
Abstract
The goal of our study was to investigate different aspects of sleep, namely the sleep-wake cycle and sleep stages, in the vegetative state/unresponsive wakefulness syndrome (VS/UWS), and minimally conscious state (MCS). A 24-h polysomnography was performed in 20 patients who were in a UWS (n=10) or in a MCS (n=10) because of brain injury. The data were first tested for the presence of a sleep-wake cycle, and the observed sleep patterns were compared with standard scoring criteria. Sleep spindles, slow wave sleep, and rapid eye movement sleep were quantified and their clinical value was investigated. According to our results, an electrophysiological sleep-wake cycle was identified in five MCS and three VS/UWS patients. Sleep stages did not always match the standard scoring criteria, which therefore needed to be adapted. Sleep spindles were present more in patients who clinically improved within 6 months. Slow wave sleep was present in eight MCS and three VS/UWS patients but never in the ischemic etiology. Rapid eye movement sleep, and therefore dreaming that is a form of consciousness, was present in all MCS and three VS/UWS patients. In conclusion, the presence of alternating periods of eyes-open/eyes-closed cycles does not necessarily imply preserved electrophysiological sleep architecture in the UWS and MCS, contrary to previous definition. The investigation of sleep is a little studied yet simple and informative way to evaluate the integrity of residual brain function in patients with disorders of consciousness with possible clinical diagnostic and prognostic implications.
Introduction
M
Together with evidence of eye opening, the presence of a sleep-wake cycle defines the threshold between a comatose state and the UWS or MCS. Although it is well known that sleep abnormalities are common in critically ill patients, there is little empirical evidence that brain-injured patients actually exhibit electrophysiological sleep phenomena or display a circadian rhythm. 5 –9 In DOC, sleep-wake cycles are typically inferred by behavioral observations of periods of eye closure, but their underlying mechanisms remain poorly understood and their fine-grained characterizations are still unknown.
Our objective is, therefore, to describe the large variety of sleep patterns existing in VS/UWS and MCS patients and to test their potential clinical interest. To our knowledge, this is the first study specifically designed for the analysis of sleep in the vegetative and minimally conscious states and based on 24-h recordings of brain activity.
Methods
Patients
A 24-h polysomnography was performed in sub-acute (1–12 months after brain injury), unsedated, and spontaneously breathing DOC patients in their usual clinical environment. Clinical assessment and diagnosis were made using the recommended Coma Recovery Scale-Revised (CRS-R), performed the day before and after the recording by the first author. 10,11 Patients also received a diagnosis from the neurologists and neuropsychologists of the Coma Science Group. Patients with continuous epileptiform activity, suppression, or burst-suppression patterns were excluded from the present study. Outcome was measured at a 6-month follow-up using the CRS-R. The study was approved by the Ethics Committee of the Faculty of Medicine of the University of Liège, and written informed consent was obtained from the patients' legal representatives.
Data acquisition and analysis
Recordings
The 24-h polysomnography was performed with a V-Amp16 amplifier (Brain Products) with infrared video monitoring. We used 12 electroencephalography (EEG) channels localized according to the conventional 10–20 system, chin-electromyography (EMG), electro-oculography (EOG in crossed montage), and electrocardiography (ECG). We applied an analog band pass filter of (0.1–200 Hz), (10–100 Hz), (0.3–35 Hz), and (0.3–70 Hz) to the respective data channels. Impedance of all channels was kept <5 kΩ at the start and <20 kΩ at the ending of all recordings. Analyses were performed using a 64-bit Linux workstation and EEGLAB freeware running in Matlab. 12 Raw data were sampled at 250 Hz and filtered using 1 Hz high-pass and 45 Hz low-pass thresholds. Epochs containing electrode movement artifacts were visually rejected (1% in average). During the recording, patients experienced their usual environmental conditions.
