
Abstract
Adequate nutritional support is a major challenge in brain injury patients, because malnutrition cannot be reversed by standard enteral nutrition. We hypothesized that an oligomeric formula could improve nutritional status by restoring intestinal trophicity. Eighteen male Sprague-Dawley rats (300–330 g) underwent gastrostomy on day −7 (D-7) and traumatic brain injury (TBI) by hydraulic percussion (D0) and were then fed for 4 days with either a polymeric formula (Sondalis® HP, TBIP, n=9), or an oligomeric formula (Peptamen® HN, TBIO, n=9). In addition, a control group of healthy gastrostomized rats was fed the polymeric diet (control, n=8). All rats were weighed daily. On D+4, the rats were euthanized. Blood was collected for plasma amino acid determination. Organs were removed and weighed. Intestinal morphometry was studied. Protein content was assessed on intestine and muscles. Enterobacterial translocation and dissemination were evaluated. Results were expressed as means±SEM and compared using analysis of variance+Newman-Keuls test. TBI induced a significant decrease in whole body weight (TBIP vs. control, p<0.05) that was totally blunted by the oligomeric diet (TBIP vs. TBIO, p<0.01). Thymus weight significantly decreased after TBI (TBIP vs. control, p<0.05) and was restored by the oligomeric formula (TBIO vs. TBIP, p<0.05). Glutamine (GLN) concentration was improved by the oligomeric diet in both plasma (TBIO: 688±19 vs. control: 591±45 and TBIP: 615±42 μmol/L, p<0.05) and soleus muscle. These results show that the use of an oligomeric diet may limit response to injury after brain injury and could be a simple nutritional strategy in this setting.
Introduction
B
The consensus is, however, that standard products for enteral nutrition lack efficacy in this setting, 3 making it vital to develop new nutritional strategies to cover TBI patient-specific nutritional requirements. We previously showed 4,5 that so-called immune-enhancing diets can improve immunological function in brain injury, but these formulas had few if any effects on nutritional status, which is essential to improve clinical outcome in these patients. There are several potential explanations for this lack of effect, one of which could be the intestinal failure that occurs after TBI; our team 3 and others 6 –8 have demonstrated that TBI induces specific damage of the gut structure and impaired intestinal function. Given this hypothesis, it seems relevant to propose a nutritional strategy aimed at restoring intestinal trophicity and thereby improving nutritional status.
Previous studies have shown that feeding injured patients with an oligomeric enteral formula offers several advantages over a polymeric diet, including improved nutritional status, limited protein catabolism, and increased nitrogen absorption. 9,10 Furthermore, higher peripheral bioavailability of amino acids has been observed in surgical patients fed an oligomeric diet compared with a polymeric diet. 11 This effect was attributed to better intestinal digestion of peptides compared with proteins and easier absorption of di- and tripeptides compared with higher molecular weight peptides, thereby stimulating protein synthesis and limiting catabolism. More recently, length of hospital stay was shorter and weight loss was lower in patients with acute pancreatitis who were fed an oligomeric diet compared with a polymeric diet. 12 These data are consistent with those obtained in experimental studies: malnourished rats fed an oligopeptide-containing diet showed better growth and nitrogen balance compared with those fed a whole protein-containing diet. 13,14
Based on the hypothesis that higher peptide absorption (with respect to proteins) improves amino acid bioavailability for protein synthesis, the present study was performed to evaluate the efficacy of a peptide-containing enteral formula (Peptamen®HN, Nestlé Clinical Nutrition [NCN]) to improve intestinal trophicity and nutritional status in rats with TBI.
Methods
Animal care complied with French regulations on the protection of animals used for experimental and other scientific purposes (D 2001-486), and with European Community regulations (Official Journal of the European Community L538 12:18:1986). Our team has French government authorization to use animal models of stress and to perform surgery on rats (Christophe Moinard, authorization #75.522, Christine Charrueau, authorization #75.456).
Animals and study design (Fig. 1)
Twenty-six male Sprague-Dawley rats (body weight 300–330 g; Charles River, L'Arbresle, France) were acclimatized in metabolic cages for 1 week before surgery (from D-14 to D-7) in a controlled-temperature environment (21±2°C) with a 12-h light-dark cycle. The rats had free access to standard laboratory chow (17% protein, 3% fat, 59% carbohydrate, 21% water, vitamins and minerals; A04, Safe, Augy, France) and water. The rats were then randomized into one of the following three groups: • Healthy gastrostomized rats fed a standard polymeric enteral nutrition (SEN) (=Sondalis® HP, NCN, control group, n=8) • TBI rats fed the polymeric diet (=Sondalis® HP, traumatic brain injury polymeric [TBIP] group, n=9) • TBI rats fed the oligomeric diet (=Peptamen® HN, NCN, traumatic brain injury oligomeric [TBIO] group, n=9).
