
Abstract
In patients with severe traumatic brain injury (TBI), a growth hormone deficiency (GHD) is frequent and may contribute to the cognitive sequelae and reduction in quality of life (QoL). Recent studies have suggested that GH replacement therapy (GHRT) can improve processing speed and memory. The aim of the study was to analyze the efficacy of GHRT on cognition, activities of daily living (ADL), and QoL and the factors that predicted and contributed to these effects. We included patients at least 1 year after their TBI and assessed pituitary functions (with stimulation tests), cognition (attention, memory, and executive function), participation in ADL and QoL. GHD was treated for at least 1 year in 23 patients, who were compared with 27 non-treated patients. Other deficiencies were also treated. Measurements were performed at baseline and 1 year later. An analysis of variance of the factors group and session (p≤0.05) showed that most cognitive parameters had improved at 1 year (evidencing a session effect). A stronger effect of GHRT (i.e. a group x session interaction) was found for Rey Osterrieth complex figure recall and 2/6 domains in the QoL questionnaire (“personal” and “functional”). Trends (p≤0.07) were also found for spatial orientation and immediate recall in the verbal memory test. Greatest improvements were associated with lower performance before treatment. The magnitude of the improvements in ADL and QoL was moderately correlated with the improvement in cognition. In conclusion, replacement therapy can improve cognition and QoL in patients with TBI who have GHD, especially in those with severe disabilities.
Introduction
T
Patients with anterior lesions to the pituitary gland (responsible for a growth hormone deficiency [GHD]) may show impairments in attention, concentration, visual and verbal memory, and executive function. 6 –9 Some persons also have physical problems, including weight gain and high fat mass. 10 These disorders make the patients less confident and can result in social isolation. All these various issues have implications for a patient's psychological well-being and QoL. 11 –13
In patients with TBI who have pituitary deficiencies, the somatotropic axis is most often affected—either alone or in combination with corticotropic, thyrotropic, and/or gonadotropic deficiencies. 14 –17 It has been suggested that GHD is related to cognitive difficulties, emotional disorders (including depressive symptoms), 17 –19 high dependence in ADL, and poor QoL. 17,20
Several studies have suggested that growth hormone replacement therapy (GHRT) improves cognition and QoL in patients in whom GHD is congenital or secondary to surgery, radiotherapy, inflammatory, or tumoral disease. 9,11,13,21 –25 In one study, the efficiency of GHRT was greater in patients with initial severe alteration of QoL. 26 An effect of growth hormone-releasing hormone (GH-RH) therapy has also been reported on cognition in healthy older adults and patients with mild cognitive impairment. 27 –29
The effects of GHRT in patients with TBI have been reported in studies with open-label designs or small numbers of subjects. Bhagia and associates 30 reported benefits for muscle strength and motor dexterity but no significant effect on cognitive performances in a patient who was treated with GH for 1 year. Another open-label study 31 described similar improvements in QoL after a year's GHRT among patients with TBI or non-functioning pituitary adenoma. In yet another open-label study 32 of six patients who were treated for 6 months, an improvement was described in the Zung Depression Inventory, psychiatric symptom-checklist, and cognitive functions (especially memory).
In a series of patients receiving both GHRT and cognitive rehabilitation, Reimunde and colleagues 33 reported an effect of treatment (relative to non-treated, non-GHD patients) at 3 months on verbal subtests of the Wechsler Adult Intelligence Scale. High and coworkers 34 treated patients with TBI 1 year with GH and compared them with patients with GHD who were receiving a placebo. Greater improvements were seen in the GH-treated group in finger tapping, a test of information processing speed, verbal learning, and the Wisconsin Card Sorting Test. A large number of test scores, however, were not influenced by therapy.
Taken as a whole, the results of the above-mentioned studies suggest that GHRT has a slight beneficial effect in patients with TBI. It is difficult to draw firm conclusions, however, because of the frequent absence of a control group. In addition, it is relatively difficult to compare patients with and without hormone deficiencies, because they are relatively inhomogeneous in a large number of other aspects.