Chronobiology
To locate the rest periods of patients, we built a map of each recording. EEG relative power spectrum, muscle tonus, eyes movements, heart-rate variability, and heart rate were plotted over time (Fig. 1). The spectrogram of the EEG activity was computed using standard Fast Fourrier Transform decomposition in EEGLAB, and missing data segment containing artifacts were interpolated. For eyes movements, we plotted the average power of the EOG channels in the 1–3 Hz frequency band, because eye channels have most power within these frequency bands at wake. For muscle activity, no artifactual data were removed from the 24-h period, because paroxysmal muscle activity can be interpreted as movement. For heart rate, we applied a band-pass filter between 1.5 Hz and 30 Hz and extracted heart beats by applying an automatic threshold, depending on the standard deviation of the recorded ECG signal. Heart beat intervals falling outside of the physiological range of 0.3–1.35 sec were considered artefactual and were removed (<1% for each recording). Finally, all data measures were finally smoothed over time using a Gaussian filter.

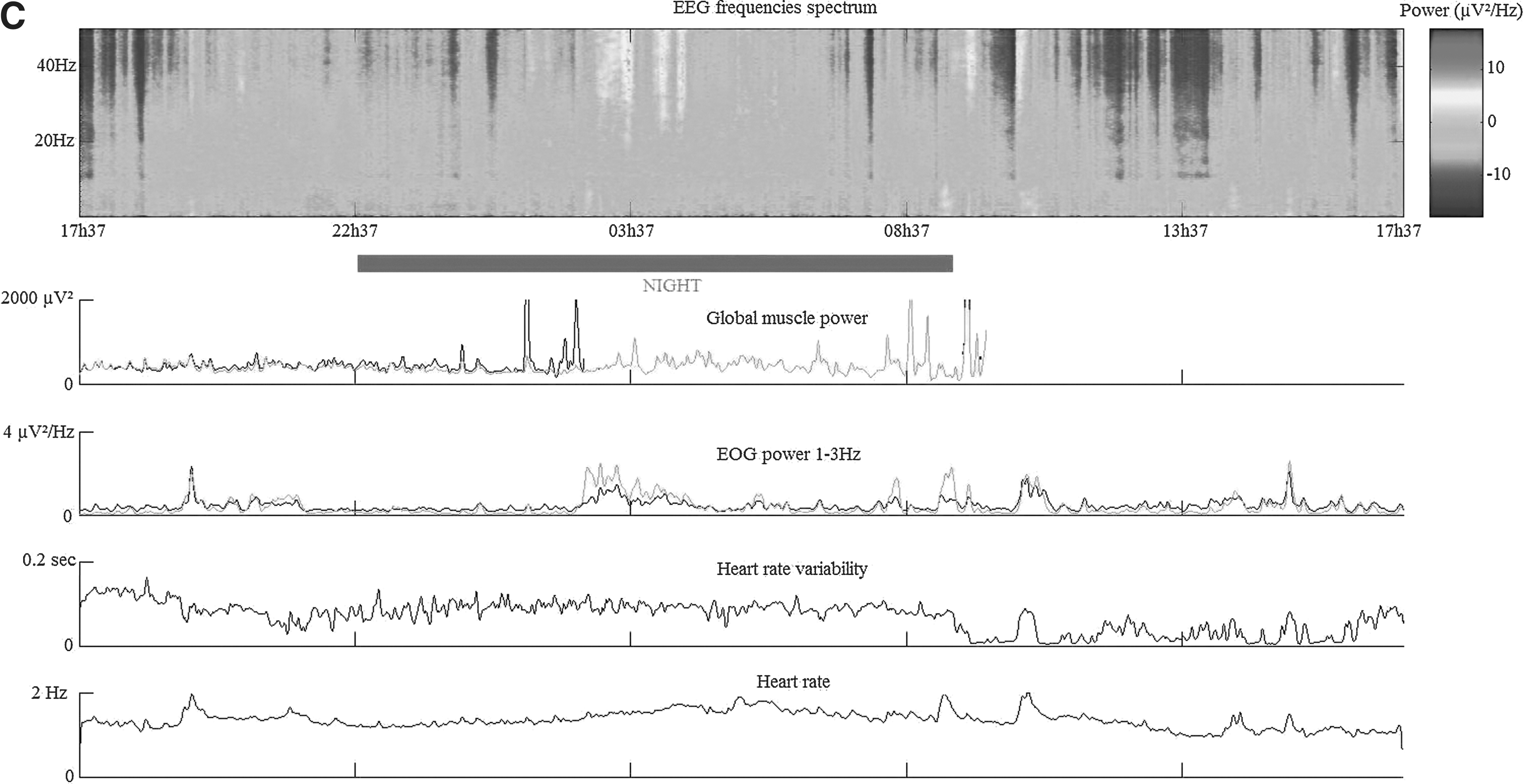
On these chronobiological plots, a “rest pattern” was defined as a simultaneous slowing of the EEG relative spectrum and decrease of the global muscle power, EOG power, heart rate, and heart-rate variability, because this is the case in healthy