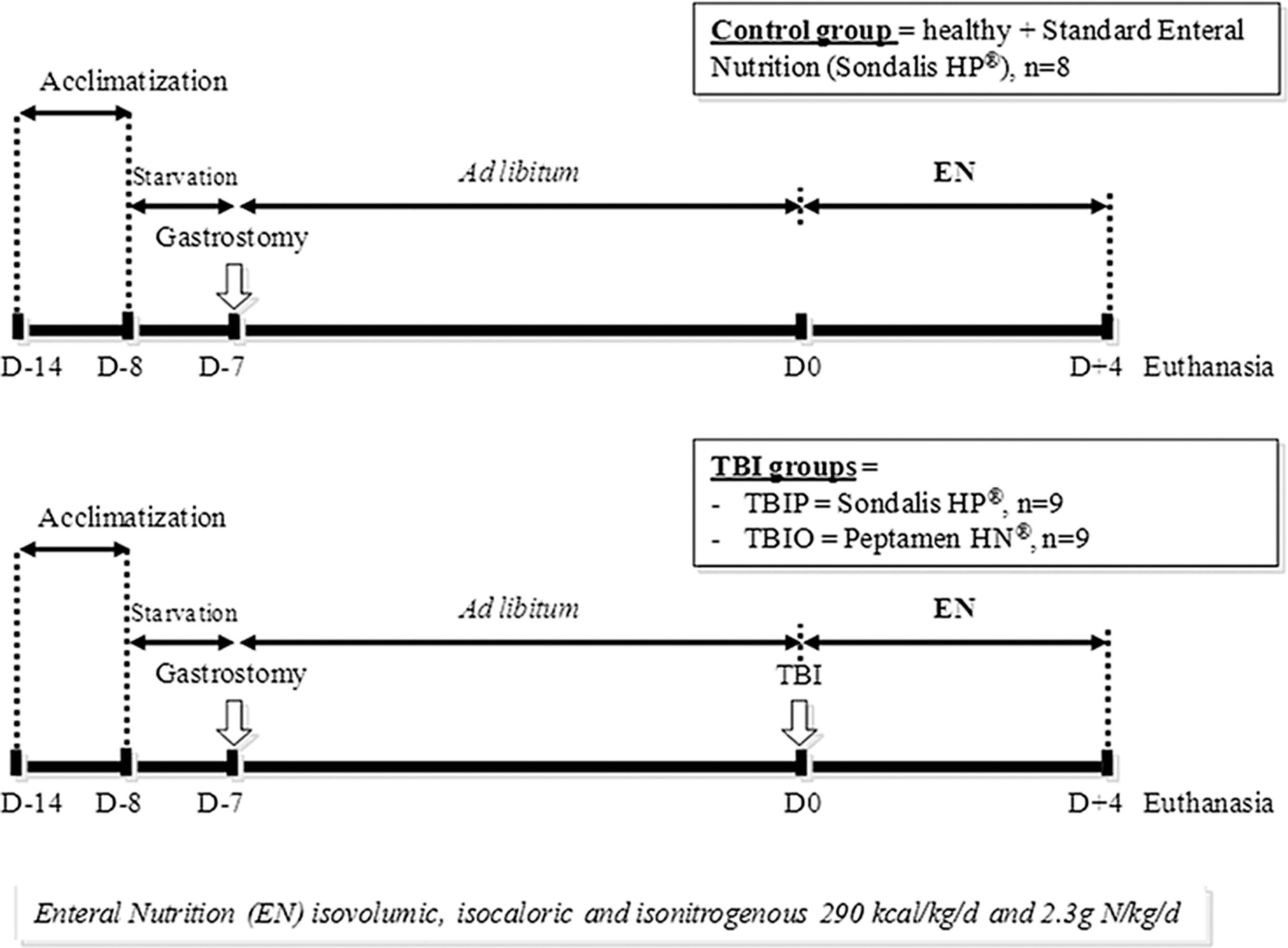
Experimental design. TBI, traumatic brain injury; TBIP, traumatic brain injury+ polymeric diet; TBIO, traumatic brain injury+ oligomeric diet.