The objective of the present study was therefore (1) to analyze the effect of GHRT on cognition, QoL, and participation in ADL in a relatively large group of patients with TBI who had GHD (relative to an untreated group) and (2) to identify predictors and explicative factors for any observed improvements. Our starting hypothesis was that the potential benefits on ADL and QoL would be relatively modest and related in part to the improvement in processing speed and cognition.
Methods
Patient inclusion and screening
Patients with TBI were recruited during follow-up consultations at the Neurological Rehabilitation Department at Lille University Medical Center and by community-based health care services.
The inclusion criteria were as follows: age between 18 and 60, at least 1 year since TBI, and the presence of cognitive and/or behavioral disorders (memory, attention, or concentration disorders, slowing, fatigability, lack of initiative and emotional lability, etc.) reported by the patient or their carer(s) or identified during a consultation. We excluded pregnant women, illiterate subjects, patients receiving corticosteroids, and those with a history of drug abuse, neurological disease, hypothalamus or pituitary disorders, or severe kidney, liver, or cardiovascular diseases. All patients (or their legal representative) provided written, informed consent to participation before involvement in study procedures. The study was performed in accordance with the Declaration of Helsinki and institutional guidelines.
During a medical consultation with a specialist, the patient's baseline parameters were recorded; these included age, educational level, the cause of the TBI (road accident, domestic accident, sports accident, assault, or attempted suicide), initial severity factors (the lowest Glasgow Coma Scale (GCS) score during the first 24 h post-injury and the length of stay in the rehabilitation ward), the time since TBI, and the MRI data recorded more than 3 months after the TBI (focal or multifocal parenchymal lesions, and/or diffuse axonal injury).
If the patient or his/her carer(s) reported the presence of cognitive difficulties, the attending physician suggested a consultation with an endocrinologist, who investigated the hormone profile. A general clinical examination was performed, and the body mass index (BMI) was calculated. The patients' main complaints were recorded, including the presence of asthenia, fatigue, cold intolerance, decreased libido, and amenorrhea.
The hormone profiling performed in our institution has been described previously. 17 The analysis of posterior pituitary function included a screen for the syndrome of inappropriate antidiuretic hormone hypersecretion (SIADH) and, in cases of polyuria and polydipsia, diabetes insipidus. Patients were also screened for hyperprolactinemia and deficiencies in the gonadotropic (GD), thyrotropic (TD) and corticotropic (CD) axes. GHD was diagnosed by using an insulin tolerance test (ITT) and/or an arginine-GH-RH assay 35 as reference tests. Severe GHD was defined as a GH peak below 3 ng/mL during the ITT or below 4.0 to 15.6 ng/mL in the arginine-GH-RH assay (depending on the patient's age and BMI). 36
According to the French guidelines, only one test was performed in patients with another pituitary deficit. In patients without any other deficit, a second test was performed and patients received a diagnosis of isolated GHD when results of the two tests were abnormal. Somatotropic function was considered to be unaffected if the response to the reference test was normal (GH>10 ng/mL in the ITT, and GH>the percentile 1 threshold values from Colao and colleagues. 37 in the arginine-GHRH test). In an intermediate situation, the GHD was classified as “partial.” Serum insulin-like growth factor 1 (IGF-1) levels were also measured.
In a group of 50 patients having undergone pituitary hormone screening and having agreed to participate in the cognitive function assessment, severe GHD was found in 28 cases, CD deficiency in 15 cases (always partial, with cortisol level >3 μg/dL), and TD deficiency in 15 cases. The TD was always the consequence of a hypothalamic-pituitary deficit. We did not find any case of diabetes insipidus.