subjects. The problem: as yet, there is no empirical description of the EEG frequencies spectrum in the UWS and MCS. Moreover, the muscular artifacts contaminate the EEG channels in the 10–100 Hz band. An EEG slowing was therefore defined here as a reduction of the muscular frequencies from positive (hot colors) to negative (cold colors) relative power values. Indeed, even if standard background and cognitive high frequencies (12–40 Hz) are preserved in brain-injured patients, these are not visible in data unfiltered for muscular artifacts because these are of much higher amplitude. As for slow wave activity during the wake and rest phases, this was found to vary too much both individually and across our sample to be used as a proven sleep criterion.
Once the chronobiological figures were plotted, we noticed three recurrent patterns. Patients were classified as “cycled” if the patient was at rest during at least 80% of the nighttime and awake during at least 80% of the daytime (Fig. 1A), or “uncycled” if this distinction was absent (Fig. 1B). Patients showing at least two periodic rest-wake patterns were classified as “ultradian” (Fig. 1C). Nighttime corresponds to the time a patient is left alone with the light off to the time he is woken by the nurse or family with the light on (10 pm±1 h to 9 am±1 h). During the day, the room ambient lighting was normalized using the room lamps when the weather was dark. We also compared the mean value of the muscular spectral power between the day and night in cycled and uncycled patients using the paired t test corrected for multiple comparisons (p<0.01) to provide an objective and quantified marker of sleep-wake cycling (Fig. 2). Because one of the two EMG channels was unreliable during the last hours of recording for 9/20 patients, we calculated the 10–100 Hz power on the EEG temporal channels (T3, T4) as an EMG proxy measurement.
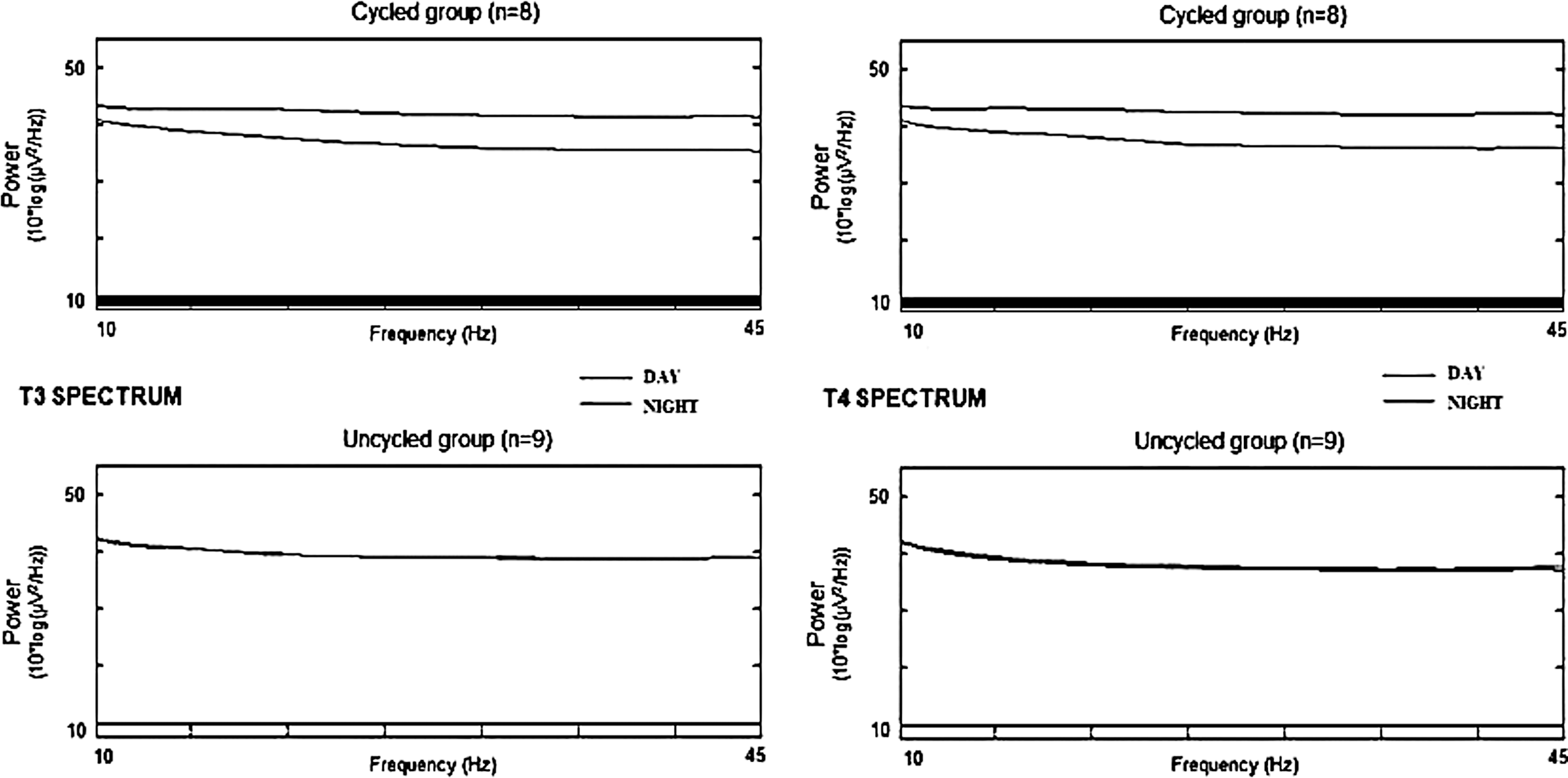
Muscular spectrum of the T3 (left) and T4 (right) channels during day and night in cycled (upper panel) and uncycled (lower panel) patients. The black bar represents significant difference between the two groups at a paired t test corrected for multiple comparisons (p<0.01). Note that the 10–100 Hz spectrum is cut at 45 Hz because of the data preprocessing.
Visual scoring
Sleep analysis was performed by three independent, experienced scorers (VC, XD, and SP). The visual scoring of sleep patterns was performed using the EEGLAB visualization window. The first scorer reiteratively explored the data and listed the different standard and alternative sleep patterns encountered. Next, the other scorers assessed the presence of the reported patterns using a blind method. Ambiguous scoring conflicts were resolved by common consensus, and standard spindles, slow wave sleep (SWS) and rapid eye movement sleep (REMS) were calculated.