Surgical procedure for enteral nutrition (D-7)
Gastrostomy was performed on day D-7 (Fig. 1) as described previously. 5 After fasting for 12 h before surgery, the animals were anesthetized by isoflurane inhalation (3% isoflurane) using a regulated airflow apparatus (Minerve, Esternay, France) before receiving a single subcutaneous injection of analgesic (0.05 mg/kg Temgesic®; Schering-Plough, Levallois-Perret, France). Abdominal and neck areas were shaved, and the skin was carefully cleaned with polyvidone iodine (Betadine,® Sarget Laboratory, Merignac, France). During surgery, the animals were maintained anesthetized by continuous isoflurane inhalation (1.5% isoflurane).
Briefly, a silicone tube (Tygon, size 0.51 mm; Fisher Bioblock Scientific, Illkirch, France) was introduced into the stomach lumen and secured with a purse-string suture, and the remaining end of the catheter was tunnelled subcutaneously to the back of the neck and attached to a spring coil-swivel mechanism (Harvard Apparatus, Les Ulis, France) allowing the rat to move freely in the cage. A polyethylene tube (Fisher Bioblock Scientific, Illkirch, France) connected the cannula to a push-syringe (model 1140-101, Harvard Apparatus). The rats were housed individually in metabolic cages and allowed a 7-day recovery period. They were given free access to standard laboratory chow (A04) and water.
Traumatic brain injury (D0)
At 7 days post-gastrostomy (D0), the rats were anesthetized with chloral hydrate (400 mg/kg, i.p.; Prolabo, Fontenay-sous-Bois, France) and placed on a stereotaxic frame. Chloral hydrate was used instead of isoflurane for technical reasons—i.e. the impossibility of managing the stereotaxic material together with the anesthesia machine. We previously demonstrated that chloral hydrate anesthetic did not influence the parameters measured. 15
During surgery, animals were positioned on a heating blanket (Harvard, Holliston, UK) to maintain body normothermia (37.5±0.5°C). TBI was induced by fluid percussion using the protocol described elsewhere. 15 Briefly, the scalp was incised, and a 3 mm craniotomy was made to the right temporoparietal cortex using a dental drill. A 3 mm polyethylene tube was placed over the dura mater, fixed securely into the craniotomy site with dental cement (Paladur, Hanau, Germany), and connected to a solenoid valve (Danfoss, Nordborg, Denmark). The opposite end of the valve was connected to an HPLC pump (Gilson, France). The system was filled with sterile water, providing a calibrated outflow pressure of 1.6–1.8 bar. A solenoid valve opening for 20 ms and controlled with a timer (Omron, Kyoto, Japan) triggered the percussion directly onto the dura mater. The applied cortical pressure was measured extracranially by a pressure transducer (Emka Technologies, Paris, France) connected to an oscilloscope (DSO 400, Gould, France). Immediately after fluid percussion, the tube was removed, the scalp sutured, and animals were placed at 26–28°C to recover from the anesthesia.
Postoperative care and nutrition program
On day D0, 4 hours after TBI, the enteral nutrition was introduced at a flow rate of 0.5 mL/h. The rats also had free access to water. The enteral nutrition flow rate was then gradually increased to a maximum on day D+1 corresponding to an intake of 290 kcal/kg/d as previously described. 3 From D+1 until the end of the experiment (D+4), the rats received enteral nutrition 24h/24h at a constant rate providing 2.3 g N/kg/d. Diet composition is given in Table 1.
Animal care and sample processing
The rats were weighed daily.
Neurological function
A neurological examination was performed blind before euthanasia, using a grading scale (Table 2) as described previously. 5
Four days after TBI, nutrition was stopped, and 2-h later, all the rats were anesthetized with isoflurane and euthanized by beheading. The 4-day end-point was chosen based on previous studies 3 –5,15 showing that the hypercatabolic state induced by TBI peaks at D+2 and persists until D+4.
