamental step in understanding the value of DTI. The predominant focus on cross-sectional studies has in its very nature limitations in terms of its ability to judge DTI's value in predicting outcome. This limitation and other factors noted previously argue strongly for the necessity for longitudinal research that follows athletes during the initial recovery period and the long term, especially in cases of recurrent concussion. Such data would provide important insights into individual differences in acute stage profiles, and also into factors that predict neuropsychological, psychiatric, or behavioral outcomes, and, possibly, the mechanisms that subserve the adjustment to or reversal of damage in what appear to be more resilient athletes.
Conclusion
The review identified eight studies that have used DTI in concussed athletes. The need for further investigation is apparent; however, one of the most attractive features of DTI in the SRC context is the potential for early identification of athletes with unresolved concussions who are at high risk for poor outcome, which may assist in more specific and effective clinical management. Uniformity in terms of methodology would certainly enable greater interpretation of the data across studies. As it is anticipated that there will be a proliferation of research employing this imaging technique within the field of sports concussion, developing an understanding of the fundamental mathematical characteristics of the various DTI indices and developing a consensus in the field regarding the most reliable and valid extraction and processing techniques is certainly recommended. Further systematic investigation will provide more information on this imaging technique for the diagnosis of SRC, monitoring the course of recovery (i.e., prognosis), and informing the management of athletes with single and recurrent SRC.
Footnotes
Author Disclosure Statement
No competing financial interests exist.