Definition of standard sleep scoring criteria
The waking state is characterized by a high-frequency (>10 Hz) desynchronized EEG, a high muscular tone in EMG channels, and eye blinks in EOG channels. Stage 1 is defined by a slower and synchronized EEG, a low muscular tone, the absence of eye blinks, and the occurrence of slow eye movements. The α waves, occurring when eyes are closed, progressively slow down toward θ activity. Persons aroused from this stage often believe that they have been awake. Sleep spindles were initially defined as 12–15 Hz bursts under 50μV amplitude, lasting 0.5–2 sec, having a typical sinus-like shape, best visible in the central channel, and generally occurring during the sleep stage 2 preceding SWS. 13 Later, it was shown that spindles can have a larger frequency band (10–16 Hz) and topography. 14
SWS is defined by a high amplitude (75–140 μV) synchronized EEG in the δ band including at least 20% (stage 3) or 50% (stage 4) slow waves that are most visible in the frontal channels, a low muscular tone close to atonia, and the absence of eye blinks and movements. Paradoxical sleep—or REMS—is characterized by a synchronized EEG in the θ band, a muscular atonia, and the presence of phasic events such as REM and muscular twitches. It is generally preceded by SWS (night start) or stage 1 (night end) and interrupted by an awakening.
Results
We included 20 patients (10 VS/UWS and 10 MCS) of traumatic (n=9) and non-traumatic etiology (anoxia, n=6 and cerebrovascular accident [CVA], n=5). Demographic, clinical, and outcome data are summarized in Table 1.
SWS, slow wave sleep; REM, rapid eye movement; itCVA, infratentorial cerebral vascular accident; UWS, unresponsive wakefulness syndrome; stCVA=supratentorial cerebral vascular accident; MCS, minimally conscious state; mCVA=meningeal hemorrhage.
CRS-R: A=Auditory, V=Visual, M=Motor, OV=Oralmotor/Verbal, C=communication, W=Wakefulness. MCS+=The MCS+ describes a clinical subpopulation with high-level behavioral responses (command following, intelligible verbalizations, or non-functional communication) and a higher degree of recovery compared with the MCS. 36
CAP: Cyclical alternating pattern of frontal cortical synchronization arousals >75μV (318.0 min in VS/UWS8).
A polysomnographic sleep-wake cycle was found in 3/10 VS/UWS and 5/10 MCS. An ultradian pattern was found in one VS/UWS and two MCS patients. In the cycled patients' group, the mean of the muscular spectral power was significantly higher (p<0.01) during the day (10 am–10 pm data segment) than during the night (10 pm–10 am) according to the paired t test with false discovery rate correction for multiple comparisons in EEGLAB (Fig. 2).
Comparison of the observed sleep patterns to the standard criteria
The wake EEG of brain-injured patients is generally described as “slowed” (i.e., from standard α–β to predominant δ–θ activity under 75 μV amplitude) and showing phasic or tonic high amplitude epileptiform bursts that reflect the brain injury (Supplementary Fig. 1; see online supplementary material at
This clinical population is by definition generally non-cooperative and can hardly be forced to relax their muscles and eyes without using drugs. Another difficulty concerning these patients is that being awake doesn't mean being “aware” for these patients, and there is also no evidence of any electrophysiological difference between an aware and an unaware waking state in the literature. In consequence, the only possible scoring criteria for the waking state in polysomnography of brain-injured patients are the presence of eye blinks and, of course, the absence of sleep patterns.
Similarly, stage 1 was defined as the absence of eye blinks (i.e., eyes closed), spindles, SWS, and REMS (Supplementary Fig. 2; see online supplementary material at
Standard sleep spindles and SWS were detected in some of our recordings. We also found some spindles in the 6–9Hz frequency range which were defined as “slow spindles” (Supplementary Fig. 3; see online supplementary material at
Finally, paradoxical sleep did match with the standard scoring criteria (Supplementary Fig. 5; see online supplementary material at
Interscorer rate
The scorers' qualitative analysis (presence or absence of sleep patterns) matched except on the following points and these cases were then discussed before reaching a common agreement: (1) The existence of rare standard spindles (n<10) in VS5, VS8, MCS1, MCS3, MCS4, MCS9 ; (2) The CAP of VS8 ; (3) The REMS primes of MCS2.