Procedures and analytical methods
Blood collection and tissue removal
Blood was collected on sodium heparinate. Jejunum, ileum, extensor digitorum longus (EDL), soleus, tibialis, gastrocnemius, spleen, and thymus were removed and weighed as previously described. 15 Jejunum and ileum samples were prepared according to the “Swiss-roll” method. 16 Mesenteric lymph nodes, liver, spleen, lung, kidney, and cecal content samples were removed under aseptic conditions for microbiological analysis, as described previously. 15,17
Amino acid concentrations in plasma and muscles
Plasma concentrations and muscle contents of all amino acids were determined by ion-exchange chromatography as described previously. 18
Tissue protein content
Total protein content in intestine and muscles was determined as described previously. 15
Intestinal morphometry
The Swiss-roll intestine samples were embedded in paraffin, and 5 μm sections were taken and stained with hematoxylin and eosin. The height of the 5 longest villi of each sample and their corresponding crypts were measured using a microscope with a computer and a monitor connected to a color video camera mounted on top of the microscope. 16
Enterobacterial translocation and dissemination
After removal in aseptic conditions, the mesenteric lymph nodes, liver, spleen, lung, kidney, and cecal content were weighed and homogenized in a brain heart infusion+glycerol medium (0.5 mL) using an Ultra-Turrax T25® homogenizer (Ika Labotechnik, Staufer, Germany). Fifty μL of organ homogenates were plated on a Drigalski medium (selective medium for isolation of enterobacteria) and incubated for 48 h at 37°C. Colonies were enumerated and the results were expressed in log10 (colony-forming units)/g of organ or cecal content.
Statistical analysis
Data were expressed as means±standard error of the mean. Datasets were compared using one-way analysis of variance (ANOVA) followed by the Newman-Keuls test (Statview software, Abacus Concepts, Berkeley, CA). Body weight was analyzed by ANOVA on repeated measurements. Neurological score was analyzed by a Kruskal-Wallis+Mann-Whitney test. Enterobacterial translocation and dissemination were analyzed by a Kruskal-Wallis test. Glutamine (GLN) in plasma and muscles was analyzed by ANOVA plus a Duncan test. Differences at p<0.05 were considered significant.
Results
Neurological function
Neurological score significantly deteriorated in the two TBI groups, without significant difference between groups (TBIP and TBIO vs. control, p<0.05) (data not shown).
Body and organ weights (Fig. 2, Table 3)
TBI induced a significant decrease in whole body weight (TBIP vs. control, p<0.05) that was totally blunted by the oligomeric diet (TBIP vs. TBIO, p<0.01). Concerning muscle weight, EDL, tibialis, and gastrocnemius were not modified whatever the group considered, whereas the effect of TBI on soleus weight did not reach significance (TBIP and TBIO vs. control, p=0.08). Intestinal mucosa weight was similar in the three groups. Thymus weight significantly decreased after TBI (TBIP vs. control, p<0.05) and was restored by the oligomeric formula (TBIO vs. TBIP, p<0.05).