GHRT was proposed to patients with severe GHD, after exclusion of the usual contraindications. This treatment was initiated in 23 cases (the treatment group). The control group comprised 27 patients who did not receive treatment because of (1) normal somatotropic function (n=15), (2) the presence of only partial GHD (n=9), or (3) contra-indications to or refusal of treatment in cases of severe GHD (n=3). The two groups were similar in terms of age, sex, educational level, the severity of the initial TBI (i.e., the GCS score), and the time since TBI (Table 1). The time since TBI was relatively long (mean: 7.8 years in the treatment group and 5.5 years in the control group). Current participation in ADL, anxiety, and depression (see patient assessment) and the presence of epilepsy (three and four patients from the treatment and control groups, respectively) were also comparable before treatment and at the 1-year follow-up. In the treatment group, 5 patients also had TD, 11 had partial CD, and two had hyperprolactinemia; the corresponding numbers of patients in the control group were respectively five, three, and zero.
Parameters are quoted as the mean (standard deviation).
TBI, traumatic brain injury; IGF-1, insulin-like growth factor.
Protocol for GHRT
All hormone deficiencies were treated (with the exception of partial GHD, in line with current French guidelines). GHRT was initiated after adequate correction of the TD and CD deficits. The initial dose was 0.3 mg per day (Nutropin®, Genentech Inc., US) and titrated progressively to 0.2 to 0.6 mg per day, depending on the IGF-1 level. The objective was to obtain an IGF-1 plasma level between 0 and +2 standard deviations (SD) of the normal range for age. At the end of the study, the dose per day was 0.2 mg in 4 patients, 0.3 mg in 11, 0.4 mg in 3, 0.5 mg in 4, and 0.6 mg in 1. The IGF-1 level significantly improved (p=0.0001) from the pre-treatment dosage (m=163.2, SD=62.9) to the 1-year control (m=261.7, SD=71.9)
Patient assessment
Patients were first assessed immediately before treatment initiation and then after 1 year of treatment. At the latter assessment, all the patients in the treatment group were still receiving somatotropin.
Attentional function was evaluated using the phasic alertness reaction time (RT), selective attention RT and flexibility subtests of Zimmerman's computerized Test for Attentional Performance (TAP) test. 38 A 2-minute verbal semantic and phonemic fluency test was used to evaluate executive functioning. Orientation in space and time were measured by asking the patient to give the exact date (score out of 5: day of the week, date, month, year, and season), and current location (score out of 4: floor, building, town, and country). Short-term verbal memory and working memory were evaluated with the forward and backward digit span tests. Verbal episodic memory was evaluated with immediate information encoding, free recall (R-3), recognition, and delayed recall (2 min) in a 16-word test. 39
Visuospatial abilities (copying) and the visuospatial episodic memory (recall) were evaluated with the Rey Osterrieth Complex Figure Test (score out of 36). 40 Cognitive and behavioral disorders were assessed on the Neurobehavioral Rating Scale-Revised (NRS-R), 41 which scores 29 items from 1 (the absence of alteration) to 4 (severe alteration). This scale evaluates memory disorders (score out of 32), motivated behavior, and emotional hypoactivation (score out of 12), anxiety and emotional and behavioral hyperactivation (score out of 32), reduced alertness (score out of 16), and language disorders (score out of 12).
Anxiety (0-1), depression (0-1), and the independence in personal and instrumental activities of daily living (pADL and iADL, respectively) was analyzed according to the European Brain Injury Society guidelines (from 0, full participation, to 18, no participation). 42
Health-related QoL was assessed with the Quality of Life after Brain Injury (QOLBI) questionnaire. 43 The 35 items concern six domains: physical, intellectual, psychological, functional, social, and personal. Each item was scored from 1 (not at all satisfied) to 10 (very satisfied). We calculated the mean score for each domain and the total score.