The quantitative analysis matched between the scorers except for the cases seen in Table 2.
REMS, rapid eye movement sleep; SWS, slow wave sleep.
The quantitative study confirms the general rule that there is always a difference between the visual scorings of several independent sleep specialists. It also raises an important point that SWS and REMS can be easily definable in some patients but not others. Indeed, we noted that SWS could have clear boundaries and good stability in some cases (especially in UWS patients), while in other cases, the limits are progressive and the slow waves' amplitude unstable, making the interscorers quantification less consistent (especially in MCS patients). As for REMS, interscorers discrepancies show that the first scorer tended to overestimate the number of episodes. This confirms that the scorer's experience affects the scoring of sleep but also suggests that brain-injured patients may have episodes resembling REMS. Nevertheless, from a clinical point of view, we argue that it is more important to know what sleep stages are preserved rather than their exact quantities in brain-injured patients.
Sleep stages
All patients showed sleep stage 1. Three MCS patients had preserved spindles (n>10), SWS, and REMS. Standard spindles were found in 4/10 VS/UWS and 7/10 MCS patients; number varied between 1 and 539. Slow spindles were found in 5/10 VS/UWS and 7/10 MCS patients. Six patients did have both standard (n<10) and slow spindles. Standard SWS was found in 3/10 VS/UWS and 8/10 MCS patients. On average, the number of epochs was 5.3±2.1 and the duration 36.0 min±21.0 min in the VS/UWS; 11.5±6.9 and 16.4 min±10.3 min in the MCS. Attenuated SWS was found in 6/10 VS/UWS and 2/10 MCS. REMS was found in 3/10 VS/UWS and 10/10 MCS patients. On average, the number of epochs was 6.3±2.9 and the duration 9.0 min±5.2 min in the VS/UWS ; 4.9±3.2 and 4.4 min±2.0 min in the MCS. All these amounts of standard sleep stages (Table 3) cannot be statistically compared yet, because the number of patients showing them is too small. The persistence of REMS is correlated with MCS patients: χ2=10.8, p=0.005 (Pearson uncorrected).
REM, rapid eye movement, UWS, unresponsive wakefulness syndrome, MCS, minimally conscious state.
Concerning the outcome study, a low number of spindles (n<10) was found in four persistent patients; in one MCS patient who recovered occasional command following; and in one VS/UWS patient who improved to the MCS. An intermediate number of spindles (in the 101 range) was found in one VS/UWS and two MCS patients who improved to the MCS+. A high number of spindles (in the 102 range) was found in one VS/UWS and one MCS+ patient who recovered consciousness (exit-MCS). Six of the seven patients with a favorable outcome showed standard spindles in their recording (Table 4). Eight of the 13 patients with an unfavorable outcome showed no spindles, and the five others showed a low number of standard spindles (n<10).
Favorable outcome=behavioral improvement according to the Coma Recovery Scale-Revised.
Unfavorable outcome=persistent or degraded behavior.
Discussion
Patients in a MCS or VS/UWS can show a circadian, ultradian, or uncycled sleep-wake pattern. This is in line with a previous study showing that the sleep cycle can be present or absent in persistent VS patients with no obvious difference in their clinical status. 20 These data suggest that the absence of a sleep-wake cycle might reflect the brainstem damage in DOC. Sleep spindles can possibly be present, slowed, or absent in both MCS and VS/UWS patients with all three etiologies. Patients who clinically improved within 6 months are more prevalent in classes with a high count of standard spindles (10<n<100 and 100<n<1000) and fewer in those with a low count (n=0 and 1<n<10) than patients with persistent or degraded outcome : χ2=12.4, p=0.002.
This correlation, however, between the number of standard spindles and outcome 6 months later remains speculative because the number of patients in the different classes is too small. It does, however, highlight the potential prognosis value of sleep spindles in brain-injured patients, which is in line with the preliminary studies of sleep in comatose and vegetative patients. 8 Standard SWS is preserved in trauma patients and in anoxic MCS patients but not in CVA patients, suggesting that this etiology is particularly prone to SWS attenuation.