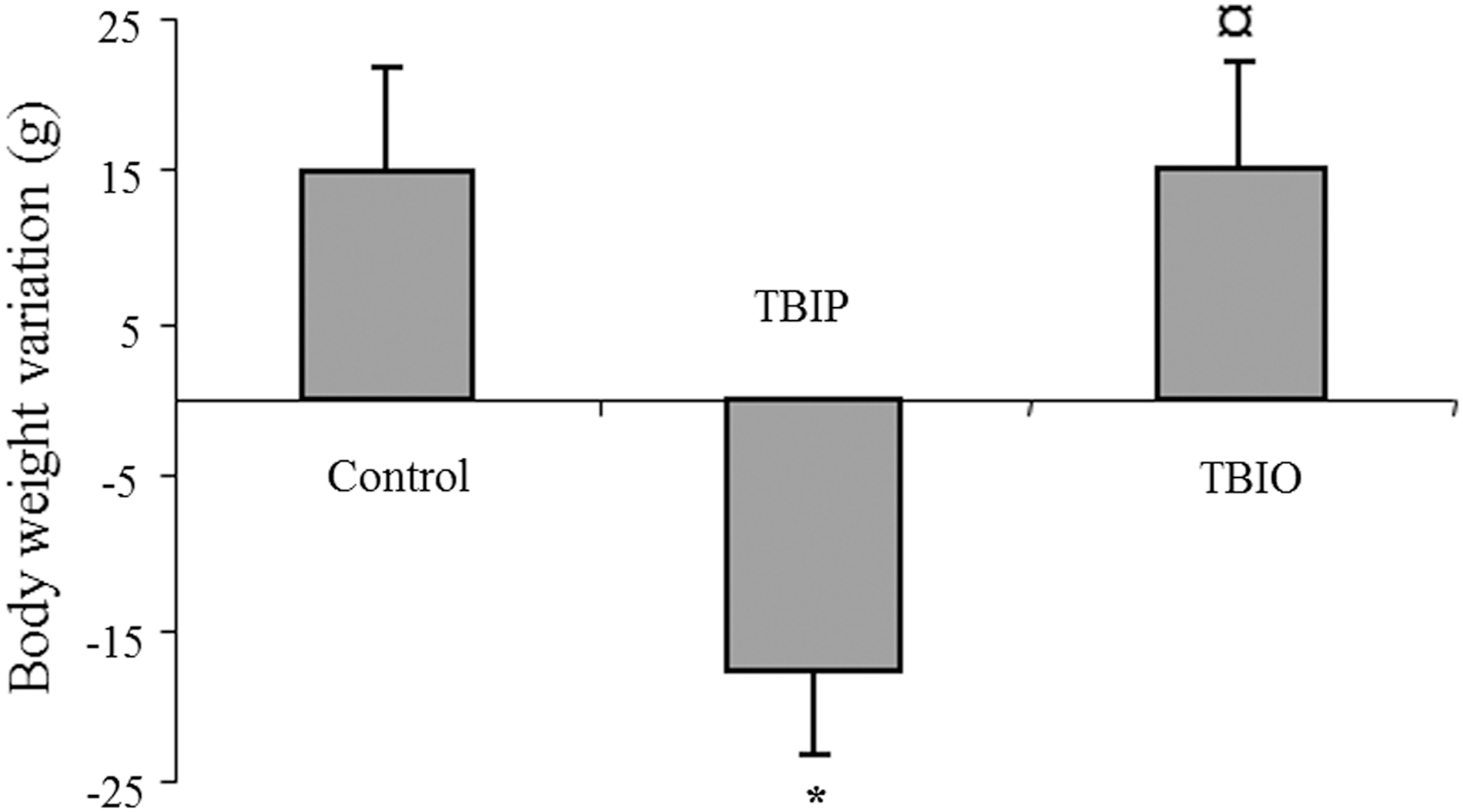
Body weight variation between day 0 and day 4. Variation in total body weight in control rats, traumatic brain injury+standard polymeric diet rats (TBIP), and traumatic brain injury+oligomeric diet rats (TBIO). Results are given as means±standard error of the mean (analysis of variance+Newman-Keuls test). *p<0.05 vs. control; ¤ p<0.05 vs. TBIP.
Weight of jejunum, ileum, extensor digitorum longus (EDL), soleus, tibialis, gastrocnemius, spleen, and thymus in control rats, traumatic brain injury+standard polymeric diet rats (TBIP), and traumatic brain injury+oligomeric diet rats (TBIO).
Results are given as means±standard error of the mean (analysis of variance+Newman-Keuls test).* p<0.05 vs. control; † p<0.05 vs. TBIP.
Tissue protein content (Table 4)
Tissue protein content was not significantly affected whatever the group considered. Jejunum protein content, however, was ≈30% higher in the TBIO group compared with the other groups.
Protein content of jejunum, ileum, extensor digitorum longus (EDL) and soleus, in control rats, traumatic brain injury+standard polymeric diet rats (TBIP), and traumatic brain injury+oligomeric diet rats (TBIO). Results are given as means±standard error of the mean (analysis of variance+Newman-Keuls test).
Amino acid concentrations in plasma and muscles (Table 5)
There were no significant differences between groups for almost all plasma and muscle amino acid concentrations (data not shown) except for GLN concentration, which was improved by the oligomeric diet in both plasma (control and TBIP vs. TBIO, p <0.05) and Soleus (control and TBIP vs. TBIO, p<0.05).
Glutamine concentration in plasma and in soleus muscle in control rats, traumatic brain injury+standard polymeric diet rats (TBIP), and traumatic brain injury+oligomeric diet rats (TBIO). Results are given as means±standard error of the mean (analysis of variance+Newman-Keuls test). * p<0.05 vs. control and TBIP.
Intestinal morphometry (Table 6)
No variation in intestinal morphometry was observed whatever the group considered.
Intestinal morphometry (villus height and crypt depth) in jejunum and ileum in control rats, traumatic brain injury+standard polymeric diet rats (TBIP), and traumatic brain injury+oligomeric diet rats (TBIO). Results are given as means±standard error of the mean (analysis of variance+Newman-Keuls test).
Enterobacterial translocation and dissemination (Table 7)
TBI induced enterobacterial translocation in the mesenteric lymph nodes and dissemination in the spleen and liver of TBI group rats (TBIP and TBIO) without influence of the enteral diet.