Statistical analyses
All statistical analyses were performed with SPSS software (version 16.0, SPSS Inc., Chicago, IL) software. We used repeated-measures analysis of variances with group (treatment or control) as the between-subject factor and session (session 1 or session 2) as the within-subject factor to analyze the effect of GHRT on each of the cognitive, behavioral, ADL, and QoL parameters. The Pearson test and the chi-square test were used to test relationships between quantitative or qualitative variables, respectively. We also performed multivariate analyses (with stepwise variable selection) to identify the best independent predictors of any observed improvements. The threshold for statistical significance was set to p≤0.05.
Results
The effect of GHRT on cognition, QoL, and participation in ADL
Cognitive functions were often found to have significantly improved (p≤0.05) or showed a trend toward a significant improvement (0.05<p≤0.07) at the second session (an effect of session). This was especially the case for attention (phasic alertness RT, selective attention RT, and flexibility RT), memory (immediate verbal recall and delayed recall), and visuospatial abilities (Rey Osterrieth complex figure copy score and time) (Table 2) (Fig. 1, 2). Improvement was also found in terms of participation in iADL, four QOLBI domains (intellectual, psychological, functional, and personal), and the total QOLBI score. However, a significant group×session interaction (suggesting a stronger effect of GHRT) was only found for the Rey Osterrieth complex figure (recall time) and the QOLBI functional and personal domains. Trends toward a significant improvement were observed (0.05<p≤0.07) for orientation in space, immediate verbal memory, and the BMI.
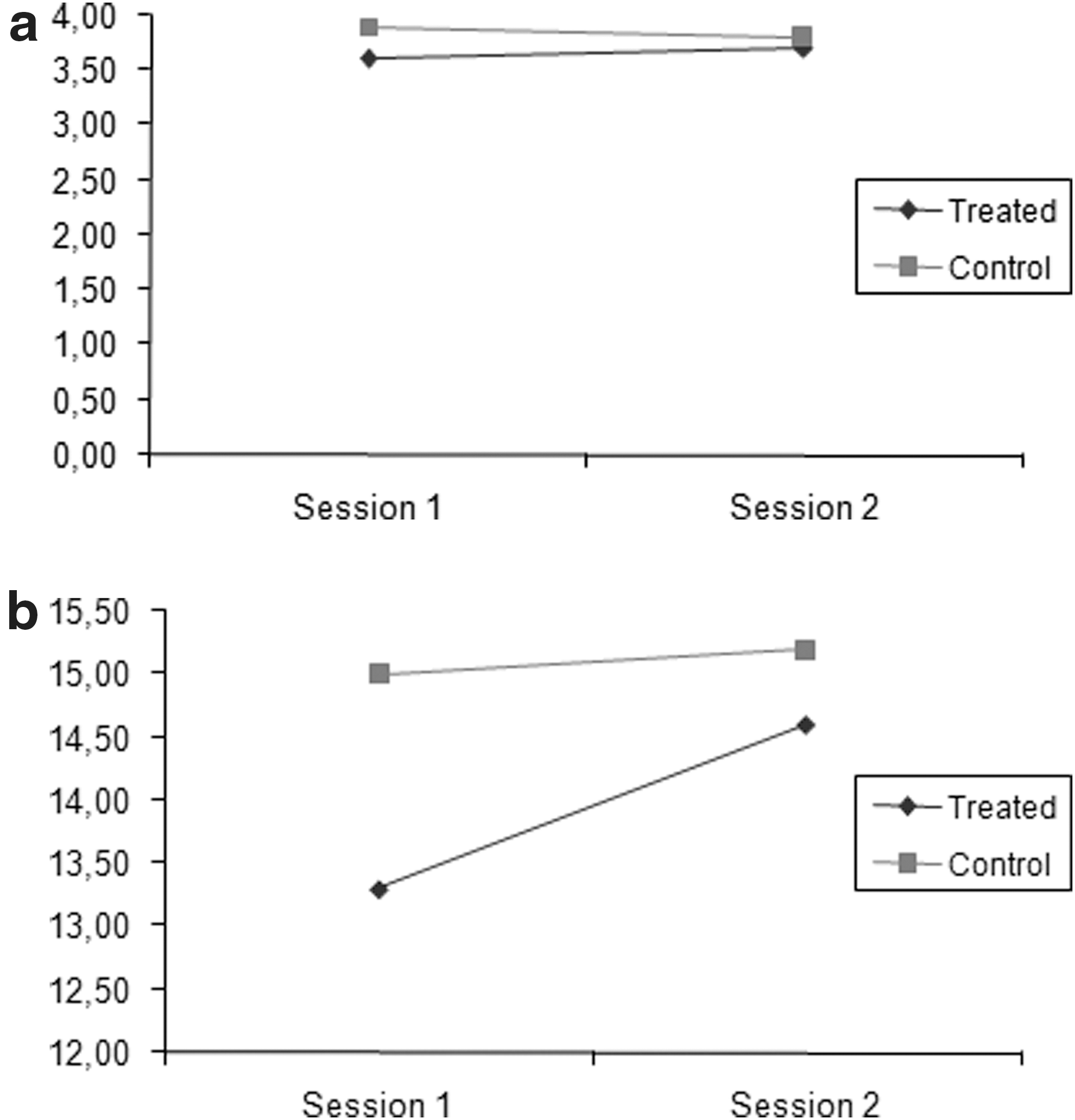
Change over time in the orientation in place (

Evolution in the functional (
The significance of the session effect and the group×session interaction are quoted.
RT, reaction time; NRS, Neurobehavioural Rating Scale; BMI, body mass index; pADL, personal activities of daily living; iADL, instrumental activities of daily living; QOLBI, quality of life after brain injury.
All the patients in the treatment group asked to continue GHRT at the end of the study.
Predictive factors for improvement in treated patients