All our MCS patients showed phasic REMS, which is associated with dreaming in healthy subjects. Dreams being by definition a conscious experience, they have a differential diagnosis value in the VS/UWS. Indeed, it is now well known that some MCS patients are not able to show signs of consciousness on behavioral assessments, so they are evaluated as VS/UWS until fMRI or EEG active paradigms show the contrary. 21 –23 Moreover, the three VS/UWS patients who showed REMS were also the only VS/UWS cases having not only a sleep-wake cycle but also some inconsistent conscious features such as food swallowing, facial expressions sometimes congruent with stimulation, or an atypical pattern on positron emission tomography. We therefore support that UWS patients showing REMS should be priority submitted to active paradigms to test the persistence of a minimal consciousness at wake.
Our findings confirm that the operational definitions of wakefulness and sleep are not applicable in DOC. 8,9 Contrary to what several definitions state, the presence of rest periods does not always imply preserved electrophysiological sleep-wake cycles nor sleep stages that should no longer be taken as a distinguishing feature for the definition of UWS or MCS. 24,25 The waking state and sleep stages do not fit the elder standard scoring criteria, which therefore needs to be adapted for polysomnography in DOC.
This study is in line with earlier studies on coma suggesting that the presence of EEG patterns resembling standard sleep may be markers of a favorable outcome. 26 –29 Sleep research is of particular interest in brain-injured patients with various etiologies because it can bring to light relationships between sleep patterns and functional neuroanatomy. In particular, the quality and quantity of spindles seem to provide a new index of the severity of the thalamocortical injury in the VS/UWS and MCS (Fig. 3). This would be in line with brain imaging studies showing not only the correlation between the extent of thalamus damage and the behavioral disability and outcome in DOC, but also the restoration of the thalamocortical connectivity during recovery of consciousness. 30 –33 Otherwise, REMS is sensitive to cortical injury, so the amount of this stage may be related to the severity of the cortical injury and behavioral impairment in brain-injured patients, but our results don't support this hypothesis.
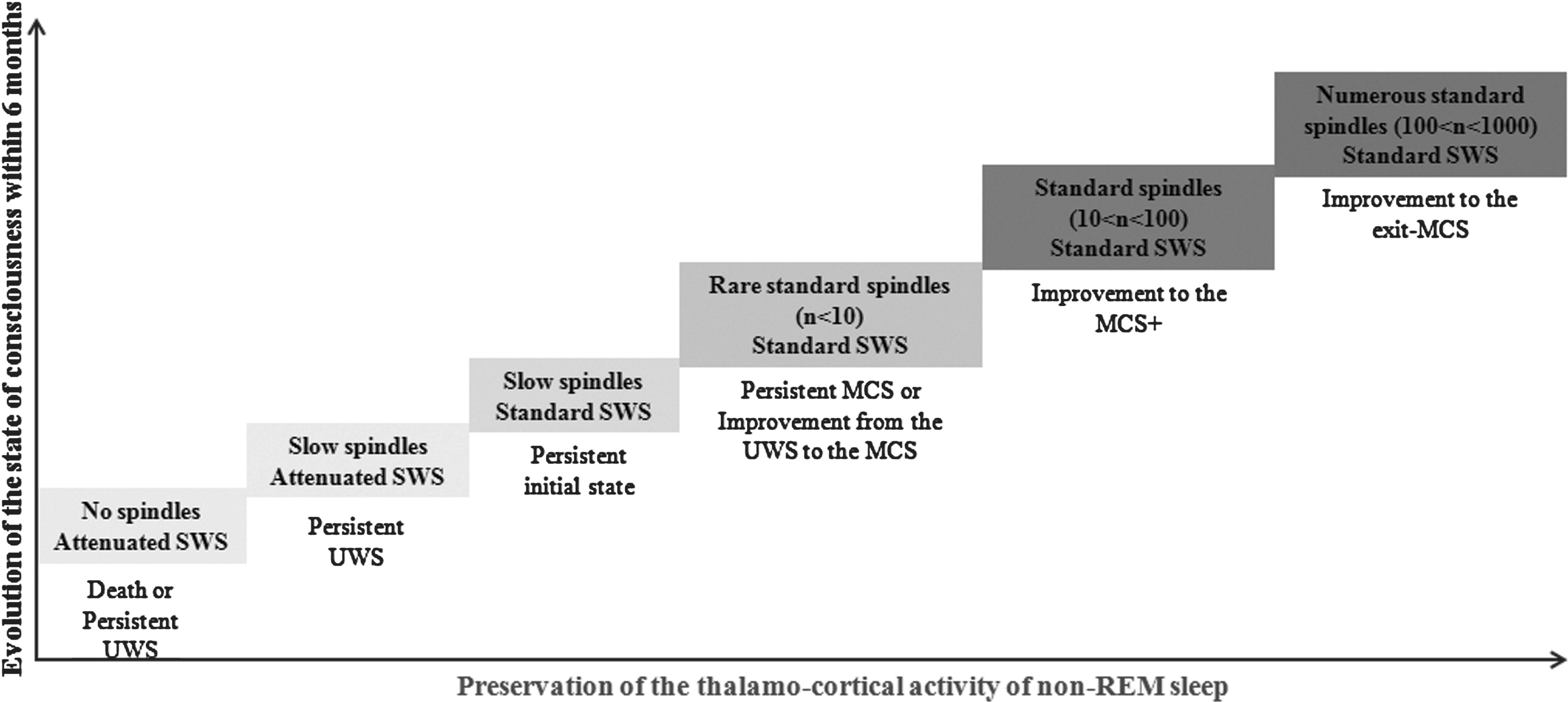