Enterobacteria content in the mesenteric lymph nodes, liver, spleen, lung, kidney, and cecal content in control rats, traumatic brain injury+standard polymeric diet rats (TBIP), and traumatic brain injury+oligomeric diet rats (TBIO). Results are given as the median (min:max) in log (colony-forming units)/g of organ or cecal content (Kruskall-Wallis test).
Discussion
TBI is recognized as one of the most severe injuries encountered in intensive care units (ICUs), and the TBI-induced hypercatabolic state can persist for several weeks post-injury. 19 Adequate nutritional support for these patients is vitally important, especially to preserve gastrointestinal function and nutritional status. 20 This situation makes the treatment of patients with TBI a real challenge, because malnutrition cannot be reversed by standard enteral nutrition. 3 It is therefore important to determine the most appropriate nutritional care for improving outcome in patients with TBI. Brain injury may be an indication for immune-enhancing diets (IEDs), which have shown their potential to limit infection, 21 but their effect on nutritional status has been little explored. Our previous work found that IED nutrition was able to limit immune dysfunction after TBI, 4,5 but the effect on nutritional status was very limited. 22 Hence, it remains vital to propose new nutritional strategies to preserve nutritional status and improve outcome in patients with TBI.
We based our rationale on two points: first, several studies have underlined the major impact of TBI on the splanchnic area 3,7,8,15 that may compromise intestinal absorption and contribute to persistent malnutrition; second, oligomeric diets (containing a majority of small–to-intermediate tri-peptides instead of proteins) could have a positive effect on the splanchnic area and thereby enable improved nutritional status. In line with this hypothesis, our results confirm the benefit of such an approach: the oligomeric diet was able to totally blunt TBI-related body weight.
On one hand, we can assert that the body weight preservation observed in the TBIO group was not related to water retention, because diuresis was similar in all groups (data not shown). Further, the increase in thymus weight was not sufficient to explain the preserved body weight. On the other hand, there was no change in the weight of the four muscles evaluated, suggesting an unchanged fat-free mass. Note, however, that hindlimb muscle mass per se is not necessarily a direct marker of lean body mass. Finally, the determination of body composition would help determine which compartment is expanded by the oligomeric diet.
The body weight preservation was associated with an increase in GLN stores at whole-body level. Because low plasma GLN levels are associated with a worsened prognosis in ICU patients, 23 better GLN pools may reflect a better health status in rats with TBI fed the oligomeric diet. These observations prompt two questions. First: could such an effect be attributed to a preservation of gut trophicity? The oligomeric diet clearly failed to improve intestinal morphometry, because neither intestinal weight (nor protein content) nor ultrastructure (i.e., villus height and crypt depth) were improved in the TBIO group. Second: despite the lack of change in intestinal morphometry, was there any effect on barrier function? The answer is no, because bacterial translocation and dissemination were similar in both TBI groups.
The explanation for the beneficial effects observed in our study may reside in a more efficient absorption of peptides than whole proteins by the intestinal brush border membrane, as previously shown. 24 Despite intestinal alterations, this better absorption could be related to preserved hydrolytic capacities of the gut toward small peptides and/or direct absorption of di- and tripeptides without digestion. This kind of approach has already demonstrated its interest. Part of our team 11 has observed in abdominal surgery patients that peripheral bioavailability of amino acids was higher when patients were fed with oligopeptides rather than whole proteins. Moreover, the same authors demonstrated that oligopeptides were more efficient at improving nutritional status in surgical patients than standard enteral nutrition. 9
We also observed that the oligomeric diet was able to limit TBI-induced thymus atrophy. This is a major finding, because total thymocyte count parallels thymic weight, and the drop in thymus weight observed in rats with TBI receiving the standard diet reflects marked impairment of immune function. 4,5 The beneficial effect of the oligomeric formula could be attributed to the restoration of GLN stores. 25 Hence, using the same model of TBI characterized by immune dysfunction, we previously clearly showed that using an IED allowed to both limit thymus atrophy and restore whole-body GLN stores. 5,22 Similar observations have been made in burn-injury and endotoxemic rats fed with ornithine α-ketoglutarate, a GLN precursor. 26,27
Taken together, these results conclude that oligomeric enteral diets are a candidate nutritional care strategy for patients with TBI. Further studies are needed to bring firm evidence of the benefit of using oligomeric diets in TBI patients and to explore the clinical relevance of this promising strategy.
Footnotes
Acknowledgments
This work was supported by an unrestricted grant from Nestlé Clinical Nutrition (NCN), Noisiel, France.
We thank Mrs. J. Moulis for excellent technical assistance.
Author Disclosure Statement
LC does receive fees from NCN.