In the GH-treated group, we analyzed the relationships between the change over time (performance in session 2–performance in session 1) in the cognitive, ADL, and QoL parameters that were significantly improved by treatment, and general factors (age, sex, and educational level), indices of TBI severity (the GCS score and presence of lesions on MRI), the time since TBI and pre-treatment (baseline) BMI, IGF-1 level, cognitive performance, presence of depression, participation in ADL, and QoL.
There was no significant association (according to Pearson correlation tests and chi-square tests) between parameters significantly improved by GHRT and general factors, GSC score, time since TBI, baseline BMI and IGF-1 level, and presence of depression. Multi-focal lesions and diffuse axonal injury were associated (Table 3) with less improvement in immediate recall in verbal memory and a trend toward a significant effect of multifocal lesions was also found for personal QoL. Concerning orientation in space, verbal memory immediate recall, QOLBI functional and personal domains, the improvement was significantly and negatively correlated with the respective pre-treatment value (Table 3). Improvement in the QOLBI functional domain was also significantly and negatively correlated with the verbal memory performance at the first session.
: 0.01<p≤0.05
: 0.001<p≤0.01
: p≤0.001
pADL, personal activities of daily living; iADL, instrumental activities of daily living; QOL, quality of life; MRI=magnetic resonance imaging;
BMI, body mass index; IGF-1, insulin-like growth factor; RT, reaction time.
We then performed a multivariate analysis (with forward stepwise variable selection: F-to-enter=0.05) to identify the variables that best explained the treatment-related improvement in ADL and QoL. In fact, the improvement was principally explained by the pre-treatment value of the variable in question.
Explicative factors for improvement in treated patients
In the treatment group, we investigated the relationships of the improvements in participation in ADL and QoL on one hand with the improvements in BMI, cognitive tests, and ADL on the other. The improvements in QoL and ADL correlated moderately with the improvements in the different cognitive domains (Table 4) in general and attention and memory in particular. The improvement in total QoL also correlated with the improvement in the pADL. Conversely, the improvements in ADL and QoL were not associated with changes in BMI and IGF-1 level.