Hypothetical model of prediction of outcome according to the quality of non-rapid eye movement sleep in traumatic and anoxic brain-injured patients. UWS, unresponsive wakefulness syndrome; MCS, minimally conscious state; SWS, slow wave sleep.
Finally, although it is still unclear whether they have distinct or sequential roles, sleep is thought to optimize the consolidation of acquired information in memory and to impact on mental abilities. 34,35 This suggests that the revalidation process may be facilitated in brain-injured patients with preserved sleep compared with those without and stresses the importance of promoting sleep in the clinical routine.
Conclusion
For the purposes of testing cerebral activity in the VS/UWS, MCS, or intermediary patients who are between these two states, clinicians should keep in mind that arousal and consciousness can be severely impaired and chronobiologically disorganized in these populations. In consequence, a prolonged measure of the brain's spontaneous activity during at least 24 h is of primary interest: first, because it can inform the clinician about the temporal organization of the patient's vigilance states before a multimodal neurological assessment over several days; second, because it can reveal the possible persistence of residual brain activities such as sleep stages and thus provide additional prognosis or differential diagnosis information.
Moreover, 24-h polysomnography is a cheap and ambulatory method that could be adapted to the clinical routine of brain-injured patients in their usual environment contrary to brain scanners or high-density EEG. Further research on sleep-wake architecture in larger samples of patients will improve the clinical evaluation and care of these patients as well as our understanding of the neural correlations of vigilance and consciousness.
Footnotes
Acknowledgments
The authors thank Pr. Maquet, head of the Sleep Group at the Cyclotron Research Center, for his collaboration. The authors also thank the doctors and nurses of the Centre Neurologique et de Réadaptation Fonctionnelle de Fraiture, the Centre Neurologique William Lennox, and the Neurology Departments of the Centre Hospitalier Universitaire of Liege for their participation in this study. The authors finally thank Mrs. Tina Duvivier for language revision.
This work was supported by the Belgian National Funds for Scientific Research (FNRS/FRIA).
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.