0.01<p≤0.05
0.001<p≤0.01
p≤0.001
pADL, personal activities of daily living; iADL, instrumental activities of daily living; QoL, quality of life BMI, body mass index; IGF-1, insulin-like growth factor; RT, reaction time.
Discussion
Our study of 50 patients with TBI (of whom 23 were treated for GHD) showed that (1) GHRT had a moderate effect on the speed of information processing and memory but did not noticeably modify attention, executive function, language, and behavioral disorders; (2) GHRT was more clearly effective on sub-components of health-related QoL; (3) the patients with the greatest improvements were those who had the most severe difficulties before treatment: and (4) improvements in QoL and ADL were related (at least in part) to the improvements in cognitive functions.
The effect of GHRT on speed of information processing and memory could be related to an effect of IGF-I and/or GH on brain structures involved in these functions, which are known to be commonly affected by TBI. These structures include hippocampal and para-hippocampal areas, the thalamus, the basal forebrain, and the frontal lobe. In animals, IGF-1 receptors are present in hippocampal and para-hippocampal structures and in the frontal neocortex. 44 Further, IGF-1 increases hippocampal cell proliferation. GH receptors are present in the choroid plexus, thalamus, hypothalamus, pituitary, putamen, hippocampus, amygdaloid nucleus, and prefrontal cortex 8,45 and may affect the development of neural cells. 46 In addition, GH treatment modulates brain neurotransmitters (especially dopamine). 47 This might explain (at least in part) the observed functional improvements, 48 because high levels of dopamine are found in the hippocampus and low GH levels impair dopamine turnover.
The cognitive functions that appeared to best respond to GHRT were the speed of information processing and memory, although the magnitude of the benefit was relatively modest. The effect on the speed of information processing was evidenced by the time for the memory subtest of the Rey Osterrieth complex figure but not by the simple RT data. This effect has also been observed in patients with GHD patients who had TBI 34 and non-TBI 49 etiologies. We found more marked effects of GHRT on immediate memory for verbal information (a measure of the encoding process).
A moderate effect on memory processes has been reported in two studies with similar patient populations. The first one 34 showed a moderate improvement in the California Verbal Learning Test score (memorization of a word list: trial 1–5 learning) and the second one 32 in a serial verbal memory test, which disappeared after treatment discontinuation. In patients with GHD and non-TBI etiologies, the effect of GHRT has yielded diverging results 9,50 ; some studies have shown a moderate effect on immediate and long-term verbal and/or spatial memories, 51,52 whereas others have failed to see any effect at all. 53,54 The sensitivity of memory processes to GH-RH, which stimulates GH release from the pituitary, has also been reported in patients with neurodegenerative disorders and mild cognitive impairment. 28,29
We did not observe any improvement of digit span and short-term memory and thus confirmed previous observations in this respect. 33,34 Neither did we find any changes attributable to GHRT for attention and executive functions. In similar patients, High and coworkers 34 reported a modest effect on the Wisconsin Card Sorting Test. Results in patients with non-TBI etiologies have been contradictory, however, with a benefit in one series, 23 that was not confirmed by other authors, 53 and a positive effect in a meta-analysis, 9 but not in another. 54 Further, we did not observe any significant effects on language, behavior, and mood in the NRS-R. A progressive effect on mood (especially anxiety, tension, and vigor) has been reported in patients with GHD who have non-TBI etiologies. 48
In our series, the effect of GHRT was more marked when considering the health-related QoL in general and its personal and functional domains in particular. Personal items are related to acceptation, independence, religious feelings, and projects. The functional component is related to pADL and iADL. Conversely, there was no specific effect of GHRT on the other QoL components, including physical, intellectual, and psychological difficulties and social relationships. It is well established that patients with TBI have from poor QoL. A number of promoting factors have been suggested and include especially the initial TBI severity, previous intellectual difficulties (such as a low intellectual quotient), personality disorders, young age, female sex, and TBI-related disability. 55 Poor QoL has also been documented in patients with GHD who have non-TBI etiologies 22,56 and may be more marked in elderly patients, women, and persons with low IGF-1 levels or taking antidepressants. 22
An effect of GHRT on the QoL (according to the Assessment of Growth Hormone Deficiency in Adults [AGHDA]) has been reported in a previous study of patients with TBI. 28 Although the AGHDA is specific to GHD (which is an advantage), the tool is unidimensional and does not distinguish between the different domains of health-related QoL, which are better explored with a TBI-specific QoL questionnaire.
Here, we observed that at least five domains of QoL were improved at the follow-up examination (i.e., an effect of session), but two domains only showed the significant group×session interaction that indicated greater improvement in treated patients. The efficacy of GHRT on QoL has been reported in patients with non-TBI etiologies, 12,57 although most such studies used the AGHDA questionnaire. 11,13 An effect has also been described on the Psychological General Well-Being Index, which provides more specific measures of anxiety, mood, well-being, self-control, general health, and vitality. 16
The mechanisms of the effect on QoL remain subject to debate. 58 Treatment with GH has general physical effects; for example, it improves the ability to perform physical exercise and decreases body fat, especially in younger patients. 59 Long-term treatment with GH increases muscle strength 60 and intermediary metabolism. In our study, we found a significant effect of GHRT on BMI, but we did not find any direct relationships between the improvements in QoL and the change over time in BMI; neither did we observe any correlation with the increase in serum IGF-1 level, confirming the observations of other researchers. 22 An effect of GH on the brain and cognition (especially memory) is another possible mechanism of action. An argument in favor of this mechanism is the presence of correlations between the improvements in ADL and QoL on one hand and the improvements in attention and memory on the other.
We also analyzed predictors of the improvements seen in our patients. The benefits in the various domains of cognition and in QoL were primarily predicted by the respective parameters' baseline (i.e., pre-treatment) values. In fact, the patients with the most severe initial difficulties showed the greatest improvements, as observed in studies of patients with GHD who had non-TBI etiologies. 58,61 Conversely, we did not find any effect of general factors, including age, the severity of the initial status, and the time since brain injury in the present study.
Several points need discussion, because they could be considered as limitations of the study. Many of our patients from both groups were treated for neuroendocrine deficiencies other than GHD (including steroid hormone deficiencies). Steroid hormones can also influence memory. 62 Many patients from the control group also presented a steroid hormone deficiency, however, which was always treated. Further, it has been shown that in patients with non-TBI etiologies, the effects of GHRT on cognitive function 63 and QoL-AGHDA 13 were similar in those with isolated GHD and those with multiple endocrine deficiencies.
A second point was in the selection of patients participating in the control group. In fact, there are at least three selection criteria for building the control group, as regards the presence/absence of endocrine deficits: (1) patients without endocrinopathy, (2) patients with endocrinopathy and GHD, but without GHD treatment, 34 and (3) patients with possible endocrinopathy, but without GHD. 33 Here, the selection criterion was intermediary between the second and the third possibilities: severe GHD was rare, and many patients presented with partial GHD or no GHD. A main point for patient equivalence, however, is to the severity of cognitive difficulties and QoL reduction, and this severity was relatively comparable in the two groups.
A third point was that the latency between TBI and GH replacement was long. At that time, it can be proposed that the effect of interventions is more difficult to arise. If an improvement is shown during a therapy, however, it more likely results from this therapy and not from the spontaneous evolution. In addition, we did not find any relationship between the improvement and time since TBI.
Conclusion
GH deficiency is a frequent consequence of TBI. GHRT appears to produce (1) a moderate improvement in processing speed and memory capacities and (2) a more marked increase in QoL. We suggest that GHRT should be considered for TBI patients with severe GHD (in compliance with the usual contraindications, of course) and especially for those with more severe cognitive or social difficulties.
Footnotes
Author Disclosure Statement
No competing financial interests exist.